Week 9: Caring for the Patient Requiring Mechanical Ventilation
1/36
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
37 Terms
Mechanical Ventilatory Support
-any means by which a mechanical device is used
to support, assist, or
control respirations
-goals: improve gas exchange, ventilation, decrease work of breathing
Indications for mechanical ventilation:
-inadequate oxygenation
-inadequate ventilation
-inability to protect the airway
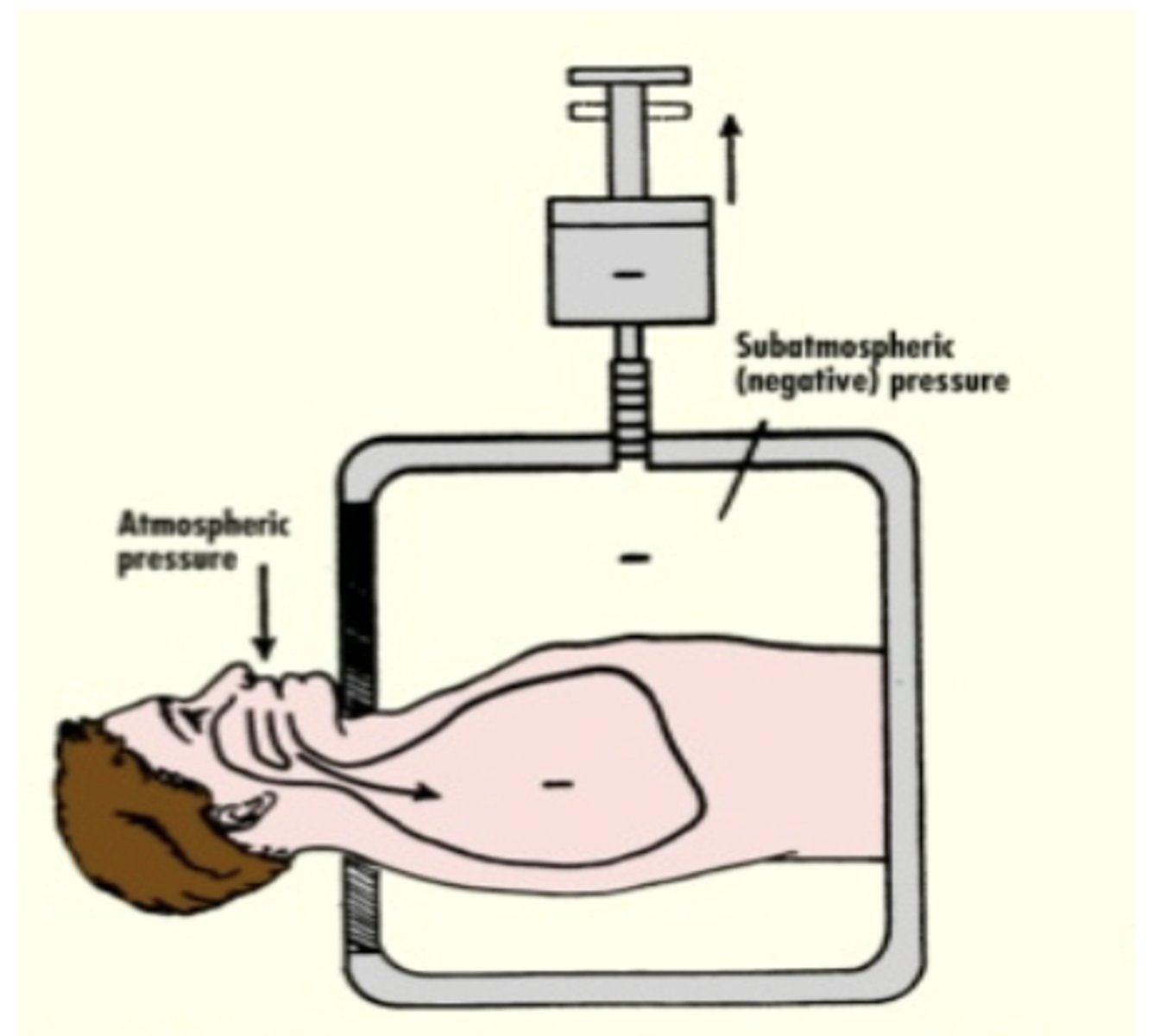
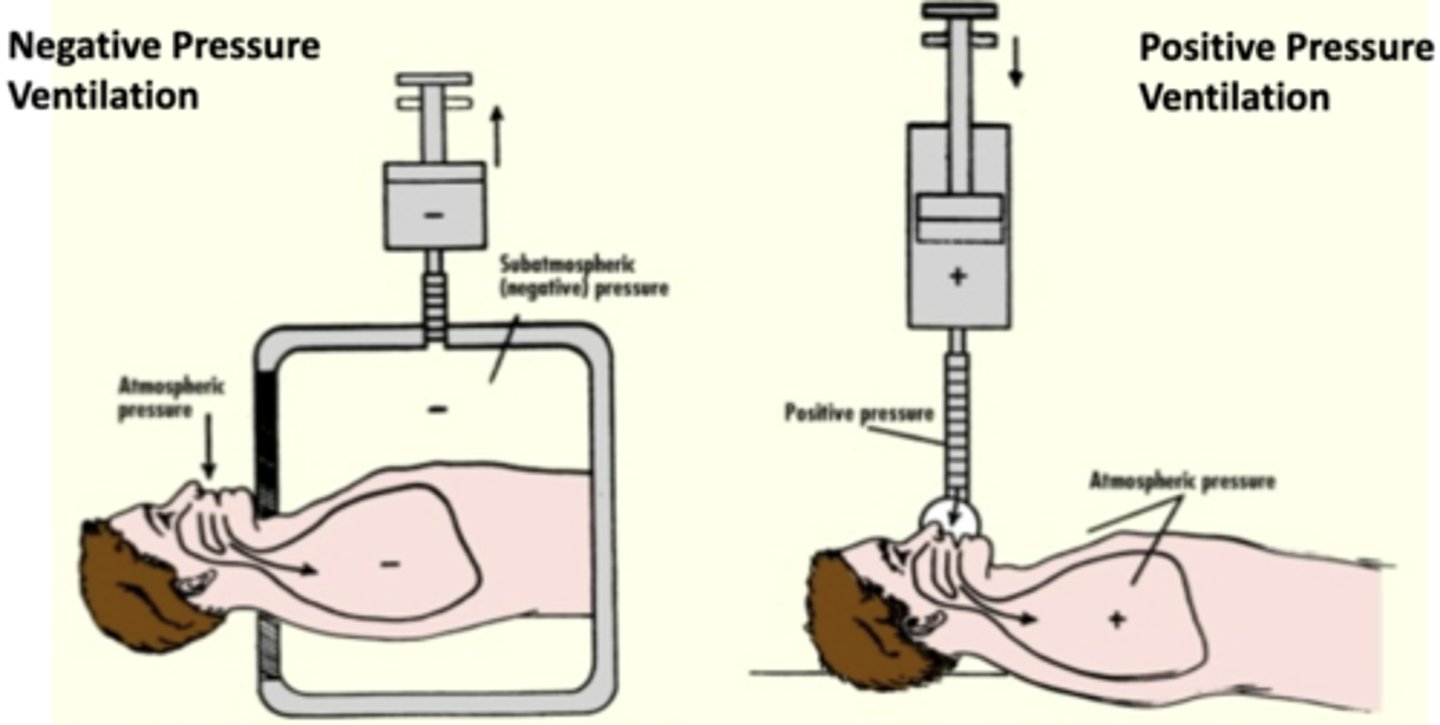
Negative pressure ventilation
-Ventilation of the lungs by expanding the rib cage to "pull" air into the lungs
-ex: iron lung, cuirass ventilation
Positive pressure ventilation
-force air into the lungs to provide breathing assistance
-ex: non invasive, invasive positive pressure
Invasive positive pressure ventilation
-volume controlled (VC) or pressure controlled (PC)
-breath controlled by either of these two modes
Volume control
-Inspiration ends when the set TIDAL VOLUME is reached
-pressure is variable
Pressure control
-Inspiration ends with the set PRESSURE is reached
-volume is variable
Airway resistace
-opposition of the
respiratory tract to airflow during inhalation and
exhalation
-higher pressure needed if present
-ex: asthma, COPD, broncospasms, anaphylaxis, secretions, fighting the vent
Stiff lung
-decreased, low lung compliance, cannot be easily distended
-think an exercise ball
Loose lung
-increased, high lung compliance, or low elastic recoil
Pos and Neg of volume ventilation:
pos: known minute ventilation regardless of changes in airway resistance or compliance
neg: higher risk of ventilator induced lung injury due to changes in resistance or pressure
Volutrauma
Damage to the lung by excess volume delivered to one lung over the other
-lower tidal volumes (6 mL/kg IBW)
-avoids over distention by reducing fixed volume
Barotrauma
Injury caused by pressure, from too much pressure in the lungs
-<30 cm H2) limits pressure
