L26- Ageing of motor function and mobility
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
what is gait
the manner or pattern of how someone walks or moves on foot
in biomechanics and clinical contexts, gait describes the coordinated movements of the limbs and body during walking or running
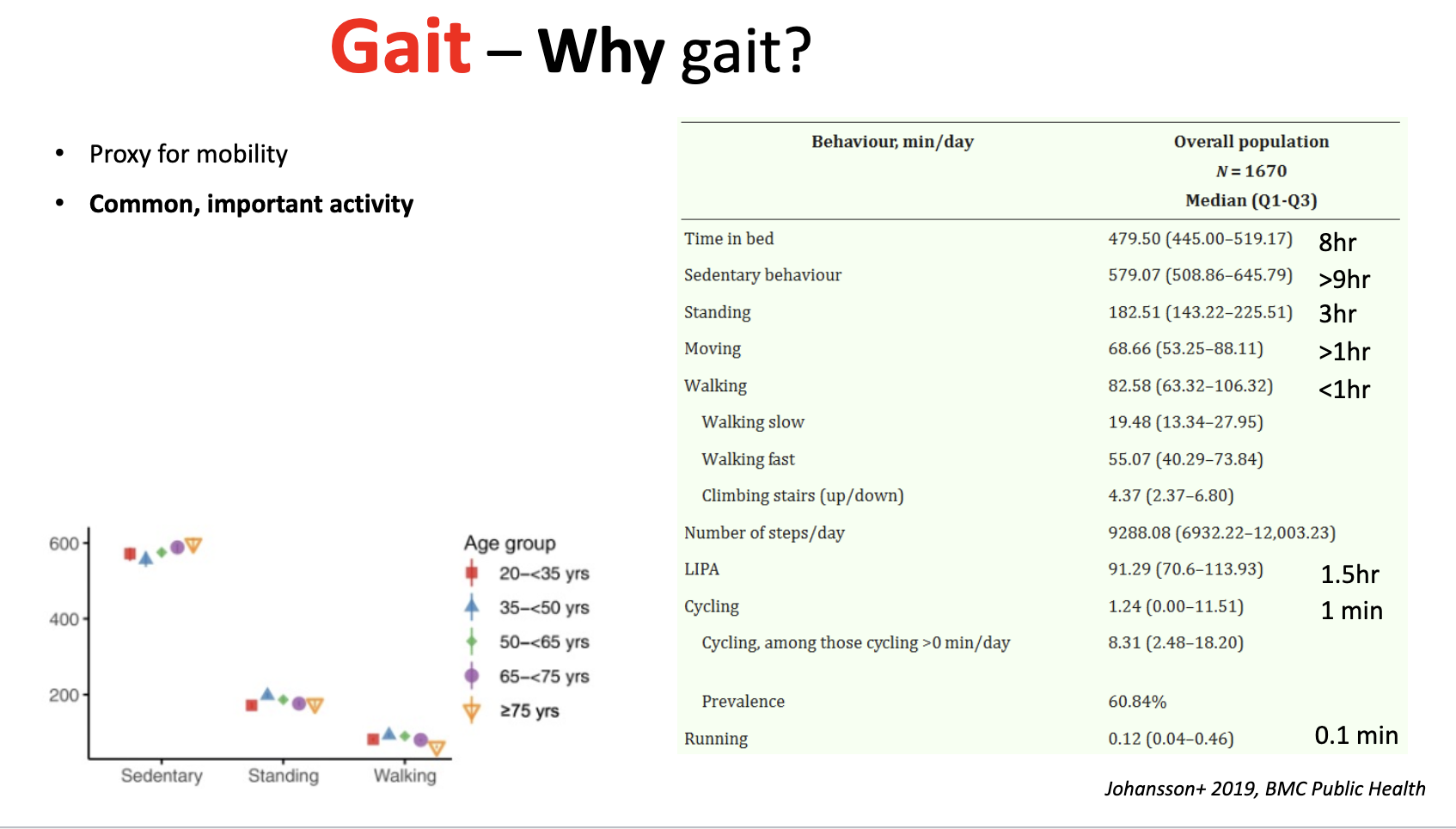
it is proxy for mobility
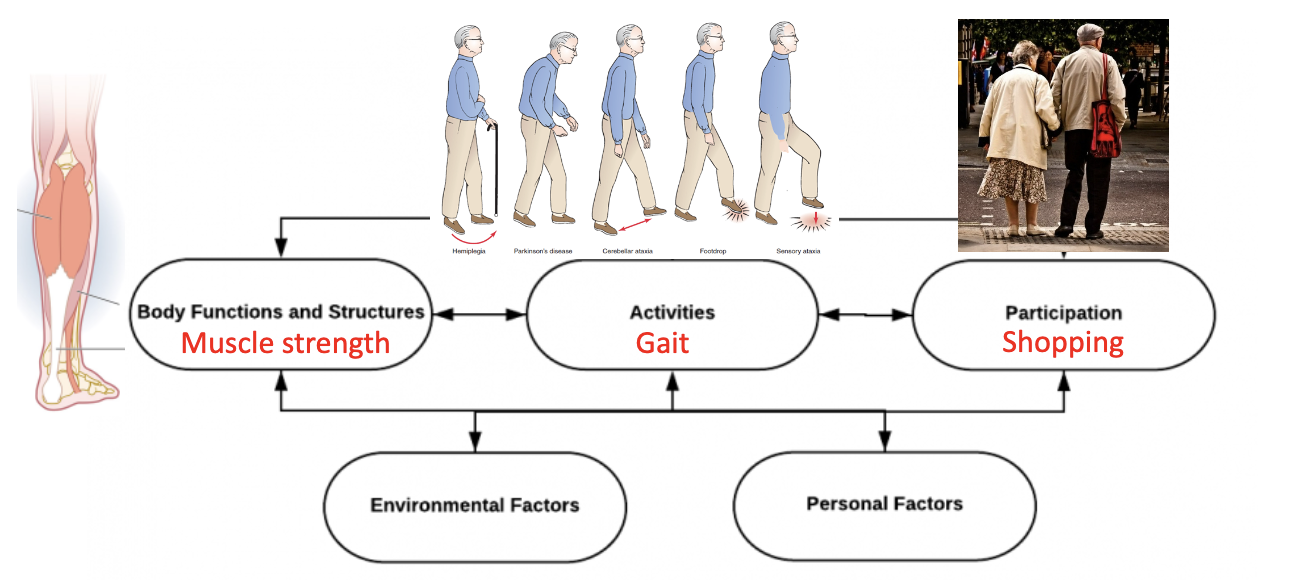
what things affect gait
-Walk or Run
• Speed
• Terrain (uneven)
• Surrounding obstacles
• Weather (slippery)
• Attention
• Muscle strength & stamina
Why is gait important in ageing research?
