Endo 24 - Root Resorption (Dr. Zeller)
1/114
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
115 Terms
Resorption
What is a condition associated with either a physiologic or a pathologic process resulting in a loss of dentin, cementum and/or bone?
Odontoclasts
Physiological resorption in the life span of a primary tooth, mediated by _____________
Odontoclasts
What have similar enzymatic and metabolic properties to osteoclasts but are smaller in size, have fewer nuclei, and form smaller resorption lacunae?
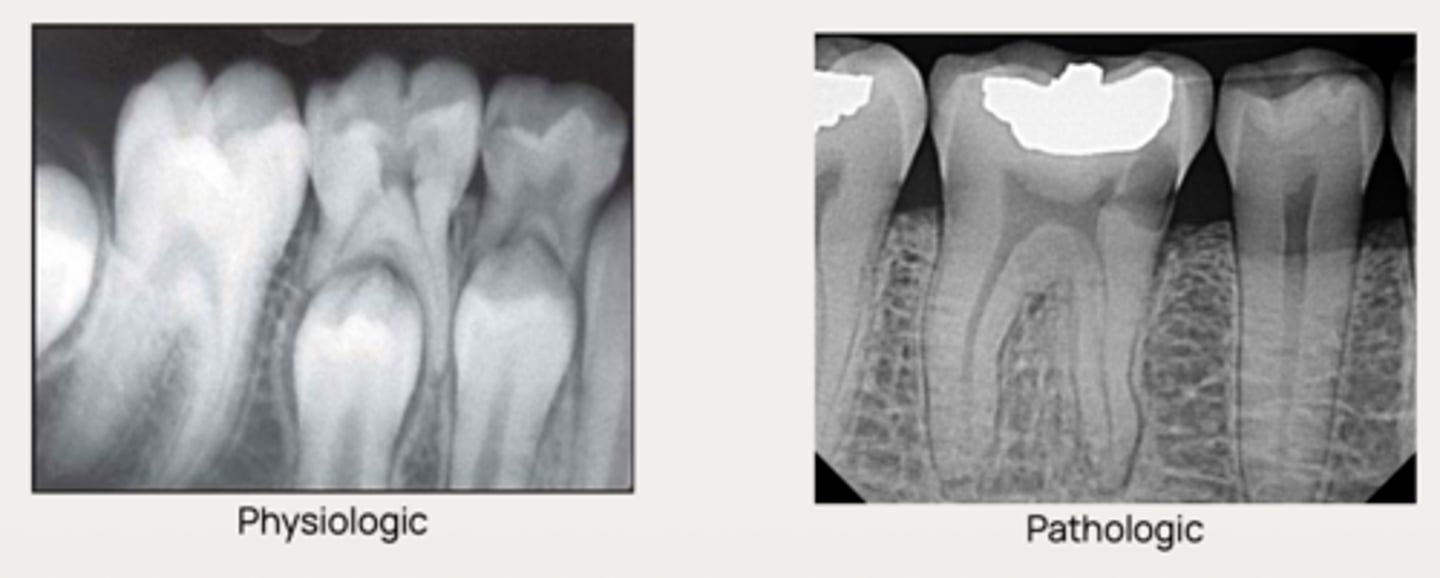
Physiologic resorption
What type of resorption allows the permanent successor tooth to erupt?
True
T/F: Physiologic resorption will occur even without a permanent successor tooth, but at a slower, more disorganized pace.
- Loss of unmineralized protective layers
- Stimulus for resorptive activity
What are the 2 criteria for pathological resorption to occur?
- Predentin → internal
- Precementum → external
One criteria for pathological resorption is Loss of unmineralized protective layer (usually some form of trauma), what are two non-mineralized protective layers that can be lost?
- Inflammation (pulpal/periodontal)
- Pressure (odontogenic/pathologic)
- Trauma
One criteria for pathological resorption is stimulus for resorptive activity, what are three stimuli?
- Inflammatory
- Replacement
What are the two types of internal root resorption?
- Inflammatory
- Replacement
- Cervical
- Surface
- Transient apical breakdown
What are the five type of external root resorption?
Based on their location in relation to the root surface and subcategorized according to pathogenesis
How are dental resorptive lesions classified?
