Vestibular system key words
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
41 Terms
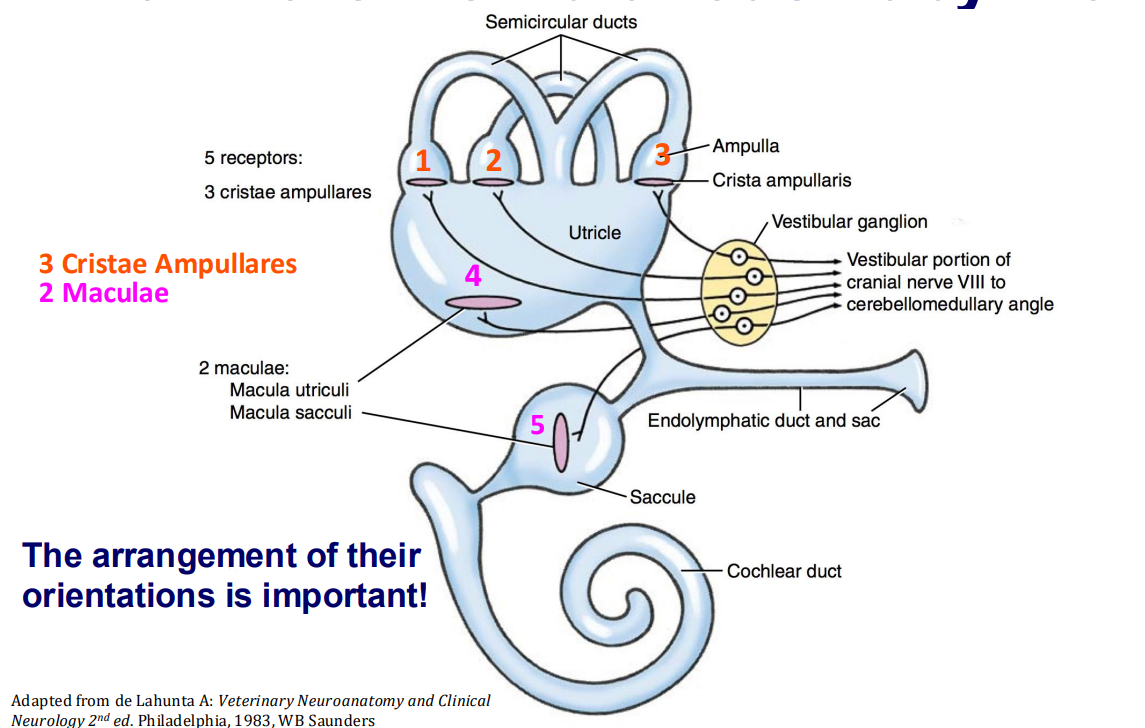
Linear acceleration detectors
Maculae
Utricle → horizontal
macula utriculi
Saccule → vertical
macula sacculi
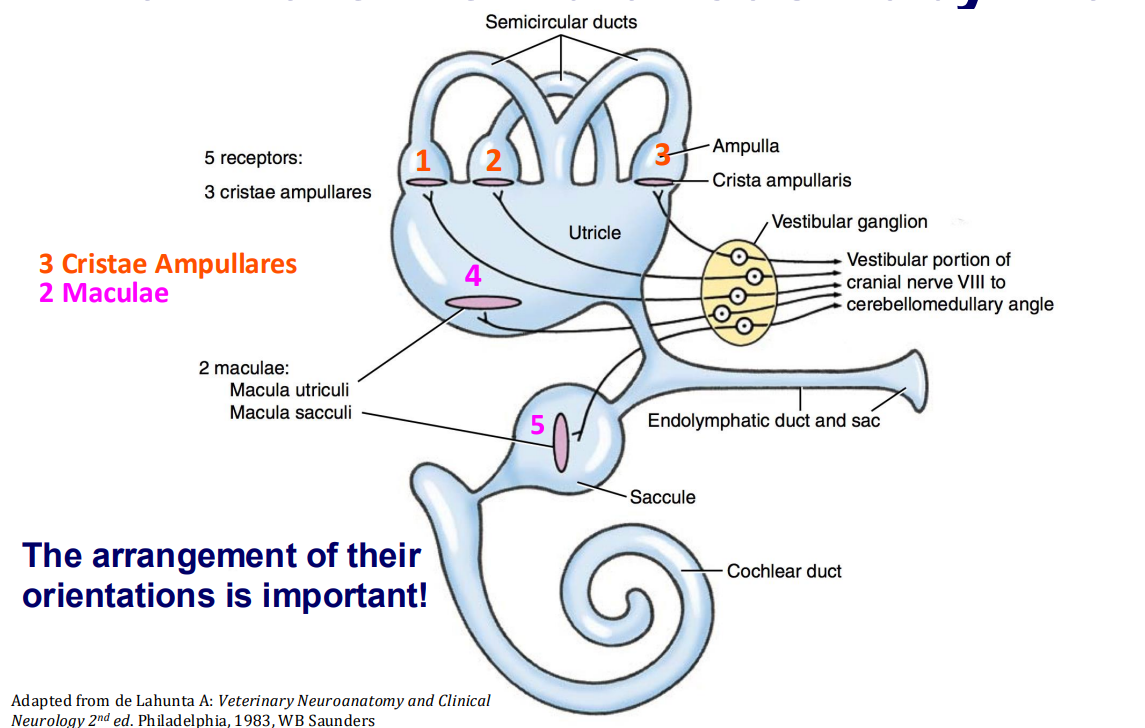
Angular acceleration detectors
Cristae ampullares (3x) within ampullary cupulae
detection of angular acceleration in three dimensions
each cupulae oriented perpendicular to each other
Primary vestibular inputs [3]
Visual
Tactile
Proprioceptive
Peripheral vestibular apparatus connections
Semicircular canals → ampullary cupulae → utricle → saccule → cochlea
Bony labyrinth
Cavity within petrous temporal bone
Membranous labyrinth
Structure within bony labyrinth
Mechanism of receptor hair cells
Head position movement
Fluid (endolymph) moves in opposite direction (inertia) against hair cells
Stereocilia deflected
towards kinocilium (rigid ‘hair’)
depolarisation → excitation
away from kinocilium
hyperpolarisation → inhibition
Hair cell transduces mechanical movement into an electrical signal (action potential)
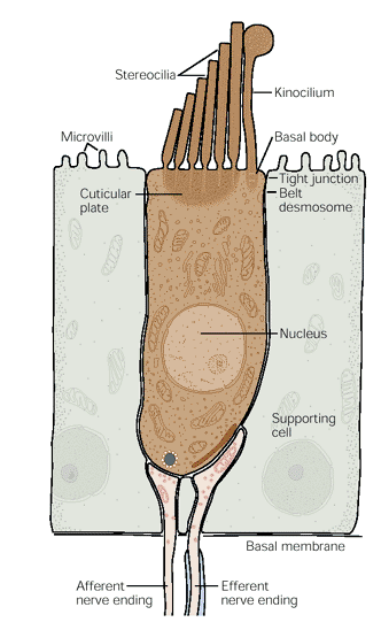
Maculae structure
Neuroepithelium
Hair cells (cilia)
Supporting cells
Gelatinous statoconial membrane
Statoconia (otoliths)
Movement of statoconial membrane displace cilia → cause excitation or inhibition
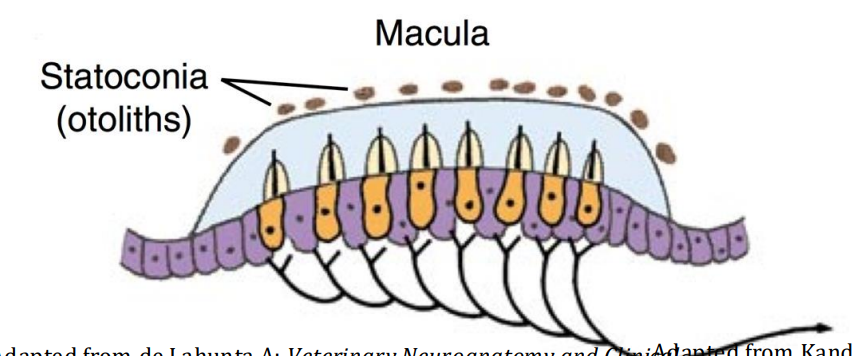
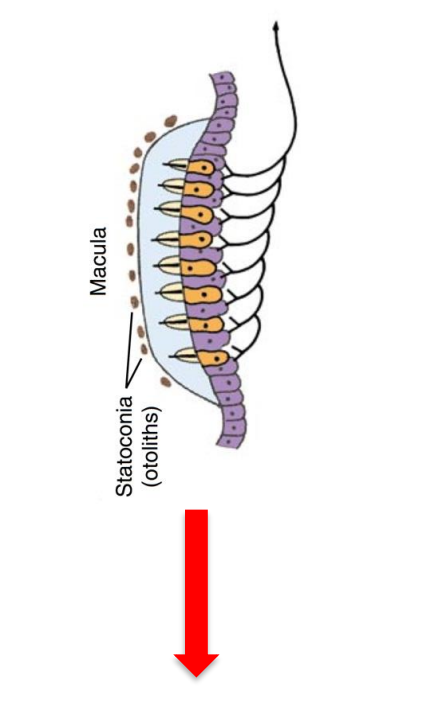
Movement upwards
causes endolymph to move downwards
(saccule → vertical linear acceleration)
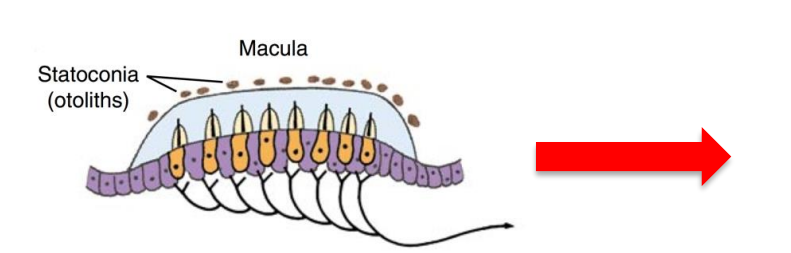
Movement to the left
causes endolymph to move to the right
(utricle → horizontal linear acceleration)
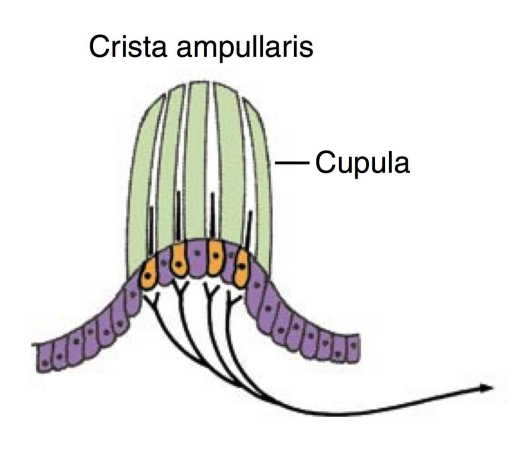
Crista ampullaris components
Neuroepithelium
Hair cells
Supporting cells