Proxy for overall mobility and health
Common, everyday activity → easy to measure
Developmentally important
• Related to falls in older persons
• Related to longevity
• Activity that remains with decline
• Cyclic patterns balance
• Complex integration of musculoskeletal and
nervous systems
• Well-developed animal and human models
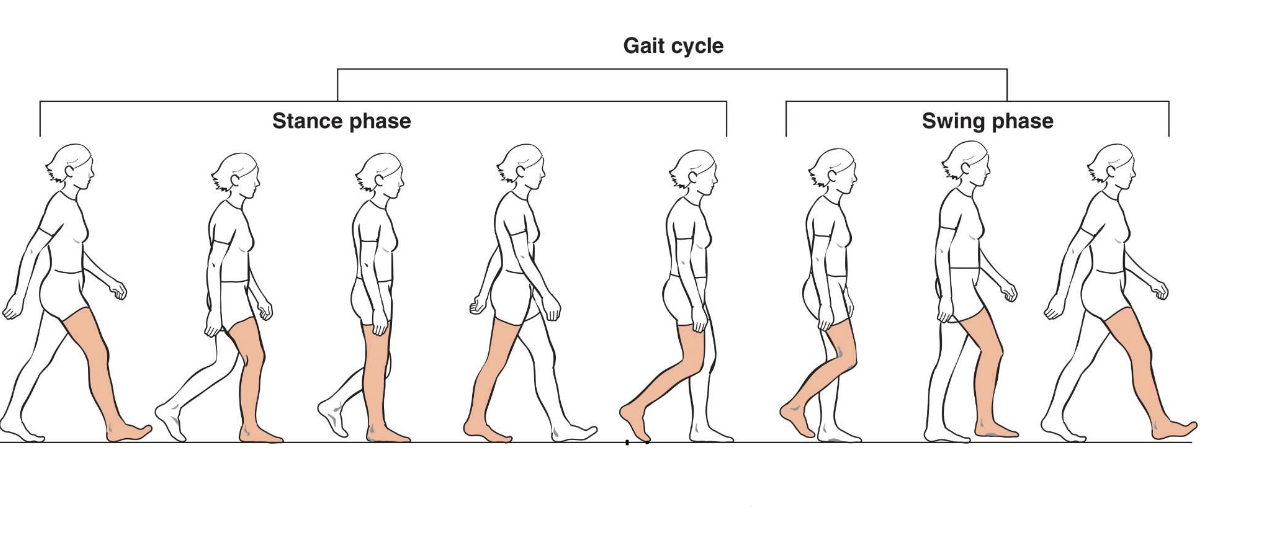
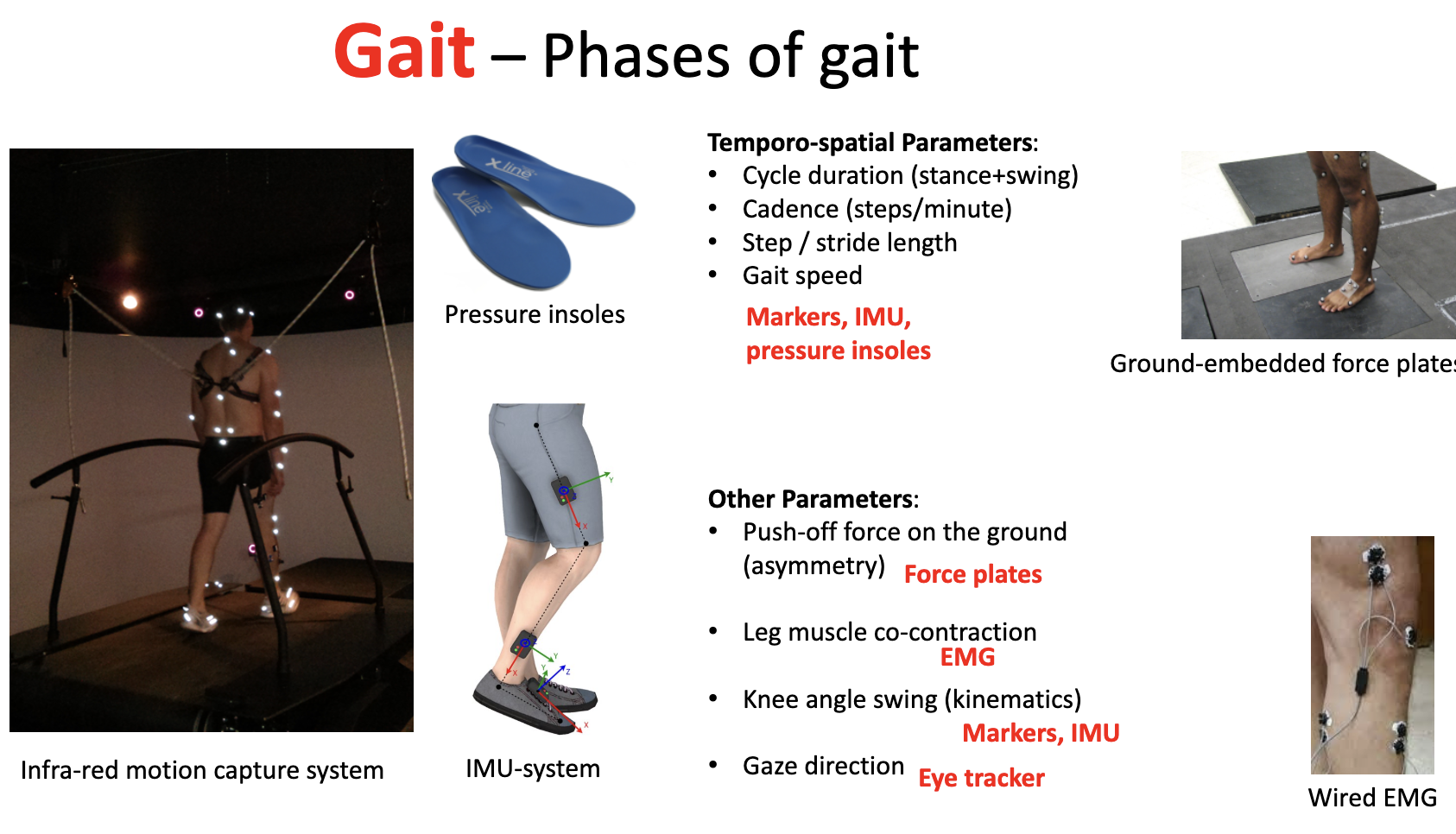
what are the phases of gait
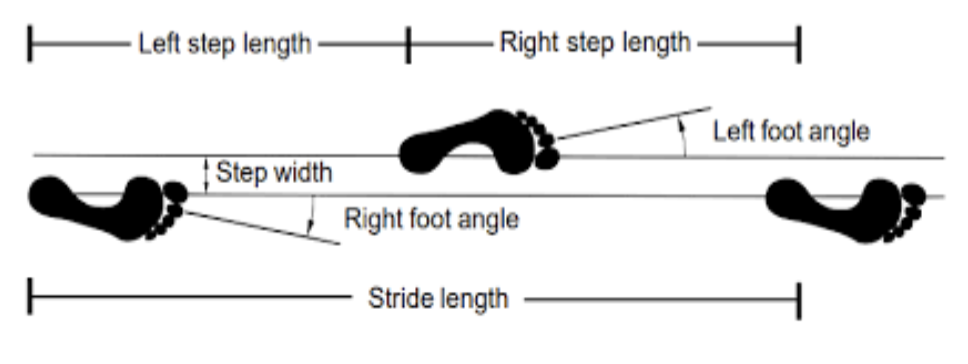
what are the temporo spatial parameters of gait
Cycle duration (stance+swing)
• Cadence (steps/minute)
• Step / stride length
• Gait speed
• Step width
• Asymmetry
• Variability
what are the other parameters of gait (not temporo spatial)
-Push-off force on the ground (asymmetry)
• Leg muscle co-contraction
• Knee angle swing (kinematics)
