health assessment exam 1
1/186
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
187 Terms
~~subjective and objective data~~
2
subjective data
anything patient says
objective data
measurement, auscultation, touch, inspection, percussion (MATIP)
objective data may be impacted by…
Open ended question, location of symptom, description of the symptom, timing, aggravating factors
objective data may be impacted by…
mental status, comfort, quality of questioning, communication, emotion
objective data may be impacted by…
accuracy of measuring devices
skill of examiner
integrity of examiner senses
ability of patient to withstand examining
~~Vital signs~~
3
weight children significant loss
>5% 1 month
>10% 6 months
weight children index
>85th: overweight
>95th: obese
adult weight cause for concern
>4.5kg 1 month
temperature normal range
98.6~100.4 F
pulse normal range
60~100
resp normal range
12~20
BP pre-hypertension
120~129/~80
BP hypertension stage 1
130~139/80~89
hypertension stage 2
140+/90+
medication for hypertension when?
at stage 2 (140+/90+)
medication for hypertension when if co-morbid?
at stage 1 (130~139/80~89)
age 60+ hypertension
not treated until 150+
UNLESS co-morbid
hypertensive crisis
>180/120 WITH SYMPTOMS
hypertensive crisis symptoms
chest pain
shortness of breath
severe headache/dizziness
vision changes
numbness/difficulty speaking
severe back pain
what to look for when hypotension?
MAP (mean arterial pressure)
MAP normal range
above 50
~~patient interview~~
5
a complete patient interview includes
Age
previous illness
surgical history
Medications history
family medical history
Allergies
Patient Identification
Chief Complaint
History of Present Illness
Surgical History, Family History, Social History
Review of Systems
during patient interview, nurses should NOT:
Give Advice
Ask biased Questions
Express false Reassurance
Use “Why Questions”
facilitation
responses designed to facilitate more information sharing
reflection
Repeating a portion of a clients statement in order to gain greater meaning "you say your getting tired of my lecture?”
clarification
Asking the client to expand on a topic to increase your understanding
empathetic responses
“I understand how you feel”
“that must be hard for you”
confrontation
Some issues or responses may require you to confront patients about their feelings
interpretation
A conclusion reached based on evidence and reasoning
~~health history~~
2
components of health history interview
Biographic Data (Patient Identification)
Allergies
Medications
Chief Complaint (CC)
History of Present Illness (HPI)
Past Medical History (PMH)
Past Surgical History (PSH)
Family History (FH)
Social History (SH)
Review of Systems (ROS)
History of Present Illness (HPI)
OLDCARTS
onset
location
duration
characteristics
aggravating and alleviating factors
radiation
temporal factors
severity
~~review of systems~~
1
review of systems
Constitutional/General OverallHealth State
Head, Ears, Eyes, Nose, Throat(HEENT) & Neck
Skin (Derm)
Respiratory
Cardiovascular
Gastrointestinal
Musculoskeletal
Neurological
~~Head, ear, nose, neck, mouth, throat~~
4
PQRST
Precipitating or palliative (what brings it on)
Quality or quantity (mild, sharp)
Region or radiation (where?)
Severity scale
Timing
head assessment
Inspect head and scalp
Inspect face
Palpate head
Palpate face for Maxillary, frontal sinuses, and check for TMJ
Palpate masseter muscle strength CN V (Trigeminal):
Facial sensation CN V(Trigeminal)
Facial symmetry CN VII (Facial)
neck assessment
position of trachea
palpate thyroid
carotid pulses
lymph nodes
muscle mass/strength CN XI
thyroid assessment
posterior or anterior approach
head normal
skull feels symmetric and smooth
Cranial bones have normal protrusions
no tenderness to palpation
temporomandibular(TMJ) joint: smooth movement with no limitation or tenderness or crepitus (popping)
maxillary & frontal sinuses has no tenderness/pain
lymph nodes normal
movable,soft, nontender
cranial nerve for swallowing?
CN IX, X
Presbycusis
age-related hearing loss
move adult pinna
up and back
move child pinna
straight down
whispered voice test CN
CN VIII
decreased saliva?
