neuroanatomy exam 2
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
Neuroectoderm derivatives including associated ventricular system structures
telencephalon
cerebral hemispheres + olf. bulb + olf. cortex
lateral ventricles
diencephalon
thalamus + hypothalamus + epithalamus
3rd ventricle
mesencephalon
midbrain
cerebral aqueduct
metencephalon
pons + cerebellum
4th ventricle
myelencephalon
medulla oblongata
4th ventricle + central canal
neural tube
spinal cord
central canal
Which ventricular system structures are associated w/ which adult structures?
lateral ventricle → cerebral hemisphere
3rd ventricle → thalamus + hypothalamus
cerebral aqueduct → midbrain
4th ventricle → pons + medulla
central canal → spinal cord
Where is the location of the choroid plexus?
lateral, 3rd, 4th ventricles
Explain the circulation of CSF from production to drainage
CSF prod. by choroid plexus in lateral, 3rd, 4th ventricles
CSF prod. in lat. ventricles must drain into 3rd ventricles via interventricular foramina → then into 4th ventricles via cerebral aqueduct
drainage:
4th ventricle → lateral apertures → subarachnoid space → arachnoid villi → dorsal sagittal sinus → cerebral veins
4th ventricle → central canal in spinal cord
What are the fxns of CSF?
suspend brain in liquid:
reduce effective weight
prevention of blood supply being cut off
cushion CNS from mechanical trauma
maintain CNS homeostasis
provide extracellular fluid
remove metabolic wastes of CNS
What problems are associated w/ obstruction of CSF circulation?
obstruction of CSF circ. → inc. intracranial pressure → compression of midbrain → narrowing of cerebral aqueduct → accumulation of CSF in lateral + 3rd ventricles → further inc. intracranial pressure → cerebral edema severity compounds
hydrocephalus = accumulation of CSF
cerebral edema = brain tissue swelling due to fluid buildup in intracellular/extracellular space causing inc. intracranial pressure
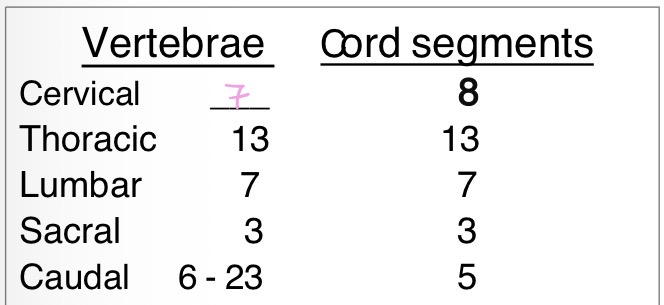
How do spinal cord segments correspond to the vertebrae? Which vertebrae do the sacral segments lie w/i?
36 cord segments → 36 pairs of spinal n.
vertebral column longer than spinal cord
sacral segments of spinal cord lie w/i L5
spinal segment nn. enter/exit thru IVF cranial to vertebrae of same #
spinal segments do not align w/ lumbar vertebrae
3 basic fxns of spinal cord?
mediate spinal reflexes
pathway for afferent sensory signals to the brain
pathway for efferent motor signals to the spinal motor neurons
What is a dermotome?
area of skin (except face) that has its sensory innervation by the dorsal root of a single spinal n.
map of dermatomes represented in somesthetic cerebral cortex
What spinal cord segments correspond to what regions of the body?
