Initiation and propagation of the heart beat
1/34
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
35 Terms
Due to myogenic property of the heart
beat without neurl input
can perform experiments of dead frog
but must be recently deceased
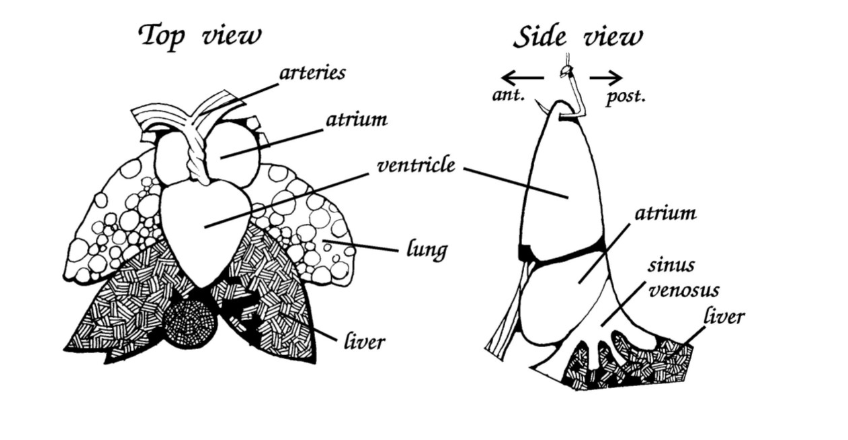
Frog heart anatomy
two atria
single ventricle
sinus venosus
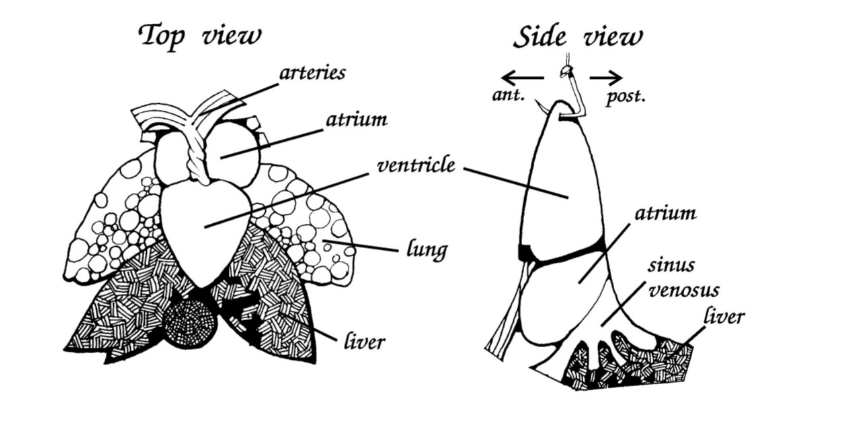
Even though has a single ventricle
loosely compartmentalised→ keeps oxygenated blood separate
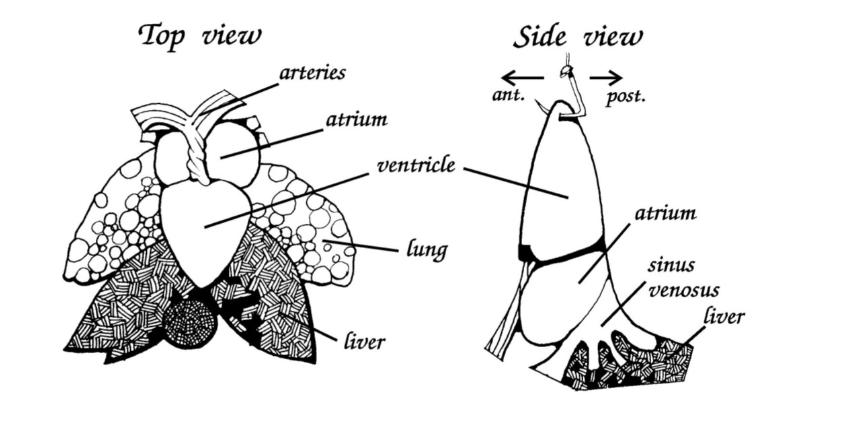
Sinus venosus
contains pacemaker region
equivalent to SAN in mammals
Antechamber created by the large veins entering the back of the heart
AVN in the frog?
no
but
there is slowly conducting pathways from the atrium to the venticle through the fibrous ring
Purkinje fibres?