Gelatinous cupula (NO OTOLITHS)
Cupula project into endolymph in ampulla of semicircular canal
angular acceleration from head rotation
inertia of endolymph within canal → cupula displaced
Vestibular nuclei paired nuclei [4]
Rostral
Medial
Lateral
Caudal
CNVIII - nuclei in medulla oblongata
Vestibular nuclei inputs [3]
Vestibular nerve
Cerebellum
Spinal cord
Vestibular projections [6]
Cerebral cortex
Conscious proprioception
Spinal cord
Automatic correction in posture (e.g. crossed extensor reflex)
autonomic reflex of body tone
Inhibit contralateral extensors when ipsilateral extensors engaged (ipsilateral flexors inhibited)
Contralateral vestibular nuclei
connecting left and right sides
Cerebellum
Archicerebellum (floccus + nodule) → balance
vestibulocerebellum = flocculonodular lobe
Paleocerebellum (vermis) → proprioception
Reticular formation
Vomiting and cardiovascular centres
nausea, increased sympathetic tone
Extra-ocular muscles → linked to nystagmus
Diseased side of the vestibular system
Animal falls/leads to diseased side
(ipsilateral side)
Cerebellum vestibular projection
Archicerebellum (floccus + nodule) → balance
vestibulocerebellum = flocculonodular lobe
Paleocerebellum (vermis) → proprioception
inhibitory dampening down of signals to ipsilateral vestibular nuclei
Reticular formation vestibular projection
Vomiting and cardiovascular centres
nausea, increased sympathetic tone
Reticular projection extraocular muscles
Medial longitudinal fasciculus (MLF) → white matter tract in brainstem
Links vestibular nuclei of CNVIII to extraocular muscle nuclei
Enables and coordinates synchronised eye movements
conjugate eye movements
Vestibular control of eye position → nystagmus
Nystagmus → rhythmic, oscillatory, involuntary eye movements