C1-C5 → cervical region
C6-T1(2) → cervical enlargement = brachial plexus → thoracic limbs
T1-L3 → trunk region
L4-S1(2) → lumbosacral enlargement = lumbosacral plexus → pelvic limbs
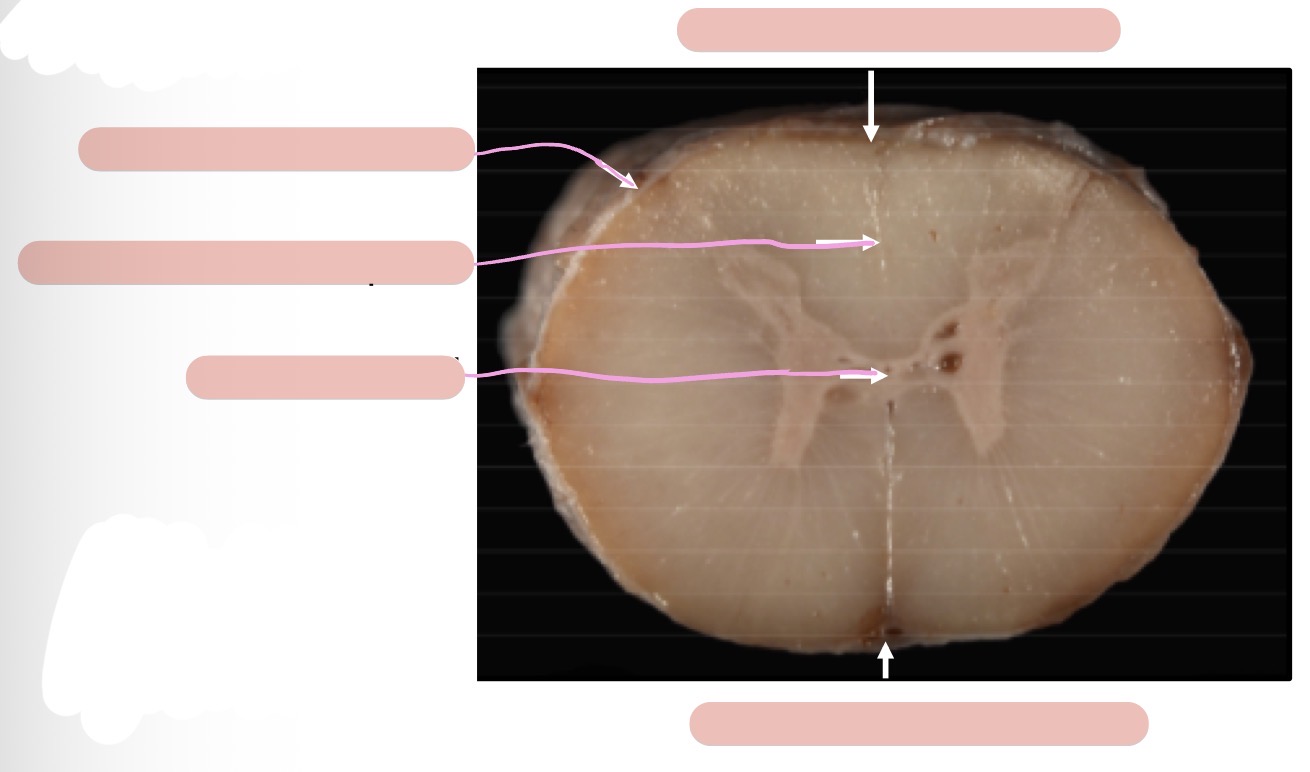
What kind of tracts are in the dorsal, lateral, and ventral funiculi?
dorsal → sensory only
lateral → sensory + motor
ventral → sensory + motor
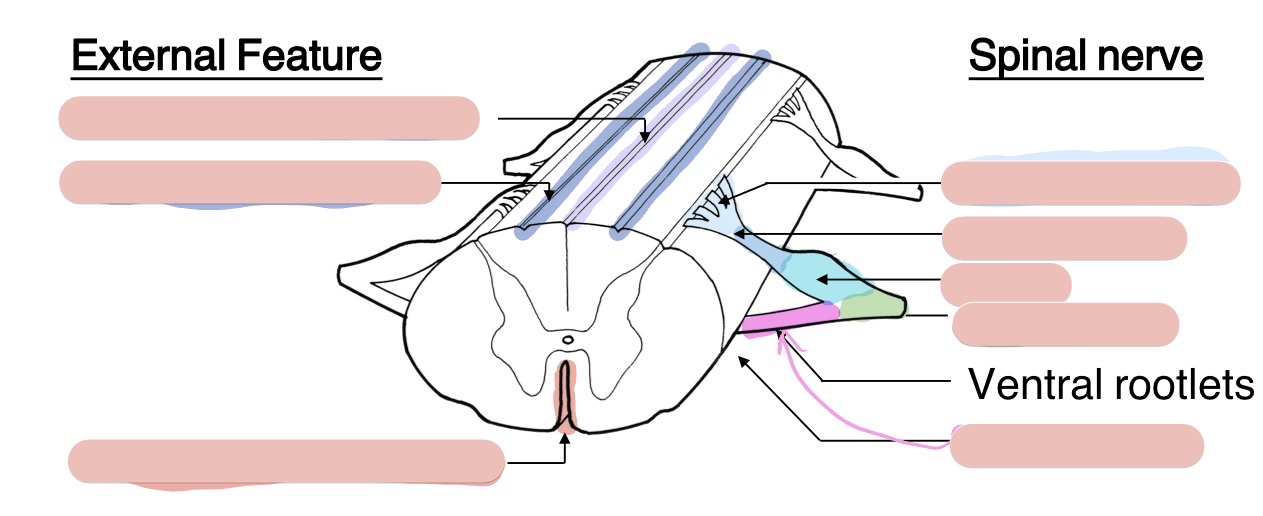
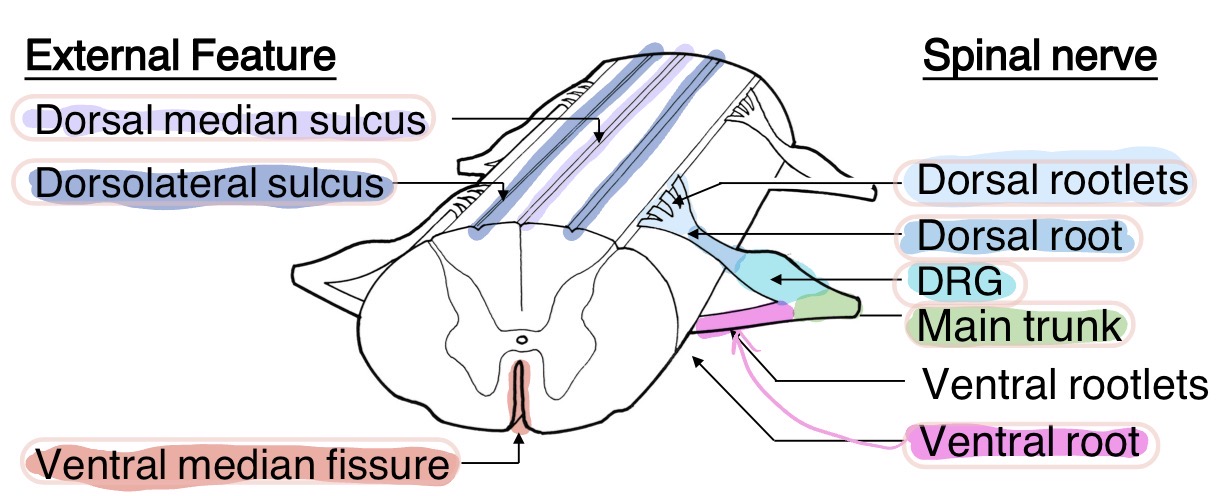
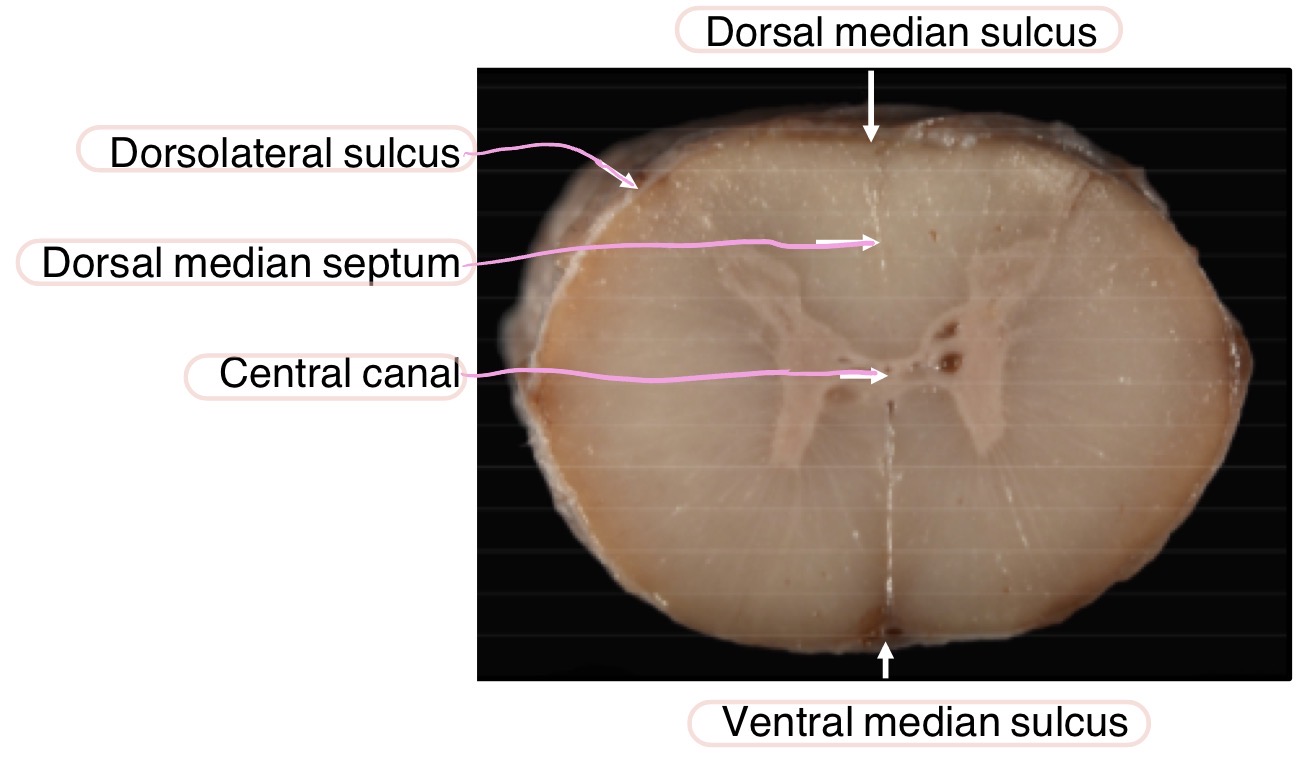
Where are glia, perikarya, dendrites, and axons located in the spinal cord?
gray matter
Where are spinal sensory + motor nuclei located in the spinal cord?
sensory nuclei in the dorsal horn
somatic motor nuclei in the ventral horn
What are the sensory receptors in the epidermis + dermis?
epidermis