none
Care of the heart during the epxeriments
heart moist
add Ringer’s solution (pseudophysiological extracellular solution)
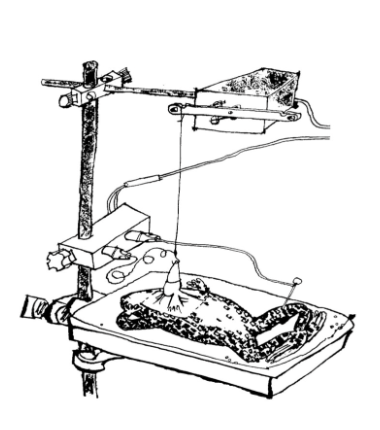
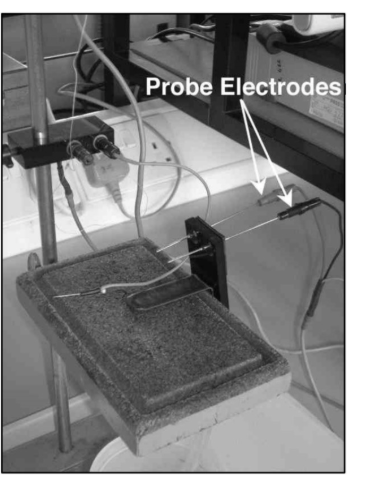
Heart pulled out of the chest cavity and attached to mechanical transducer for recordings
BUT THIS MEANS→ atria must pump blood upwards against gravity
THEREFORE: helpful to periodically discounnet pin from electrode and allow heart to lie back in chest cavity
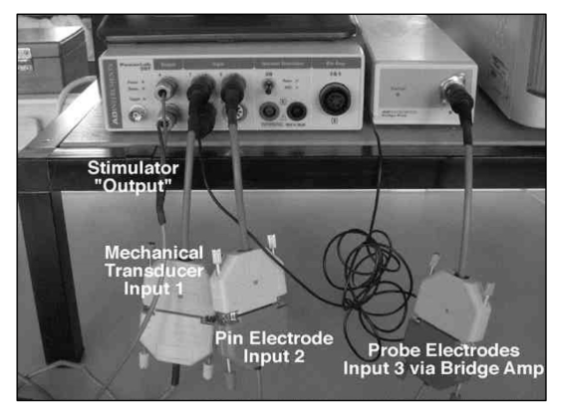
Powerlab connections
simultaneously record the contraction of the heart and electrical activity of the heart via the pin electrode
Mechanical activity → redcord at input 1
Electrical acitivty→ record at input 2
Also electrical activity from the probe→ input 3 through bridge amplifier
used to stimulate probe electrodes connected to the output for this bit?
Recording electrical and mechanical activity using the pin electrode: Experiment 1
Record electrical acitivty of heart
using pin electrode through tip of ventricle
simultaneously
record contraction of heart→ connect pin electrode to mechanical transducer
using long piece of thread
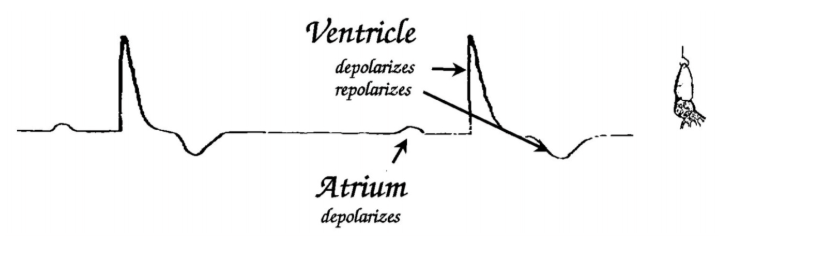
Experiment 1: Electrical recordings
Because the hook has penetrated some of the cells of the ventricle:
