Anatomy of the Heart and Blood Flow Through the Fetal Heart
1/17
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
18 Terms
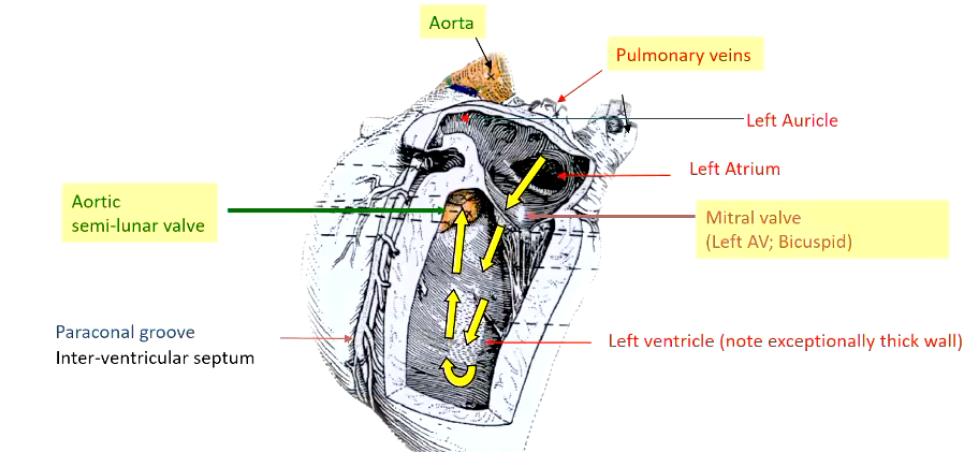
Describe the main features of the left atrium and ventricle.
• Blood flow: Oxygenated blood enters the L. Atrium (& auricle) via Pulmonary veins
• Mitral valve (bicuspid) or left AV valve guards' entrance to the left ventricle
Two major cusps in this location, has chordae tendinae, papillary muscles, acts similarly to tricuspid valve
• L. Ventricle: forms Apex of heart - very thick wall
• Aortic semi-lunar valve - guards entrance to aorta
• Aorta exits middle of base of heart → to the body
What tissue do the coronary arteries supply?
Coronary arteries supply oxygenated blood and nutrients specifically to the heart muscle (myocardium), enabling it to function and pump blood throughout the body.
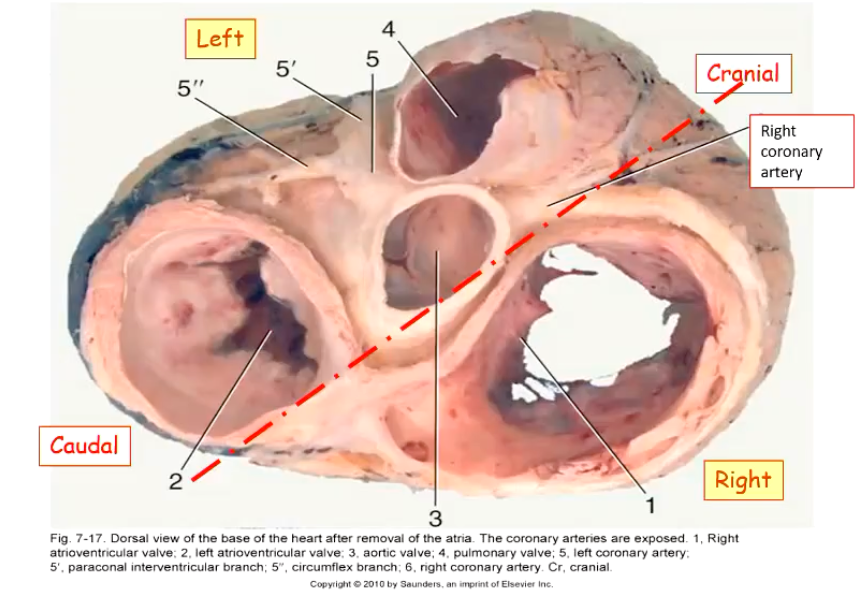
List the four valves of the heart and describe their anatomical position within the body.
