ANP1115 Midterm 2 Flashcards
1/338
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
339 Terms
Two main immune defenses
Innate immunity (non-specific), and adaptive immunity (specific/acquired)
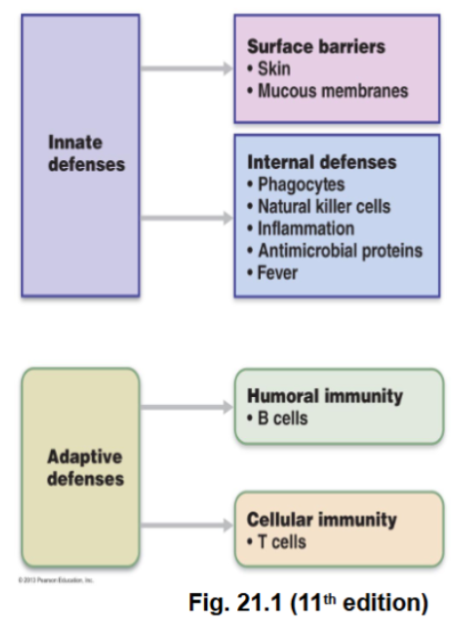
Innate immunity
The non-specific immune defence.
Protects without recognizing a specific pathogen. Instead, it recognizes general molecular patterns on microbes (carbohydrates/lipids on cell surfaces).
It’s present at birth, is a rapid response, has no immunological memory, main response every time.
The main components are surface barriers (think skin, mucus membranes), and internal defences. (Think phagocytes, natural killer cells, inflammation, antimicrobial proteins and fever.)
Activated by PAMPs (Pathogen-associated molecular patterns), and DAMPs (damage-associated molecular patterns)
PAMPs and DAMPs alert the innate immune system that something is wrong, and don’t require identification of a specific microorganism.
Adaptive immunity:
The specific/acquired immunity.
Defined as an immune response carried out by lymphocytes that recognize specific antigens.
The key features of this type of immunity are that it’s highly specific, has memory, and develops after exposure to antigens.
There are 2 major types:
Humoral immunity: Mediated by B cells and produces antibodies.
Cell-Mediated Immunity: Mediated by T cells, destroys infected or abnormal cells.
Macrophages are a key player in this too. They attack antigen-presentin cells.
PAMPs (Pathogen-Associated Molecular Patterns)
Molecules found on microorganisms but not normally in the body
Eg: Bacterial cell wall molecules
Recognized by Toll-like receptors (TLRs) on phagocytes
Effects
Trigger phagocytosis
Trigger inflammatory response
Notify adaptive immune system
DAMPs (Damage-Associated Molecular Patterns)
Defined as molecules located in the wrong place in the body
Example: DNA outside the nucleus or cell
They signal tissue damage even if no infection is present
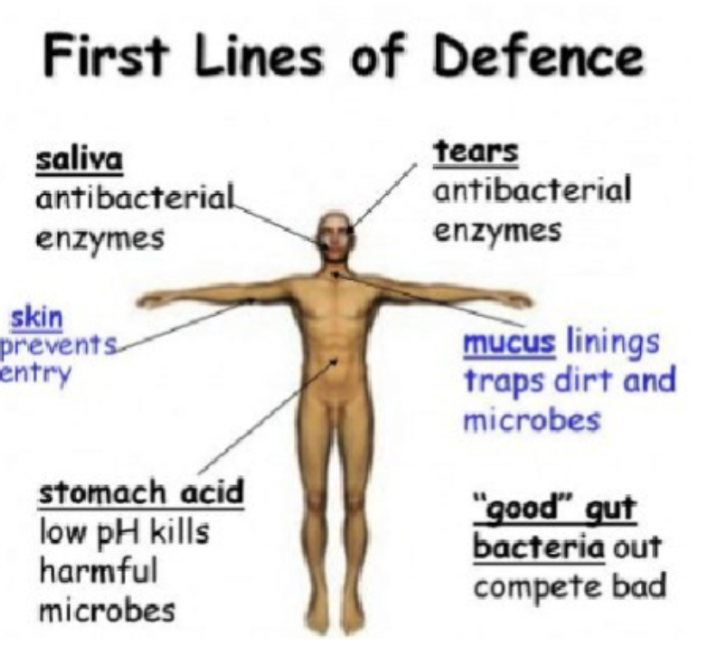
Innate Defenses
These are the “surface barriers”. They are effective, but can be breached.
Acid
Skin acidity
Vaginal secretions
Stomach acid
Enzymes
Lysozyme (an antimicrobial enzyme) in:
Saliva
Respiratory mucus
Tears
Protein-digesting enzymes in stomach
Mucus
Traps microorganisms in respiratory and digestive tracts
Defensins
Antimicrobial peptides secreted by skin and mucous membranes
Other Chemicals
Lipids in sebum
Dermicidin in sweat
Toxic to bacteria
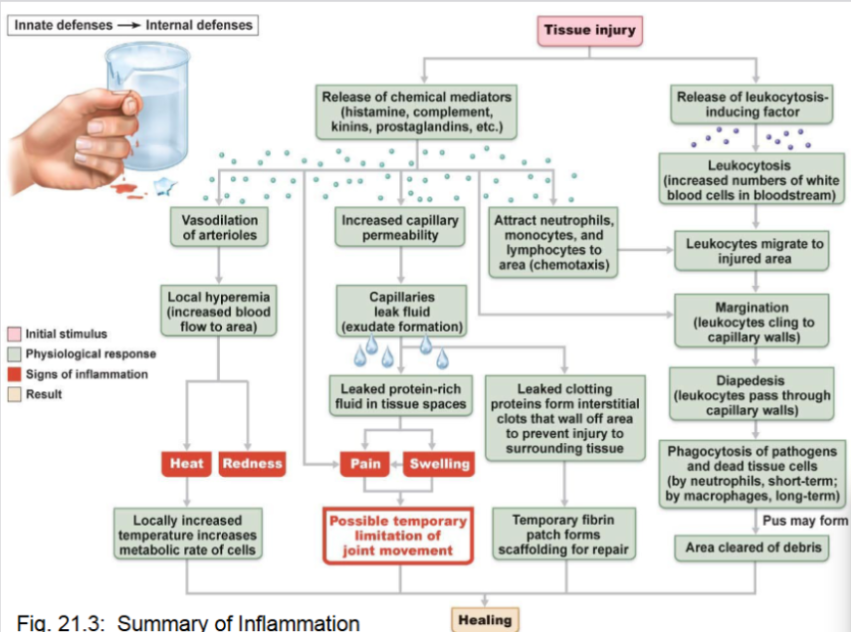
Inflammation
A response to tissue injury or infection.
The four key signs of inflammation are redness, heat, swelling & pain.
Functions:
Preventing spread of microorganisms
Removing pathogens and cell debris
Initiating tissue repair
Alerting the adaptive immune system
Inflammatory chemicals (eg: histamine, kinins, prostaglandins, and complement proteins) are released by injured cells and immune cells and cause vasodilation, increased capillary permeability, and attraction of immune cells.
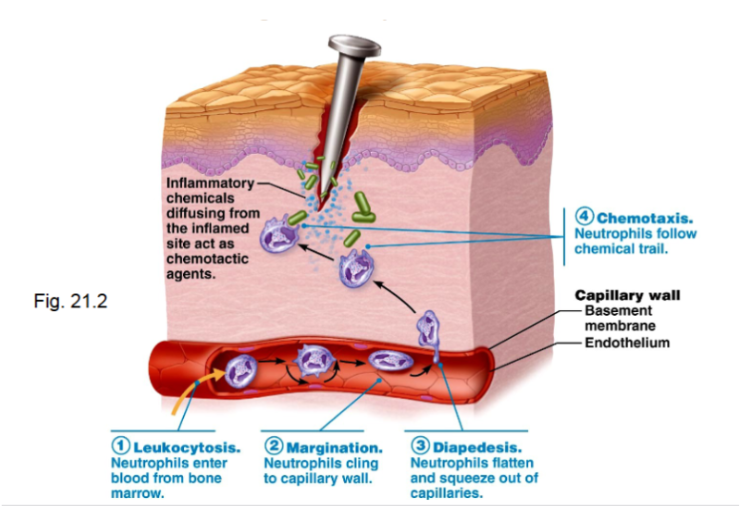
Leukocyte Response During Inflammation
Leukocytosis
Increase in circulating white blood cells
Margination
Leukocytes adhere to capillary walls
Diapedesis
Leukocytes squeeze through capillary walls
Chemotaxis
Leukocytes follow chemical signals to the injury site
Inflammatory Process Summary
Tissue injury occurs
Chemical mediators released
Vasodilation increases blood flow
Capillary permeability increases
Protein-rich fluid leaks into tissues
Immune cells migrate to site
Phagocytosis of pathogens
Debris cleared
Healing begins
Interferons
An antimicrobial protein released by virus-infected cells.
Effects:
Diffuses to nearby cells
Blocks viral protein synthesis
Degrades viral RNA
It also activates macrophages, mobilizes natural killer cells and may have anti-cancer effects.