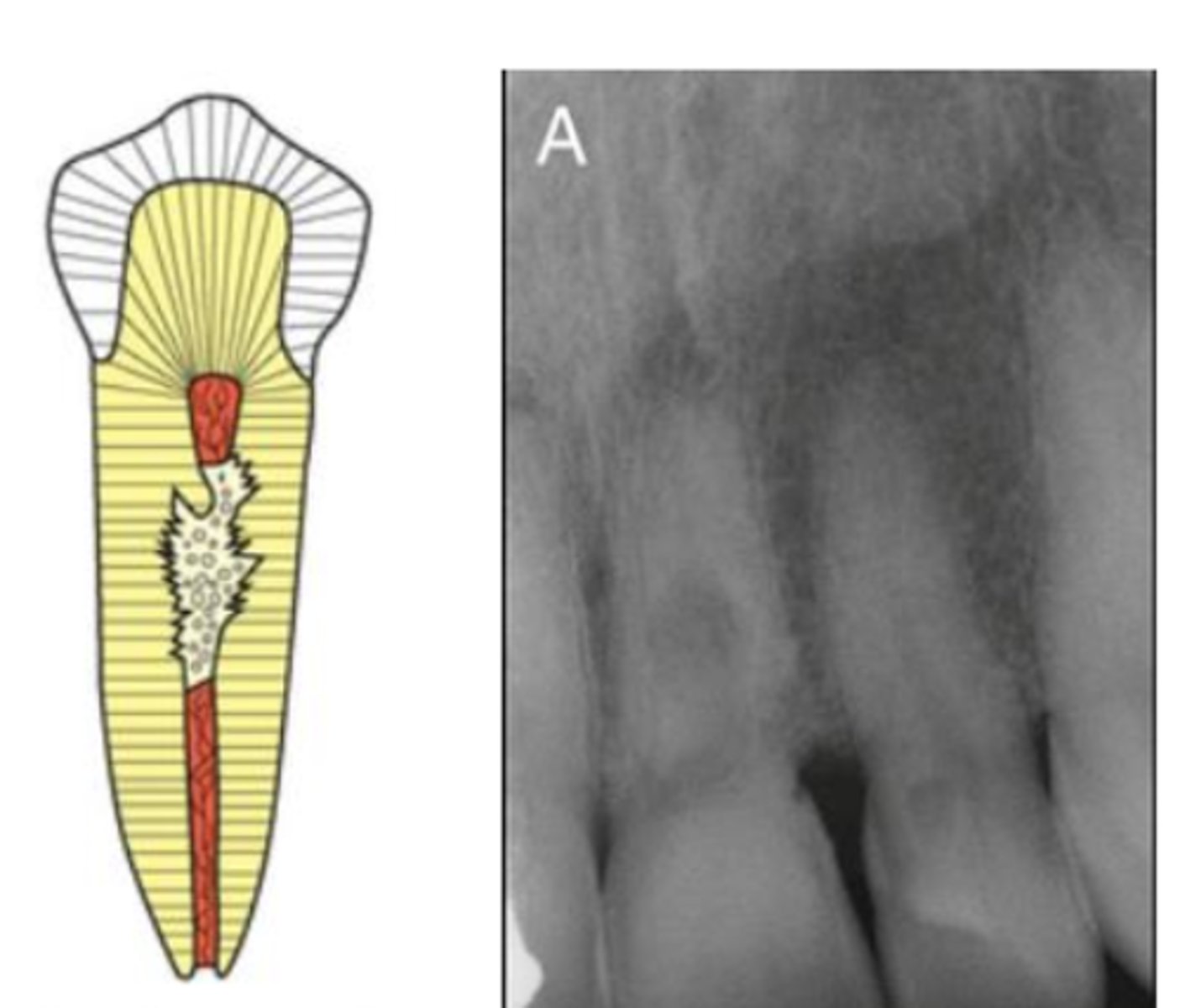
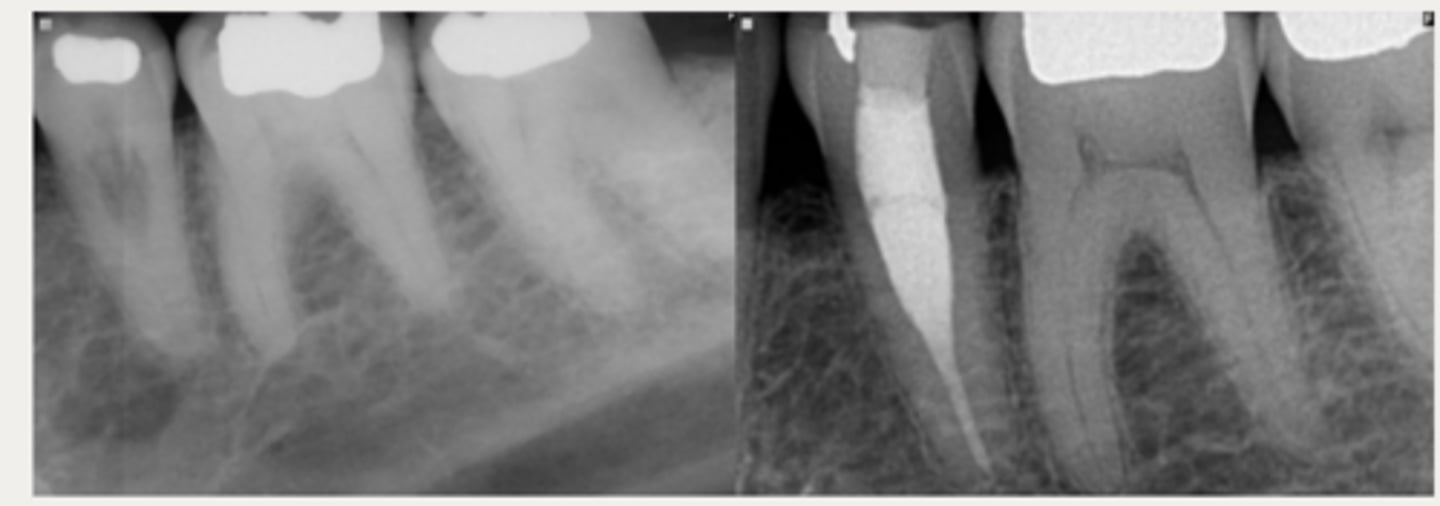
Internal root resorption
What type of resorption is the following?
