Concept of metabolism - hepatic A&P 5
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
Liver - internal anatomy
Accessory organ of GI tract along with the pancreas and gall bladder
Vascular organ
Complex venous, arterial and bile system
Hepatic blood supply
hepatic artery
hepatic vein
hepatic portal vein
Hepatic blood supply - hepatic artery
branch of aorta; brings oxygenated blood to the liver (goes into liver)
(400 ml/min)
Heaptic blood supply - hepatic vein
returns deoxygenated blood from the liver to inferior vena cava (goes away from liver)
which will then move to the superior vena cava, to the right atrium, to the right ventricle
Hepatic blood supply - hepatic portal vein - very important!!!
Union of veins bringing deoxygenated blood from spleen, stomach, esophagus, pancreas, intestines (GI Tract) allll up into the liver
Rich in dissolved nutrients from these areas (food we consumed)
Contains toxins and medications - within blood supply of the hepatic portal vein - need to be removed by liver through metabolism!!!
Blood enters liver where the portal vein divides into sinusoids!
Specialized capillaries within hepatocytes
Liver functions:
Removes toxins from bloodstream
Metabolizes nutrients from food
Removes bacteria from blood
Stores sugar, vitamins and minerals
Regulates blood clotting
Produces bile to digest fat and absorb vitamins A, D, E, K
Produces protein (albumin!)
Conjugates bilirubin
Liver - production of bile/ bile salts
Bile – bitter, yellow/green fluid produced by liver (hepatocytes)
Bile salts – solid salts within bile that aid fat digestion
Needed for digestion of fat and absorption of fat-soluble vitamins A, D, E, and K
Liver - metabolism of drugs
almost ALL drugs detoxified and metabolized in the liver
drug induced liver toxicity a concern with many medications
helps to detoxify and metabolize!!
Liver - metabolism of alcohol
80-90% of ingested alcohol metabolized here
Alcohol can disrupt other functions of the liver
consumption of alcohol can damage the ability of the liver to have its phagocytic function - important in preventing bacteremia - increase their risk of septicemia
alcohol use disorder - malnutrition and anorexia
Metabolism and synthesis of glucose
Glucose – main fuel source for brain, muscle and renal tissues
Liver contributes to the stability of blood glucose
Glycogenolysis – breakdown of glycogen (which is stored in the liver) to glucose
When more glucose is needed!!
Gluconeogensis – ability of the liver to “make new glucose” from non-carb sources (protein, fat)
Glycogenesis – formation of glycogen from glucose
When glucose is adequate, and more is available
Metabolism and glucose - glycogenolysis:
breakdown of glycogen (which is stored in the liver) to glucose
When more glucose is needed!! - don’t have glucose available
Metabolism and glucose - Gluconeogensis:
ability of the liver to “make new glucose” from non-carb sources (protein, fat)
Metabolism and glucose - Glycogenesis:
formation of glycogen from glucose
When glucose is adequate, and more is available (extra) - stored for later use
Liver - synthesis of nutrients
Proteins
Fats
Vitamins
Clotting factors
Liver - synthesis of nutrients - proteins
takes amino acids (AA) and turns in to proteins
Albumin, most globulins, enzymes
Liver - synthesis of nutrients - fats
synthesized from carbohydrates and protein in liver
Liver can make fat
Need some fat in body for energy
Fat absorbed from intestines as triglycerides
Affects cholesterol levels - pt with liver failure/cirrhosis, will see alterations in their cholesterol levels
Liver - synthesis of nutrients - vitamins
A, D, E, K
B 12
Liver - synthesis of nutrients - clotting factors
prothrombin, fibrinogen - controlled by the liver
Clotting cascade begins here in the liver - not functioning properly, will see alterations in pts ability to clot - won’t have ability to clot quickly - INR will increase (dependent on vit. K)
Dependent on Vitamin K production and storage!!
Liver - protein metabolism
Within hepatocytes, amino acids (proteins) are converted from ammonia to urea - if liver not functioning properly, lose ability to convert ammonia to urea
Ammonia is very toxic to the central nervous system
Especially the brain!
hepatic encephalopathy!!!!
Liver - removes bacteria from the blood
Filtration of blood and removal of bacteria and particulate matter
The Kupffer cells are phagocytic macrophages
Liver - bilirubin elimination - review
bilirubin is a component of hemoglobin breakdown
Begins with breakdown of RBCs (old or hemolyzed) (in spleen)
Hemoglobin broken down into - heme (waste) and globin (protein returned to blood)
Heme is then converted to biliverdin and then quickly to bilirubin (bilirubin makes the pigment color of bile)
Liver - bilirubin elimination cont. - unconjugated
bilirubin travels in the bloodstream to the liver: this is called UNCONJUGATED/FREE/INDIRECT bilirubin
This unconjugated bilirubin travels attached to albumin - its life raft!! - needs this life raft to travel through blood
Once in liver, the bilirubin is “freed” from the albumin and enters the hepatocytes
Liver - bilirubin elimination - conjugated
Bilirubin in the hepatocytes (liver) is then converted to DIRECT/CONJUGATED bilirubin
Conjugated means “united together”
The bilirubin unites to an enzyme as part of this process
The conjugated bilirubin is then secreted from the liver as part of bile
Bilirubin gives bile it’s color
Stored in gall bladder
Eventually enters GI Tract
What does it mean for bilirubin to be unconjugated
this is bilirubin that is traveling in the bloodstream to the liver
it attaches to albumin
What does it mean for bilirubin to be conjugated:
conjugated within the liver itself!!