records quasi-intracellular electrical potential→ (injury potential)
also
partly record extracellular potentials generated by rest of heart
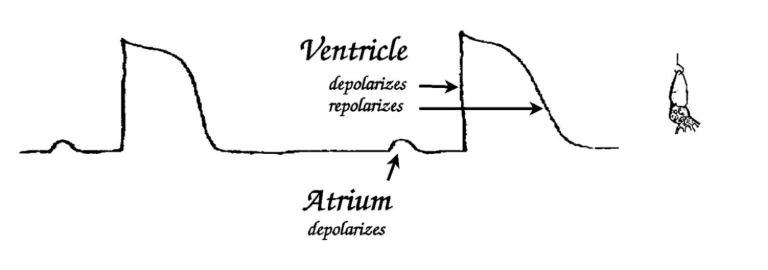
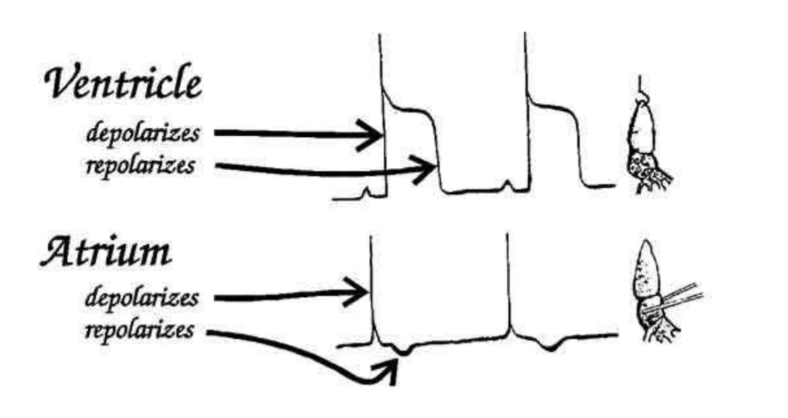
Picture: shows early recordings
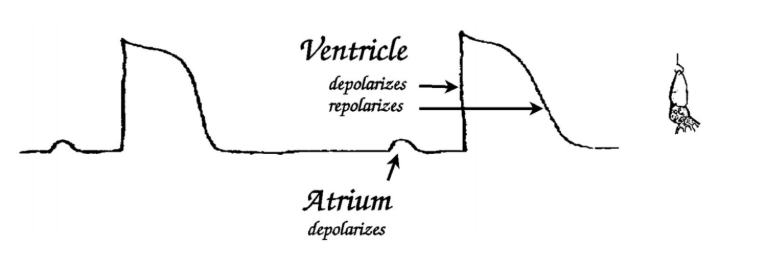
Description of recording
largest electrical event→ ventricle
coz where pins are and venticle is a large mass of tissue
Plataeu→ looks similar to what expect if record cardiac AP from single cells with intracellular potential
Recording with time
Lose the plateau as cells die off
Recodring becomes more extracellular in form
but
Ventrical de and re- polarisation are still obvisous as dominant electrical events
Small event before ventricular dep→ depolarisation of atria
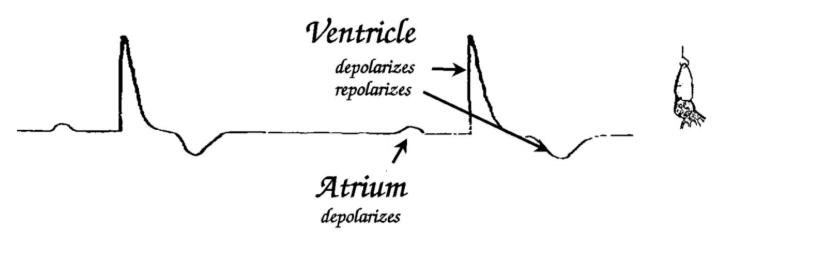
Repolarisation of atria?
→ masked by depolarisation of ventricle
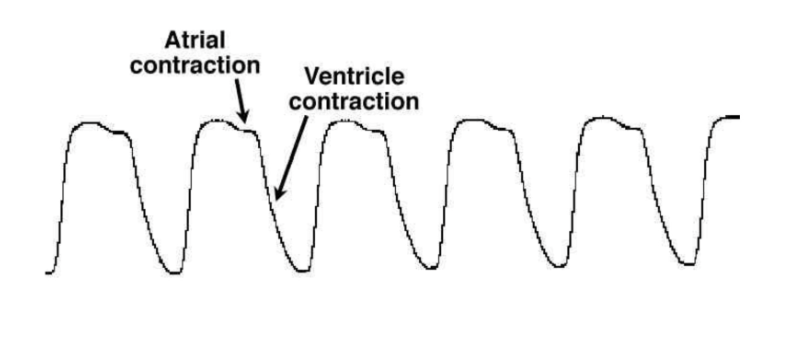
Experiment 1: Mechanical recordings
seen separately to the elctrical→ so can be compared
see temporal relationship
Typical mechanical recording
Atrial contraction→ associated with small downward deflection of lever arm of mechanical transducer
Ventricular contraction→ associated with much larger downward deflection of the arm
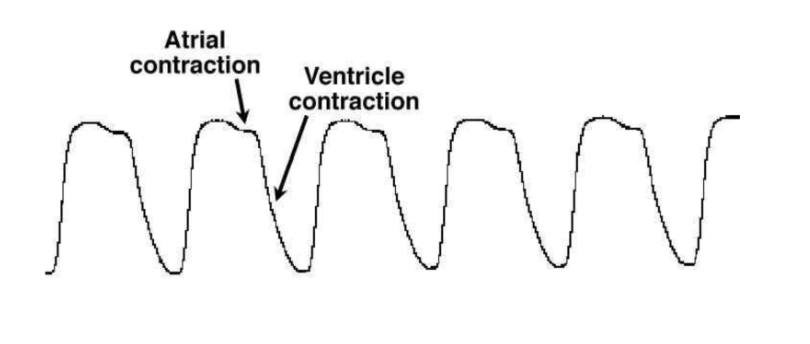
Why may the recording be a bit off?