What does puncta maxima mean?
Puncta maxima (Latin for "points of maximum" [intensity]) in the context of the heart refers to the specific locations on the chest wall where the sound of a particular heart valve is best heard during auscultation.
Describe the proximal positions of where the valves of the heart are best heard when auscultating.
• Pulmonic valve: @ ventral part of left 3rd intercostal space
• Aortic valve: @ dorsal part of left 4th intercostal space
• Mitral valve: @ ventral part of left 5th intercostal space
• Tricuspid valve: @ mid right 4th intercostal space
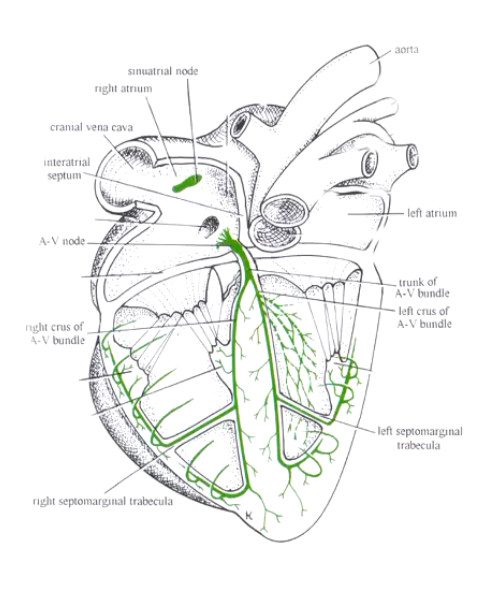
What structures in the heart are part of the impulse conducting system of the heart?
SA and AV nodes - part of the impulse conducting system of the heart:
• Spontaneous contraction
• Location SA; AV nodes both in the right atrium
•AV bundle travels within the interventricular septum- directs the impulse to the apex (So therefore the ventricles contract first)
•Trabecula septomarginalis- (moderator band): papillary muscles associated with each AV valve receives impulse in advance of main contraction. More prominent feature of the right ventricle
Describe the ANS innervation of the heart and what effects the innervation has on the structures.
Sympathetic: Increases rate/strength of contraction
Parasympathetic: Decreases rate of contraction
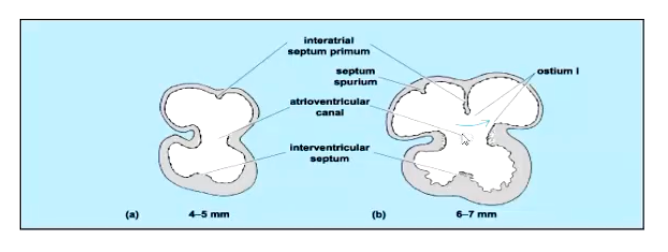
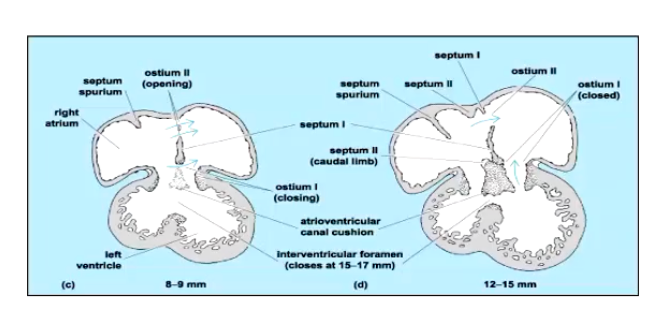
Describe the steps involving the formation of the four chambered heart (Pt. 1)
When does the fully functional four chambered heart form?
Starts with just 2 chambers
Subdivision of the primitive atrium and ventricle -beginning marked by appearance of interatrial septum primum and interventricular septum
Single atrioventricular canal between the primitive atrium and ventricle also begins to divide- will eventually form separated right and left atrioventricular ostia
Fully functional 4-chambered heart does not form until birth.
