Clinical Pysch test 2 (mood and anxiety disorder)
1/159
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
160 Terms
Epidemiology
The scientific study of how diseases and other health conditions are distributed (who, when, where) and determined (causes, risk factors) within populations, and then applying that knowledge to control health problems
Prevalence, gender, culture
Etiology
the study of the causes, origins, or reasons behind a disease, symptom, or medical condition
Evidence-based Treatment
Medication and psychotherapy
First line approaches, and in some cases, second line approaches when those fail
Clinical description
Symptoms, syndromes, diagnostic criteria, case studies
Test fromat
Clinical description
Epidemiology
Etiology
Evidence-based treatment
Mood disorders
Disorders, such as depressive disorders or bipolar disorders, in which there are disabling disturbances in emotion.
Two Broad types of mood disorders
Unipolar depressive disorders
Bipolar disorders
Unipolar depressive disorders
a mental health condition characterized by persistent, intense feelings of sadness, low mood, and a lack of interest in activities (anhedonia) without any manic or hypomanic episodes
Bipolar disorder
a chronic mental health condition characterized by intense mood swings, ranging from extreme highs (mania/hypomania) to severe lows (depression)
How many Unipolar depressive disorder
Major depressive disorder (MDD)
Persistent depressive disorder (PDD)
Premenstrual dysphoric disorder (PDSD)
Disruptive mood dysregulation disorder (DMDD)
4
How many Bipolar disorders
Bipolar I disorder
Bipolar II disorder
Cyclothymia
3
Major depressive disorder (MDD) Criteria
5+ Symptoms
o Sleeping too much or too little
o Psychomotor retardation or agitation
o Poor appetite and weight loss, or increased appetite and
weight gain
o Loss of energy
o Feelings of worthlessness or excessive guilt
o Difficulty concentrating, thinking, or making decisions
o Recurrent thoughts of death or suicide
(Including sad mood or anhedonia) (must have one)
For 2 weeks (nearly all or most days)
anhedonia
the reduced ability to experience pleasure or a total loss of interest in activities once enjoyed
Major depressive disorder Symptom list (5)
o Sleeping too much or too little
o Psychomotor retardation or agitation (Slow movement vs fidgeting)
o Poor appetite and weight loss, or increased appetite and
weight gain
o Loss of energy
o Feelings of worthlessness or excessive guilt
o Difficulty concentrating, thinking, or making decisions
o Recurrent thoughts of death or suicide
Psychomotor retardation
Thoughts and movements may slow
Psychomotor agitation
Cannot stand still (Fidget, pace etc)
Episodic disorder (Which disorder)
MDD because symptoms present for a period then clear. Once one episode finishes it can appear in a couple months or years etc.
Among people with a first depressive episode
15% state symptoms persists for about 10 years
50% who recover from first MDD episode experience at least one more across 10 years
Persistent Depressive Disorder (PDD) Criteria
Depressed mood for at least 2 years
o 1 year for children/adolescents
At least two of the following during that time (2):
Sleeping too much or too little
Poor appetite or overeating
Low energy
Poor self-esteem
Trouble concentrating or making decisions
Feelings of hopelessness
Persistent depressive disorder
chronically depressed—more than half of the time for at least 2 years, they feel blue or obtain little pleasure from activities and pastimes.
Premenstrual dysphoric disorder
Mood symptoms in the week before menses
Disruptive mood dysregulation disorder
Severe recurrent temper outbursts and persistent negative mood for at least 1 year beginning before age 10
Epidemiology and Consequences of Depression (1 of 2)
Depression is common
o Lifetime prevalence:
• 16.2% MDD (FOR US in some point in their life)
• 5% Depression more than 2 years (US)
• Twice as common in women as in men
o Three times as common among people in poverty
• Prevalence varies across cultures
o MDD
• 6.5% in China
• 21% in France
o Cultural factors play an important role in depression rates
(4 things to remember)
MDD and PDD comorbidity %
45
Approximately _______ % of people will experience MDD during their lifetime.
