EPIDEMIOLOGY EXAM 2
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
41 Terms
Sensitivity
The ability of a test to correctly identify people who have disease.
Specificity
The ability of a test to correctly identify people who do not have disease.
Sensitivity Calculation
a/a+c
Specificity Calculation
d/b+d
Positive Predictive Value
proportion of positive test results that are true positives
Negative Predictive Value
proportion of negative test results that are true negatives.
PPV Calculation
(a)/(a+b)
NPV Calculation
d/c+d
Measures of Association
relative risk
prevlance raito
odds ration
measures of occurance
incidence
prevalence
Relative Risk
Best for cohort studies, ratio of risk of disease in exposed versus unexposed
Relative Risk Calculation
(a/a+b)/(c/c+d)
Odds Ratio
Best for Case Control Study, compares the odds that people with the disease were exposed compared to those without the disease, will approximate the relative risk / risk ratio when prevalence ratio is less than 10% (rare disesase)
Odds Ratio Calculation
([a*d)/(b*c)]
Prevalence Ratios
Best for cross sectional study, having” the outcome, same calc as RR
Risk Difference
Risk of disease in the unexposed, if exposure was removed how would the risk change?
Risk Difference Calculation
(a/a+b)-(c/c+d)
Bias
A systematic error in design or conduct of study which leads to error in estimation
of association
Systematic Error
This leads to bias, confounding leads to this → does not arise by chance!
Random Error
Arises by chance, hard to account for
Selection Bias
How participants care chosen for a study.
how it happens:
Participant selection procedure
Non compliance selective survival
Loss to follow up/missing data
Types of Selection Bias
Admission rate bias (includes Berkson’s)
Prevalence-Incidence Bias (aka Neyman’s)
Membership Bias (includes “healthy worker effect”)
Non-response bias (includes volunteer and compliance bias)
Loss to follow-up bias
Information Bias
The way information is collected in a study, can result in misclassification
Information Bias Types
Interviewer bias: Systematic error due to the interviewer’s conscious or sub-conscious gathering of selective data.
Observer bias: Systematic difference between a true value and what was observed due to observer variation
Detection bias: When individuals with certain exposures are under closer surveillance by medical care system
Temporal bias
Publication bias: Occurs because of the influence of study results on the chance of publication
Recall Bias
People with disease remember or report exposures differently (more or less accurately) than those without disease
Confounding
leads to systematic error, failure to control for common causes of the exposure and outcome
Validity
Accuracy, The ability of the test to correctly identify people with and without disease-> when test can actually do the thang, but how often its doing the thang we dont know: sensitivity and specificity
Reliability
Precision, The ability of the test to give the same result on repeated tests
Interobserver variation
Screening
The examination of asymptomatic people in order to classify them as likely or unlikely to have disease. (not a diagnosis)-> wants to lead to a diagnostic test
Detectable Preclinical Phase
The period between the earliest time at which the disease can be detected by screening and the usual time that a diagnosis would be made for a symptomatic patient. -> mass screening best at this time, high risk is prioritized.