this is bilirubin that has made its way into the liver, unattached from albumin, enters the hepatocytes
once in the hepatocytes, the bilirubin unites to an enzyme as part of process
conjugated bilirubin is then secreted from the liver as bile
Liver - When bilirubin enters intestines, bacteria converts the bilirubin to urobilinogen..
Urobilinogen is formed in the intestines by bacterial action on bilirubin. About half of the urobilinogen formed is reabsorbed and taken up via the portal vein to the liver, enters circulation and is excreted by the kidney
kidneys take important role in the excretion and removal of some of our bilirubin
Liver - Or it converts the bilirubin to stercobilinogen
Stercobilinogen is formed from the half of the urobilinogen that is not reabsorbed. Stercobilinogen gives feces its color. This is then excreted through intestines and is eliminated as feces. - poop!!!
if bilirubin not eliminated by kidneys, its eliminated by our GI tract
Liver - jaundice
A symptom, not a disease itself!!!
Symptom we see due to elevated bilirubin in blood!!!!
Visible sign of underlying disease process of the liver or associated organ
Usually seen when total bilirubin levels in the blood reach 2.5-3 mg/dL
(Normal = 1.2 mg/dL or less)
can appear first in the sclera but can appear throughout the pts skin
Jaundice causes: hemolytic or PRE-HEPATIC
Unconjugated bilirubin traveling TO liver!
Cause of jaundice due to:
Hemolytic/Pre-hepatic reasons – “before the liver” – not really liver disease
An increased destruction (hemolysis) of RBC’s – “too much” for the liver to handle
Causes:
•Hemolytic Anemia
•Autoimmune or transfusion hemolysis
•Hemolytic processes caused by Sickle Cell Disease or Thalasssemias
•Septicemia - infection throughout body - causes our spleen to enlarge - starts to break down our cells such as RBC at a higher level than it should
•Newborns
Labs: Increased total bilirubin and indirect/unconjugated bilirubin (unconjugated before it gets to the liver so makes sense!!)
Jaundice cause - hepatocellular or INTRAHEPATIC
This is where/when bilirubin becomes conjugated!
Cause of jaundice Hepatocellular/Intra-hepatic – problem within the liver – liver disease
Cirrhosis, hepatitis, cancer, drugs (pharmaceuticals/illicit)
Either liver is unable to:
Take in the increased bilirubin from the blood - coming in as unconjugated
OR
Is unable to conjugate or excrete the bilirubin once it enters the liver
Labs: Increased total bilirubin and either increased indirect/unconugated (if the problem is occurring when the bilirubin is just getting into the liver and has had yet to conjugate) or direct/conjugated bilirubin
Jaundice - obstruction or POST HEPATIC
Bilirubin ready to leave the liver as part of bile
Obstruction of bile flow/Posthepatic “beyond the liver”
Obstructed outflow of bile from the liver
Ex: Cholelithiasis (gall stones), biliary tract tumors, cancer of gall bladder, pancreatitis (comes distal to the gallbladder)
Will cause clay/light colored, frothy stools
Bilirubin that was conjugated in the liver cannot leave the liver and accumulates in the liver and enters the blood
Labs: Increased total bilirubin or increased direct/conjugated bilirubin
S&S of jaundice:
The manifestations will depend on the underlying cause
Example:
Hemolytic anemia
Cirrhosis
Gall stones
Collaborative care for Jaundice:
Treat causes and complications
Hemolytic anemia (pre hepatic)– Administer iron or blood transfusions
Cirrhosis (intra hepatic)
Gall Stones (post hepatic) – cholecystectomy
The liver is a large organ..
also very vascular
has consistently large volumes of blood flowing through it
has a right and a left lobe - the right being larger than the left
The liver is surrounded by the:
Glisson’s capsule
What is the Glisson’s capsule:
the liver is surrounded by it
tough capsule that helps to protect it from internal damage and trauma that a pt might sustain
(a laceration to the liver could be life threatening due to it being very vascular - could result in hemorrhagic shock)
What is seated right below the liver?