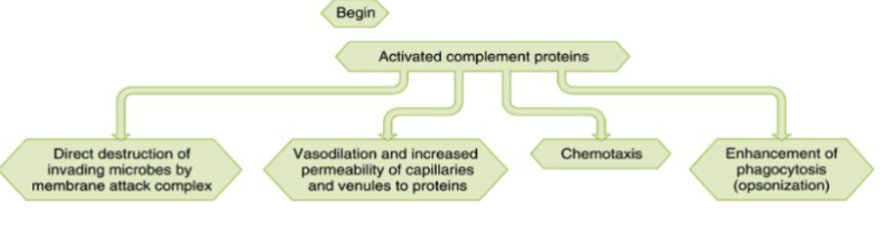
Complement system
A group of approx 20 plasma proteins circulating in inactive form
When activated, they enhance inflammation and pathogen destruction
The major effects of this system are:
Direct destruction of microbes via membrane attack complex (MAC)
Basodilation & increased permeability
Chemotaxis which attracts immune cells
Oopsonization (coating pathogens to enhance phagocytosis)
Complement Pathways
Classical pathway
Triggered by antibodies
Lectin pathway
Activated by lectins binding sugars on microbes
Alternative pathway
Activated spontaneously on microbial surfaces
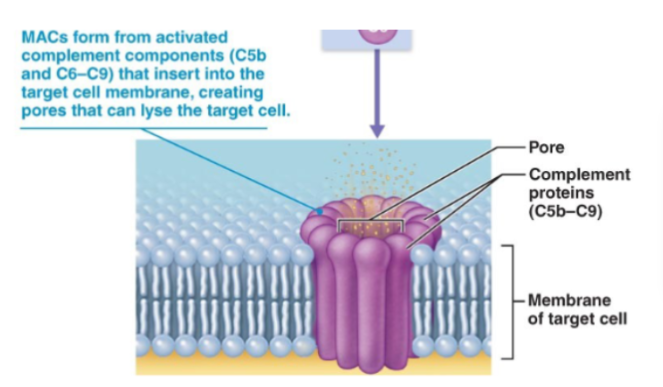
Membrane Attack Complex (MAC)
Formed by complement proteins C5b–C9
It inserts into the pathogen membrane, then creates pores which causes cell lysis
Fever
Defined as an elevated body temperature caused by resetting of the hypothalamic thermostat
It’s caused by pyrogens released by leukocytes and macrophages exposed to pathogens
The benefits are that it increases metabolic rate and causes the liver and spleen to sequester (isolate) iron and zinc, which limits microbial growth.
Natural Killer (NK) Cells
A type of lymphocyte in the innate immune system. It’s not antigen-specific
It targets virus-infected and cancer cells.
The mechanism of detection:
Note that all normal cells express MHC I proteins.
NK cells attack when MHC I is missing or reduced, or if stress markers are present.
Many infected or cancer cells reduce MHC I expression, triggering NK.
NK cells can express toll-like receptors and respond to PAMPs or DAMPs
Lymphocytes
Derived from hemocytoblasts in red bone marrow
All of them start identical, then become B cells (mature in bone marrow) or T cells (mature in thymus).
During maturation, they develop immunocompetence and self-tolerance.
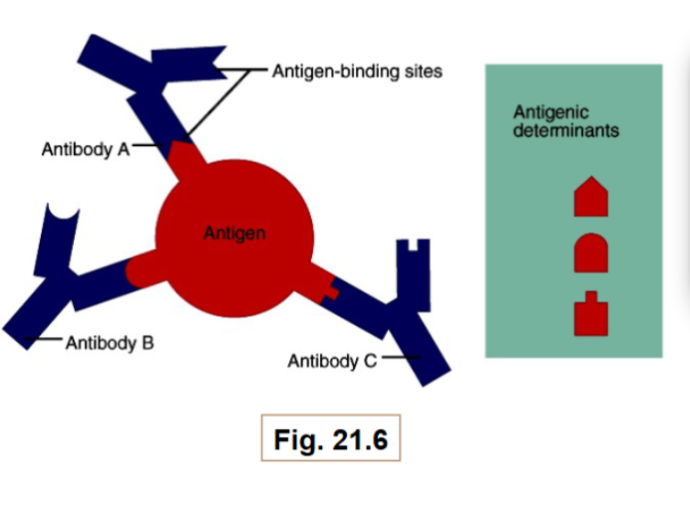
Antigen
A substance capable of mobilizing adaptive immune responses
They may have multiple antigenic determinants (epitopes)
Major histocompatibility complex (MHC)
Refers to cell surface glycoproteins which mark cells as “self”, and present antigens to T cells.
Each MHC molecule contains a groove where a self-antigen or foreign antigen can bind
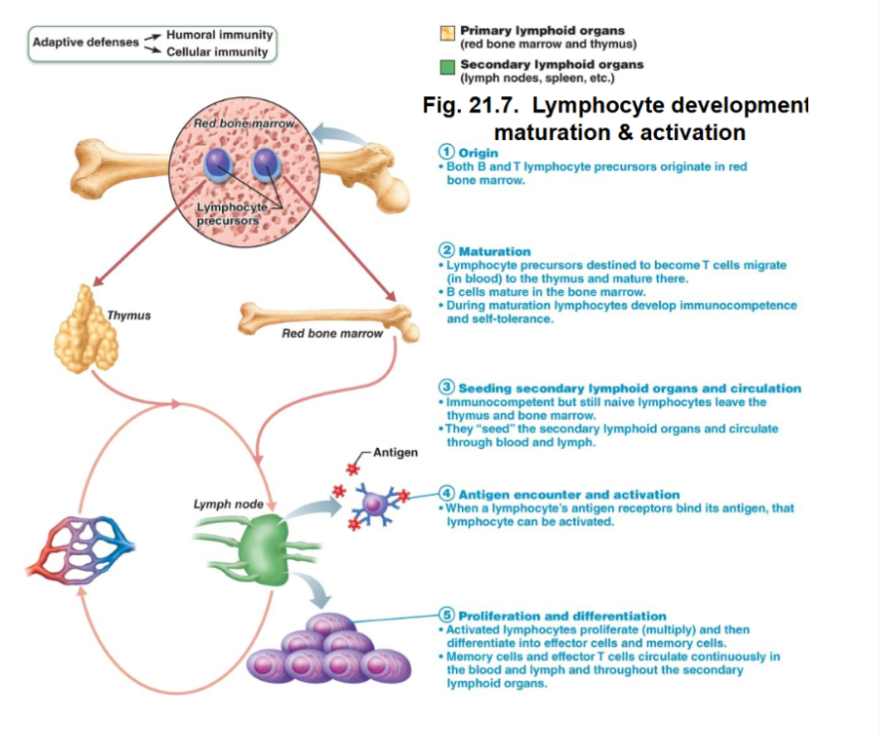
Lymphocyte development
1. Origin
Both B and T lymphocyte precursors originate in bone marrow
2. Maturation
T cells migrate to the thymus to mature, and B cells mature in bone marrow
During maturation, they acquire immunocompetence (recognizing and defending) and self-tolerance.
3. Seeding secondary lymphoid organs
Naive lymphocytes migrate to lymph nodes, spleen and other lymphoid tissues
4. Antigen encounter
When lymphocyte receptors bind their specific antigen, they become activated
5. Proliferation and differentiation
Activated lymphocytes proliferate (clonal expansion), then differentiate into effector cells or memory cells.
Memory cells provide long-term immunity.
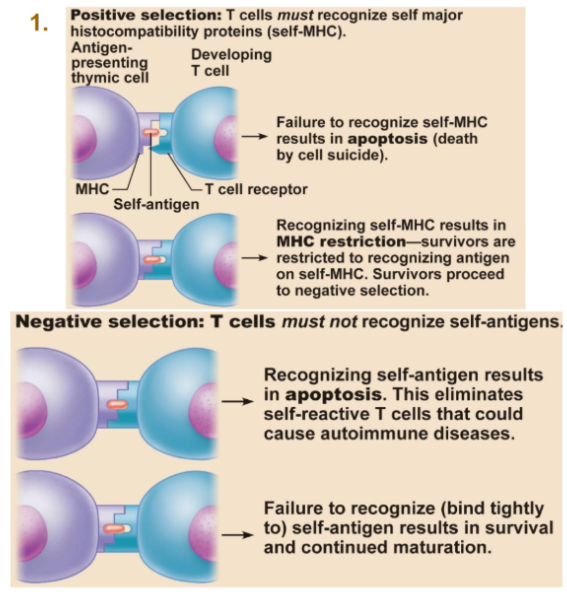
T cell education in the thymus
As we know, T-cells imgrate tot he thymus where they undergo maturation.
Positive selection:
T cells must recognize self-MHC; if it doesn’t, apoptosis occurs.
Successful cells survive but are restricted to recognizing antigen on self-MHC.
Negative selection:
T cells must not recognize self-antigens strongly. If they do, they undergo apoptosis to prevent autoimmune diseases.
B Cell Maturation
The immature B cells mature in bone marrow. The self-reactive ones are eliminated.
After maturation, B cells express unique antigen receptors, and each B cell responds only to one antigen.
Lymphocytes become immunocompetent before encountering antigens.
Humoral immune response
Occurs when B lymphocytes respond to an antigen.
Antigen challenge usually occurs in lymph nodes or the spleen
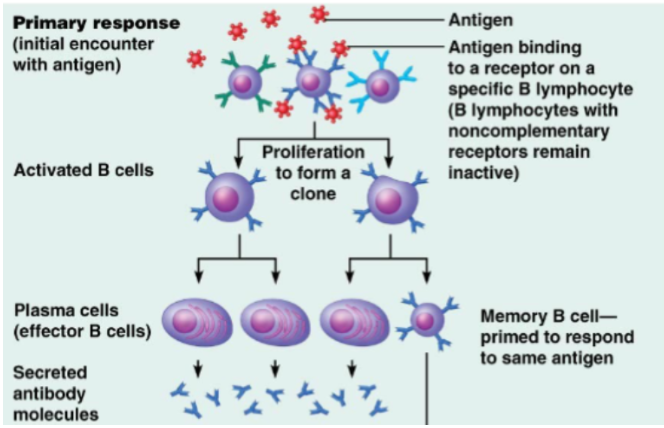
Activation of B cells
Antigen binds to the receptor on a specific B lymphocyte
Only the B cell with the complementary receptor becomes activated
The activated B cell proliferates (clonal expansion) which produces a clone of identical cells.
After proliferation, B cells differentiate into two main types of cells. Plasma cells (effector B cells) and memory B cells.
Plasma cells
Also known as effector B cells
A type of B cell
Their function is to procude large amount of antibodies
They typically survive 4-5 days
The antibodies circulate in body fluids, they bind antigens and mark pathogens for destruction.
Memory B cells
A type of B cell
Their function is to provide long-term immunity.