- Originates inside the tooth, on the root canal wall
- Initiated by damage to the odontoblastic and
unmineralized predentin layer, resulting in →
- - Exposure of mineralized dentin to pulp tissue
- - Migration of odontoclasts to the site of injury
- - Resorption of the altered root canal walls
Internal root resorption
Predisposing factors of _________ resorption is history of trauma, caries or periodontal infections affecting the pulp
Other etiological factors include:
- Periodontal infections
- Excessive heat generated during restorative procedures
- CaOH procedures (vital pulpotomy and pulp capping)
- Cracked tooth
- Orthodontic treatment
- Idiopathic dystrophic changes in normal pulps
Odontoclasts
What cell initiates resorption of dentin from within the root canal, causing resorption that expands circumferentially and apico-coronally from the spot of initiation, in internal inflammatory resorption?
Inflammatory infiltrate
(Becomes more like periodontal connective tissue than normal, healthy pulp tissue)
What is pulp tissue replaced with in internal inflammatory resorption?
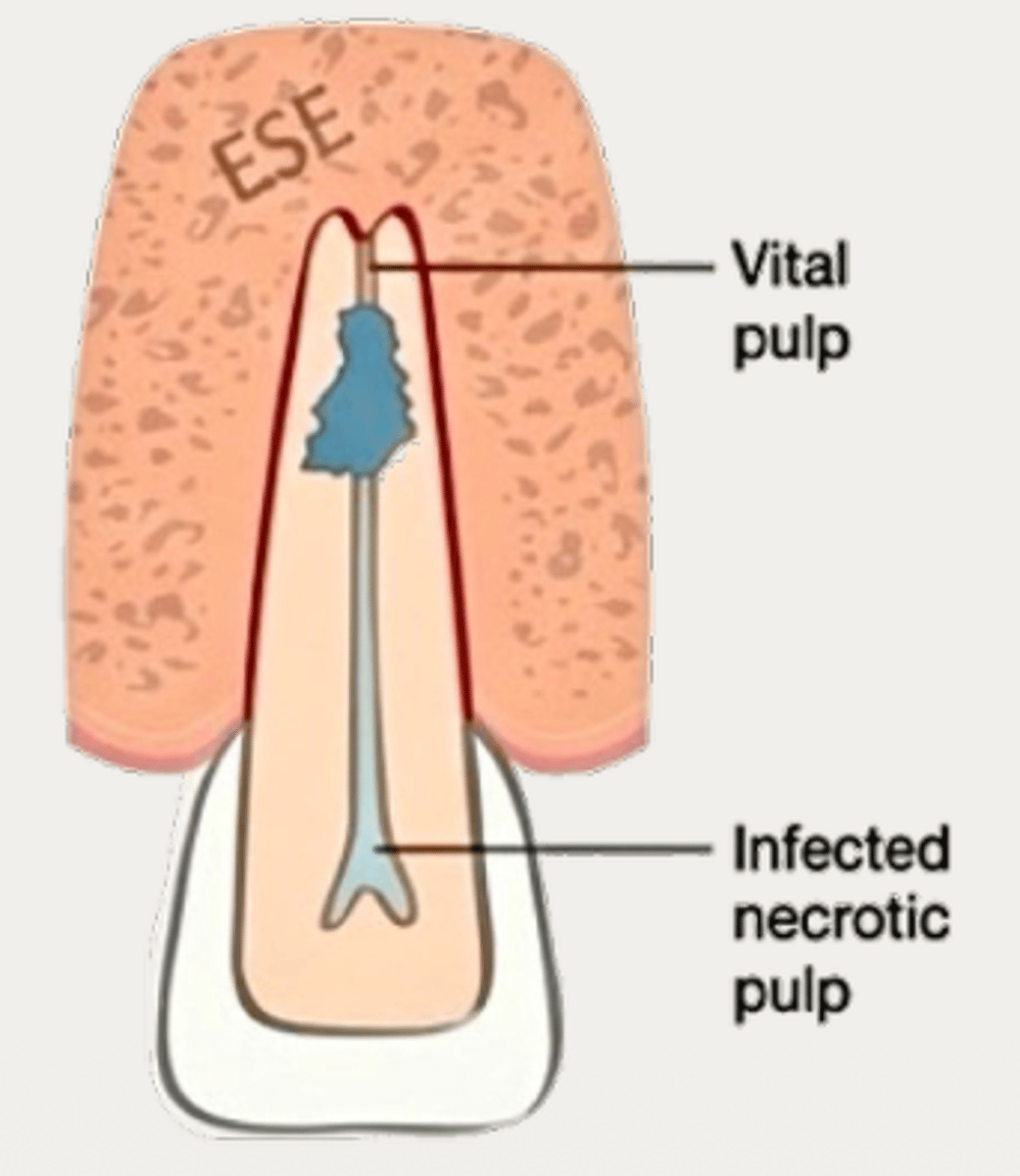
Internal inflammatory resorption
What type of resorption?
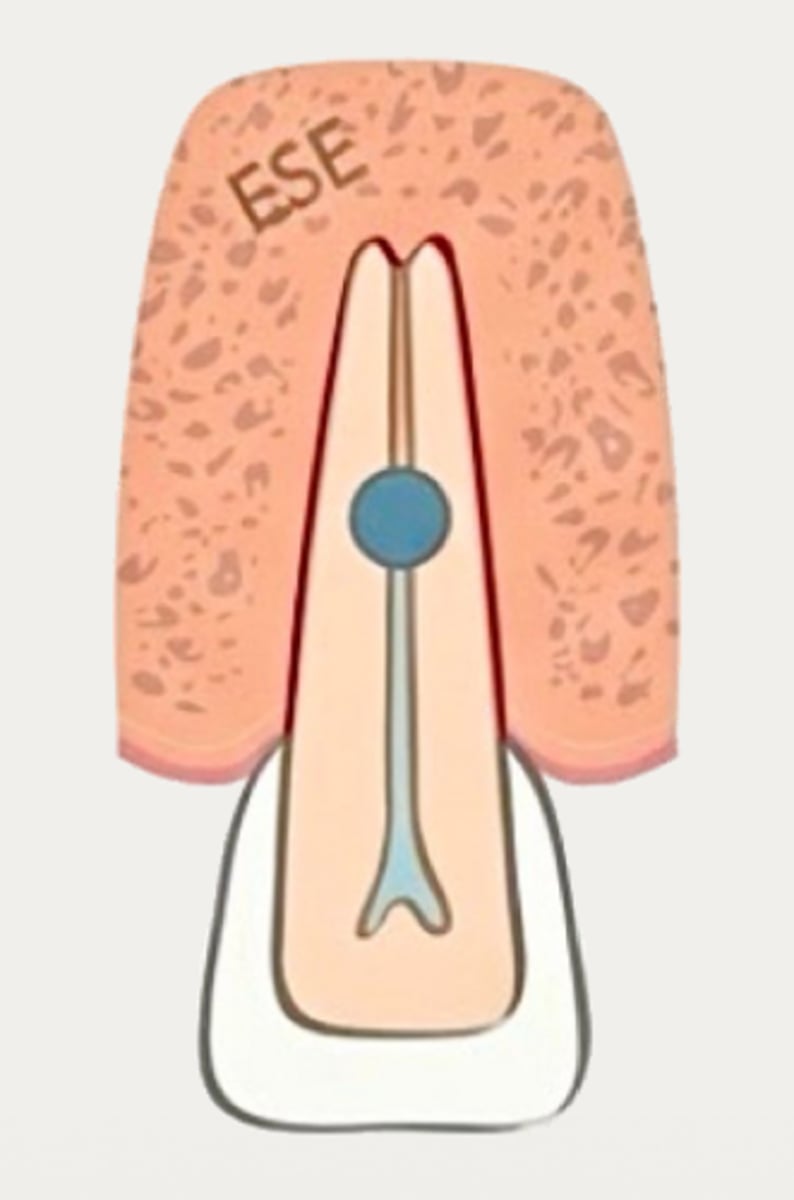
necrotic
With Internal Inflammatory Resorption, pulp coronal to resorptive lesion is __________
vital
With Internal Inflammatory Resorption, pulp apical to resorptive lesion is __________
Clastic cells and their nutrients
Vital pulp apical to internal inflammatory resorptive lesions provide what?
microbial stimulation
Necrotic pulp coronal to internal inflammatory resorptive lesions provide what?
