CNS Stimulants
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
Cocaine MOA
Blocks reuptake of NE, DA, and serotonin (NET, DAT, SERT); also blocks voltage‑gated Na+ channels(local anesthetic) and cardiac K+ channels(pro arrhythmic)
Main CNS effect of cocaine
Increased DA in synapse → euphoria, reward.
Main CV effect of cocaine
Increased NE → tachycardia, hypertension, vasoconstriction. Inc risk of Intracranial hemmorhage, stroke, MI, seizures
Cocaine pharmacologic effects
Increased HR/BP, alertness, euphoria, decreased appetite/sleep, risk of stroke/MI/seizures.
Cocaine overdose risks
Hyperthermia, seizures, coma, death.
Cocaine withdrawal
Depression, dysphoria, bradycardia, anxiety, craving, fatigue, hypersomnolence.
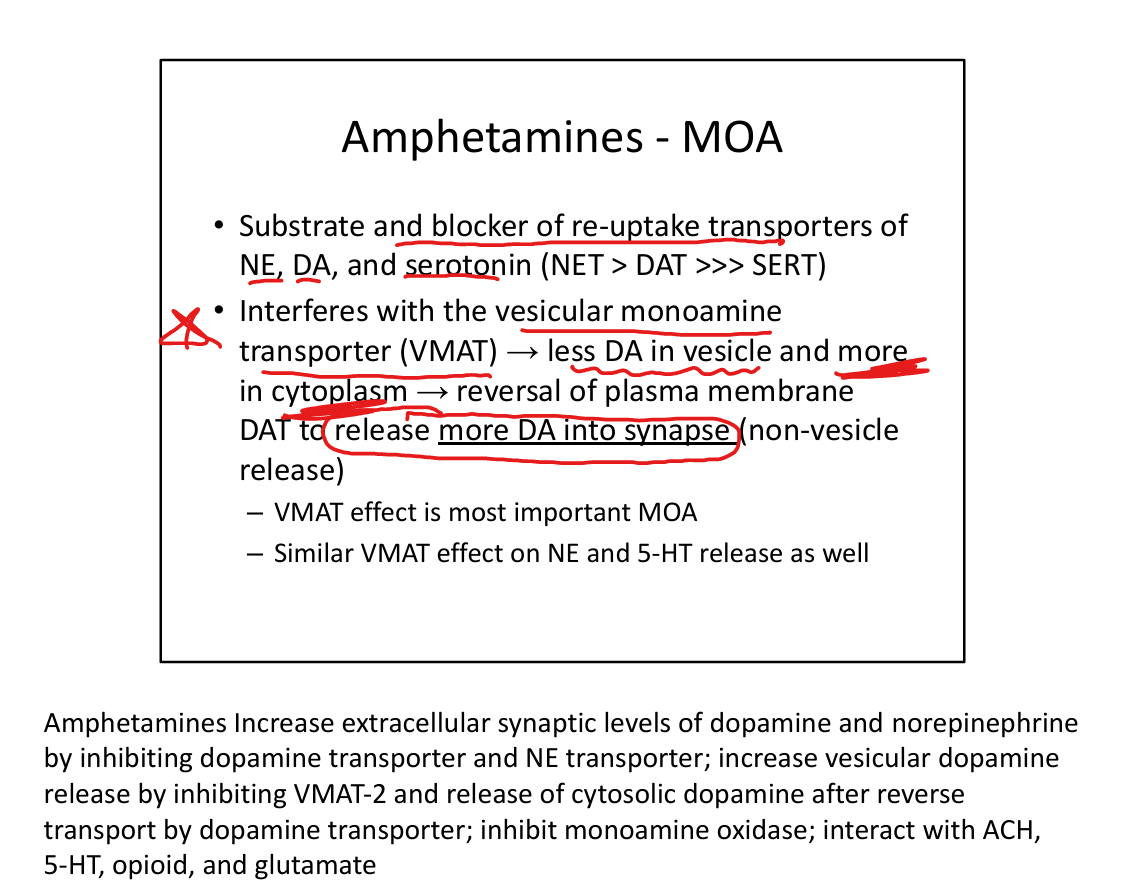
Amphetamine MOA
Substrate for NET/DAT/SERT(blocks reuptake); reverses transporters; inhibits VMAT → increased cytoplasmic monoamines → non‑vesicular DA/NE release.