They don’t immediately produce antibodies
Remain in the body for years
Can respond rapidly upon future exposure to the same antigen
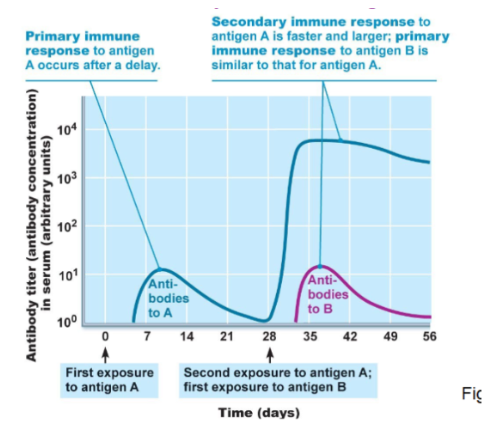
Primary immune response
Occurs during the first encounter with an antigen
A slower response
Produces less antibodies
Antigen binds to B-cell receptor
B cells proliferate
Plasma cells produce antibodies
Memory B cells are formed
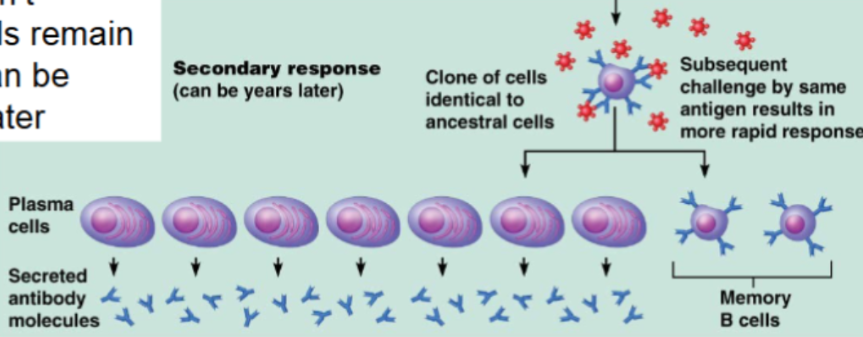
Secondary immune response
Occurs during later exposure to the same antigen
It’s much faster
Produces more antibodies
Memory B cells rapidly become plasma cells
Macrophages
A type of white blood cell
They engulf athogens
Present antigen fragments to T cells
Help activate adaptive immune responses
Humoral Immunity
The immunity that has to do with B cells
The antigen binds to B-cell receptor
Helper T cell sends chemical signalsB cell diffrenaites into lpasma cells
Plasma cells release antibodies
Mechanisms of Antibody Action
Note: Antibodies don’t directly kill pathogens, rather they tag them so other immune mechanisms can destroy them.
1. Neutrization
Antiboides bind dangerous parts of pathogens, which prevents viruses or toxins from entering cells
2. Agglutination
Antibodeis bind multiple pathogens, causing them to clum together.
This is easier for phagocytes to remove
3. Precipitation
Antibodies bind double antigens, which forms complexes that settle out of solution.
4. Complement activation
Antibodies activate compliment proteins which cause inflammation, phagocytosis and cell lysis.
Immunoglobulin classes (antibodies)
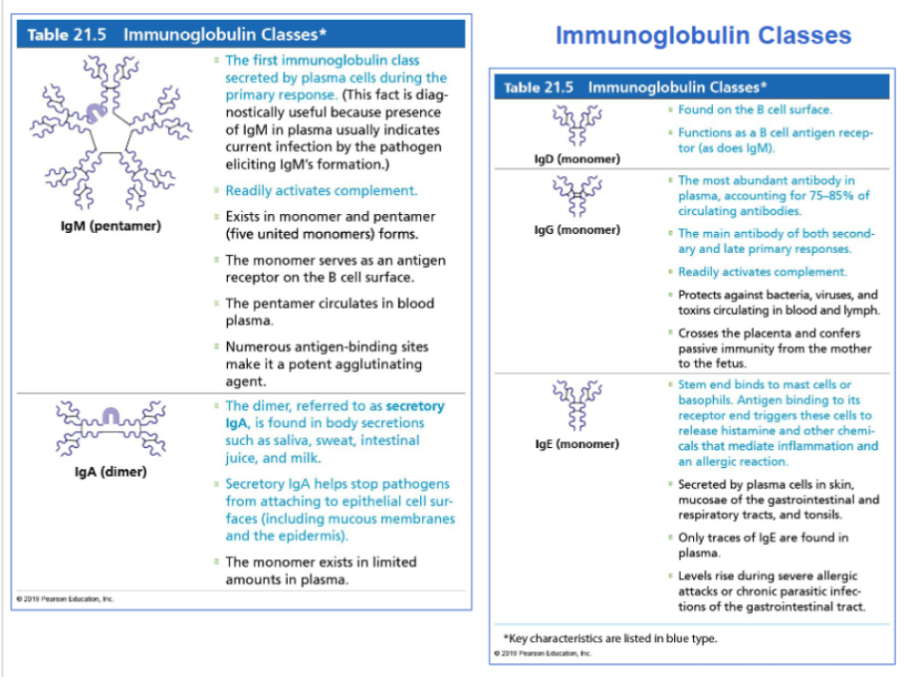
IgM
The first antibody produced during primary response
Indicates current infection
Strong activator of complement
Exists as pentamer in plasma

IgG
Most abundant antibody in blood (75–85%)
Major antibody in secondary immune response
Activates complement
Crosses placenta which provides fetal immunity

IgA
Found in body secretions:
Saliva
Sweat
Intestinal fluid
Milk
Protects mucosal surfaces

IgE
Binds to mast cells and basophils
Triggers histamine release
Important in:
Allergic reactions
Parasitic infections

IgD
Found on B-cell surfaces
They function as B-cell antigen receptors

Vaccine mechanisms
They work by triggering a primary immune response without causing disease
This creates memory B and T cells
Upon a later exposure to the pathogen, it causes a rapid secondary immune response
Active immunity
A type of immunity where the body produces it’s own antibodies
It can either be naturally acquired (via infection with pathogen), or artificially acquired (via vaccination)
Only active immunity produces immunological memory.
Passive immunity
A type of immunity where antibodies come from another source
They can be naturally acquired from the mother (fetus gets antibodies through the placenta, or infant through milk) or artifically acquired via injection of antibodies (gamma globulin)
It provides immediate protection, but holds no memory.
T cells
A type of cell that destroys infected or abnormal body cells
Targeted cells include virus-infected cells, cancer cells, transplanted tissues, and cells with intracellular bacteria.
These cells recognize antigen fragments presented on MHC molecules
Types are:
Cytotoxic T Cells (CD8) (the killers)
Helper T cells (CD4) (coordinate adaptive immune response)
Regulatory T Cells (suppress or stop immune responses)
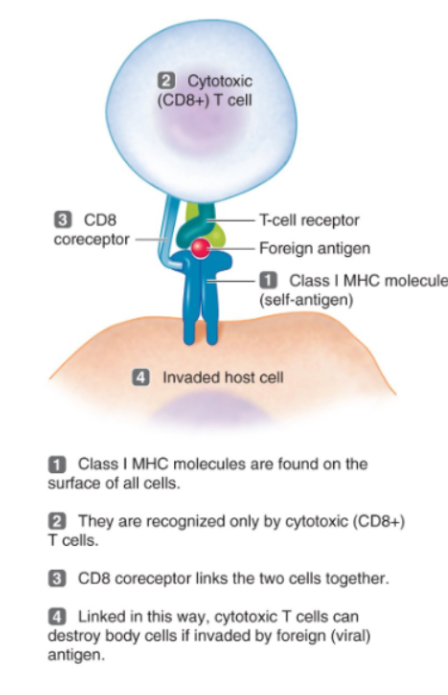
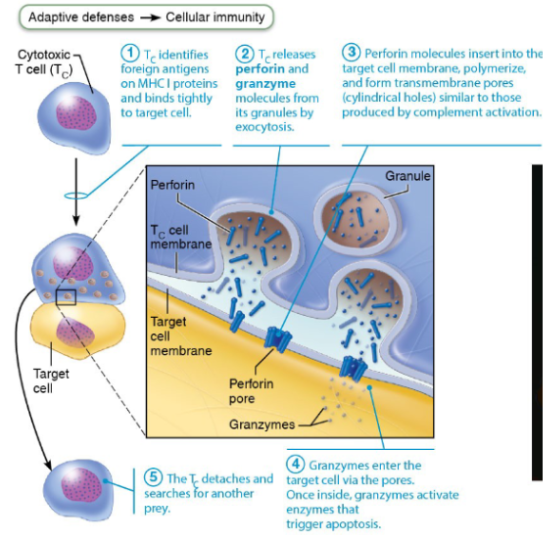
Cytotoxic T Cells (CD8)
The killer T cells.
They destroy infected or abnormal cells
Mechanism of killing:
Release perforin
Release granzymes
Cause apoptosis (cell death)
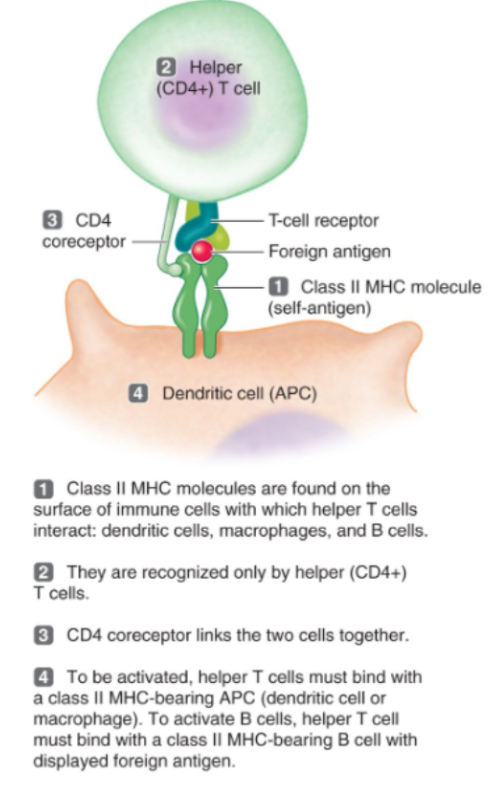
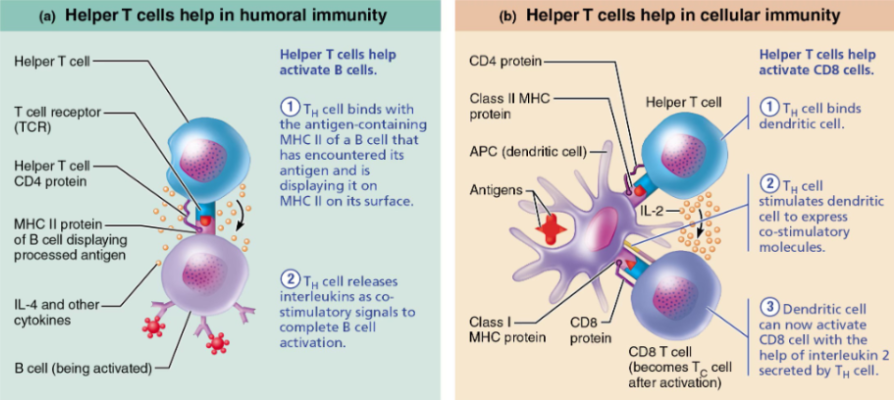
Helper T Cells (CD4)
Most common T cells.