Resorption will cease to progress
If the tooth with internal inflammatory resorption loses vitality, what will happen?
Pulp tissue apical to the resorptive lesion will undergo necrosis → resulting in apical periodontitis
If the tooth with internal inflammatory resorption is left untreated, what will happen?
Internal inflammatory resorption
What is the diagnosis?
- Usually asymptomatic and have a normal appearance
- May have pink/red spot on the crown due to granulation tissue in the coronal dentin
- May display signs of pulpitis:
+ to sensibility tests in (partially) vital cases
- to sensibility tests in necrotic cases
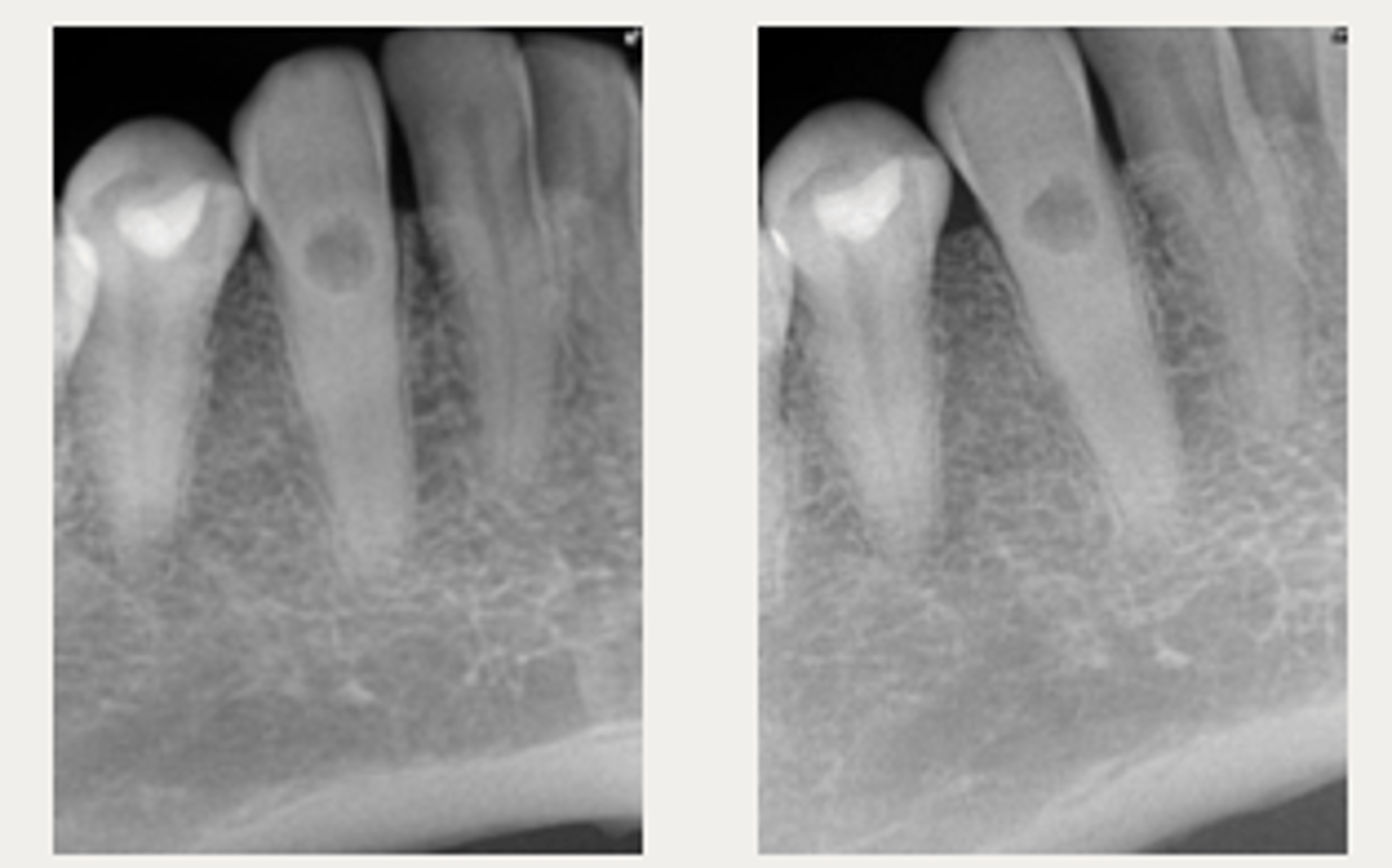
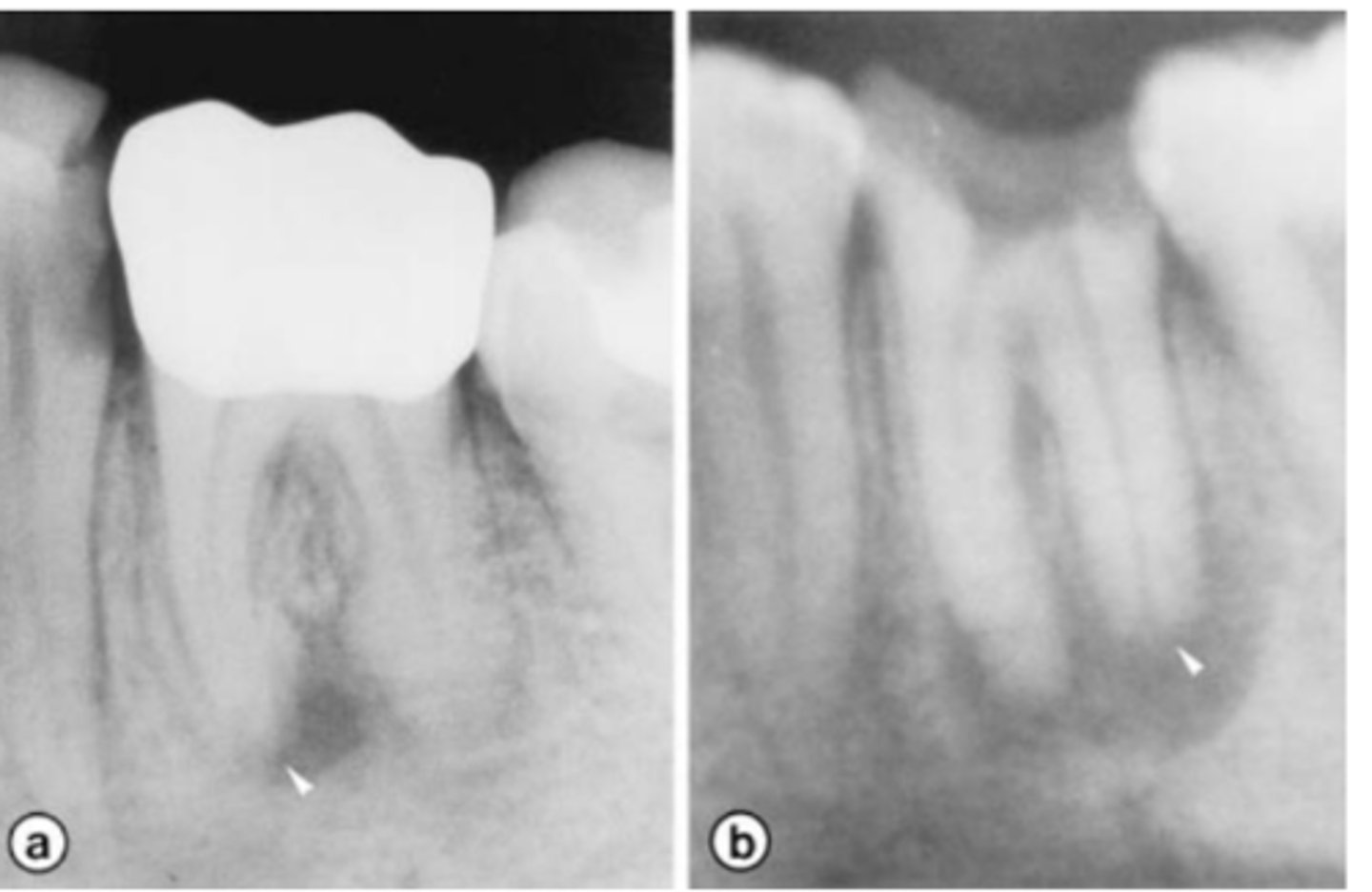
Internal inflammatory resorption
What is the diagnosis?
- Symmetrical ballooning of root canal
- Lesion does not move when PA is taken from
different angles
- Usually does not have periapical lesion (Apical portion of root is vital!)
- Lesion may perforate into alveolar bone
- CBCT is recommended
Internal inflammatory resorption
Patient presents asymptomatic with a normal appearance but there is a pink/red spot on the tooth, what is the most likely diagnosis?