free nerve endings → pain, temperature, touch
dermis
Meissner’s corpuscle → touch, vibration
Merkel’s corpuscle → touch, pressure
Ruffini’s corpuscle → stretching
hair follicle terminal → touch
Spinothalamic tract sensory receptors + modality, primary sensory neuron, location of perikarya of projection neurons + ascending tracts, destination
1) pain + temperature sensory receptors
2) primary sensory neurons: DRG neurons
3) enter spinal cord at dorsal horn
4) travel bilaterally L/R in lateral funiculus
5) thalamus → somesthetic cortical area of cerebral cortex
Fasciculus gracilis sensory receptors + modality, primary sensory neuron, location of perikarya of projection neurons + ascending tracts, destination
1) tactile sensory receptors innervating body caudal to T1
2) primary sensory neurons: DRG neurons
3) enter spinal cord at dorsal horn
4) travel unilaterally + ipsilaterally at medial aspect of dorsal funiculus
5) cross over to contralateral thalamus → somesthetic cortical area
Fasciculus cuneatus sensory receptors + modality, primary sensory neuron, location of perikarya of projection neurons + ascending tracts, destination
1) tactile sensory receptors innervating body C1-T1 (thoracic limb + neck) + conscious proprioception of thoracic limb
2) primary sensory neurons: DRG neurons
3) enter spinal cord at dorsal horn
4) travel unilaterally + ipsilaterally in lateral aspect of dorsal funiculus
5) cross over to contralateral thalamus → somesthetic cortical area of cerebral cortex
How do animals know the location of stimuli applied to the skin?
dermatomes = area of skin supplied by a single spinal n.