• Gaze direction
how can the temporo-spatial parameters of gait be measured
Markers, IMU, pressure insoles
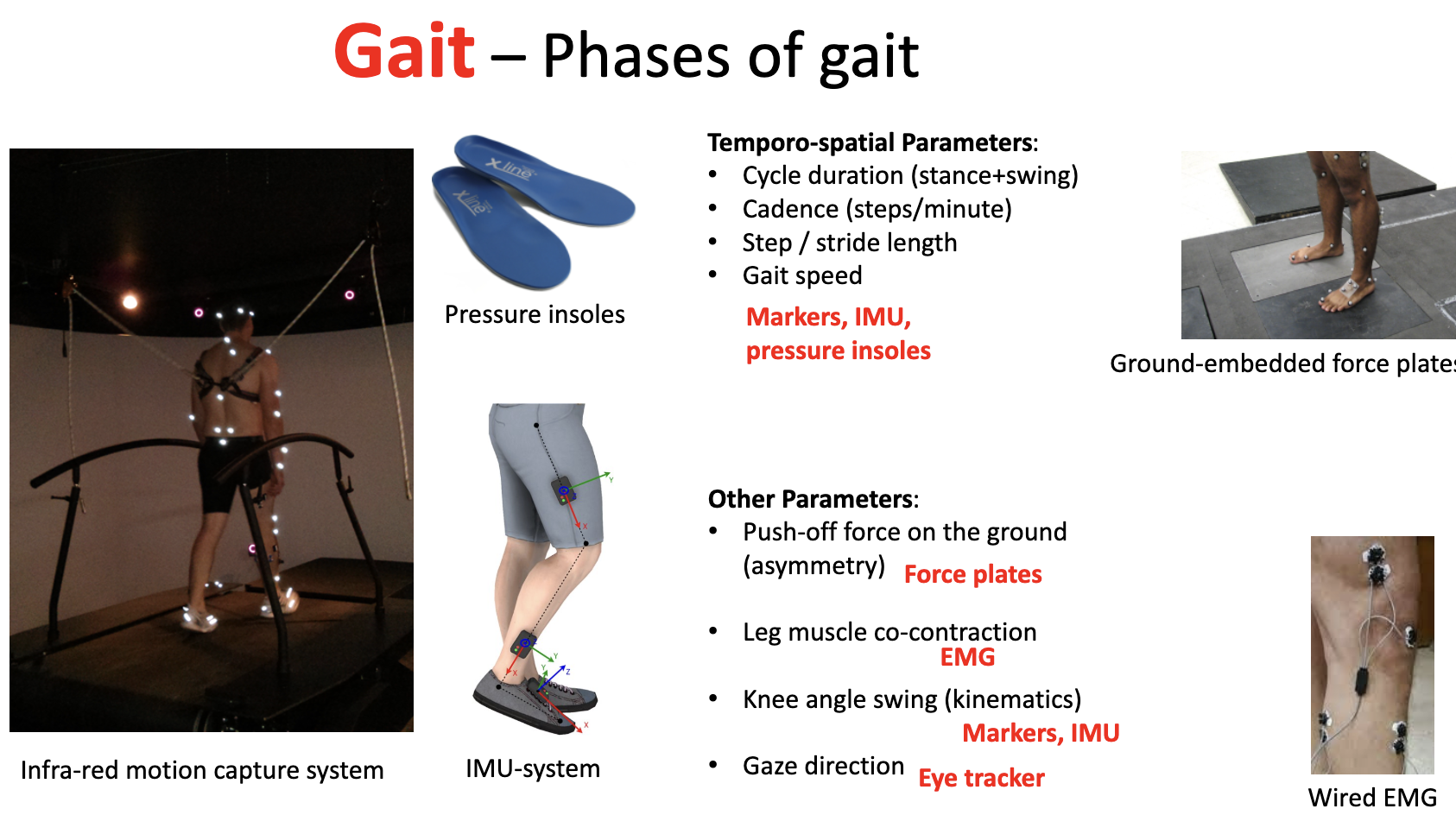
how can the other parameters of gait (not temporo spatial) be measured
Push-off force on the ground (asymmetry)- force plates
• Leg muscle co-contraction- EMG
• Knee angle swing (kinematics)- markers, IMU
• Gaze direction- eye tracker
how many people are affected by gaot issues
35% of adults over 70 yr have clinically diagnosable gait abnormalities
what changes in gait do we commonly see with age
Shorter steps
Longer double support
Shorter swing length
Lower speed
Less push-off power
Hunched posture
Reduced balance/stability
Wider steps
Problems navigating, turning
what causes gait speed to reduce with age
What causes this decline in speed?