They activate B cells
Activate cytotoxic T cells
Activate macrophages
Release cytokines (ex: IL-2)
They basically coordinate the entire adaptive immune response./
Regulatory T Cells
They suppress or stop immune responses
They do this to prevent excessive immune activity
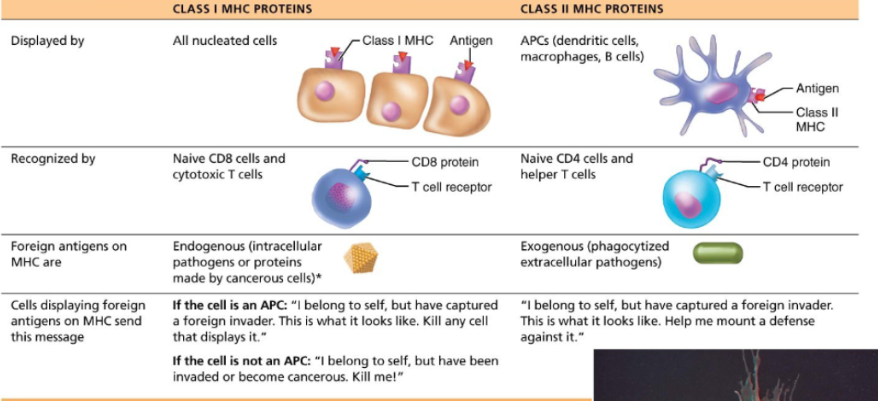
MHC Class I proteins
These proteins are found on all nucleated cells.
They are recognized by CD8 cytotoxic T cells
These proteins display internal (endogenous) antigens… So viral and cancer proteins.
The signal sent is basically “I belong to self, have been infected. Destroy me.”
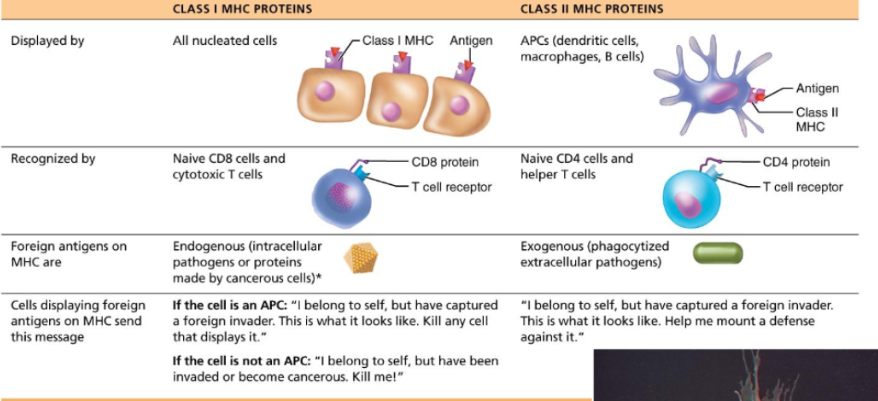
MHC Class II proteins
These proteins are found on antigen-presenting cells. Think macrophages, dendritic cells and B cells.
They are recognized by CD4 helper T cells.
They display external (exogenous) antigens.
The signal sent is basically “I captured a pathogen. Activate immune response”
Macrophages (antigen-presenting cells)
They are derived from monocytes from bone marrow
Functions are:
Phagocytosis (engulfing pathogens)
Antigen presentation (displaying antigen fragments to T-cells)
Immune activation (releasing signalling proteins, activating T cells)
Note: Activated T cells then stimulate macrophages, which creates a feedback loop.
Mechanism of Helper T Cell Mechanism
Antigen presentation
Dendritic cell presents antigen on MHC II
Double recognition
T-cell receptor binds antigen
CD4 binds MHC
Costimulation
Additional receptor interactions occur
Clonal expansion
Helper T cells proliferate
Formation of:
Effector T cells
Memory T cells
Cytotoxic T Cell Killing Mechanism
Cytotoxic T cell recognizes antigen on MHC I
Releases perforin
Perforin creates pores in target cell membrane
Granzymes enter the cell
Trigger apoptosis
T cell detaches and attacks another cell/
Lines of immune defence
First line of defence: (Surface barriers):
Skin
Mucous membranes
Enzymes in saliva and tears
Stomach acid
Mucus
Second line of defence (Innate internal defences):
Phagocytes
Natural killer cells
Inflammation
Complement
Interferons
Fever
Third Line of Defence (adaptive immunity)
This line of defence provides specific, long-term protection
Components are B cells (antibodies), T cells and memory cells
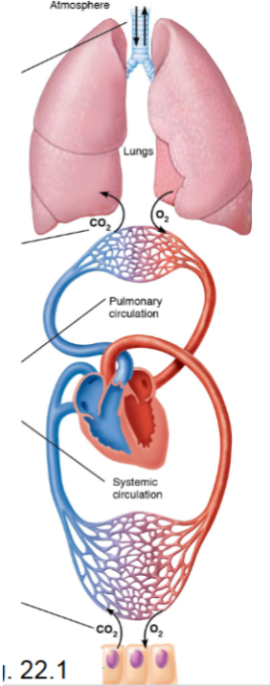
Four processes of respiration
Pulmonary ventilation
Movement of air into and out of lungs
External respiration
Exchange of gases between air in alveoli and blood
Transport of respiratory gases
Blood transports O₂ and CO₂ between lungs and tissues
Internal respiration
Exchange of gases between blood and tissue cells
Note that the respiratory system performs ventilation and external respiration, while the cardiovascular system handles transport and internal respiration
Conducting Zone
Provides a passageway for air
Filters, warms and humidifies incoming air
No gas exchange occurs here
Structures include:
Nose
Nasal cavity
Pharynx
Larynx
Trachea
Bronchi
Bronchioles
Terminal bronchioles
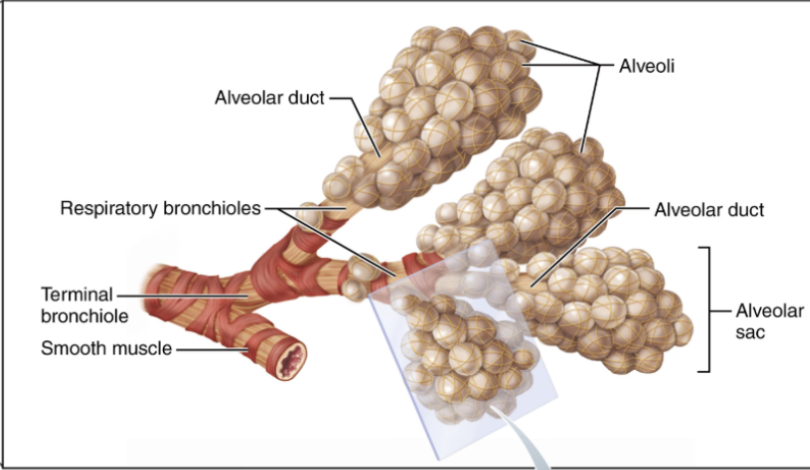
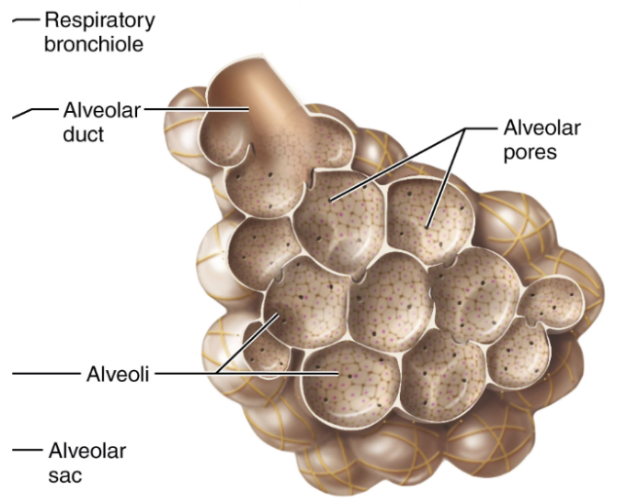
Respiratory Zone
The sites of gas exchange in the body
Structures include:
Respiratory bronchioles
Alveolar ducts
Alveoli
Gas exchange occurs via diffusion across the respiratory membrane.