16.2
Epidemiology and Consequences of Depression (2 of 2)
Symptoms vary across cultures
o Focus on somatic symptoms (e.g., pain, fatigue)
• Ethnic minorities in the US
• People from Latin America and some Asian countries
• Age of onset
o Early 20s
o Decreased over past 50 years
• Co-morbidity
o 5-30% with MDD experience PDD
o 60% of those with MDD will also meet criteria for anxiety disorder at some point
With each generation, age of onset gets lower for MDD
Manic and hypomanic Episode criteria (Ask in class)
4 (3) symptoms (5 (4) if mood is not elevated)
• Distinctly elevated or irritable mood
• Abnormally increased activity and energy
• PLUS other symptoms:
o Increased goal-directed activity or psychomotor agitation
o Talkativeness or rapid speech
o Flight of ideas or racing thoughts
o Decreased need for sleep
o Increased self-esteem or grandiosity
o Distractibility
o Excessive involvement in activities that are likely to have undesirable
consequences (e.g., reckless spending/sexual behavior/driving)
Manic episode criteria presentation
Symptoms last at least 1 week, require hospitalization, or include psychosis
o Symptoms cause significant distress or functional impairment
hypomanic episode criteria presentation
o Symptoms last at least 4 days
o Clear changes in functioning that are observable to others, but impairment is not marked
o No psychotic symptoms are present
(Less intense and does not disrupt life)
Bipolar I Criteria
1.At least one episode or mania during the lifetime
2.May or may not have a depressive episode during the lifetime
In fact, even someone who experienced only 1 week of manic symptoms years ago is still diagnosed with bipolar I disorder.
mania
Intense elation or irritability, accompanied by symptoms such as excessive talkativeness, rapid thoughts, distractibility, grandiose plans, heightened activity, and insensitivity to the negative consequences of actions.
Bipolar II Criteria
o At least one major depressive episode
o At least one episode of hypomania
o No episodes of mania
hypomania
a change in functioning that does not cause serious problems.
Cyclothymic disorder criteria
o Milder, chronic form of bipolar disorder
o Symptoms lasts at least 2 years in adults
• 1 year in children/adolescents
o Numerous periods with hypomanic and depressive symptoms
• Does not meet criteria for hypomania or major depressive Episode
• Symptoms do not clear for more than 2 months at a time
• Symptoms cause significant distress or impairment
Prevalence of Bipolar disorders
1% in U S; 0.6% worldwide for Bipolar I
0.4% – 2% for Bipolar II
4% for Cyclothymia
age of onset in Bipolar disorders
Average age of onset in 20s
No gender differences in rates of bipolar disorders
Consequences of Bipolar disorder
o 15% unemployed full-time in past year
o Suicide rates high
o One in four report suicide attempt
• More than half report suicidal ideation in past 12 months
Heritability Mood disorders Estimates
o 37% MDD
o 93% Bipolar Disorder
• Unlikely one gene explains these illnesses
o More likely Gene x Environment Interaction
Gene for MDD
• Serotonin transporter gene (5-HTT) polymorphism
o Short allele combination of the 5-HTT gene and childhood maltreatment or adulthood stressful life events increases risk of MDD
Etiology of Mood Disorders: Neurotransmitters (NTs)
Norepinephrine, dopamine, and serotonin effect mood disorders
New models focus on sensitivity of postsynaptic receptors
o Stress may lead to changes in sensitivity of serotonin receptors
o Dopamine plays a major role in the reward system
o Dopamine dysfunction may be connected to specific symptoms
(e.g., changes in energy and motivation)
o Dopamine receptors may lack sensitivity in MDD
o High receptor sensitivity in mania– fluctuating?