- Decline in propulsive muscle strength?
Hiding by shifting ankle and hip muscles?→ sooner fatigued
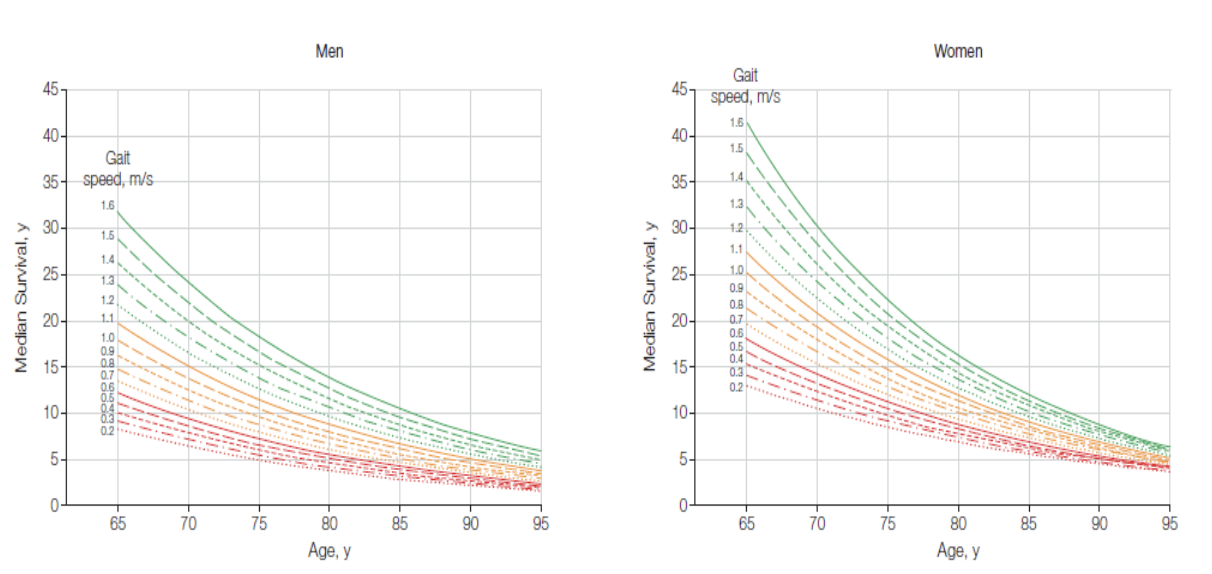
what can speed and age predict
survival
Gait speed is a simple accessible indicator of health/brain function of the older adult
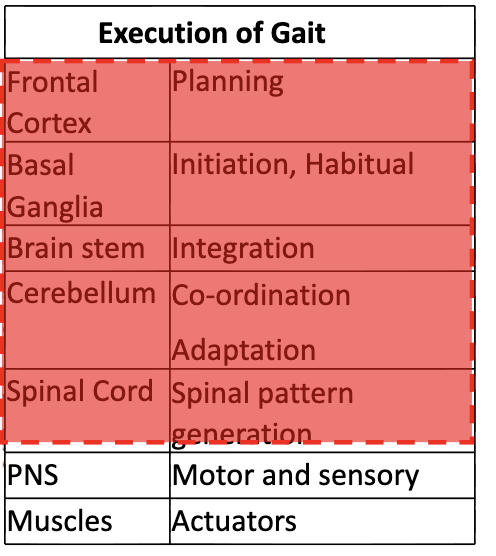
what are the contributions of the CNS to gait control
what bodily functions contribute to feedback of gait control
• Visual
• Vestibular
• Auditory
• Cutaneous
• Proprioceptive
what bodily functions contribute to support of gait control
• CVS
• Pulmonary
• Bones
• Joints
• Ligaments
• Feet
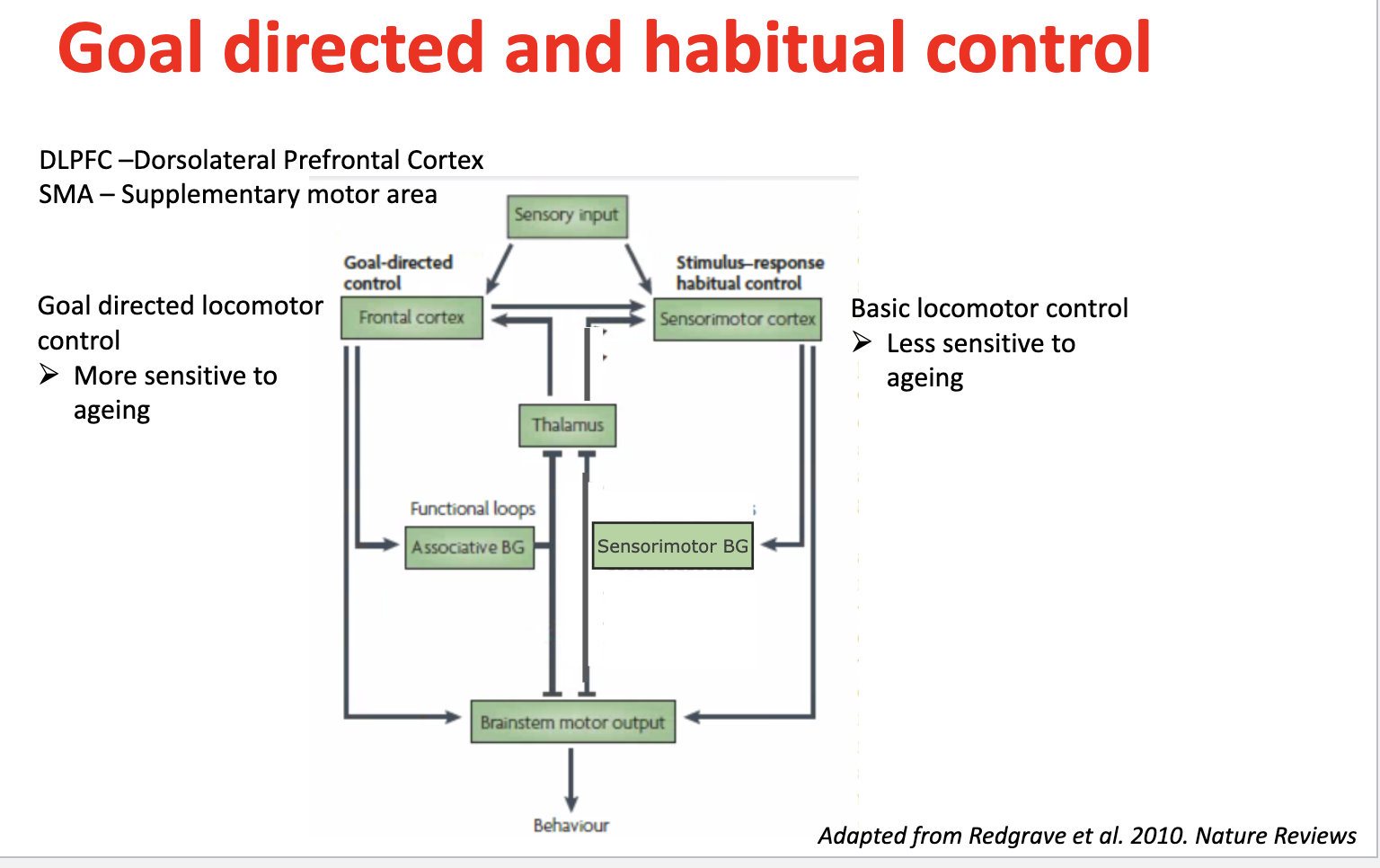
Goal-directed locomotor control — brain regions & ageing effects
Controlled by:
DLPFC (dorsolateral prefrontal cortex)
SMA (supplementary motor area)
Frontal cortex + associative basal ganglia loops
Role: planning, decision-making, flexible movement
→ More sensitive to ageing → declines earlier
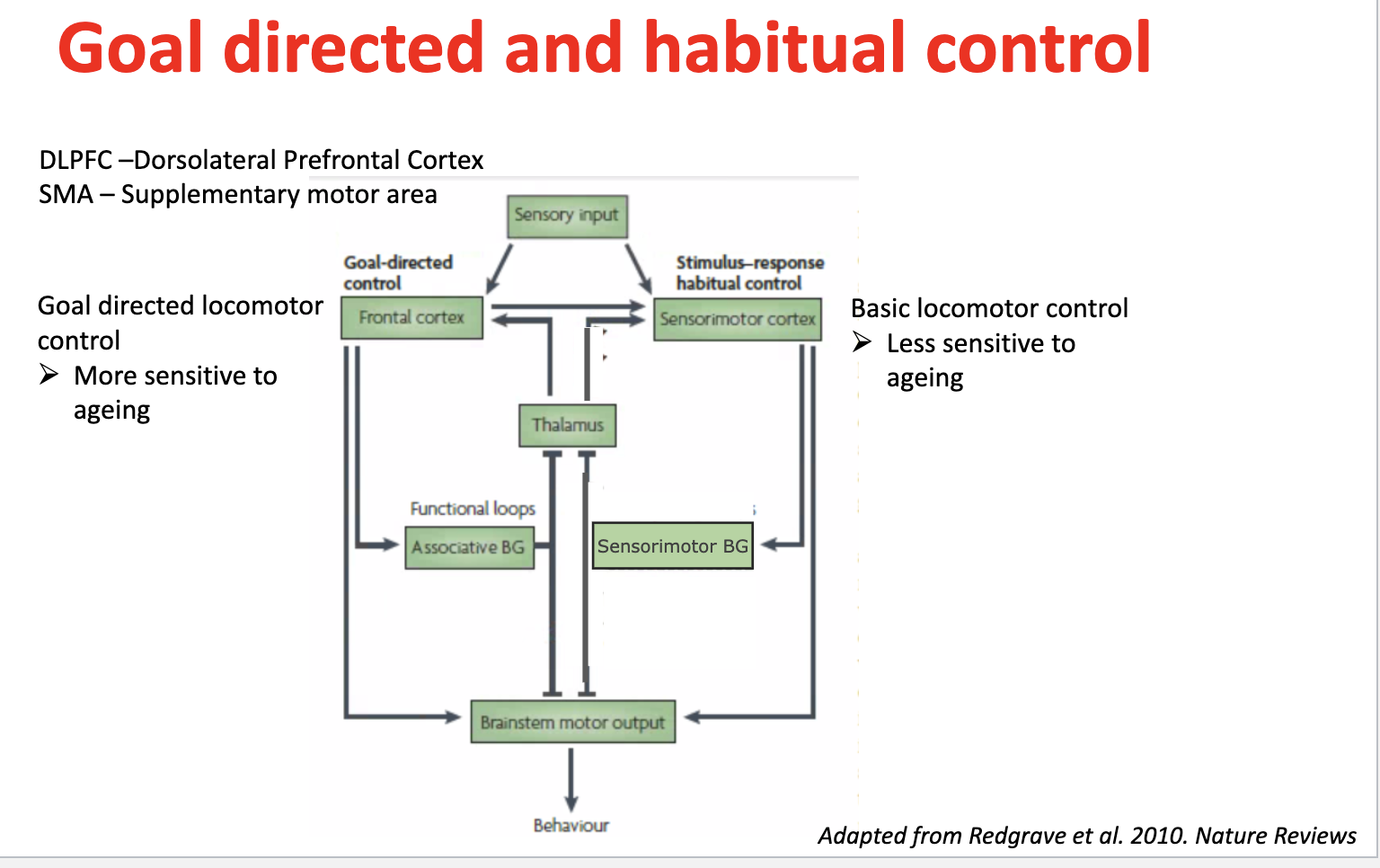