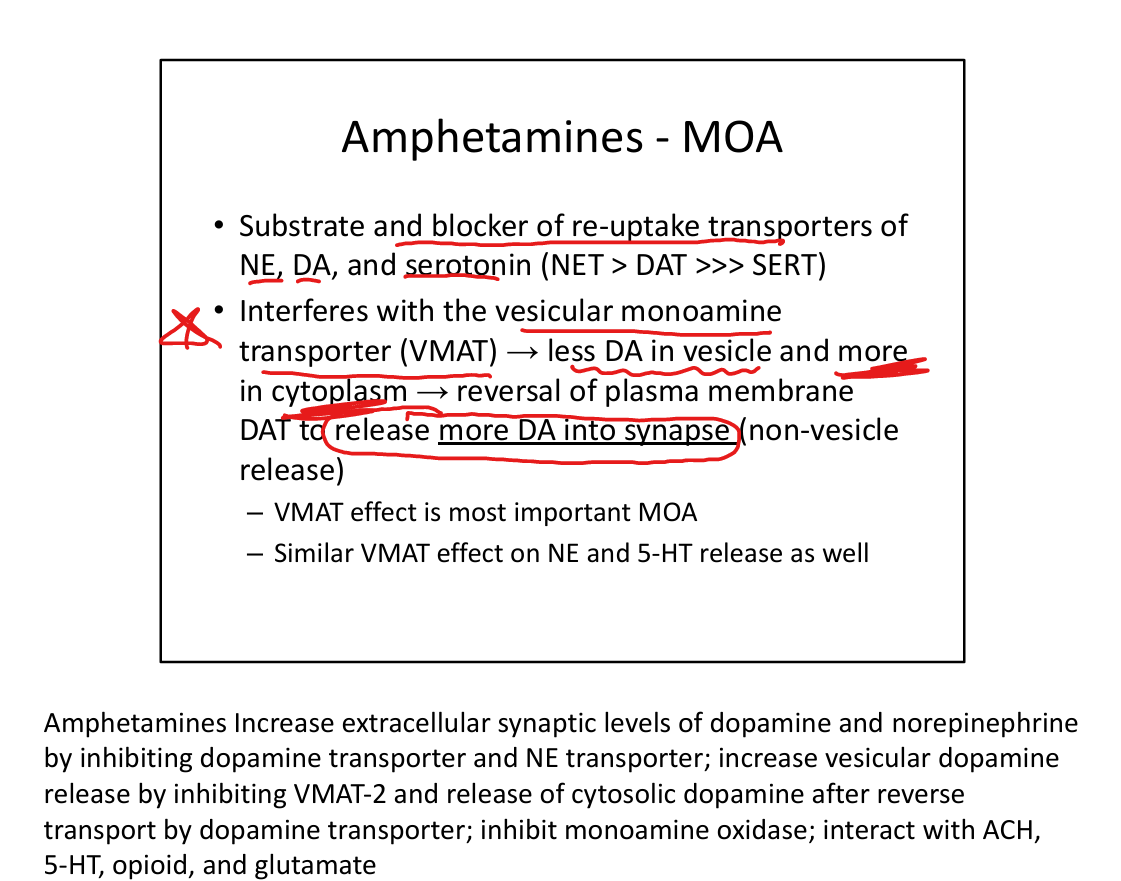
Most important amphetamine MOA
VMAT inhibition → increased cytoplasmic DA.