the gallbladder
has bile ducts which flow up into the liver
The gallbladder is responsible for:
releasing the bile which is initially created in the liver
Blood flow review:
venous blood flows up into the larger hepatic vein (at the very top of the liver), then dumps into the vena cava
Aorta delivers the oxygen rich blood down into the liver via the hepatic arteries
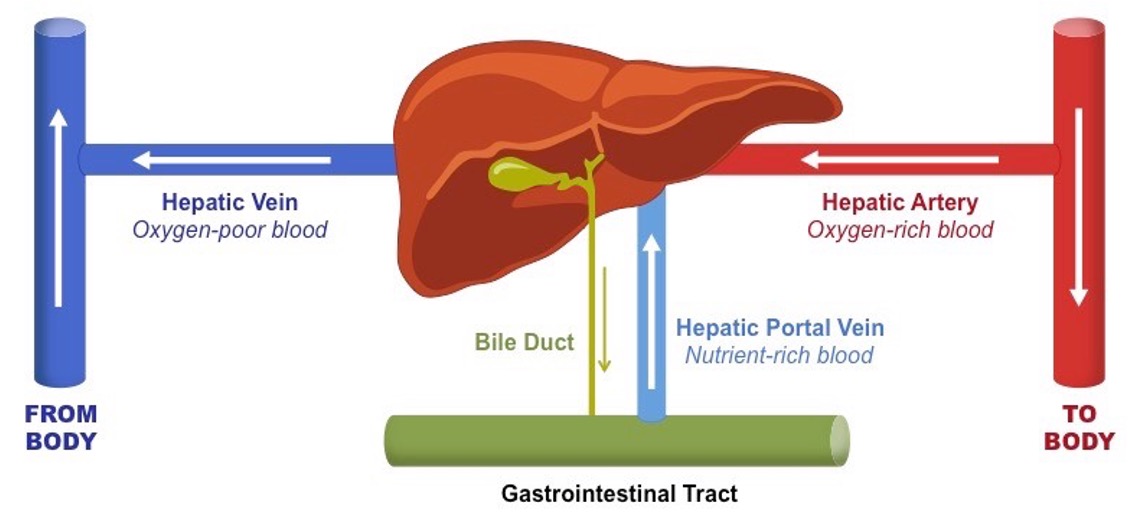
Hepatic circulation image:
aorta sending that oxygen rich blood out to our entire body
hepatic artery which branches off of the aorta and goes into the liver again delivering oxygen rich blood
blood supply from GI tract goes up into the hepatic portal vein - nutrient rich blood
gallbladder releases bile through bile ducts, goes down into the GI system/GI tract where it works to dissolve and break down fats - metabolism of fats!!
venous blood goes out of the liver, back to the heart through the hepatic vein - oxygen deprived blood - goes to inferior vena cava, superior vena cava, right atrium, right ventricle, yada yada
Liver lobule:
within them are sinusoids that have large gaps which allow for nutrients and bacteria to drain within the liver
Liver lobules are the functional hexagonal units of the liver, consisting of plates of hepatocytes radiating from a central vein toward portal triads. Within these lobules, Kupffer cells (KCs) are specialized
Liver lobules have Kupffer cells:
phagocytic macrophages
important in eliminating and cleansing bacteria
stationary macrophages located in the sinusoidal lumen, serving as the body's largest population of tissue macrophages
At the lobular level and within the sinusoids, our liver…
metabolizes products
works to release and produce albumin
produces bile
Bile (produced by the liver) includes:
some cholesterol, electrolytes, bile salts
comes from the hepatocytes themselves
without bile we wouldn’t be able to dissolve our fats or absorb our fat soluble vitamins A, D, E, K
Once conjugated, bilirubin travels how:
From the intrahepatic bile ducts, to the gallbladder, to be released into our intestinal tract
Bilirubin metabolism summarized:
Spleen - responsible for housing many of our blood cells including our old RBCs
RBCs get broken down or destroyed as they’re old - producing and breaking apart that hemoglobin into heme and globin
Travels UNCONJUGATED via albumin through our bloodstream into our liver
As it goes into the liver, starts out unconjugated but then gets conjugated
CONJUGATED bilirubin is then excreted into the bile duct, into our gallbladder
Goes out of the gallbladder, secreted into the intestines
CONJUGATED bilirubin goes into the small intestine, is then converted into stercobilinogen
Half of that is going to stay within the intestines and half goes back up into the portal vein and then is excreted out through the kidneys (urobilinogen)
Vitamin K deficiency leads to…
increased INR - takes longer to clot
What does it mean for the liver Kupffer cells to be phagocytic macrophages?
they filter blood, remove 80-90% of bacteria, toxins and cellular debris, ensuring clearance of pathogens
so when someone drinks too much and this phagocytic function isn’t as efficient, less bacteria is being removed so they are now at higher risk for septicemia
Why in the post hepatic reasons for jaundice is our stool going to be frothy?
Fat in the stool - wasn’t able to be metabolized and broken down