ventricle will not fully relax before the atria contracts
→ masks the initial contraction phase of atria
more common with larger hearts
Important to interpret records carefully
Although the frog’s heart electrical activity is myogenic
Still affected by
Sympathetic stimulation
→ via cardioaccelerator nerves
parasympathetic
→ via vagus nerve
Temperature
Experiment 2: Parasympathetic effects easily observed by
applying ACh directly to sinus venosus
→ EFFECT→ bradycardia
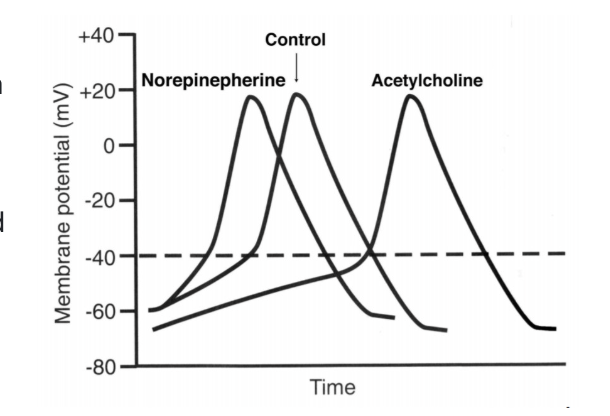
can also observed sympathetic effects with noradrenaline
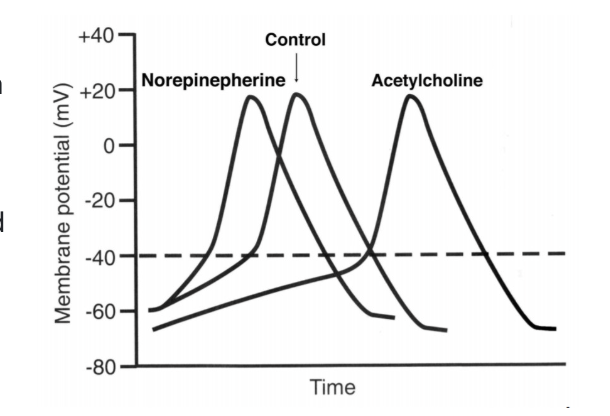
How does ACh exert these effects
Reducing the rate of spontaneous depolarisation of the pacemaker cells in sinus venosus
activate K+ channels
reduce number of open Ca2+ channels (and Na+ channels probs)
membrane potential held closer to K+ equilibirium potential
If enough K+ channels activated→ pacemaker potential may neer reach threshold
will not initiate AP
heart stop beating
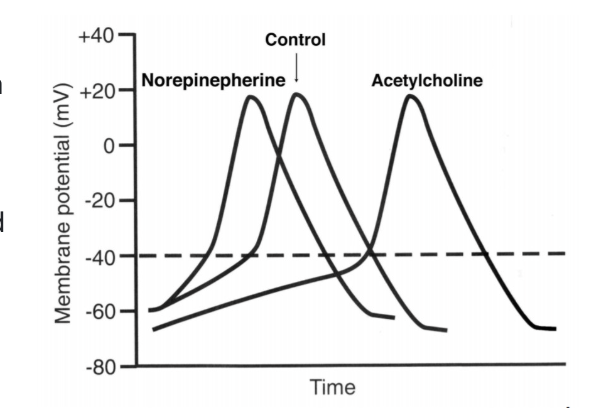
What noradrenaline does
increase the slope of pacemaker potential
threshold is reached more rapidly
heart rate increases
Tachycardia
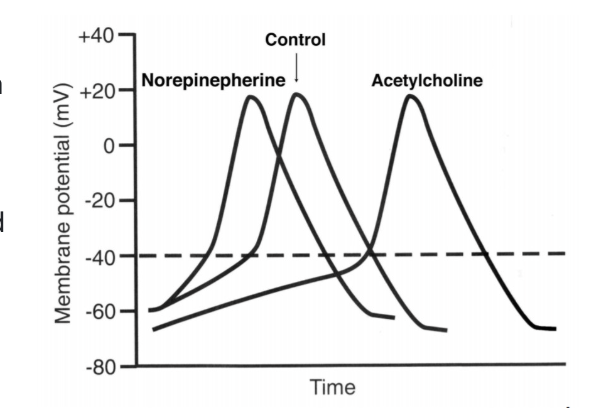