NOT normal with aging—anticholinergic effect of medication
epistaxis
nosebleed
smell CN
CN I
polyps
benign, may grow inside nose due to allergies
tongue movement CN
CN XII
tonsil grade 1
visible
tonsil grade 2
halfway between tonsillar pillars and uvula
tonsil grade 3
touching uvula
tonsil grade 4
touching each other
~~Thorax and lungs~~
11
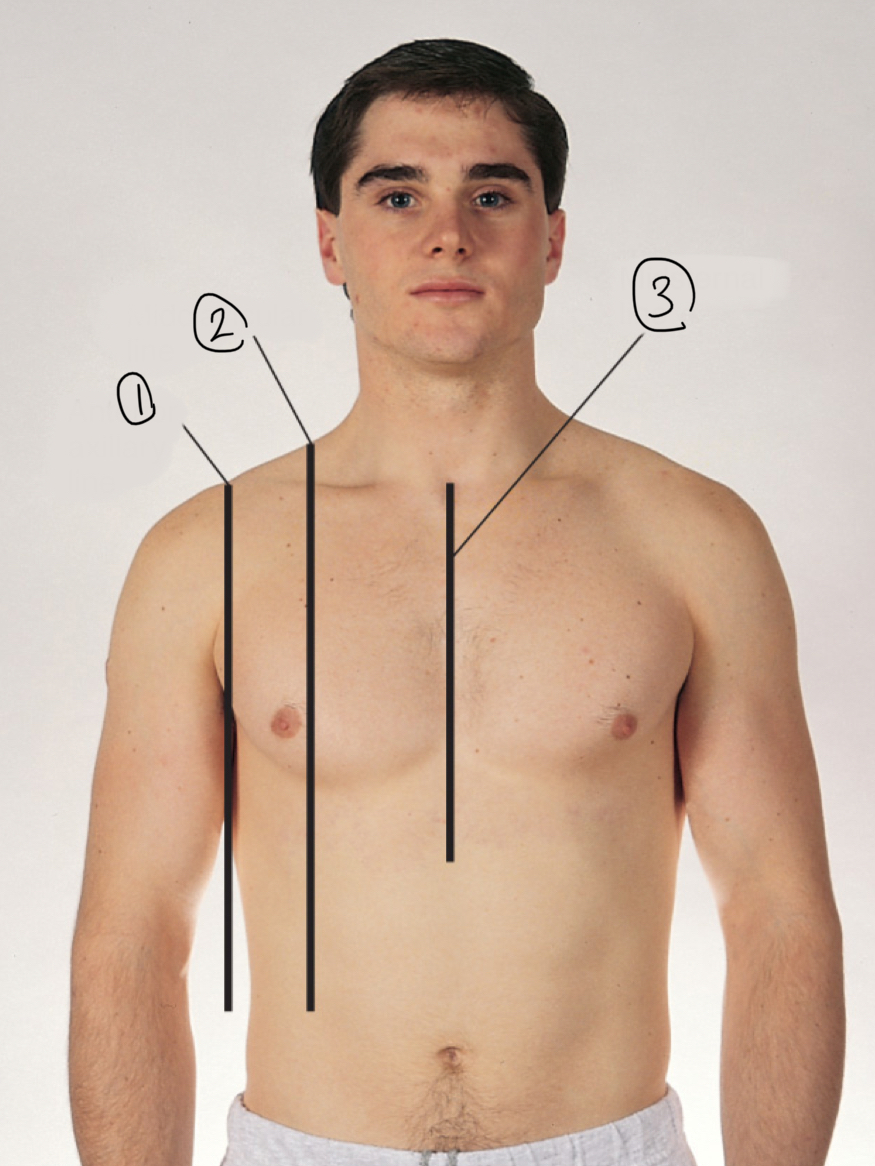
1
anterior axillary line
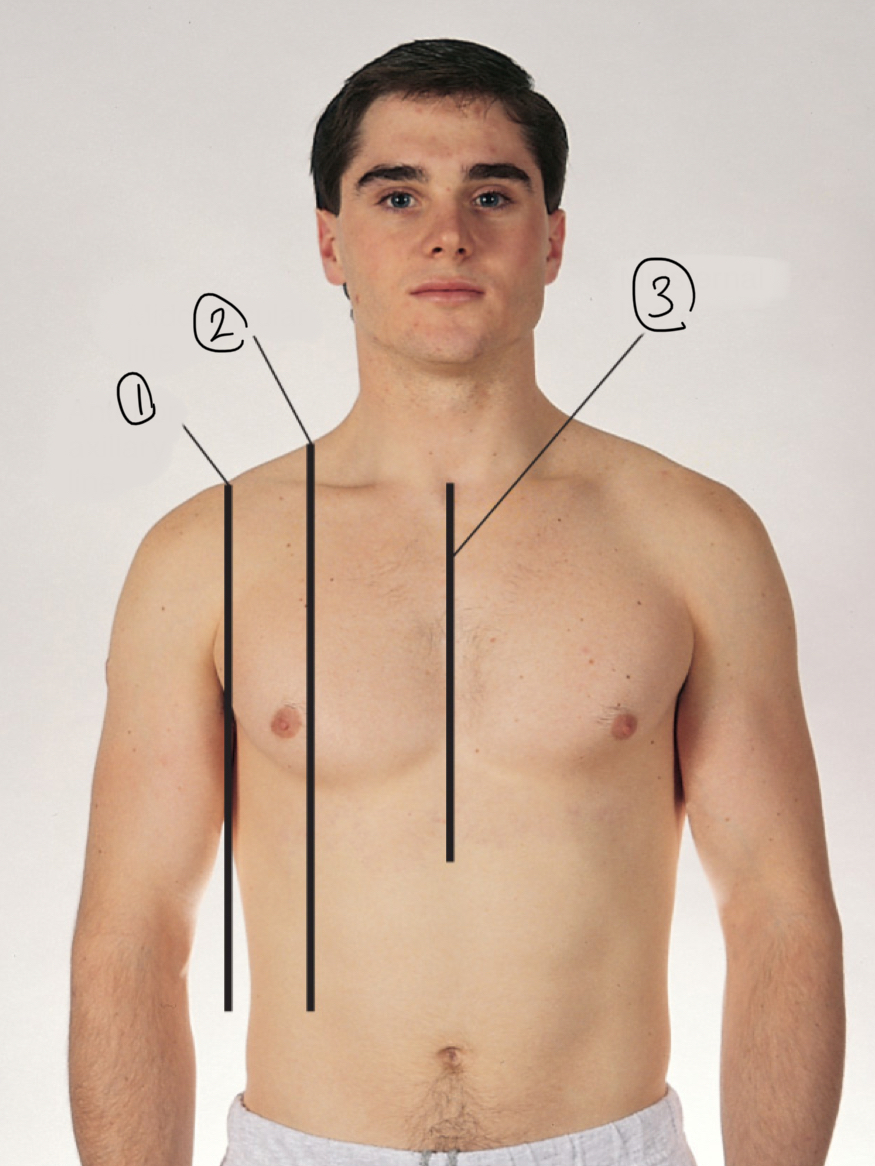
2
midclavicular line
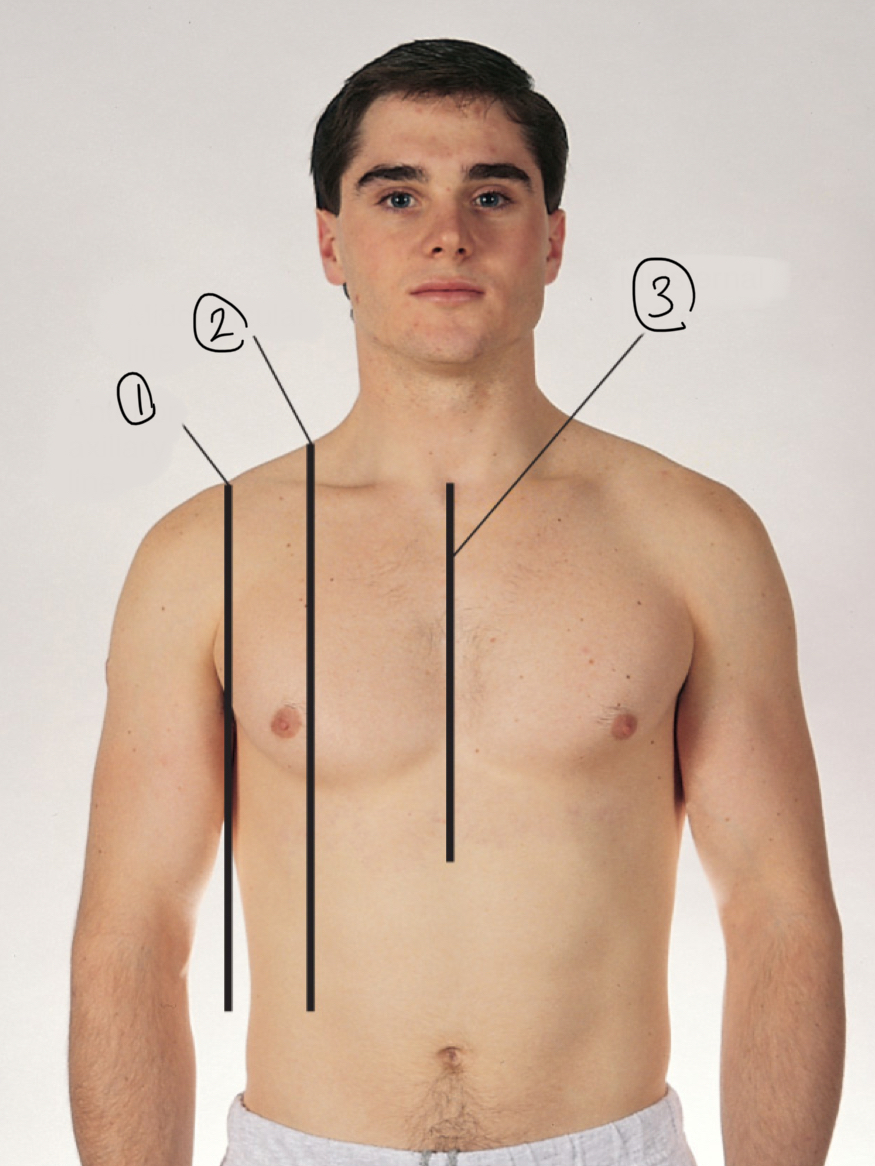
3
midsternal line
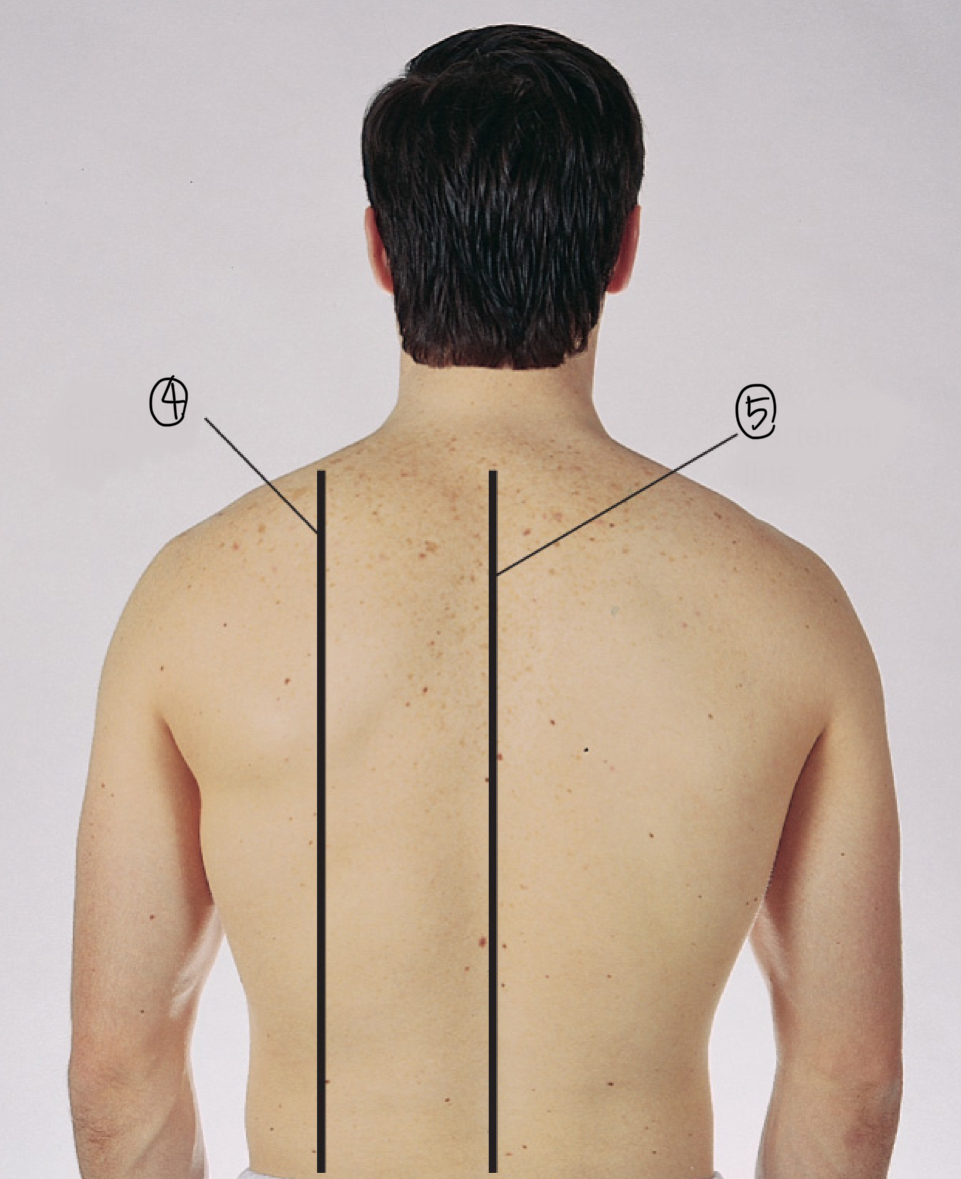
4
scapular line
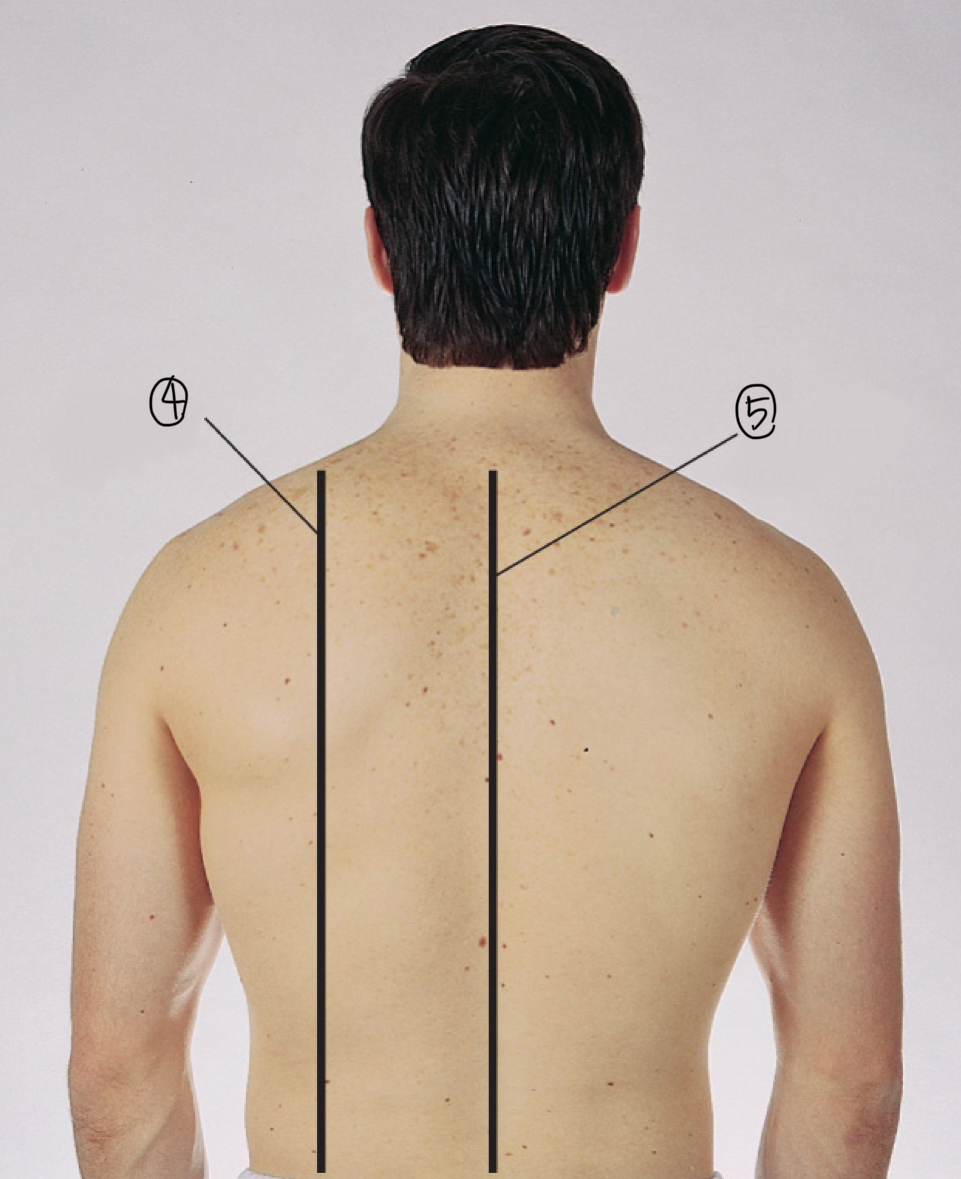
5
vertebral line
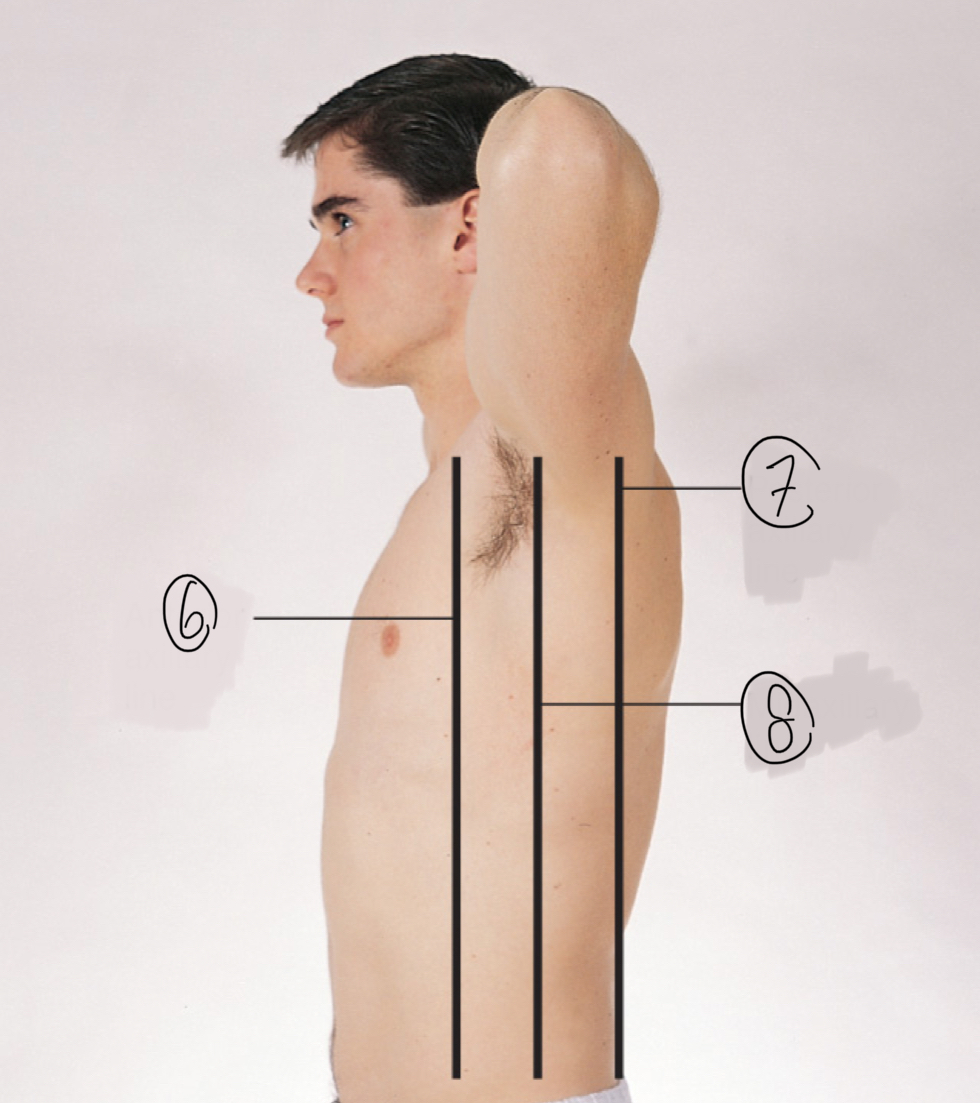