Internal inflammatory resorption
Patient presents with symmetrical ballooning of the root canal and lesion does not move when PA is taken from different angles. There is no PARL. What is the most likely diagnosis?
Root canal therapy
(Remove pulp → removes the inflammatory stimulus → resorption will stop)
What is the treatment recommendation for internal inflammatory resorption?
- Sonic activation, passive ultrasonic irrigation, lasers
- Intracanal antibacterial medicament may be used to further reduce the microbial load and improve disinfection
What are some adjunctive irritation methods for the treatment of internal inflammatory resorption?
Warm Vertical Condensation
(Can also obturate resorptive space with Bioceramics, RMGI, composite, etc.)
If an internal inflammatory resorptive lesion is non-perforating, what is the preferred obturation technique?
Depend on location of perforation; an external, surgical approach may be considered:
- Supracrestal: GI, RMGI → Geristore), composite, Biodentine
- Subcrestal: MTA, Root Repair Material → BC putty), Biodentine
If an internal inflammatory resorptive lesion is perforating, what is the preferred obturation technique?
100%
According to a study by Caliskan, Treatment of non-perforating internal inflammatory resorptive lesions were ____% successful after 2-4 years
25%
According to a study by Caliskan, Treatment of perforating internal inflammatory resorptive lesions were ____% successful after 2-4 years
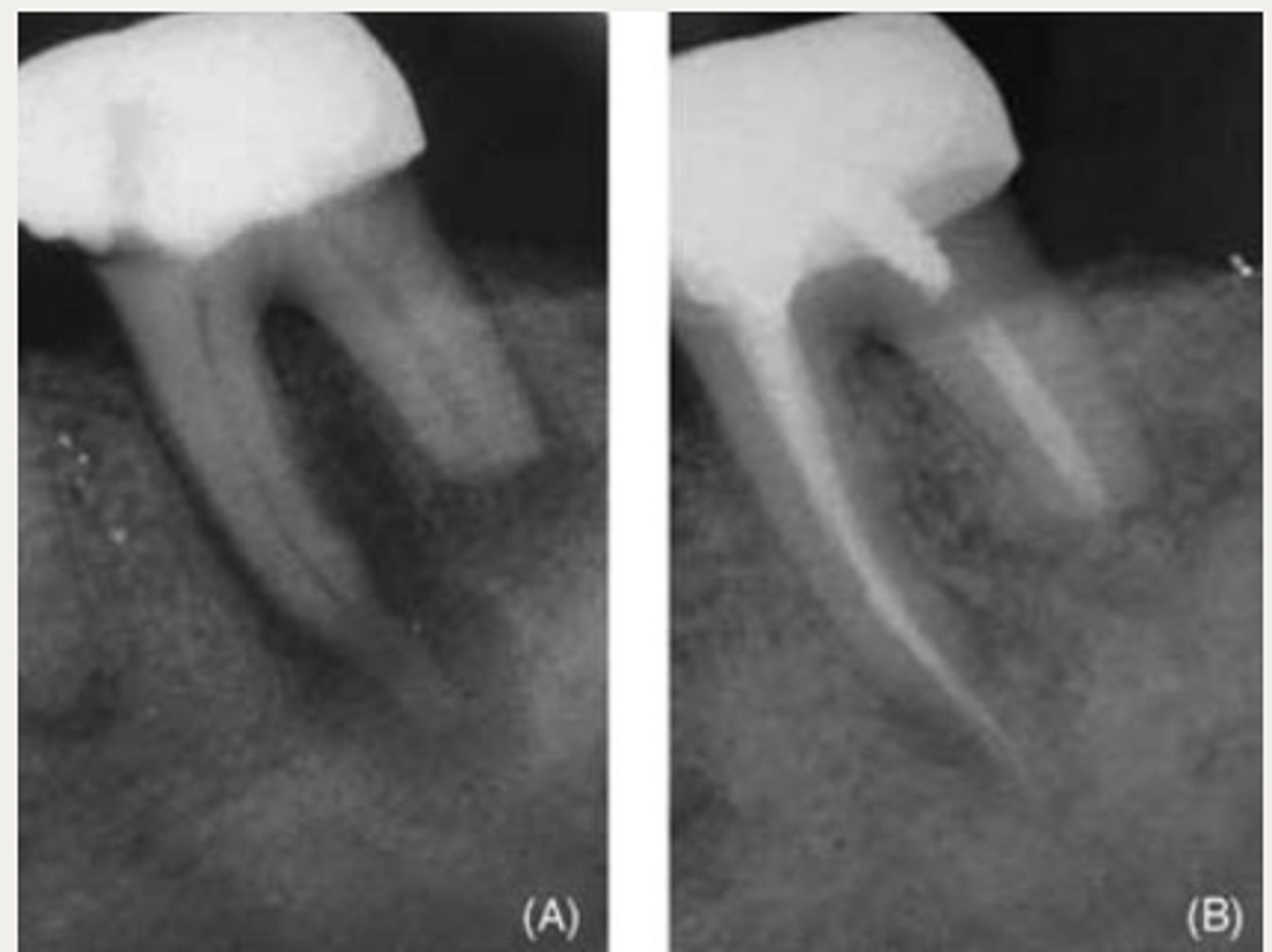
Internal replacement resorption
What type of resorption?