Habitual locomotor control — brain regions & ageing effects
Controlled by:
Sensorimotor cortex
Sensorimotor basal ganglia loops
Role: automatic, stimulus–response movements (habits)
→ Less sensitive to ageing → relatively preserved basic movement
what are some CNS abnormalities in older adults that contribute to mobility and cognitive decline
• White matter hyperintensities
• Brain atrophy
• Small vessel disease
• Cerebral infarcts
• Lewy Bodies
• Neuritic
• Neurofibrillary tangles
how is cognition in gait control demonstrated
• Continuous gait disturbance
• Episodic (freezing of gait)
what is cognition in gait control assed by
• Association task
• Dual-task protocols
what is the dual task principle in gait control
Walking uses shared cognitive resources
When doing a second task (e.g. counting + walking):
↓ cognitive performance (more mistakes, slower responses)
↓ gait performance (reduced walking speed)
→ Called dual-task interference
→ Shows gait requires cognitive input, not just automatic control
What does dual-task walking demonstrate about cognition and gait?
Example tasks: naming animals, counting backwards
Gait speed ↓ under dual-task conditions
Strong link between gait speed and executive function + attention
Demonstrates in real-time:
Attention/working memory used to compensate
Task prioritisation (executive function)
Limits of compensation
→ Sensitive to task difficulty → useful for detecting cognitive decline
what is the risk of dual task walking
falling
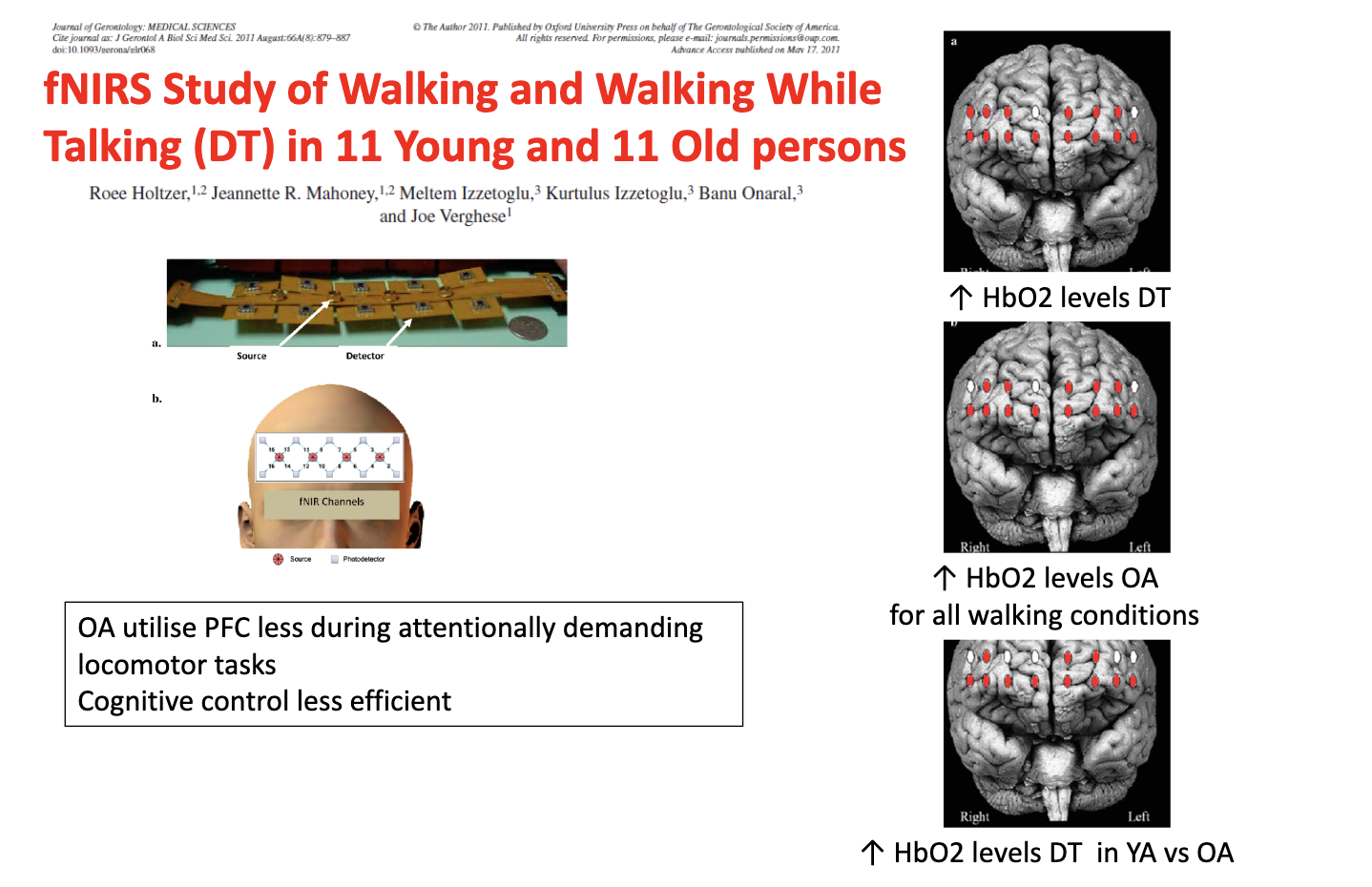
what 3 ways ca brain activity during walking be measured
1. Functional near-Infrared spectroscopy (fNIRS)
measures oxygenated and deoxygenated haemoglobin
2. Electroencephalography (EEG)
measures voltage changes
3. Functional magnetic resonance imaging (fMRI):
imagined walking measures changes in blood oxygenation level
What does the fNIRS study show about brain activity during dual-task walking in young vs older adults?