-continuous monitoring and adjustment to prevent pressures or during stiff lungs
Pos and Neg of pressure ventilation:
-pos: limits peak pressures, less over distention
-neg: no idea how much volume a patient will recieve
Continuous Mandatory Ventilation (CMV)
-delivers a preset number of fully controlled breaths, regardless of the patient’s effort
-ALL BREATHS MANDATORY
Intermittent Mandatory Ventilation (IMV)
-delivers a set number of
mandatory breaths while allowing the patient to breathe spontaneously
between them
-MANDATORY AND SPONTANEOUS BREATHS
Continuous Spontaneous Ventilation (CSV)
-allows the patient to initiate every breath, with the ventilator providing supportive pressure rather than mandatory breaths
-only used with pressure-controlled ventilation
-ALL BREATHS SPONTANEOUS
Pressure Controlled: Continuous
Mandatory Ventilation (PC-CMV)
-delivers a preset number
of mandatory breaths at a preset inspiratory pressure and inspiratory
time
Pressure Controlled: Intermittent
Mandatory Ventilation (PC-IMV)
-delivers a preset
number of mandatory breaths at a
preset inspiratory pressure and
inspiratory time
-between breaths patient can breathe spontaneously
Continuous Spontaneous Ventilation (PC-CSV)
-patient regulates their own tidal volume and respiratory rate each breath is assisted by a preset inspiratory pressure
-decreases patient's work of breathing
-can be used as a weaning trial to see extubation
Positive End Expiratory Pressure (PEEP)
-the application of positive pressure at the end of exhalation
- the amount of pressure
remaining in the lung at the END of the
expiratory phase
Complications of high levels of PEEP:
-DECREASES CARDIA OUTPUT = DECREASED BP
-increases intracranial pressure
-can cause pneumothorax
High pressure causes:
-tube or vent is kinked
-secretions or water blocking tube
-coughing
-bronchospasms
-fighting the vent
-patient biting down on vent
Low pressure causes:
-vent tubing disconnected
-ET cuff leak