How NA works to increase slope
opens Na+ and Ca2+ channels
inhibit K+ channels
Experiment 3: effects of temperature
irrigate heart with warm or cold Ringer’s solution
will be able to observe reversibility of response too as it returns to room temp
measure:
interval between beats
duration of ventricular AP
interval between the start of the atrial and ventricular APs
Probe electrode for stimulating the heart experiment
adjust probe to record extracellularly from specific places in the heart
→ to identify different components of the pin electrode recording
Probe set up at input 3 via bridge amplifier
Recording from the atria
largest deflection→ electrical activity of atria
compare events recorded from the pin electrode with probe
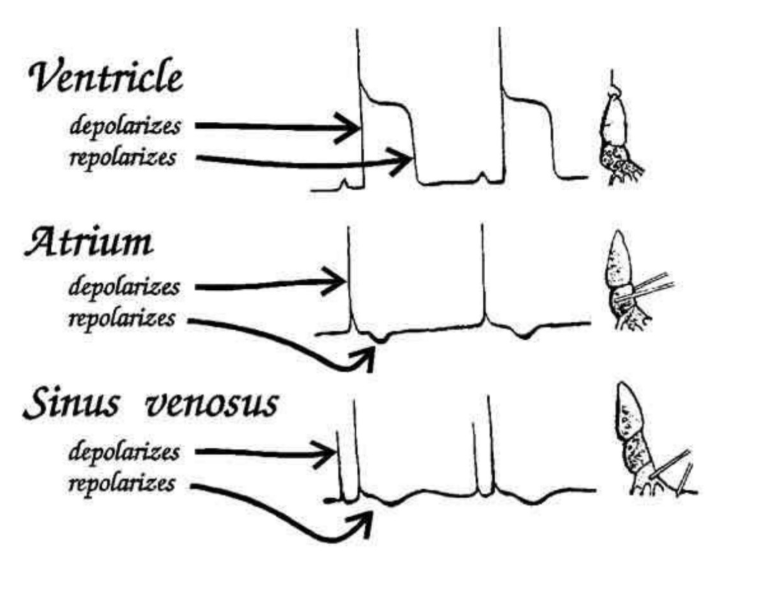
Recording from sinus venosus: how set up
BLACK→ abdominal viscera
RED→ sinus venosus
must increase sensitivity of probe→ electrical signal is very small
Result
See a small deflection BEFORE the atrial deflection
figure:
compare the lectrical timing of the electrical activity of the heart
recorded from the pin and probe electrodes
OVERALL: establish order at which the electrical activity of the different chambers occurs