The nose
A facial organ
Provides an airway for respiration
Warms and moistens the air
Filters air
Is a resonating chamber for speech
Contains olfactory receptors for smell
It has a rich blood supply (thin veins beneath epithelium), which makes nosebleeds common
Has sensory nerves, hence why infants have a sneeze reflex
Cold air slows cilia movement, leading to runny nose
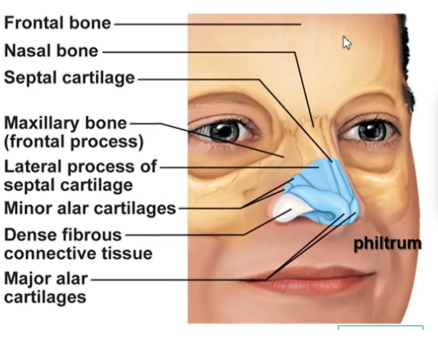
External nose structure
The shape of the nose is determined by nasal cartilages
The skin covering the nose contains many sebaceous glands
Important structures include the nasal bone, septal cartilage, major and minor alar cartilages
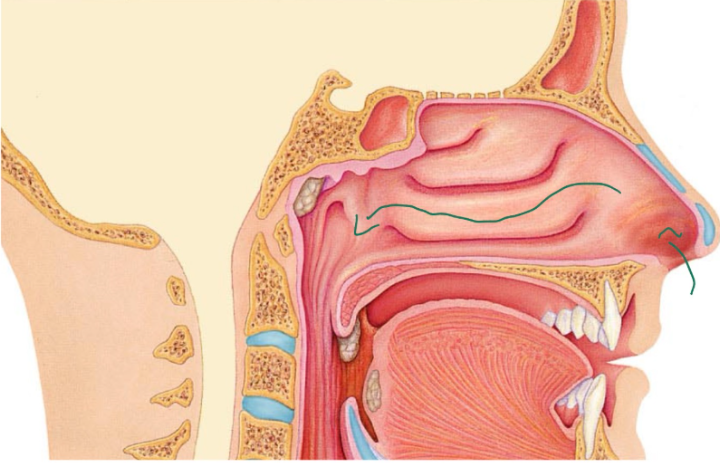
Air entering the nasal cavity
Air enters from the external nares (nostrils) to the nasal cavity, internal nares, and then nasopharynx. It’s divided by the nasal septum, which is made up of cartilage and bone.
Olfactory mucosa
A type of nasal mucosa
It contains receptors for smell
Respiratory Mucosa
A type of nasal mucosa
Structure is pseudostratified ciliated columnar epithelium and goblet cells, which produce mucus.
Function is trapping dust and microbes via the mucus, and cilia moves mucus towards the pharynx.
Mucus contains lysozyme, which is an antibacterial enzyme
Vibrissae
Refers to the coarse hairs inside the nostrils
They trap large particles
Nasal Conchae
There are 3 pairs. Superior, middle and inferior.
They increase surface area, create air turbulence and improve warming, humidifying, and filtering of air.
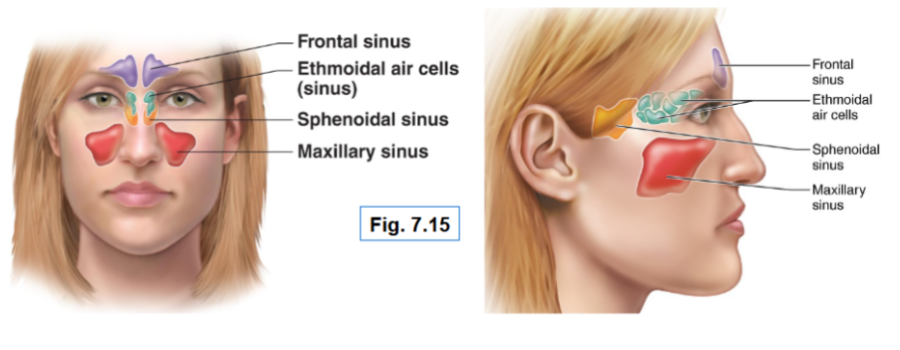
Paranasal sinuses
They are located in the bones surrounding the nasal cavity
Frontal
Sphenoid
Ethmoid
Maxillary
Their function is to lighten the skull, produce mucus and help warm and moisten air
Sinus headache occurs from sinus drainage pathways being blocked, which causes air in the sinuses to be absorbed and create a partial vacuum, causing pressure & pain.
Pharynx
A common pathway for air and food
Its walls are composed of skeletal muscle, it’s approx 13 cm long.
There are 3 regions to this:
Nasopharynx
Oropharynx
Laryngopharynx
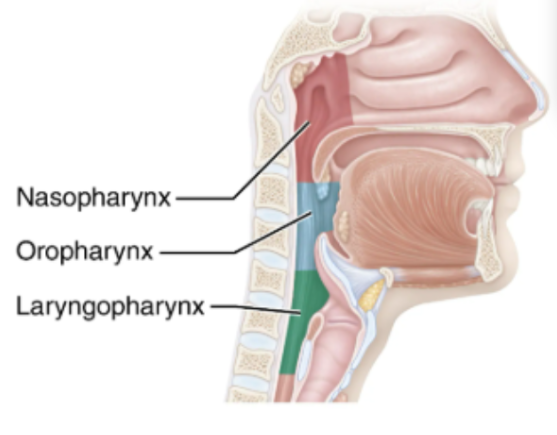
Nasopharynx
Located below the sphenoid bone and above the soft palate
Allows for air passage only
It’s structure is pseudostratified ciliated columnar epithelium
Contains pharyngleal tonsil and pharyngotympanic (auditory) tubes, which drain into the middle ear.
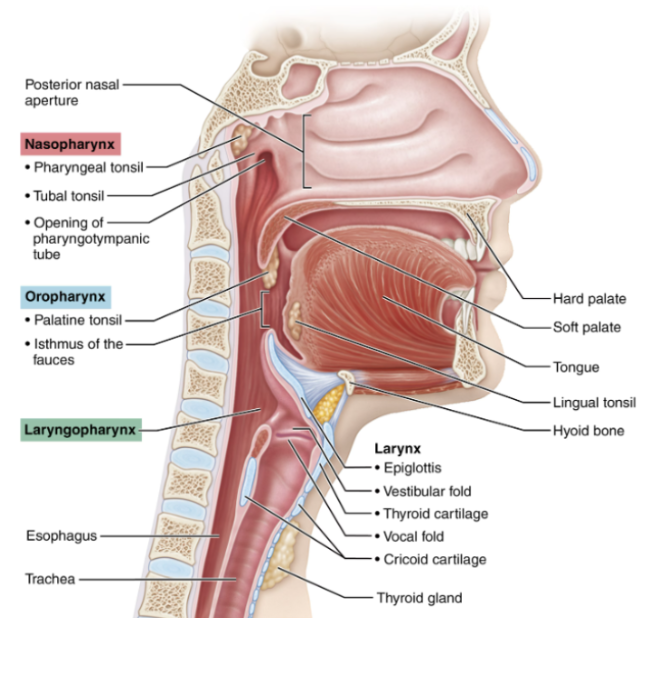
Oropharynx
Extends from the soft palate to epiglottis
Connected to the mouth via the isthmus of the fauces
Provides a passageway for air and food
Has stratified squamous epithelium, which protects against abrasion
Structures include the palatine tonsils and lingual tonsils.
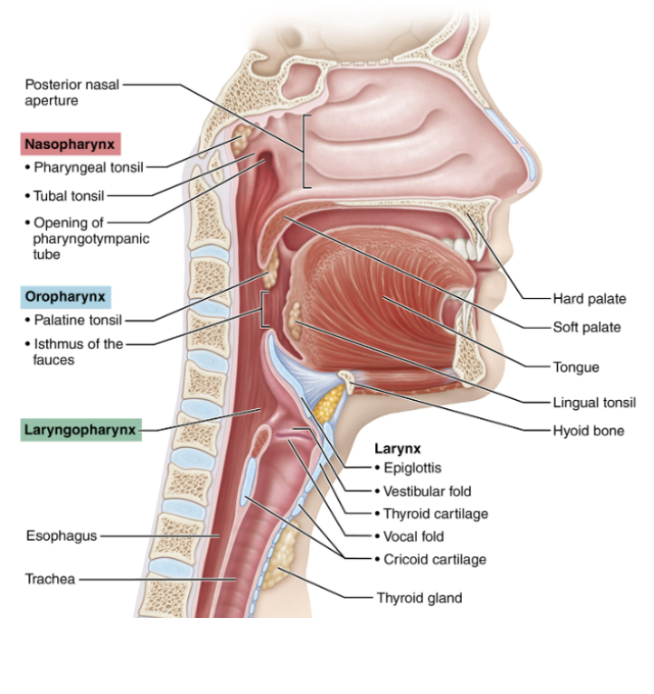
Laryngopharynx
Extends from the epiglottis to the larynx
Provides a passageway for air and food
Has stratified squamous epithelium
During swallowing, it directs food into the esophagus
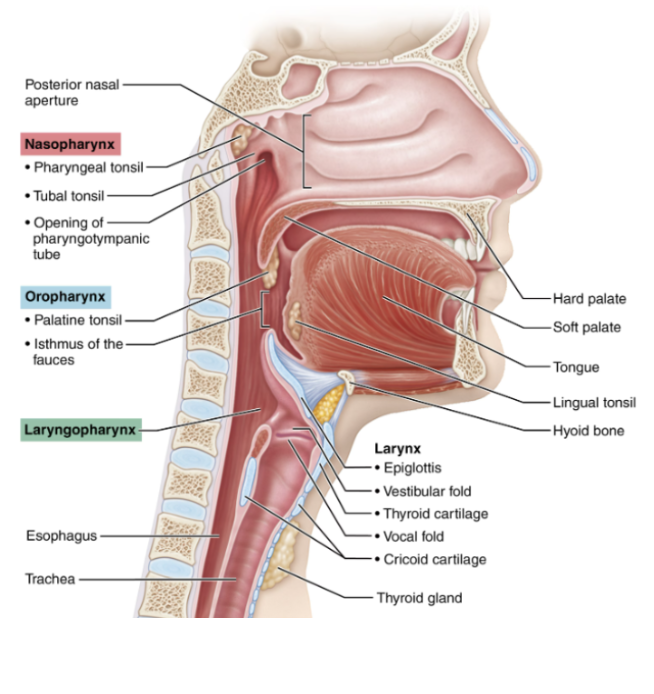
Larynx
The voice box
Located between the pharynx and trachea. It’s roughly 5cm long
It’s attached to the hyoid bone
Functions are to maintain an open airway, switching pathway between air and food, and producing voice
In laryngitis, the vocal cords are inflamed, which prevents normal vibration causing hoarseness
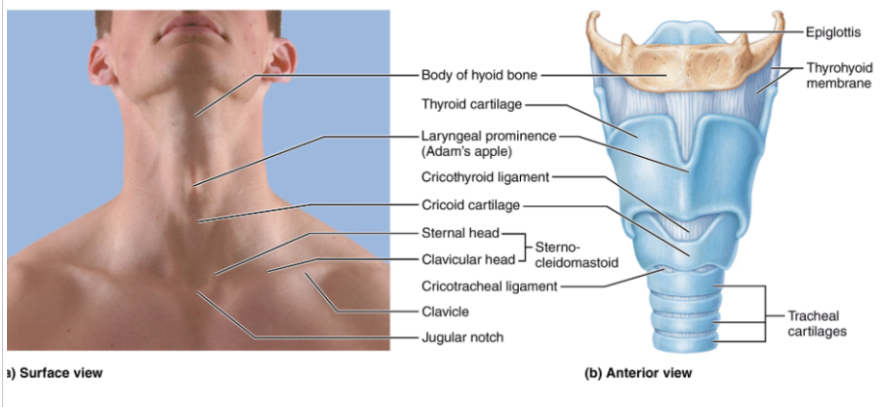
Laryngeal cartilages
There are a total of 9
Thyroid cartilage:
A large shield-shaped cartilage. It forms the Adam’s apple
Cricoid cartilage:
Located below the thyroid cartilage
Arytenoid cartilages:
Anchor vocal cords
Epiglottis:
An elastic cartilage that covers the airway during swallowing.