6
anterior axillary line
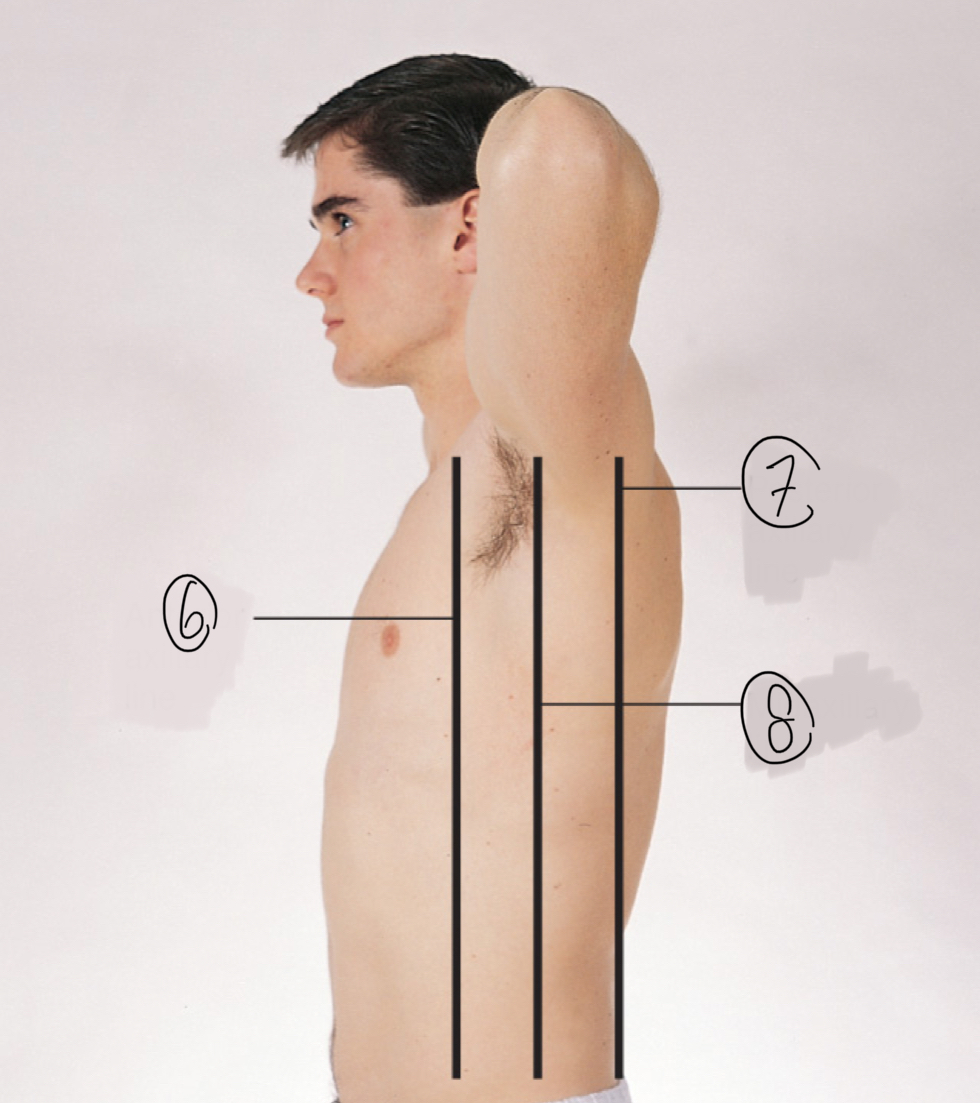
7
posterior axillary line
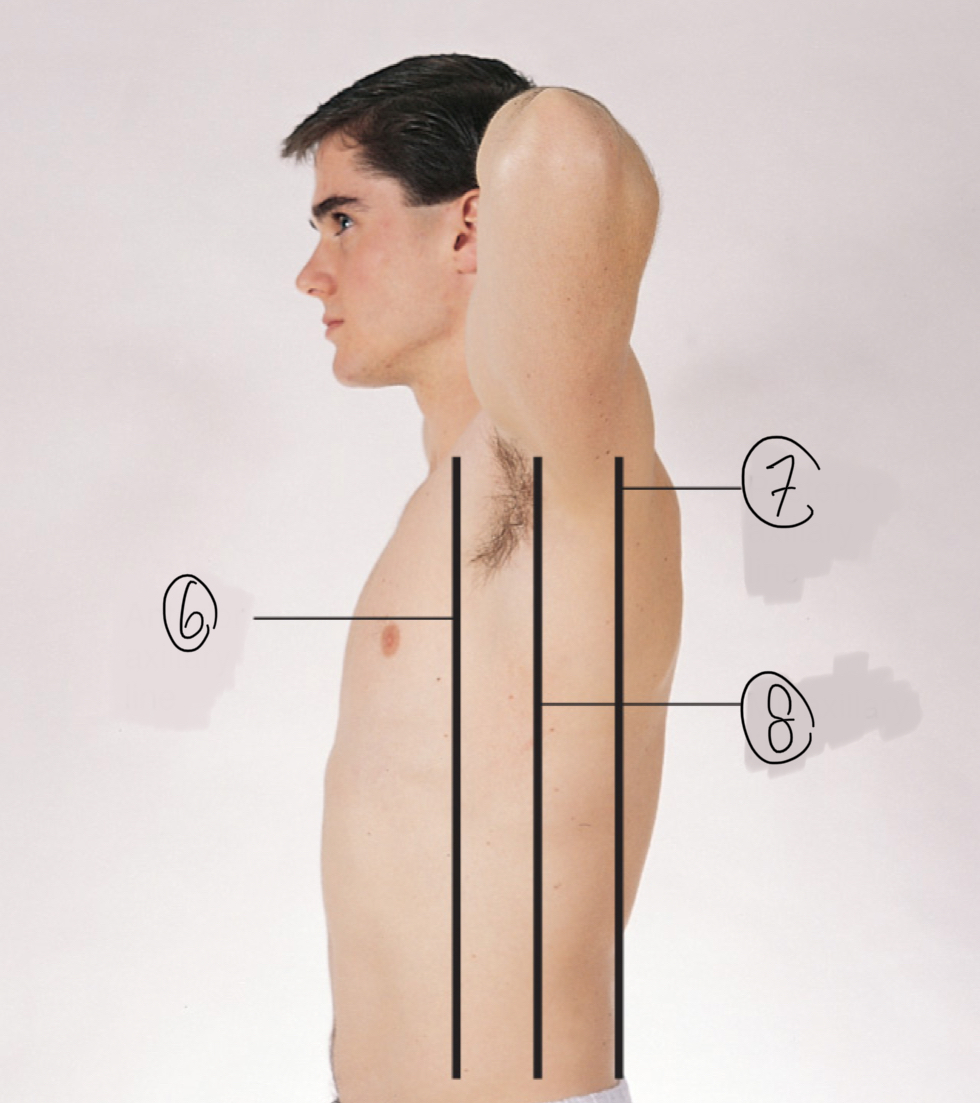
8
midaxillary line
pediatric respiratory
lack surfactant to keep alveoli open
pregnancy respiratory
elevated diaphragm, widened thoracic cavity
aging adults respiratory
less elasticity in sternal cartilage