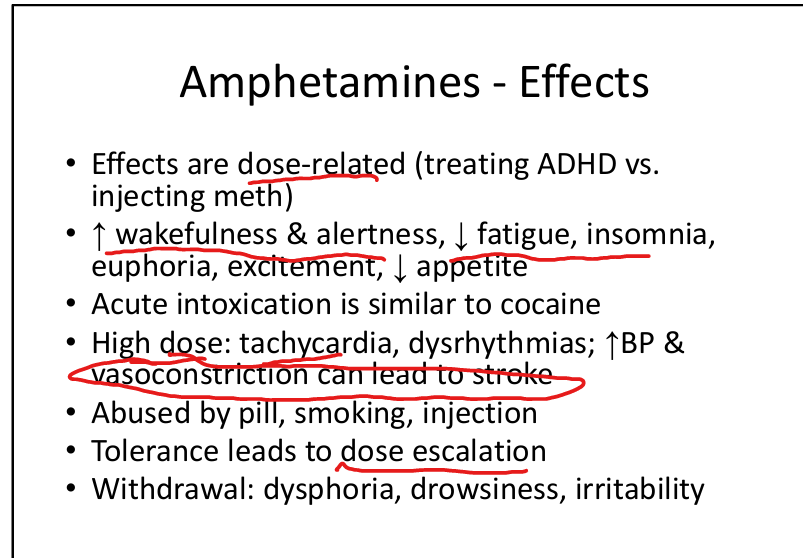
Amphetamine effects
Increased wakefulness, alertness, euphoria, decreased appetite; high doses → tachycardia, arrhythmias, stroke.
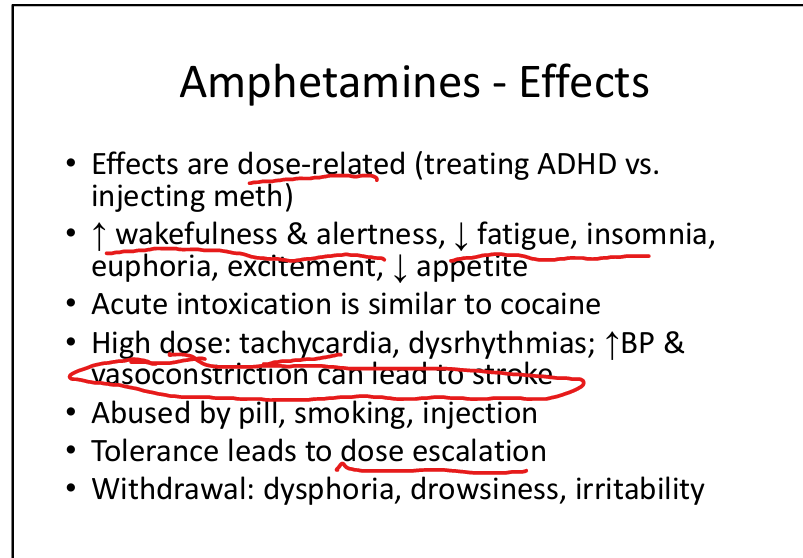
Amphetamine withdrawal
Dysphoria, drowsiness, irritability.
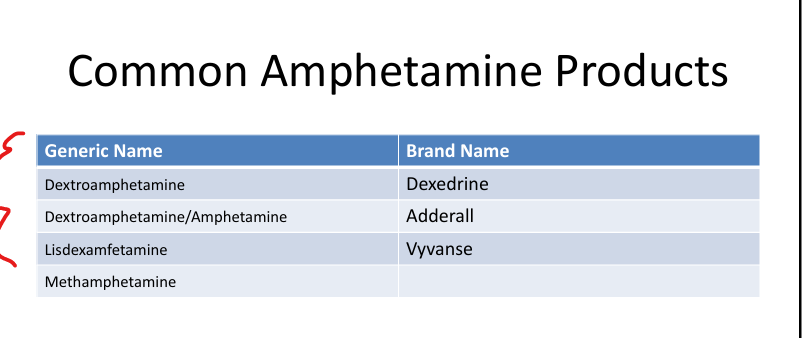
Common amphetamine products
Dextroamphetamine(Dexedrine), Dextroamphetamine/Amphetamine (Adderall), Lisdexamfetamine (Vyvanse), methamphetamine.
Methylphenidate MOA
Blocks reuptake of NE and DA (NET > DAT >> SERT).
Methylphenidate uses
ADHD.