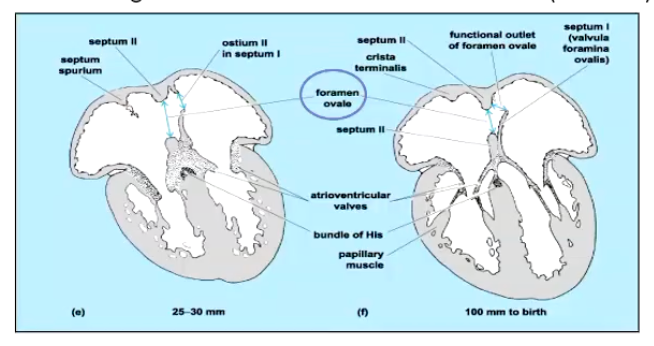
Describe the steps involving the formation of the four chambered heart (Pt. 2)
Subdivision of the primitive ventricle continues-via interventricular septum
The interventricular foramen will eventually close
The atrioventricular canal is now splits into two
The interatrial septum continues to form but separation is never complete- communication between the two atria continues until birth (foramen ovale)
This hole only closes at birth
Describe the steps involved in the formation of the 4-chambered heart (Pt. 3).
• Ventricles are now separate
• AV valves form between the atria and ventricles on each side of the heart
• The left and right atria continue to intercommunicate (RA to LA) via foramen ovale
Foramen ovale remains patent until birth
Before birth, the lungs are not functional, what important modifications are made to fetal blood flow due to this phenomenon?
• Before birth:
- Lungs are not functional- high resistance pulmonary circulation
- Blood flows mainly through the low resistance systemic
circulation and the placenta
• Two important shunts allow bypassing of the pulmonary circuit
- foramen ovale
- ductus arteriosus
• A third shunt in the liver maximises the pO2 of blood entering the heart from the placenta
ductus venosus
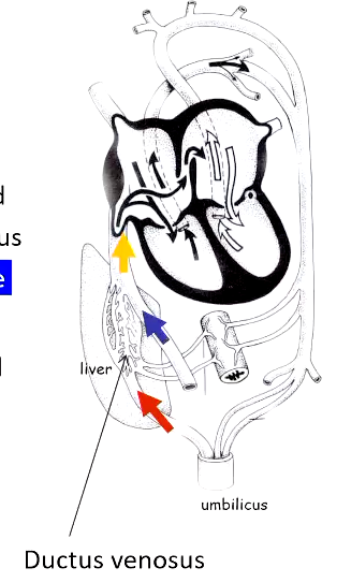
Describe the function of the ductus venosus in fetal circulation.
Oxygenated blood from the placenta travels from the umbilicus toward the liver via the umbilical vein. (Red arrow)
The fetus needs to preserve this high-oxygen blood, so it should not be significantly mixed with or metabolised by the liver.
The ductus venosus is a vascular shunt within the liver that allows most of the oxygenated umbilical venous blood to bypass the hepatic circulation, preventing mixing with the less-oxygenated venous blood returning from the fetal gut (Blue Arrow)
This relatively high pO₂ blood then enters the caudal (inferior) vena cava (Yellow arrow) and flows into the right atrium, where it preferentially contributes to oxygen delivery to vital organs (especially the brain and heart)
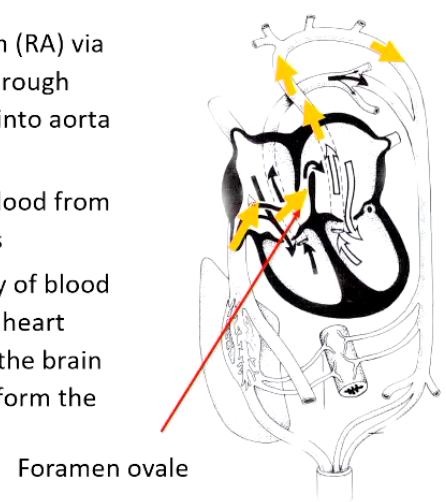
Describe the function of the foramen ovale in fetal circulation.