Dual-task (walking + talking) → ↑ PFC activity (↑ HbO₂)
Older adults (OA):
↑ HbO₂ across all walking conditions
BUT less efficient PFC use
Reduced cognitive control
Young adults (YA):
Greater PFC activation specifically during dual-task
→ Ageing = less efficient neural recruitment + compensatory overactivation
what findings have been found correlating gait speed with cognitive decline
gait speed predicts dementia
gait speed differentiates dementia disease subtypes
gait speed predicts MCI-mild cognitive impairment
faster gait- associated with slower cognitive decline
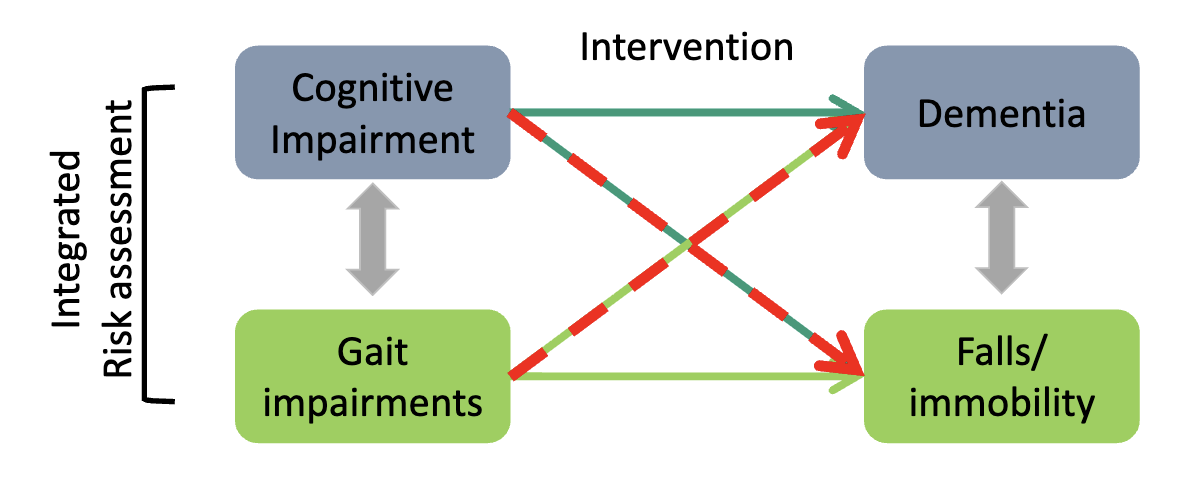
how does gait and cognition interact
→ Gait and cognition are bidirectionally linked; both predict dementia and falls → assess together and target both in interventions.
what are our gaps in knowledge regarding gait and ageing
• How gait changes during the lifespan and age- related diseases – what is normal?
• Which gait deviations are biomarkers for different diseases?
• Underlying mechanism from neuropathology to gait impairment not clearly understood
• How brain reserve compensates for neuropathology
what is balance
the ability to control the position of your body above your feet
keeping yourself upright and not fall

what is stability
the ability to resist or recover from disturbances to prevent a fall
disturbances can be internal or external
static- standing
dynamic- moving
what are some facts regarding balance related to falls
1 in 3 people above 65 yrs of age fall yearly
Increases to 50% of those above 80 years of age
Falls are leading cause of injury in older persons
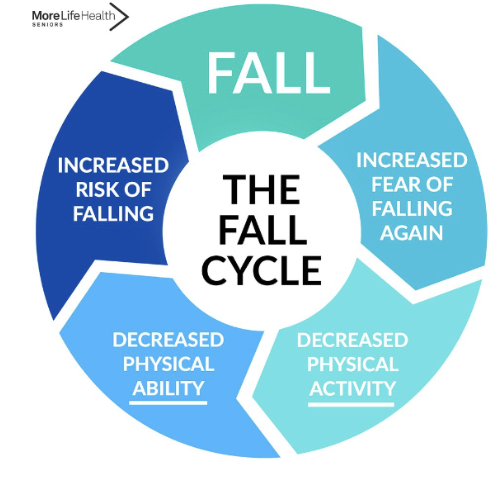
what is the fall cycle
increased fear of falling again
decreased physical activity
decreased physical ability
increased risk of falling
fall
cycle repeats
what is used to make a clinical assessment of balance
the berg balance scale
14 items, 15-20 mins
Assesses changes in static and dynamic sitting and standing balance
No reactive balance
No specific balance problems (one score)
Limited sensitivity: 5-point scale
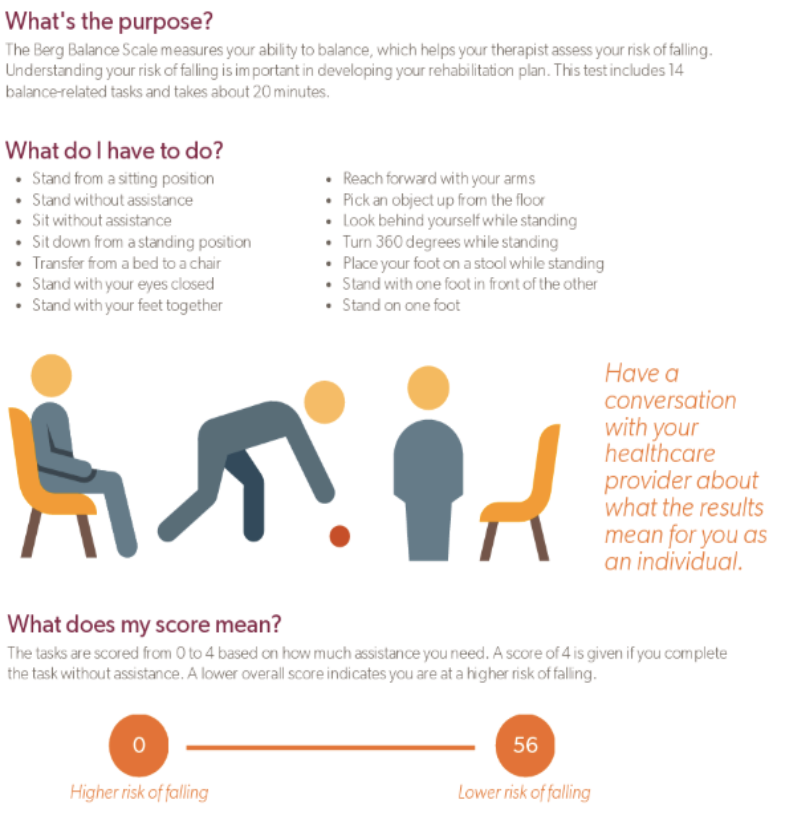
What clinical tests are used to assess balance?