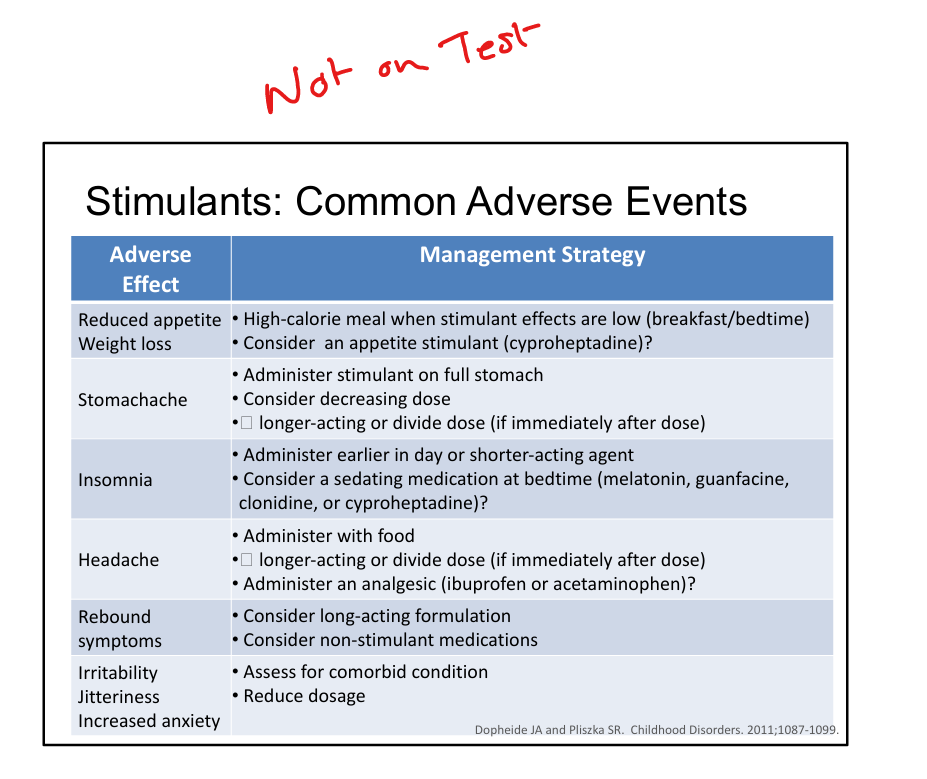
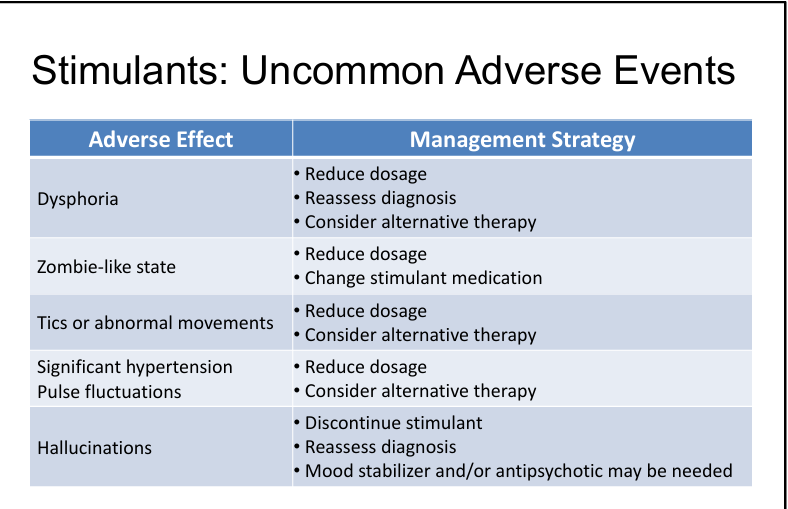
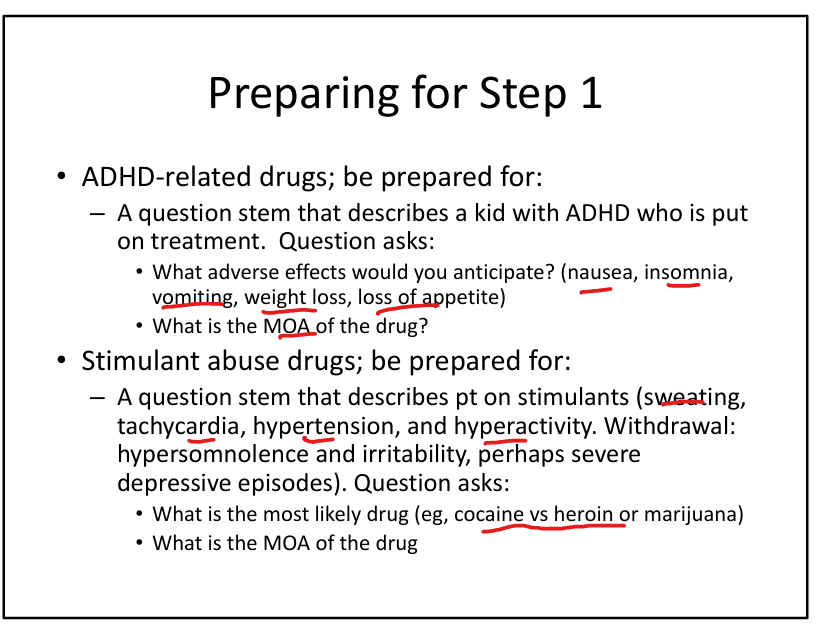
Stimulant common ADEs
Headache, dizziness, reduced appetite, weight loss, insomnia, irritability, increased BP/HR, tics.