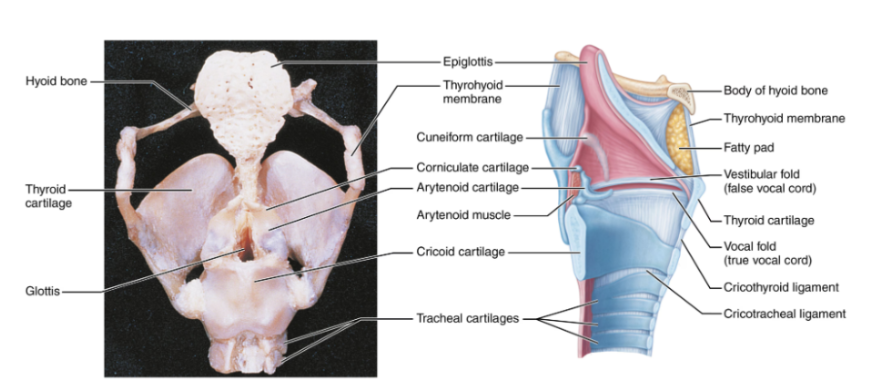
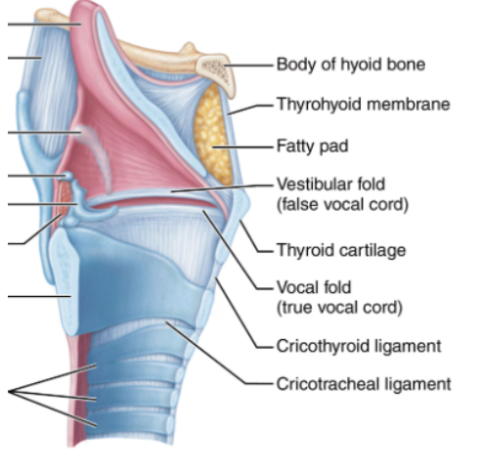
Vocal cords
True vocal cords:
White bands of elastic tissue, which vibrate to produce sound
False vocal cords:
Are located above true cords and have no role in sound production
The glottis is an opening between the true vocal cords
Voice Production
Speech occurs when expirated air passes through the vocal cords. The vocal cords open and close rapidly.
Pitch is influenced by the length and tension of the vocal cords.
During puberty in males, the vocal cords lengthen, hence the lower voice.
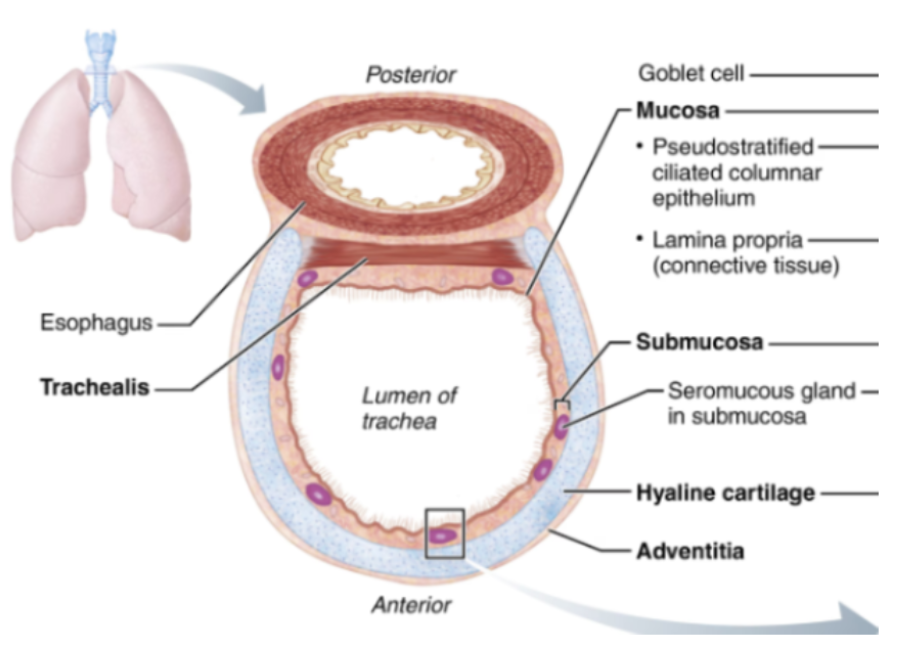
Trachea
A flexible and mobile airway
10-12 cm in length, has a diameter of approx 2.5cm
It has pseudostratified ciliated columnar epithelium
The cilia move mucus towards the pharynx. Smoking is bad because it destroys cilia, resulting in only coughing being able to clear mucus.
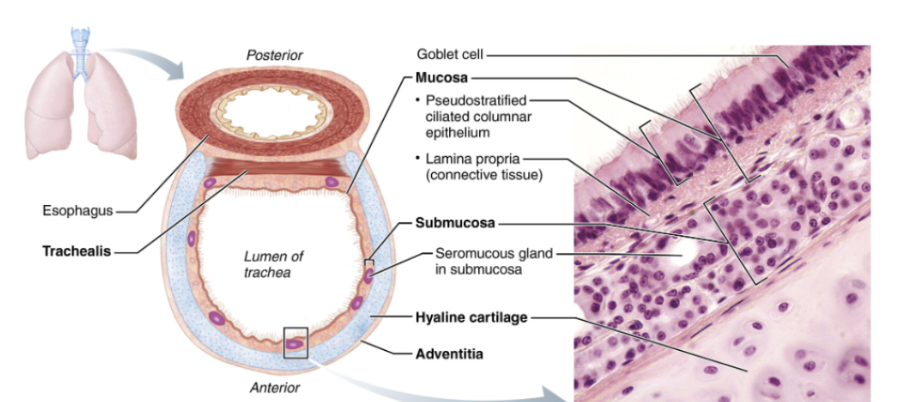
Tracheal Wall Layers
Mucosa
Submucosa
Contains seromucous glands
Hyaline cartilage rings
16–20 C-shaped rings
Prevent airway collapse
Adventitia
Respiratory membrane
Made up of alveolar wall, capillary wall and basal lamina
It forms an air-blood barrier. Gas exchange occurs by diffusion
Type I Alveolar Cells
Made up of simple squamous epithelial cells
Form a thin gas-exchange surface
Type II Alveolar Cells
Create a surfactant which reduces surface tension and prevents alveolar collapse.
Notable features of Alveolis
Elastic fibres
These allow lungs to expand and recoil
Alveoloar pores
These equalize air pressure between alveoli
Provide alternate pathways if the bronchi are blocked
Alveolar macrophages
Remove dust and pathogens
Over 2 million macrophages are cleared per hour
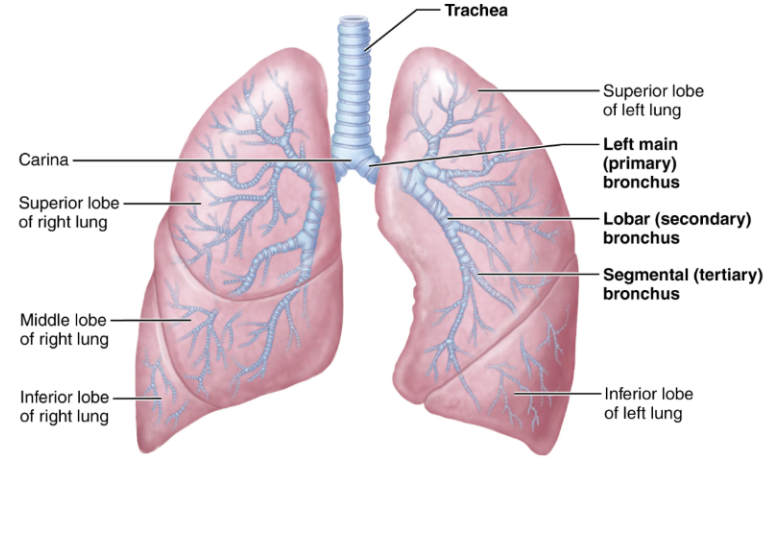
The Bronchial Tree
Refers to the branching system of airways inside the lungs. Air travelling through will become warmed, humidified, and cleansed of impurities.
There are approximately 23 orders of branching air passages.