more fracture during CPR
pack-year
packs per day x how many years
O2 normal levels
97~98%
clubbing fingernails
chronic hypoxemia
barrel chest
chronic lung disease
Pectus carinatum
sternum sticks out like pigeon chest
pectus excavatum
sternum is dished in
tactile fremitus
palpate both sides of the chest, comparing density
lung percussion normal findings
dull over scapulae
Dull over heart on left
Dull on right over liver
Diaphragmatic excursion
patient inhale & exhale, percuss and compare resonant and dull areas on both sides
pneumothorax
air in pleural space
effusion
serous fluid in the pleural space
hemothorax
blood in the pleural space
empyema
pus in the pleural space
~~cardiac and pulmonary vasculature~~
10
AV valve
tricuspid & mitral
SL valve
aortic & pulmonary
right AV valve
tRicuspid
left AV valve
mitraL
which is thicker: atrium or ventricles
ventricles
thickest heart chamber
left ventricle
what happens during diastole
ventricles relax and fill with blood
what happens during systole
heart contracts
blood leaves ventricles and travel through arteries
what happens during s1
lub
close AV valves
beginning of systole
what happens during s2
dub
close SL valves
end of systole
s3 & s4
abnormal
when is s3?
after s2
why s3 happens?
ventricles are resistant to filling (ventricular gallop)
when is s4?
before s1
why does s4 happen?
atrial gallop