Oxygenated blood entering the right atrium via the caudal (inferior) vena cava is directed across the foramen ovale into the left atrium, bypassing the non-functioning lungs.
Because the fetal lungs receive very little blood flow, the left atrium does not receive blood from the pulmonary circulation.
This relatively high-pO₂ blood passes from the left atrium into the left ventricle and is pumped into the aorta.
The aortic flow is arranged so that the most oxygen-rich blood is preferentially delivered to vital organs, particularly the heart (via the coronary arteries) and the brain, before blood continues into the descending aorta.
Describe the function of the ductus arteriosus in fetal circulation.
Deoxygenated blood returning from the head and upper body enters the right atrium via the cranial (superior) vena cava (Blue arrow) and is directed into the right ventricle.
Because the fetal lungs are fluid-filled and not ventilated, the pulmonary vascular resistance is very high, so little blood can flow into the pulmonary arteries.
Instead, blood is diverted through the ductus arteriosus (Star), a shunt that connects the pulmonary artery directly to the aorta, bypassing the lungs.
This shunted blood mixes with the more oxygenated blood in the aorta, resulting in a lower pO₂ in blood supplied to the lower body compared with blood going to the brain and heart (Green arrow)

What happens to fetal circulation at birth?
If these maturation processes do not happen, what are the defects that might occur?
• Ductus venosus (liver) often persists until birth in carnivores, ruminants and humans then closes
Defect: Patent ductus venosus results in a portacaval shunt: portal blood by passes liver
• Ductus arteriosus- turbulence due to inflation lungs causes smooth muscle to constrict DA - forms ligamentum arteriosum
Defect: Patent ductus arteriosus- serious- characteristic machinery murmur
• Foramen ovale (heart) - lungs inflate, blood flows to lungs- increase blood flow to LA results in functional closure before anatomical closure- forms scar tissue in interatrial wall= fossa ovalis in RA
Defect: Patent foramen ovale -generally is not problematic
What is the ligamentum arteriosum?
Ligamentum Arteriosum:
A feature of foetal circulation associated with the pulmonary trunk
Ligament linking the pulmonary trunk and aorta
Foetal remnant of the ductus arteriosus -directly linked the pulmonary trunk to the aorta in the foetus (see foetal circulation)
Describe the 3 main categories of congenital defects in failure of closure of structures, as well as great vessel defects within the fetus.
• Failure of closure of foetal structures
foramen ovale
ductus arteriosus (PDA)
ductus venosus (liver)
• Septal defects e.g. interventricular septum
• Great vessel defects
defects of outflow tracts - aortic or pulmonary valves
dysplasia - malformed or disorderly
stenosis — decreased lumen size
malposition / fusion of great vessels
Explain how the right atrium recieves deoxygenated AND oxygenated blood and what implications this has for fetal blood flow.
How is the right atrium receiving oxygenated blood?
In the fetus, the placenta, not the lungs, oxygenates blood.
Placenta → umbilical vein
Blood here has the highest pO₂ in the fetus.
Umbilical vein → ductus venosus → caudal (inferior) vena cava
The ductus venosus bypasses the liver, preserving oxygen content.
Caudal vena cava → right atrium
This blood is relatively well oxygenated compared with the rest of fetal venous blood.
⚠ Important nuance:
The RA receives a mix of blood:
Higher pO₂ blood from the caudal vena cava (placenta-derived)
Lower pO₂ blood from the cranial vena cava (head/upper body)
So the RA is not purely deoxygenated in the fetus.
Why is passing this blood into the left atrium so important?
Because the fetus needs to prioritize oxygen delivery to vital organs.
Key reasons:
Lungs are not functioning
High pulmonary resistance
Very little blood should go to the lungs
Foramen ovale creates a shortcut
Directs the most oxygenated blood from the RA → LA
Bypasses the right ventricle and pulmonary circulation
Left ventricle pumps to brain and heart
Blood entering the LA → LV → ascending aorta
Supplies:
Brain
Coronary circulation (heart muscle)
➡ This ensures that the organs most sensitive to hypoxia get the best-oxygenated blood available.