There are two primary bronchi, with the rIght primary bronchus being wider, shorter and more vertical. As a result, foreign objects are more likely to enter it
The bronchial tree progressively branches into smaller airways. It goes like this
Primary bronchi
Secondary bronchi
Tertiary bronchi
Bronchioles
Terminal bronchioles
Bronchioles and terminal bronchioles
Bronchioles have a diameter less than 1mm, while terminal ones have a diameter less than 0.5mm (they’re the smallest structures of the conducting zone)
After the terminal bronchioles, the respiratory zone begins
Structural changes along the bronchiole tree
Cartilage (function is keeping larger airways open):
The trachea has C-shaped rings
Bronchi have cartilage plates
Bronchioles have no cartilage
Epithelium:
Changes from Pseudostratified ciliated columnar epithelium (larger airways) to columnar and cuboidal epithelium (smaller bronchioles)
Bronchioles have no cilia or mucus-secreting cells
Smooth muscle (function is to allow bronchoconstriction and bronchodilation, which regulates airflow):
Relative amount present increases as airway diameter decreases.
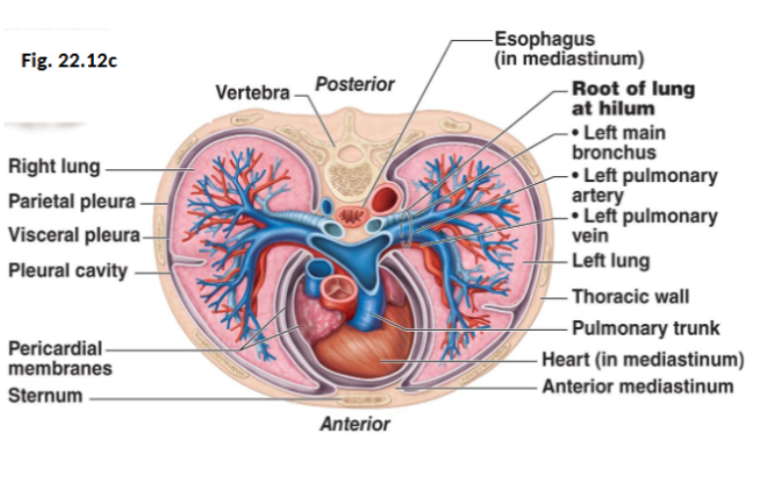
Lung structure
Lungs are paired organs, occupying most of the thoracic cavity
The mediastinum lies between the lungs
Each lung sits in its own pleural cavity
Lungs are connected to the mediastinum through vascular and bronchial attachments
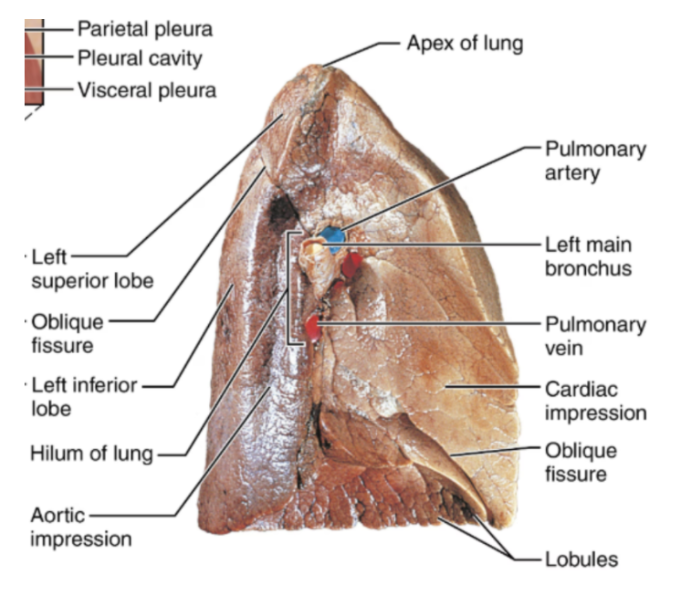
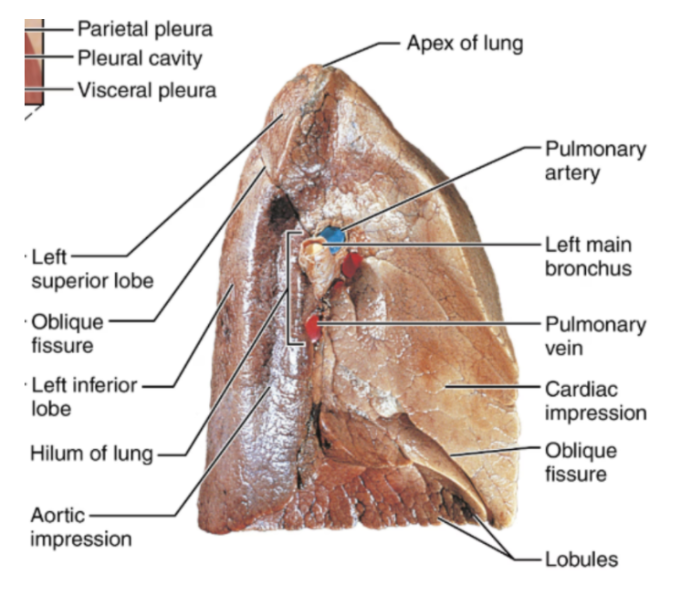
External Lung Features
Apex
The superior tip of the lung
Base
The inferior surface rests on the diaphragm
Hilium
A region where structures enter and leave the lungs.
Structures include bronchi, blood & lymphatic vessels, and nerves.
Costal surface
Lung surface that contacts the ribs
Cardiac Notch
An indentation in the left lung that accommodates the heart
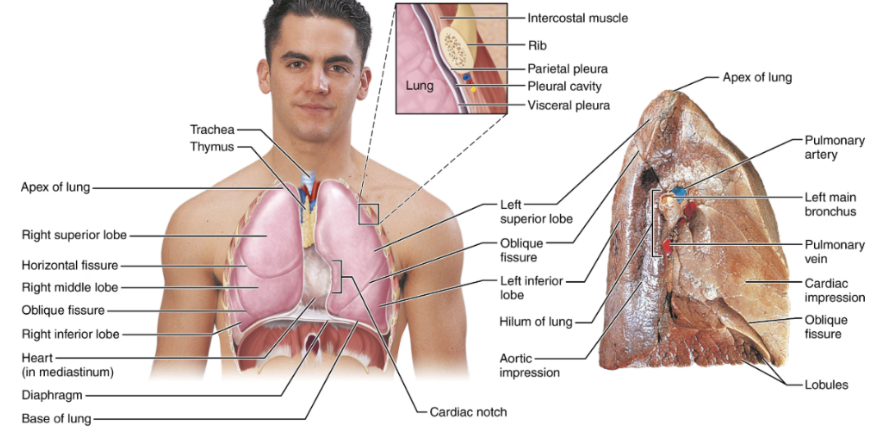
Lung fissures
Oblique fissure
Present in both lungs
Horizontal fissure
Present only in the right lung
The fissures divide lungs into lobes
Bronchoulmonary segments
Subdivided by the septum, approx 10 segments.
Each segment has its own tertiary bronchus, pulmonary artery and pulmonary vein
Lobules
The smallest visible subdivisions of the lung
They are hexagon-shaped
Approx the size of a pencil eraser
Supplied by a large bronchiole
Pulmonary circulation
Pulmonary arteries carry deoxygenated blood to the lungs
Pulmonary veins return oxygenated blood to the heart
Both the parasympathetic and sympathetic nervous systems control airway diameter and other lung functions
Bronchial circulation
Bronchial arteries deliver oxygenated systemic blood to lung tissues
Bronchial veins return blood to the right side of the heart
Pleurae
Thin, double-layered serous membranes
Parietal pleura:
Lines the thoracic cavity wall
Visceral pleura:
Covers the lung surface
They have 3 chambers, the central mediastinum and 2 lateral pleural compartments
Pleurisy refers to inflammation of the pleural membranes, causing painful breathing.
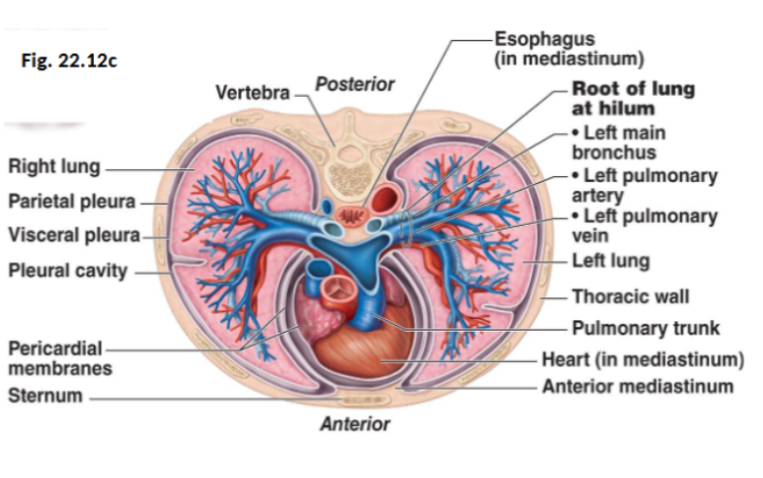
Pleural cavity
The space between the pleural layers
It’s filled with pleural fluid
Functions of pleural fluid include:
Lubricating lung movement during breathing
Keeping lungs attached to the thoracic wall via surface tension
Physiologic Dead Space
Refers to the air that does not participate in gas exchange
Typical dead space is 150mL.