short physical performance battery / SPPB → includes 30s sit-to-stand
Berg Balance Test → gold standard, 14 static + dynamic tasks, score 0–4
Timed Up & Go (TUG) → mobility test requiring static + dynamic balance, scored on time
Tinetti / POMA → assesses STS + gait, rates symmetry & trunk posture
Single Leg Stance (SLS) → ability to stand ≥5 seconds
Functional Reach Test → distance reached (inches)
What aspects of balance do these tests measure?
Combination of static + dynamic balance
Functional tasks:
Standing
Walking
Sit-to-stand (STS)
Assess:
Mobility
Postural control
Gait performance
Symmetry & trunk control
→ Mostly performance-based scoring
What are the limitations of clinical balance assessments?
Subjective scoring
Non-specific to balance systems
Not sensitive to change
Poor for guiding targeted interventions
Limited distinction: standing vs movement
Do NOT assess reactive balance (no perturbation/recovery testing)
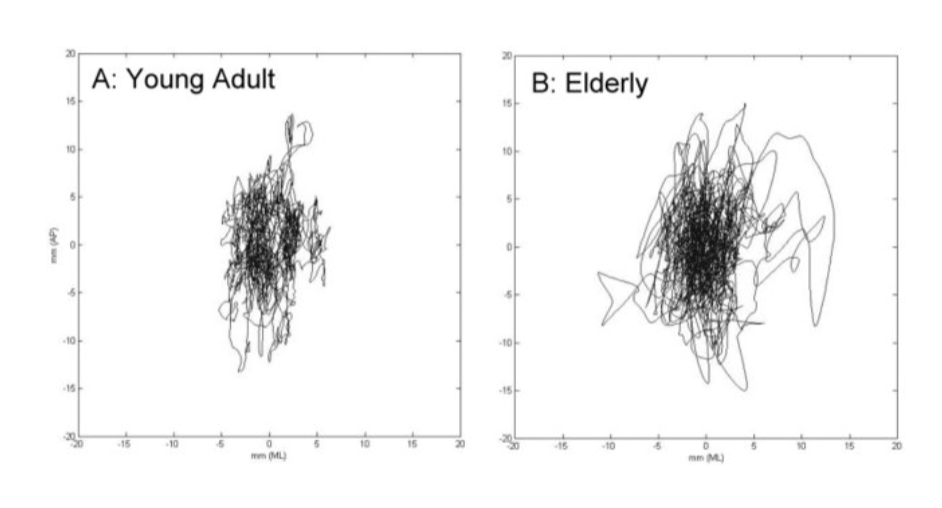
How is balance assessed biomechanically during standing?
Postural control assessed via:
Body trajectory / sway
Challenges:
Many interacting variables
Complex relation between motion and stability
→ Focus = control of COM relative to base of support (feet)
How is balance assessed biomechanically during walking?
Measures of dynamic stability:
Step variability
Step width (↑ width = larger support base)
Margin of stability (MoS)
(Lyapunov exponents – less commonly used)
Limitations:
Ambiguous interpretation
Internal variability
Requires periodic movement
How is reactive balance assessed in perturbed walking?
Recovery response after perturbation
Key measures:
Number of steps to return to baseline
Margin of stability (MoS)
Characteristics:
Discrete events (clear baseline vs perturbation)
Requires full-body motion capture
→ Captures real-world balance recovery ability
How is reactive balance (recovery response) experimentally assessed?
Perturbations applied during standing or walking:
Standing:
Cable-release perturbations
Robot-controlled moving plate
Walkway:
Obstacles from floor
Disappearing floor
Slippery surface / moving tiles
→ Used to assess balance recovery strategies after perturbation
What perturbation methods are used in treadmill-based balance assessment?
Objects on belt
Cable pulls (ankle or pelvis)
Active orthosis / boot
Split-belt treadmill
Belt acceleration / deceleration
Sideways treadmill translation
→ Used to create controlled mechanical perturbations during walking
What non-mechanical perturbations are used to assess reactive balance?
Visual perturbations (VR screens, cues)
GVS (galvanic vestibular stimulation)
Vibrations
→ Target sensory systems involved in balance control
→ All methods assess reactive balance (ability to recover after perturbation)
how does postural control change with age
there is an increase in postural sway
how does dynamic balance change with age
increase in step width
increase in step variability
body closer to / more within support area
what are our gaps in balance and ageing
• How balance changes during the lifespan and age- related diseases – what is normal?
• How to best assess balance to identify fall-prone individuals to offer fall training
• What are the underlying mechanisms of different balance problems?