( sinus venous→ atria→ ventricles)
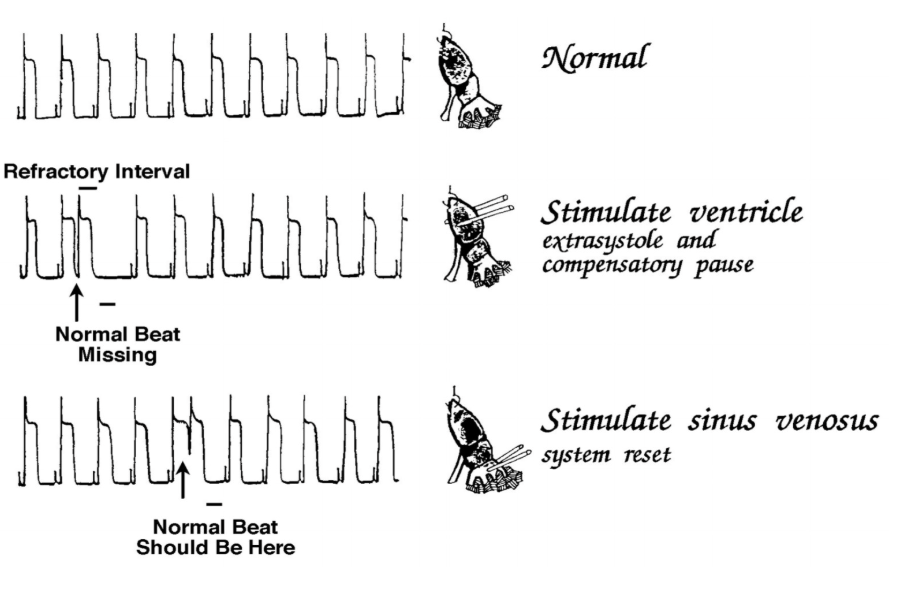
Experiment 4?: Stimulation of the heart
Use to get further evidence for localising actual pacemaker region
Principle of experiment:
if stimulate part of heart that is being driven elsewhere→ you may get abnormal premature contraction
but
→ basic cycle is not disturbed
MEANING: pacemaker continues to output normally
HOWEVER: beat may be absent→ as a result of normal beat attempting to stimulate ventricle during its refractory phase
→ ‘extra systole’ and ‘Compensatory phase’
Why does the compensatory pause arise
as a result of the long refractory period of cardiac tissue
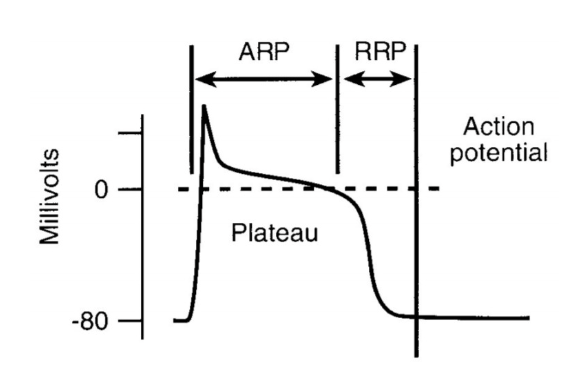
THEREFORE: a slower look at the refractory period is in order
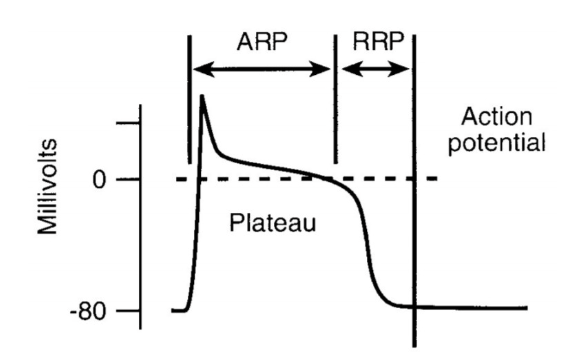
Reminder of the refractory period
Picture→ recorded with intracellular electrode in myocyte
point where cell cannot fire a second AP
due to inactivation of voltage-ativated Na+ channels
lasts for more than 100ms
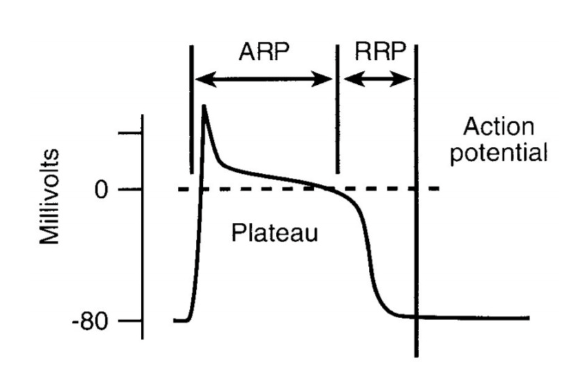
There are two refractory periods
Absolute refractory period (‘effective’)
not possible to stimulate an AP
due to Na+ channel inactivation
Relative refractory period