-self extubation
What happens as compliance decreases in volume-controlled ventilation?
Higher peak inspiratory pressures (PIP) leading to
barotrauma
The "high pressure" alarm on the mechanical ventilator starts to go off. Patient is experiencing desaturations of 83%
manual resuscitation with ambu bag and 100% FiO2
-ALWAYS TAKE PT OFF AND BAG if cannot determine reason
Minute ventilation equation:
RR x tidal volume
20 breaths/min x 500 mL = 10 L/min
Nursing considerations for intubation:
-REMOVE DENTURES
-place patient in sniffing position with neck extended
-induction and then paralytic agent
Capnography
-provides feedback about the adequacy of ventilation
-assesses how much CO2
Under inflation of cuff:
-escape of ventilator gases
-aspiration (secretions can pool around cuff)
Over inflation of cuff:
tracheal damage
Closed Inline suction system:
-maintains oxygenation better than the open technique
-decreases exposure to
secretions
-DOES NOT decreased ventilator associated pneumonia
Indications for suctioning
-high pressure alarm sound
-coarse breath sounds
-RR increases
-sustained cough
-sudden drop in SpO2
Nursing considerations for suctioning:
-pre oxygenate w/100% FiO2
-limit suctioning 5-10 sec for infants
-limit suctioning 10-15 sec for adults
-if pt cannot tolerate: STOP and manually hyperventilate
-maintain sterile technique
-do NOT put NS into ET tube
-for thick secretions provide hydration and humidification
Nursing considerations for tracheostomy:
-improves pt comfort, allows oral care, nutrition, communication
-provide enteral nutrition (AVOID BOLUS TUBE FEEDINGS)
-maintain HOB at least 30 degree
-NG tube connected to low, intermittent suction if placed below pylorus
Weaning from mechanical ventilator:
-patients who are intubated for less than 24 hours do not need to undergo a
weaning trial
Spontaneous awakening trials (SAT)
-sedation is temporarily paused to see if the patient can
wake up without severe agitation or pain