When Dpcp is prevalent in pop, mass screening is cost effective and reasonable
When dpcp prevalence is low, targetted screening of hugh risk is best
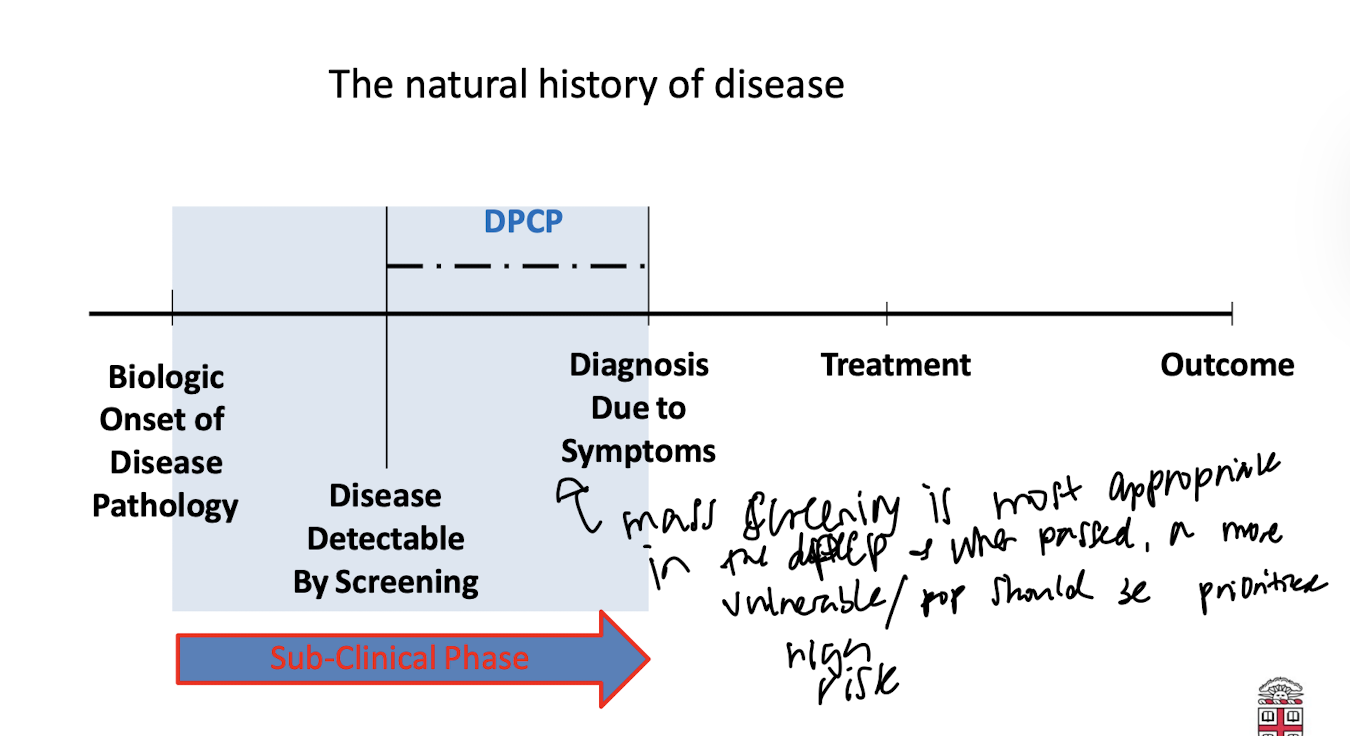
The Natural History of Disease
Biologic onset of disease pathology→ disease detectable by screening(DPCP here) diagnosis due to symptoms→treatment→ outcome
Lead Time
The interval between disease detection by screening and the time that the disease would have been diagnosed due to symptoms.-> amt of time that screening improves disease diagnosis
Lead Time Bias
Overestimation of survival duration among screened cases compared to unscreened cases when survival is measured from time of diagnosis to time of death.-> overestimation of screening benefits
Casuality
An event, condition, or characteristic without which the disease would not have occurred. permits rational plans and actions to break the links between the
factors causing disease, and disease itself.
Direct Casuality
Factor → Disease
Indirect Casuality
Factor→ Step 1→ Step 2→ Disease
Necessary
In presence of the factor, the disease develops.The factor is ______ to cause disease (cant do it alone, but the factor is needed w/ something else)
Sufficient
Factor inevitably causes disease, the factor ALONE can cause the disease
Bradford Hill Criteria
Strength of the association
2. Consistency - replication
3. Specificity of the association
4. Temporality: cause must be present before effects
5. Biological gradient: higher exposure=higher disease
6. Plausibility
7. Coherence
8. Experiment
9. Analogy
Bradford Hill Criteria Limitations
Strength:Depends on the prevalence of other causes of disease present in the population, not a biologic characteristic
Consistency: There are plausible reasons for not seeing consistent results, and these exceptions are best seen with hindsight
Specificity: A cause can have many effects
Temporality: Difficult to establish
Biologic gradient: Threshold effects
Plausibility: Too subjective
Coherence: Vague; too similar to plausibility
Experiment: Not always available or feasible
Analogy: Analogies abound
Diseases Appropriate for Screening
Serious with major consequences
Earlier identification leads to more effective
treatment
Progressive with a detectable preclinical phase
(DPCP)
DPCP is long and prevalent in the target
population