Normal/physiological nystagmus
Vestibulo-ocular reflex
Test via moving head to side
Eyes locked onto target until target leaves FOV
Jerky movement of eyes → snaps back to resting position
Abnormal nystagmus
Pathological/spontaneous
Standing still → nystagmus occurs
Lack of vestibulo-ocular reflex
Vestibulo-ocular reflex
When eyes focused on target → receptor cells constantly firing
Increased firing on side towards movement
Decreased firing on side away from movement
Head still → equal firing (dynamic equilibrium)
Movement of head and eye during vestibulo-ocular reflex
Animal test - constant target on the right
Vet physically turns head left
Head turns left → eyes move right
Focus on object on right
Constant gaze on moving target
When focussed object exits FoV → eyes jerk left, back to the centre
Vestibular syndrome
Collection of clinical signs caused by vestibular dysfunction
Not a disease → syndrome
Bilateral vestibular syndrome
Head moves weirdly (bobbles) since both sides affected
Peripheral vestibular syndrome- source of pathology
Vestibular apparatus (inner ear)
Vestibulocochlear nerve
Central vestibular syndrome- source of pathology
Vestibular nuclei
Central vestibular projections
Central vestibular projections [5]
Vestibulospinal tract
Palaeocerebellum (floccus and nodule, vestibulocerebellum)
Proprioception
Medial longitudinal fasciculus
Thalamus (through towards)→ somatosensory cortex
Reticular formation → cardiac and vomit centres
Central V peripheral vestibular syndrome using clinical signs → general points
Horner’s syndrome more commonly peripheral
All other clinical signs can happen with central
Head tilt and ataxia always happen with both
Vestibular syndrome clinical signs [9]
Head tilt
Ataxia
Proprioceptive deficits
Muscle weakness (paresis)