repolarisation phase
AP may be initiated BUT stimulus is greater than that required to initiate an AP
WHY?: result of incomplete recovery of inactive Na+ channels
cell is in a state of reduced excitability
As the cell continues to repolarise
Na+ channel inactivation is removed
normal electrical input can induce an AP
THEREFORE: if we stimulate a cell that is being driven by electrical events from elsewhere
it is then possible that the arrival of the pacemaker induced event may occur at a time when the cells are refractory
→ resulting in no AP generation (so get a missing beat)
→ This is what underlies the compensatory pause folloing electrical stimulation of the ventricle
leading to an extra systole
This is observed as
normal beat missing
but
pacemaker is firing at its normal point in time
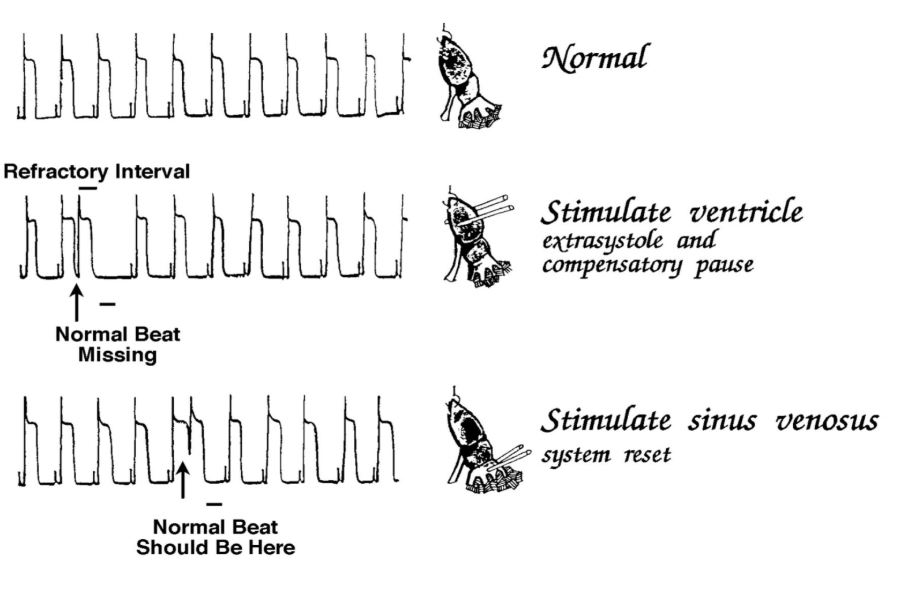
BUT: if we stimulate the pacemaker: result
reset the rhythm of the heart
Observation
displacemnet of the normal beat in time
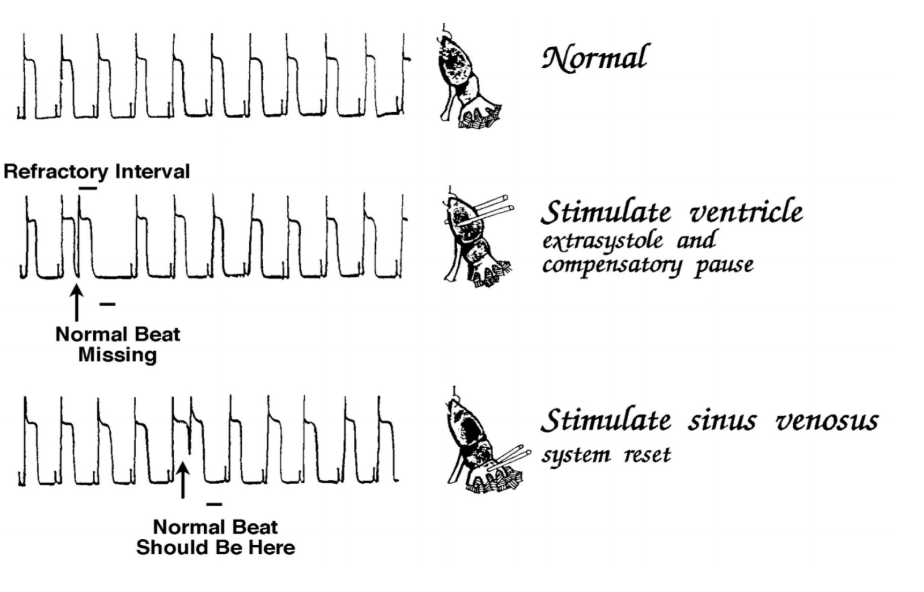
OVERALL the stimulating experiment is used to
Find which specifica areas are the pacemakers
if a pacemaker→ will just reset the cycle
if not a pacemaker→ will miss a beat coz it is in refractory period