map of dermatomes represented in somesthetic area of cerebral cortex
conscious vs. subconscious proprioception
conscious proprioception → contralateral thalamus + cerebrum
active awareness of where body is in space
subconscious proprioception → ipsilateral cerebellum
not consciously aware like regulation of muscle tone to maintain posture
Spinocuneocerebellar tract sensory receptors + modality, primary sensory neuron, location of perikarya of projection neurons + ascending tracts, destination
1) proprioceptive receptors (m. spindle, pacinian corpuscle, golgi-tendon organ, Ruffini’s corpuscle) for subconscious proprioception of thoracic limb
2) primary sensory neurons: DRG neurons
3) enter through dorsal horn of spinal cord
4) travel unilaterally + ipsilaterally in dorsal funiculus next to fasciculus cuneatus
5) ipsilateral cerebellum
Spinomedullary tract sensory receptors + modality, primary sensory neuron, location of perikarya of projection neurons + ascending tracts, destination
1) proprioceptive receptors for conscious proprioception of pelvic limb + tail
2) primary sensory neurons: DRG neurons
3) enter at dorsal horn of spinal cord
4) travel unilaterally + ipsilaterally in dorsal funiculus briefly before reaching nucleus thoracicus in lateral funiculus
5) ascend in spinomedullary tract in lateral funiculus
6) cross over to contralateral thalamus → cerebral cortex
Dorsal spinocerebellar tract sensory receptors + modality, primary sensory neuron, location of perikarya of projection neurons + ascending tracts, destination
1) proprioceptive receptors for subconscious proprioception of pelvic limb + tail
2) primary sensory neurons: DRG neurons
3) enter at dorsal horn of spinal cord
4) travel unilaterally + ipsilaterally in dorsal funiculus briefly before reaching nucleus thoracicus in lateral funiculus
5) ascend in dorsal spinocerebellar tract tract in lateral funiculus
6) ipsilateral cerebellum
Proprioceptive positioning test what does it test, how to perform it, what functioning structures does it require?
tests conscious proprioception
turn paw over → animal should flip paw back over to normal position
req:
spinal n. + peripheral n. (sensory + motor)
spinal cord
thalamus + cerebellum
somesthetic + motor cortices
How is pain, temperature, touch, and conscious/subconscious proprioception sensed in the thoracic limb?
1) sensory receptors
2) primary sensory neurons: DRG neurons
3) information enters at dorsal horn of spinal cord at cervical enlargement
4)
pain + temperature → ascends bilaterally in spinothalamic tract in lateral funiculus → bilateral thalamus + cerebral cortex
touch → ascends unilaterally + ipsilaterally in fasciculus cuneatus in dorsal funiculus → contralateral thalamus + cerebral cortex
conscious proprioception → ascends unilaterally + ipsilaterally in fasciculus cuneatus in dorsal funiculus → contralateral thalamus + cerebral cortex
subconscious proprioception → ascends unilaterally + ipsilaterally in spinocuneocerebellar tract in dorsal funiculus touch → ipsilateral cerebellum
How is pain, temperature, touch, and conscious/subconscious proprioception sensed in the pelvic limb?
1) sensory receptors
2) primary sensory neurons: DRG neurons
3) enter at dorsal horn of spinal cord at lumbosacral enlargement
4)
pain + temperature → ascends bilaterally in spinothalamic tract in lateral funiculus → bilateral thalamus + cerebral cortex
touch → ascends unilaterally + ipsilaterally in fasciculus gracilis in dorsal funiculus → contralateral thalamus + cerebral cortex
conscious proprioception → starts in dorsal funiculus → nucleus thoracicus → ascends unilaterally + ipsilaterally in spinomedullary tract in lateral funiculus → contralateral thalamus + cerebral cortex
subconscious proprioception → starts in dorsal funiculus → nucleus thoracicus → ascends unilaterally + ipsilaterally in dorsal spinocerebellar tract → ipsilateral cerebellum
Corticospinal tract origin, pathway, location in spinal cord, fxn, lesion
origin + pathway: cerebral motor cortex (postcruciate gyrus + rostral suprasylvian gyrus) → internal capsule → crus cerebri → pyramid → pyramidal decussation → lateral corticospinal tract + ventral corticospinal tract in spinal cord
location:
majority corticospinal fibers cross over at pyramidal decussation → become lateral corticospinal tract → descend in lateral funiculus
rest travel ipsilaterally as ventral corticospinal tract → ventral funiculus → do eventually cross contralaterally at enlargements
fxn:
UMN
precise + refined voluntary control of extremities
lesion:
Rubrospinal tract origin, pathway, location in spinal cord, fxn, lesion
origin + pathway: red nucleus → axons cross over → descend contralaterallay as rubrospinal tract in spinal cord
location: lateral funiculus
fxn:
key voluntary motor tract in dog
UMN
excite flexors
lesion:
Medullary reticulospinal tract origin, pathway, location in spinal cord, fxn, lesion
origin + pathway: medullary RF → descend ipsilaterally as medullary reticulospinal tract in spinal cord
location: lateral funiculus
fxn:
UMN
excite flexors
inhibit extensors
maintain m. tone necessary for supporting body against gravity, postural adjustments, synergistic mvmt
lesion:
decrease of excitation of flexors on the same side of the body
Pontine reticulospinal tract origin, pathway, location in spinal cord, fxn, lesion
origin + pathway: pontine RF → descend ipsilaterally as pontine reticulospinal tract in spinal cord
location: ventral funiculus
fxn:
UMN
excite extensors = anti-gravity mm.