Change in mentation (brain function)
CN deficits
Horner’s
Strabismus
Nystagmus
Strabismus
Deviated eye position WHEN EYE FIXED
Positional strabismus
Ventral strabismus (when head elevated)
Ipsilateral strabismus (if peripheral ipsilateral lesion)
Vertical nystagmus
Up and down beats of eye movement
Positional nystagmus
Changes nature according to head position
Dysconjugated nystagmus
Nystagmus between eyes not coordinated
Spontaneous vertical nystagmus
(can also be horizontal or rotatory)
Eyes involutarily jerk up and down by default
Inducible nystagmus
PATHOLOGICAL
Nystagmus not noticeable at rest
animal has adapted to nystagmus in regular position
When animal put in new position nystagmus appears
Pendular nystagmus
GENETIC/non pathological
Eyeball movements same speed both directions (no jerky movments)
Spontaneous, congenital
Accompanies ocular albinism → cats with blue irises
Unilateral lesion pathological nystagmus
Loss of constant stimulation from side of lesion
No dynamic equilibrium:
Perceived as head rotating away from side with lesion
Lesion on left
Perceived a head rotating to the right
eyes look left and then snap to the right
Peripheral vestibular system summary
Vestibular apparatus (labyrinth)
Vestibular nerve
Central vestibular system summary
4 pairs vestibular nuclei
Rostral
Medial
Lateral
Caudal
Flocculonodular lobe (archicerebellum)
Projections to higher/lower centres
Vestibular syndrome summary
Underlying syndrome → can have many disease causes
Nystagmus may be physiological (normal → pendulous) or pathological
Pathological nystagmus → characterised by direction
Character of nystagmus etc → determine central V peripheral (to determine possible causes)
nystagmus → look towards lesion location (for unilateral lesion)