Stimulant rare serious ADEs
Priapism, seizures, stroke, MI, sudden cardiac death, mania, hallucinations.
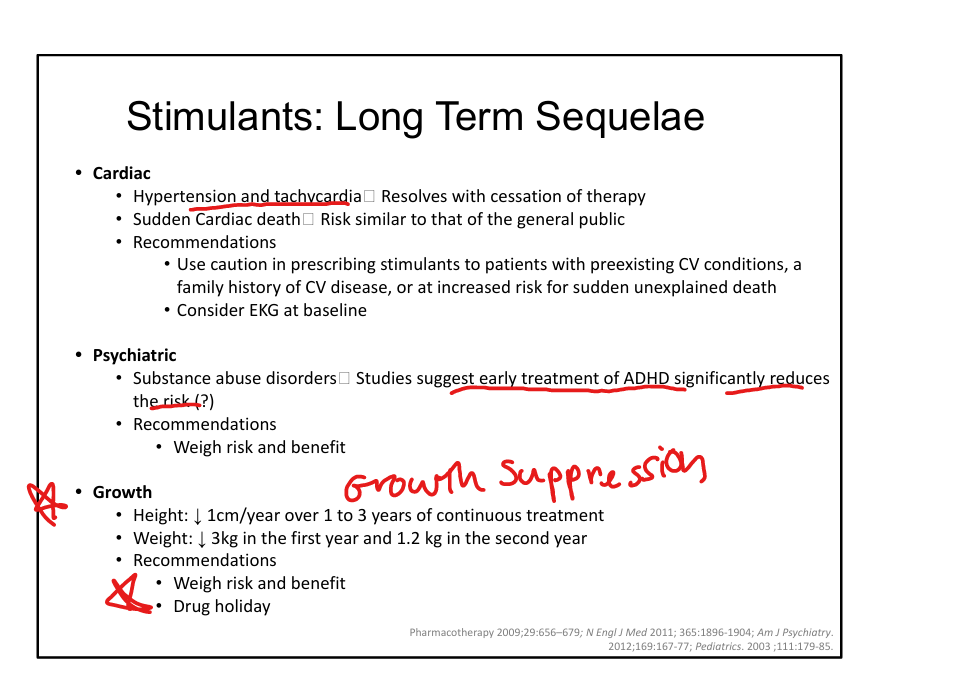
Long‑term stimulant risks
Mild growth suppression, hypertension/tachycardia, rare sudden cardiac death.
MDMA (Ecstasy) MOA
Reverses monoamine reuptake transporters; serotonin >>> NE, DA.