Etiology of Mood Disorders
o Genetic factors
o Neurotransmitters
o Brain regions
o Neuroendocrine System
o Social factors
o Psychological factors
Etiology of Mood Disorders: Brain Function
Oversensitivity to emotional stimuli (elevated amygdala)
• Interference with emotion regulation (elevated anterior cingulate, diminished prefrontal cortex and hippocampus)
• Motivation to pursue rewards (striatum, dopamine activity) • Disruptions in the connectivity of these regions
Etiology of Mood Disorders: Neuroendocrine System
Overactivity of HPA axis (Releases cortisol)
High cortisol damages hippocampus
effects in MDD and BD
Etiology of Mood Disorders: Social Factors in Depression
o 42-67% report a stressful life event in year prior to depression
o 40% risk of developing depression when experiencing stressful
life event without support (4% risk with support)
• Interpersonal difficulties
o High levels of expressed emotion predict relapse
o Marital conflict also predicts depression
o Lack of social support
o Reassurance-seeking
Etiology of Mood Disorders: Psychological Factors in Depression (1 of 4)
Neuroticism
o Tendency to experience frequent and intense negative affect
o Also predicts onset of anxiety, which is highly comorbid withdepression
• Cognitive Theories
o Negative thoughts and beliefs cause depression
o Beck’s Theory, Hopelessness Theory, Rumination Theory
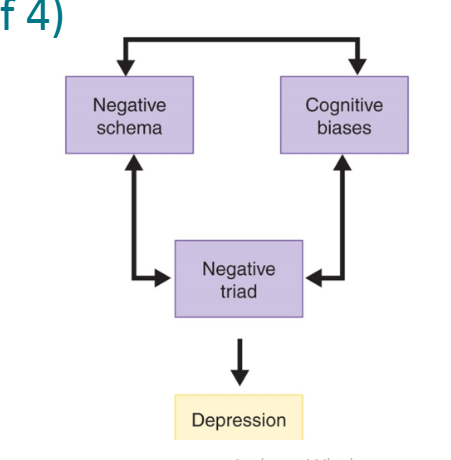
Beck’s theory
Consists of Negative triad, negative Schema, Cognitive biases
3 negative thinking patterns
Negative triad: negative view of self
Negative schema: Negative view of world
Cognitive biases: process info negative
Negative triad
negative view of self
Negative schema
Negative view of world
Cognitive biases
process info negative
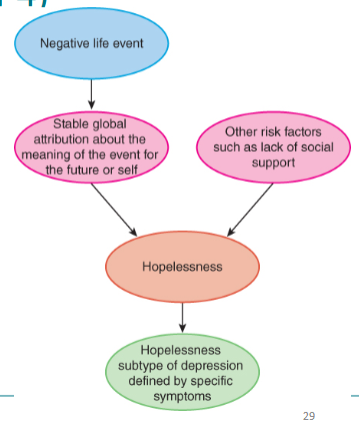
Hopelessness Theory
People become depressed when they start to feel hopeless about the future
Most important trigger of
depression is hopelessness
• Desirable outcomes will
not occur
• Person has no ability to
change situation
Due to global or specific causes and stable or unstabe
Global causes
Effects all areas
Specific causes
Only effects on area
Stable
Will always last is true
Unstable
Temporary
Rumination
o Tendency to repetitively dwell on sad thoughts
o Most detrimental form is to brood regretfully over causes of event
Predictors of mania
Reward sensitivity
• High responsively to rewards
• Life events that involve attaining goals
• Excessive goal pursuit
o Sleep disruption
Bipolar and MDD similarity
Triggers of depressive episodes in BD appear similar to triggers in MDD
Psychological Treatment of Depression
Interpersonal psychotherapy (IPT)
Cognitive therapy (CT)
Mindfulness-based cognitive therapy (MBCT)
Behavioral activation (BA) therapy
Behavioral couples therapy
Interpersonal psychotherapy (IPT)
o Focus on major interpersonal problems (e.g., role transitions) (relations)
o Identify feelings, make decisions, and resolve problems related to interpersonal issues
Cognitive therapy (CT)
o Altering maladaptive thought patterns
o Monitor and identify automatic thoughts
• Challenge and replace negative thoughts with more neutral or
positive thoughts
Mindfulness-based cognitive therapy (MBCT)
o Use of strategies, including meditation, to detach from depression-related thoughts and prevent relapse
o Evidence stronger when depression is highly recurrent
Behavioral activation (BA) therapy
Increase participation in positively reinforcing activities to disrupt spiral of depression, withdrawal, and avoidance
o BA is also one component of cognitive therapy
Behavioral couples therapy
Enhance communication and relationship satisfaction
Psychological Treatment of Bipolar Disorder
Psychoeducational approaches
Cognitive Therapy (CT)
Family-focused treatment (FFT)
Psychoeducational approaches for BD
o Provide information about symptoms, course, triggers, and treatments
Cognitive Therapy (CT) for BD
o Similar to depression treatment with additional content to address early signs of mania
Family-focused treatment (FFT)
o Educate family about disorder, enhance family communication, improve problem solving (BD)
Biological Treatment of Mood Disorders
Electroconvulsive therapy (ECT)
Transcranial Magnetic Stimulation for Depression (rTMS)
Electroconvulsive therapy (ECT)
Reserved for treatment non-responders o Induce brain seizure and momentary unconsciousness o Side effects: Short- term confusion and memory loss
Transcranial Magnetic Stimulation for Depression (rTMS)
o Electromagnetic coil placed against scalp
o Pulses of magnetic energy increase activity in key regions of