inhibit flexors
maintain m. tone necessary for supporting body against gravity, postural adjustments, synergistic mvmt
lesion:
decrease of excitation of extensors on the same side of the body
Vestibulospinal tracts origin, pathway, location in spinal cord, fxn, lesion
origin + pathway: vestibular nuclei → descend ipsilaterally in spinal cord as lateral + medial vestibulospinal tracts
location: ventral funiculus
fxn:
UMN
excite extensors
help maintain normal standing posture
lesion:
decreased excitation of extensors on the same side of the body
Describe how UMN + LMN work
UMN
CNS
cell bodies in brain? + axons in spinal cord
synapse on other neurons
always excitatory
excite inhibitory or excitatory interneurons
interneurons
CNS
cell bodies + axons in gray matter of spinal cord
innervate LMN
either excitatory OR inhibitory
LMN
CNS
cell bodies in ventral horn of spinal cord
alpha motor neuron → inn. skeletal m.
ALWAYS excitatory
visceral motor neuron → inn. smooth + cardiac mm.
gamma motor neuron → inn. muscle spindle
How do motor units fxn in voluntary mvmts? Are they activated all at the same time or in sequence? How is appropriate force generated?
motor unit = a motor neuron coming from ventral horn spinal cord + all the m. fibers it innervates
voluntary mvmt → alpha motor neuron bc they inn. skeletal m.
activated in sequence PRN to gen. more force
appropriate force generated by activating more motor units until enough force is generated for any given task
motor units are on/off
4 basic aspects of a reflex
sensory component
motor component = LMN
local
do NOT depend on UMN
tho UMN have a net inhib. effect on the body
Limbs affected, touch, pain, proprioception, motor fxn, reflexes, muscle tone in L side complete hemisection C1-C5
limbs: L thoracic + pelvic
touch: absent in L thoracic + pelvic limbs
pain: present in both L limbs
proprioception: absent in both L limbs
motor fxn: absent in both L limbs
reflex: present in both L limbs
Limbs affected, touch, pain, proprioception, motor fxn, reflexes, muscle tone in 1 side complete hemisection C6-T1 cervicothoracic enlargement
Limbs affected, touch, pain, proprioception, motor fxn, reflexes, muscle tone in 1 side complete hemisection T2-L3
Limbs affected, touch, pain, proprioception, motor fxn, reflexes, muscle tone in L side complete hemisection L4-S1 lumbosacral enlargement