Eg: If tidal volume is 500mL, 150mL is dead sace, and 350mL is alvelolar ventilation
Anatomical dead space: Refers to air in conducting airways
Functional Dead Space: Refers to air reaching non-erfused alveoli
Pulmonary ventilation is made up of inspiration + expiration
If some alveoli are no longer functional, total dead space = 150mL + alveolar dead spaces
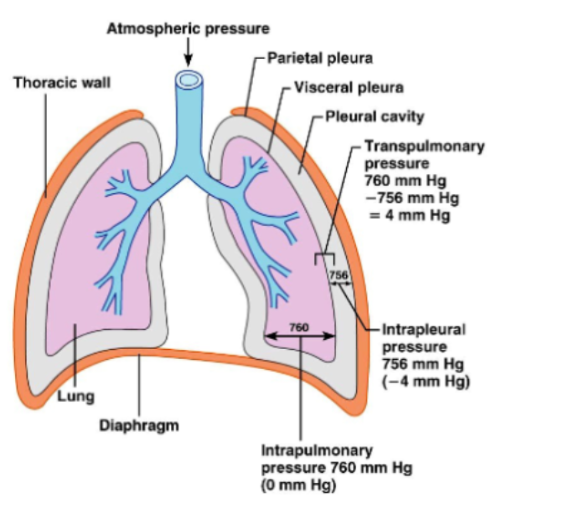
Atmospheric pressure
Refers to the pressure exerted by the air around the body
At sea level, it’s 760mmHg
Respiratory pressures are measured relative to atmospheric pressure
Eg: 04mmHg relative pressure = 756 mmHg absolute pressure
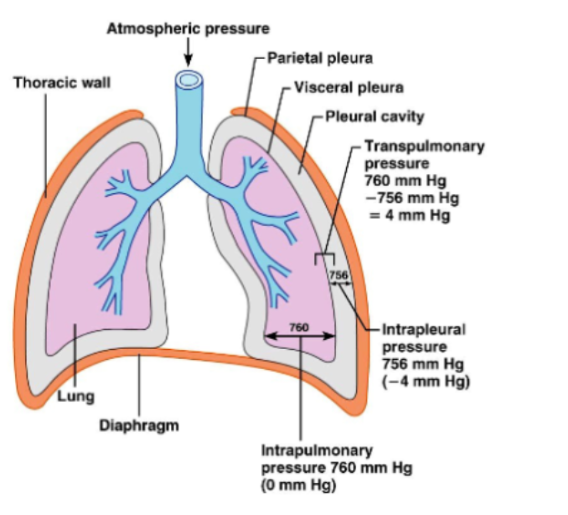
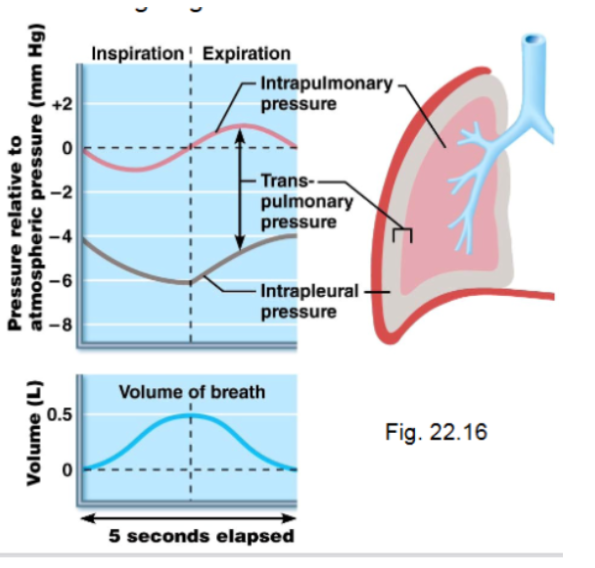
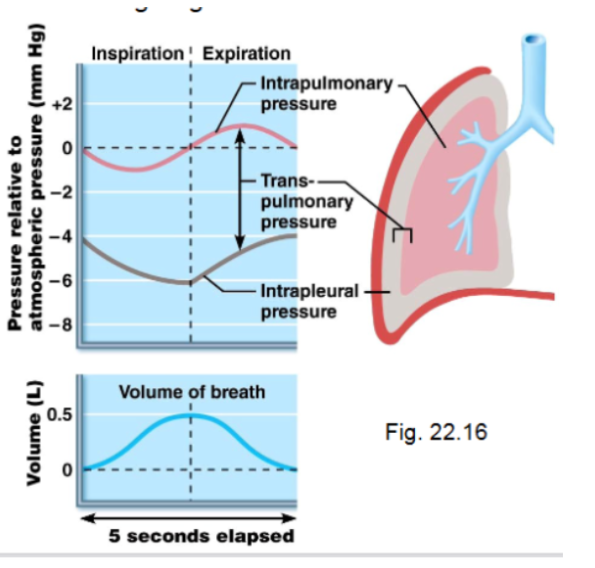
Intrapulmonary Pressure
Refers to pressure inside alveoli.
Changes during breathing.
Eventually equalizes with atmospheric pressure.
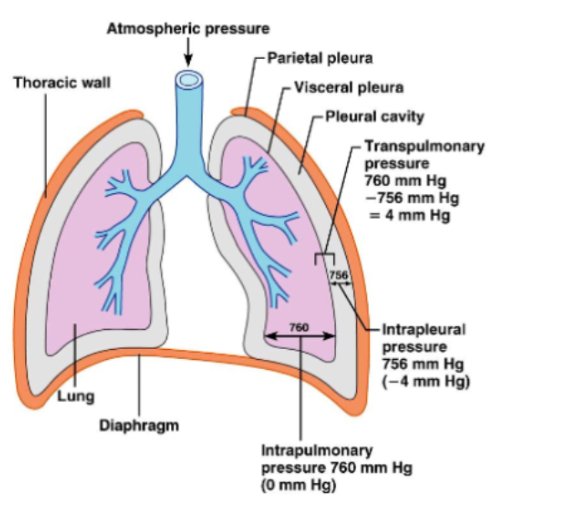
Intrapleural Pressure
Pressure inside the pleural cavity.
Normally, about 4 mmHg lower than alveolar pressure.
This negative pressure is due to:
Elastic recoil of lungs
Surface tension of alveolar fluid
Elasticity of chest wall
If intrapleural pressure becomes equal to atmospheric pressure, the lung collapses. It’s possible for only one lung to collapse because they are in separate pleural cavities.
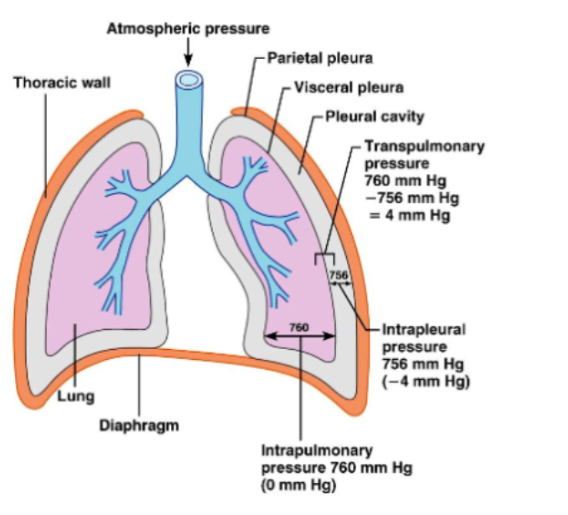
Transpulmonary pressure
The pressure that keeps the lungs expanded
TP = Intrapulmonary pressure - Intrapleural Pressure
Quiet Inspiration
A mechanic of breathing
Muscles involved are the diaphragm and the external intercostals
Basically
Thoracic cavity volume increases
Intrapulmonary pressure decreases
As a result, air flows into the lungs
The lung volume increases by about 0.5L, and intrapleural pressure drops ot about -6mmHg
Quiet Expiration
A mechanism of breathing. It’s a passive process. Depends more on the elastic recoil of the lungs
Inspiratory muscles relax
The rib cage descends
Lungs recoil
Thoracic volume decreases
As a result, intrapulmonary pressure rises to +1mmHg, and air flows out of the lungs
Deep/Forced Inspiration
This process is assisted by accessory muscles (neck and chest)
These muscles raise the ribs further and expand the thoracic cavity more.
Forced Expiration
An active process
The muscles involved are the abdominal muscles and the internal intercostals
This process increases abdominal pressure and depresses the rib cage.
As a result, air is forced out of the lungs.
3 major factors influencing pulmonary ventilation
Airway resistance
Alveolar Surface Tension
Lung compliance
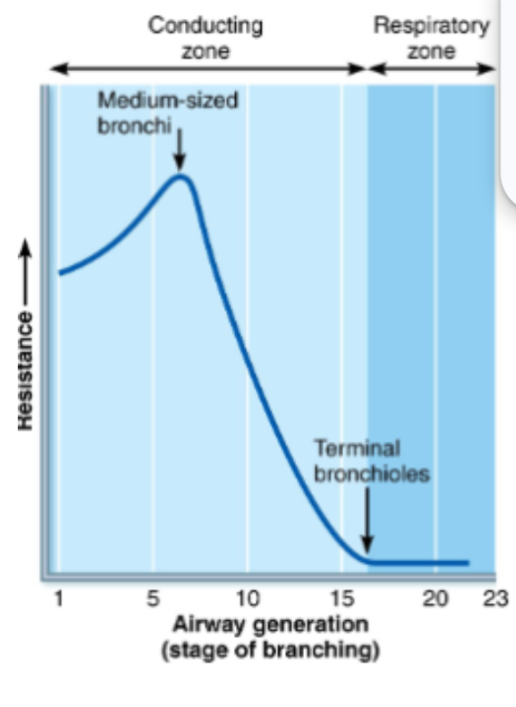
Airway Resistance
A major factor influencing pulmonary ventilation
Note: Gas Flow = Pressure Gradient/Resistance
As a result, resistance depends mainly on airway diameter.
Resistance is greatest in medium-sized bronchi
The parasympathetic nervous system causes bronchoconstriction. This can occur during asthma attacks
The sympathetic nervous system causes bronchidilation
Airway resistance also increases with mucus, infection or tumours
Alveolar Surface Tension
A major factor influencing pulmonary ventilation
Surface tension occurs at the air-liquid interface in alveoli
Water molecules are more attracted to each other than to the gas, and as a result, tend to collapse alveoli.
They resist any force to increase surface area.
I guess they take up space that should be occupied by air?
Surfactant
Produced by type II alveolar cells
A detergent-like lipoprotein
It reduces surface tension and prevents alveolar collapse by interfering with the cohesiveness of water molecules
Infant Respiratory Distress Syndrome (IRDS)
Occurs in premature infants
Caused by insufficient surfactant production
The result is alveoli collapsing, and as a result, the infants need assisted ventilation