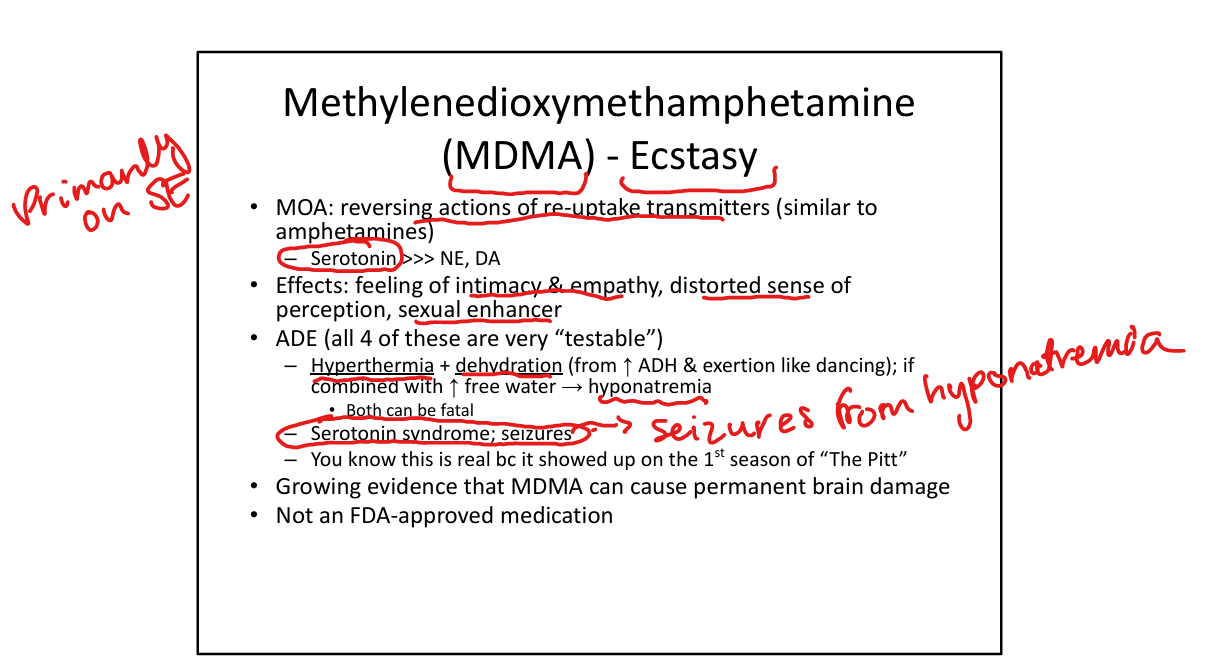
MDMA effects
Intimacy/empathy, sensory distortion, sexual enhancement.
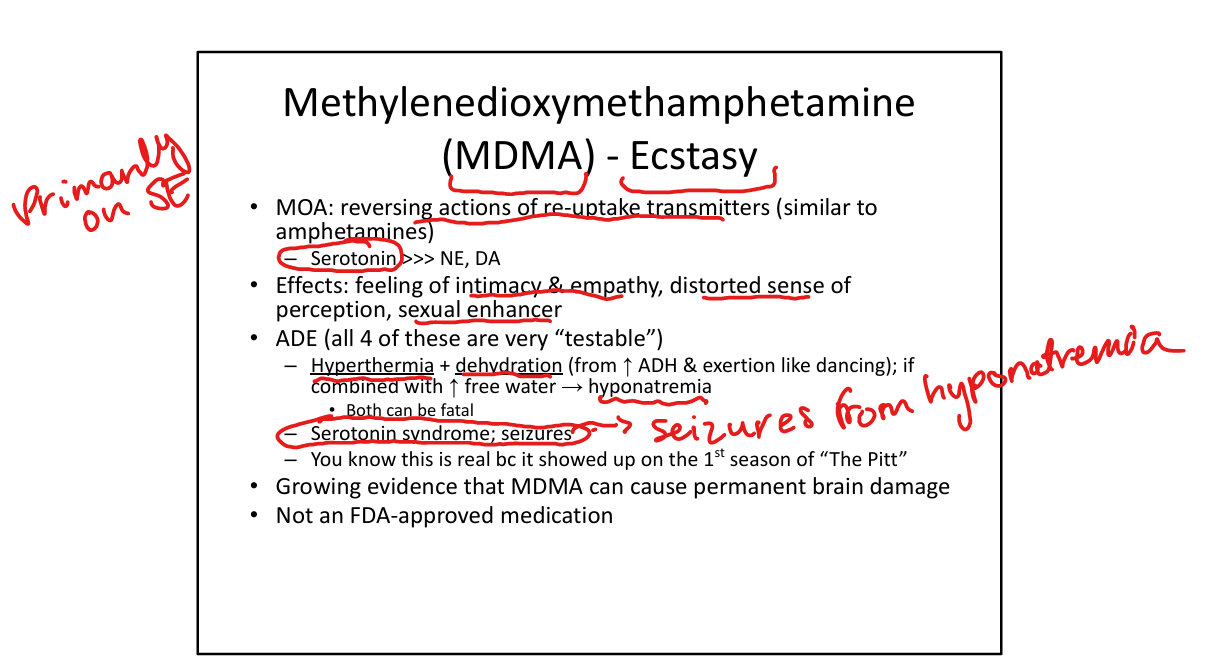
Two lethal MDMA complications
Hyperthermia and hyponatremia(seizures).