limbs: L pelvic
touch: absent in L pelvic limb
pain: absent in L pelvic limb
proprioception: absent in L pelvic limb
motor fxn: absent in L pelvic limb
reflex: absent in L pelvic limb
this is bc no sensory info from the limb can enter in a complete lesion of an enlargement
Monosynaptic vs. polysynaptic reflexes w/ an example of each
Myotatic (stretch) reflex pathway using quadriceps reflex as example
Golgi tendon reflex pathway
crossed extensor reflex pathway
Perineal reflex pathway
Flexor reflex pathway
UMN disease effect on spinal reflexes, muscle tone, paralysis, and muscle atrophy
spinal reflexes: present to exaggerated
hyperreflexia bc loss of opposing Golgi tendon reflex means loss of the general inhib. effect from UMN
ex) Parkinson’s is an UMN disease and patients shake bc loss of inhibition on shaking
muscle tone: present to increased
hypertonic
paralysis: present
muscle atrophy: present
LMN disease effect on spinal reflexes, muscle tone, paralysis, and muscle atrophy
spinal reflexes: decreased to absent
hyporeflexia to areflexia
muscle tone: decreased to absent
hypotonia to atonia
paralysis: yes
muscle atrophy: yes
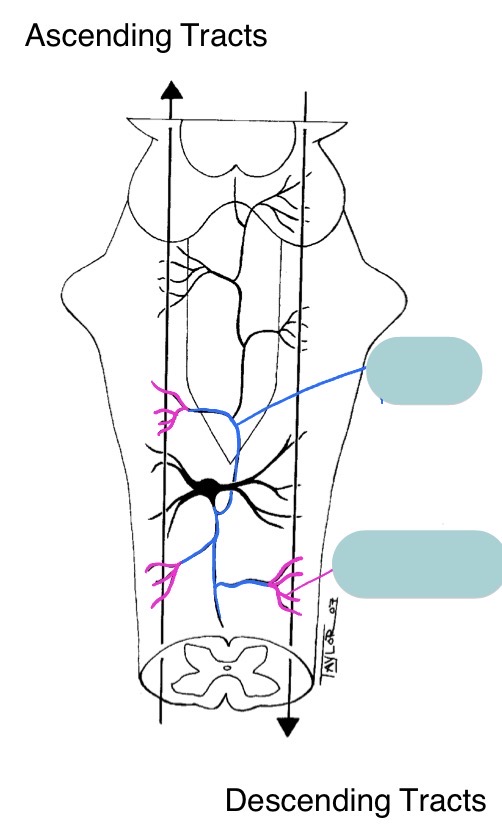
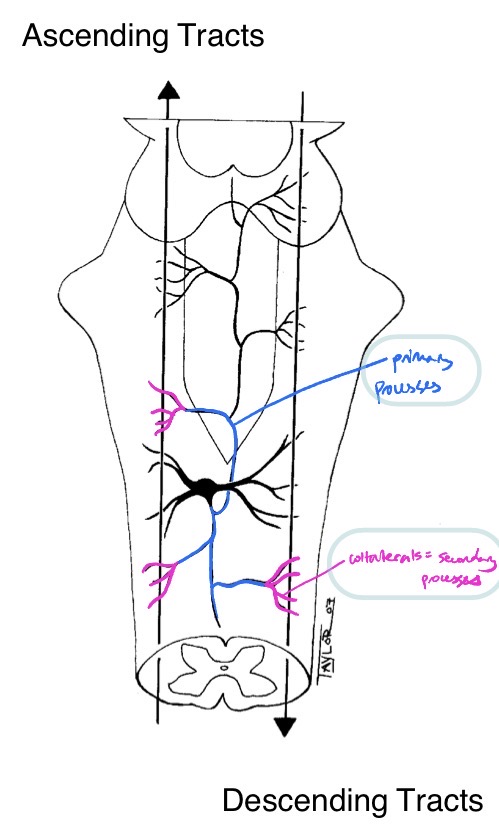
Name these RF structures + their significance
RF neuron has many collaterals comparatively →
allow monitoring of various ascending + descending tracts
receive input from thousands of cells to monitor entire state of body
Explain the role of the RF in consciousness + list the structures involved. Explain using waking up to the sound of an alarm as an example
structures involved in staying awake:
ARAS = ascending reticular activating system
rostral RF (in midbrain)
thalamus
cortex
ARAS wakes up cortex via thalamus
sensory receptors →
rostral RF → (via ARAS) nonspecific thalamic nuclei → cortex + specific thalamic nuclei → primary cortical area(s)
specific thalamic nuclei → primary cortical area(s)
ex) alarm clock rings
cochlear receptors →
rostral RF → nonspecific thalamic nuclei → cortex + medial geniculate nucleus → primary auditory area
medial geniculate nucleus in thalamus → primary auditory area in cortex
Explain the role of the RF in unconsciousness. What do anesthetic drugs usually target and why isn’t it the RF?