the brain (different target regions)
o For those that fail to respond to first antidepressant
o Questions about how well controlled the trials are
Medications for Depressive Disorders stats
• 75% of people in US receiving treatment for depression are
prescribed antidepressants
Effective at treating severe, persistent depression
o May not be helpful for those with mild or moderate Symptoms
Medication to treat severe persistent depression
Antidepressants
May not be helpful for those with mild or moderate Symptoms
STAR-D
(Sequenced Treatment Alternatives to Relieve Depression)
Attempted to evaluate effectiveness of antidepressants in real-
world settings (comorbid psychiatric conditions)
• Only 33% achieved full symptom relief with citalopram
• About 30% of non-responders achieved remission with a
different anti-depressant
• Remission rates were low and relapse rates were high
Medication for severe depression
CT (Cognitive therapy) as effective as medication for severe depression
CT more effective than medication at preventing relapse
Combining psychotherapy and medication
Combining psychotherapy and antidepressant medications
increases odds of recovery over either alone by 10-20%
Medications for Bipolar Disorder
Lithium
(80% relief but toxic)
Anticonvulsants
Antipsychotics
(if unable to tolerate lithium effects)
Suicide ideation
thoughts of killing oneself
Suicide attempt
behavior intended to kill oneself
Suicide
death from deliberate self-injury
Non-suicidal self-injury
behaviors intended to injure oneself
without intent to cause death
Epidemiology of Suicide and Suicide Attempts
• 10th leading cause of death in US
• Rates are increasing in the US but not in other Western countries
• Guns are the most common means of suicide in the US (50%)
• Rates of suicide are highest in states with more gun
Women and men Suicide stats
Men are more likely than women to kill themselves
• Women are more likely than men are to make suicide attempts that do not result in death
• Men are more likely to shoot or hang themselves
• Women more likely to use less lethal means
• The highest rates of suicide in the United States are for white males over age 50
• The rates of suicide for adolescents and children in the United States are increasing dramatically
• Being divorced or widowed elevates suicide
risk four- or fivefold
Risk Factors for Suicide
• Psychological Disorders
o 90% of people who attempt suicide meet diagnostic criteria for a psychological disorder
More than half of those who attempt suicide are depressed
Suicide heritability
Heritability of about 50% for suicide attempts
Social Factors for suicide
o Economic recessions
o Media reports of suicide
o History of multiple physical and sexual assaults
o Perceived sense of burden to others and a lack of social belonging
Psychological Models for suicide
o Ineffective problem-solving
o Hopelessness
o Impulsivity
Preventing Suicide
Talk about it
Hospitalization
Broader Approaches to Suicide Prevention
• Studying suicide prevention within the military
o Higher rates of suicide than the general population
o Programing to encourage and destigmatize help seeking,
o Make highly lethal methods less available
• Keep guns in locked cabinets
• Restrict access to lethal drugs
normalize distress, and promote effective coping
Anxiety
Apprehension/worry over an anticipated problem
Fear
A reaction to immediate danger
What does Fear and anxiety both envolve?
Arousal
o Anxiety – moderate arousal (e.g., restless energy,
tension)
o Fear – higher arousal (e.g., overpowering urge to run)
Anxiety pros and cons
• Absence of anxiety interferes with performance
• Moderate levels of anxiety improve performance
• High levels of anxiety are detrimental to performance
U shape curve
Fear pros and cons
o Fear triggers “fight or flight” response
o In the right circumstance, fear saves lives
o Fear system seems to misfire in some anxiety
DSM-5 TR Anxiety Disorders List
o Specific phobias
o Social anxiety disorder
o Panic disorder
o Agoraphobia
o Generalized anxiety disorder
(5)
Most common psychological disorders
Anxiety disorders
28% of people report anxiety symptoms
• 10th leading cause of disability worldwide in 2015
Specific phobia
Fear of objects or situations that is out of proportion to any real danger
Social anxiety disorder
Fear of unfamiliar people or social scrutiny
Panic disorder
Anxiety about recurrent panic attacks
Agoraphobia
anxiety about being in places where escaping or getting help would be difficult if anxiety symptoms occurred
Generalized anxiety Disorder
Uncontrollable worry