Other MDMA risks
Serotonin syndrome, seizures, dehydration; possible long‑term neurotoxicity.
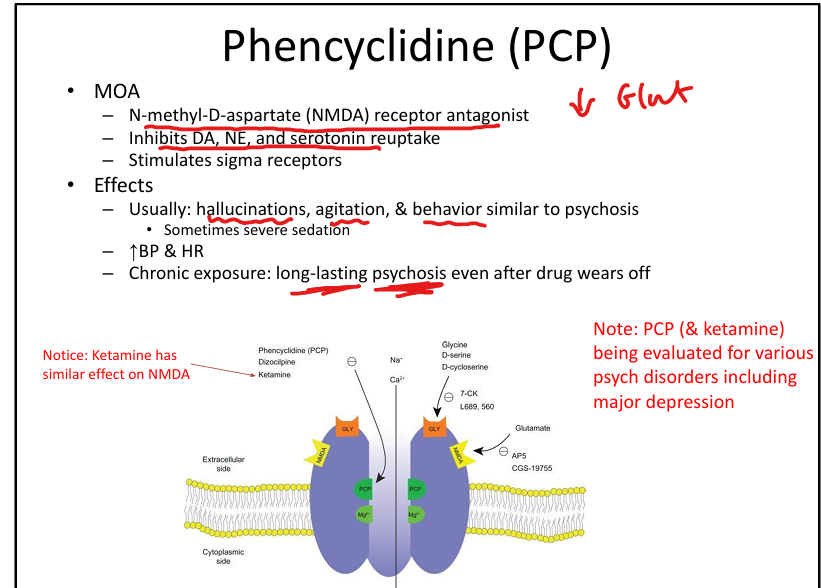
Phencyclidine (PCP) MOA
NMDA receptor antagonist; inhibits DA/NE/5‑HT reuptake; stimulates sigma receptors.
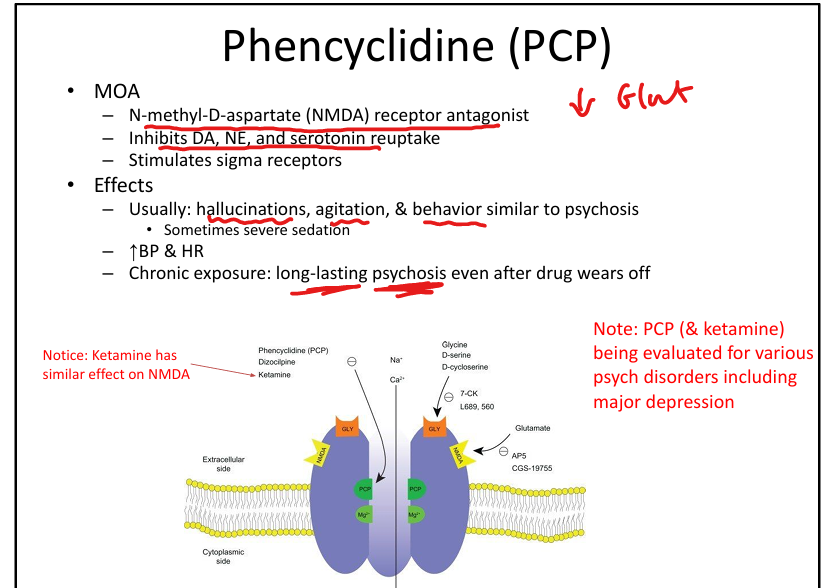
PCP effects
Hallucinations, agitation, psychosis‑like behavior; sometimes severe sedation; increased BP/HR.