dec. ARAS activity + dec. thalamus activity → sleep
anesthetic drugs usually target thalamic neurons
targeting RF riskier bc RF has many jobs
thalamus only job = keep us awake + make sure sensory info gets to the right place
Explain the role of the RF in swallowing
CN 9, 10, 11
swallowing center = central pattern generators that work tgt to cause swallowing
nuc of solitary tract in medullary RF receives sensory input from CN 9 + 10 (pharyngeal mucosa senses bolus) → sends sensory info to swallowing center → facilitates via nuc ambiguus in medullary RF to coordinate motor outputs to CN 9 + 10 + 11
soft palate contracts → pharynx pulled fwd + larynx closes → pharyngeal peristalsis → esophageal peristalsis
What are central pattern generators + their importance to RF?
dedicated network of neurons that act tgt to produce a specific sequence of events
multiple different CPG networks in RF to regulate visceromotor fxns
Explain the role of the RF in vomiting
vomiting center = CPGs in medullary RF
receive inputs from:
chemical trigger zone
vestibular receptors
stomach + small intestine
cortical centers
outputs: (don’t need to know exact)
salivation
inspiration then inhibition of breathing
peristalsis in small intestine
relax pyloric + esophageal sphincters
contract ab. mm.
jaw opens
eject vomitus
Explain the role of the RF in motor fxn
origin of:
pontine reticulospinal tract
ipsilateral
ventral funiculus
UMNs that excite extensors (anti-gravity mm.) + inhibit flexors
medullary reticulospinal tract
mostly ipsilateral
lateral funiculus
UMNs that excite flexors + inhibit extensors
Explain the 4 categories of inputs to the vomiting center
1) chemical trigger zone
located in area postrema = wall of ventricle adjacent to obex
incomplete blood-brain barrier → allows sampling of blood to monitor for bad stuff we may have ingested → input to vomiting center
commonly triggered by anesthetics, opioids, uremia, hypoxia, emetic drugs, chemo drugs
2) vestibular receptors
vestibular receptors sense abnorm. motion → input to vomiting center
mechanism for motion sickness
3) stomach + small intestine
receptors sense irritation/distention → send afferent signals via vagus n. → nuc solitary tract → input to vomiting center
4) cortical centers
fear/smell/sight/trauma processed by cortical centers → input to vomiting center
Describe the general organization + overall fxn of the vestibular system
bilateral vestibular organ senses change in head position → sends afferent signals via vestibular n. of CN 9 → cerebellum + vestibular nuclei
cerebellum → vestibular nuclei
bilateral vestibular nuclei →
vestibulospinal tract → skeletal mm. → change body position
medial longitudinal fasciculus → motor nuclei of CN 3, 4, 6 → change eye position
fxn = reflexively control eye + body position in response to change in head position
Where will head tilt, body circle, and eyes move in normally functioning vestibular sys
head tilt → twd side w/ more activity
body circle → twd side w/ more activity
eyes move → opp. head mvmt
Where will head tilt, body circle, and eyes move in unilateral vestibular sys lesion?
head tilt → twd lesion
body circle → twd lesion
eye mvmt →
quick phase away from lesion
slow phase twd lesion
Structures of the vestibular organ?
located inside petrous portion of temporal bone
membranous labyrinth
osseous labyrinth
3 structural units
3 semicircular ducts w/ ampulla at 1 end → crista ampullaris
utricle → macula
saccule → macula
What are the sensory cells of the vestibular organ + how do they work? Describe the signal transduction
ampulla → crista ampullaris = sensory epithelium
sensory cells lined w/ kinocilium + stereocilia
kinocilium
stereocilia
supporting cells
utricle → macula = sensory epi.
sensory cells
supporting cells
saccule → macula = sensory epi.
sensory cell
supporting cells
signal transduction
stereocilia deflected TWDS kinocilium → inc. firing rate → depolarized
stereocilia deflected AWAY from kinocilium → dec. firing rate → hyperpolarized