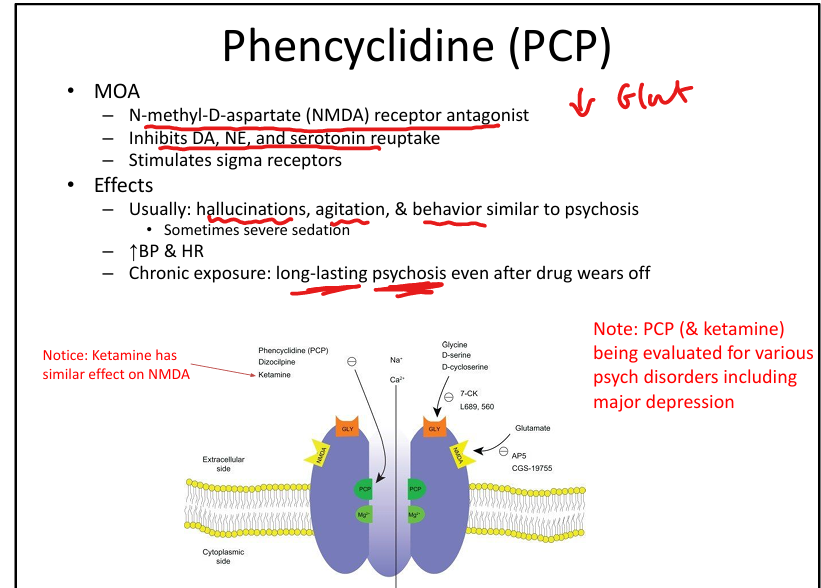
PCP chronic effects
Long‑lasting psychosis even after drug wears off.
Atomoxetine(Strattera) MOA and use
Selective NE reuptake inhibitor. Non stimulant for ADHD, less abuse potential but less effective
Guanfacine MOA, Use, ADEs
Central alpha‑2 agonist. ADHD (extended‑release). ADE: Orthostatic hypotension, fatigue, headache, somnolence, abdominal pain, dry mouth.
Modafinil use, tie?
Narcolepsy + CNS stimulant. Less euphoric and lower abuse potential than amphetamines.
Oxybate salts use + note
Narcolepsy with cataplexy. GHB is oxybate salts in salt form»dangerous
Caffeine class + MOA
Methylxanthine. MOA: Blocks adenosine receptors; inhibits phosphodiesterase → ↑ cAMP/cGMP.
Caffeine Pharmacokinetics
Well absorbed; half‑life ~5 hrs; hepatic metabolism.
Caffeine effects
Increased alertness, mild BP increase, diuresis, headache relief (adjunct), anxiety/insomnia at high doses.
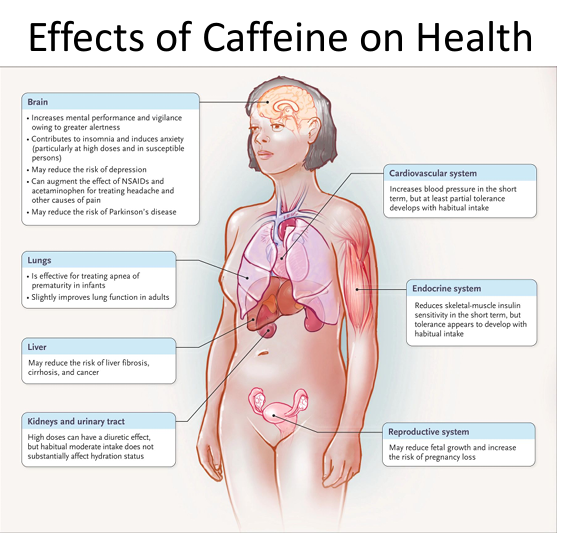
Caffeine medical uses
Apnea of prematurity; adjunct for headaches; wakefulness.
Medical uses of Amphetamines
ADHD, Nacrolepsym Binge eating disorder (Vyvanse)
Step 1 stimulant clues
Sweating, tachycardia, hypertension, hyperactivity → stimulant intoxication; withdrawal → hypersomnolence, irritability, depression.
Step 1 MDMA clue
Party/dancing → hyperthermia + hyponatremia.