Internal replacement resorption
What type of resorption?
Predentin
(associated with a history of trauma, caries or periodontal infections affecting the pulp)
Which layer is damaged with Internal Replacement Resorption?
Metaplastic hard tissue (resembles bone/cementum)
With internal replacement resorption, what is the resorbed tissue replaced with?
Internal replacement resorption
It is suggested that __________ is an attempt to replaced the damaged, resorbed dentin in inflammatory internal resorption (IIR)
Internal replacement resorption
Which lesion has a similar diagnosis, management, and prognosis of internal inflammatory resorption (IIR) but radiographic findings will have radiopaque material in the resorptive area?
Ultrasonic tips
What may be required to navigate through the bone-like hard tissue in internal replacement resorption?
External root surface
What surface does external root resorption originate on?
Precementum
External Root Resorption is damage to what layer?
- History of trauma
- Caries
- Periodontal infections
- Orthodontic treatment
- Pressure
What are the predisposing factors of External Root Resorption?
External Inflammatory Resorption (EIR)
Which type of resorption?
Precementum
External Inflammatory Resorption is damage to the _______ layer of infected, necrotic root canals most commonly due to trauma or caries
Lateral External Inflammatory Resorption
Which type of External Inflammatory Resorption (EIR)?
- Observed following severe traumatic injuries such as luxation injuries and avulsions.
- Trauma causes damage to PDL → leads to denuded areas on the root
surface which are chemotactic to clastic cells
- Necrotic pulp (bacteria) + PDL damage (trauma) ⇒ initiates resorption
Apical External Inflammatory Resorption
Which type of External Inflammatory Resorption (EIR)?
Observed in cases of apical periodontitis secondary to pulp necrosis.
- Inflammatory stimulators from the necrotic root canal communicate with the apical foramina → triggers an inflammatory response → activates clastic cells
Severe traumatic injuries
Lateral EIR is most commonly seen following what?
Apical periodontitis secondary to pulp necrosis
Apical EIR is most commonly seen with what?
External Inflammatory Resorption (EIR)
Which type of resorption?
Lateral External Inflammatory Resorption
ID the type of resorption:
CLINICAL:
- History of trauma
- Pulpal Dx → necrotic
- Symptoms of apical periodontitis
- - May be tender to percussion and/or palpation
RADIOGRAPHIC:
- Radiolucent, crater shaped indentations on the root surface with adjacent bone loss and periradicular radiolucencies
Apical External Inflammatory Resorption
ID the type of resorption:
CLINICAL:
- Heavily restored or carious tooth
- Pulpal Dx → necrotic
- Symptoms of apical periodontitis
- - May be tender to percussion and/or palpation
RADIOGRAPHIC:
- Heavily restored/carious
- Roots may appear shorter than expected and/or have ragged root ends
- Periapical radiolucency usually present
Lateral External Inflammatory Resorption
Patient presents with history of trauma, does not respond to sensibility tests (necrotic pulp), is tender to percussion and/or palpation and has these radiographic findings. What is the most likely diagnosis?
Apical External Inflammatory Resorption
Patient presents with a heavily restored tooth or carious tooth, does not respond to sensibility tests (necrotic pulp) and may be tender to percussion and/or palpation. Radiographs show roots shorter than normally expected/ragged root ends. A PARL is also observed. What is the most likely diagnosis?
Root canal treatment
(Removing the inflammatory stimulus will arrest the
resorption)
What is the recommended treatment for External Inflammatory Resorption (EIR)?
Further reduces bacterial load and favorably influences the local environment at the resorption sites through dentinal tubules
Why is intracanal antibacterial medicament (CaOH, Ledermix paste) advised in the treatment of External Inflammatory Resorption (EIR)?
Apical plug may be needed (bioceramic putty, MTA)
T/F: Obturation/apical preparation of Apical EIR may be difficult depending on the extent of the resorption. What may be needed if tugback cannot be achieved?
- High success rates, similar to success of NS-RCT
- If severe or perforating, prognosis may become more unfavorable/surgical intervention may be necessary
What is the prognosis of external inflammatory resorption (EIR)?
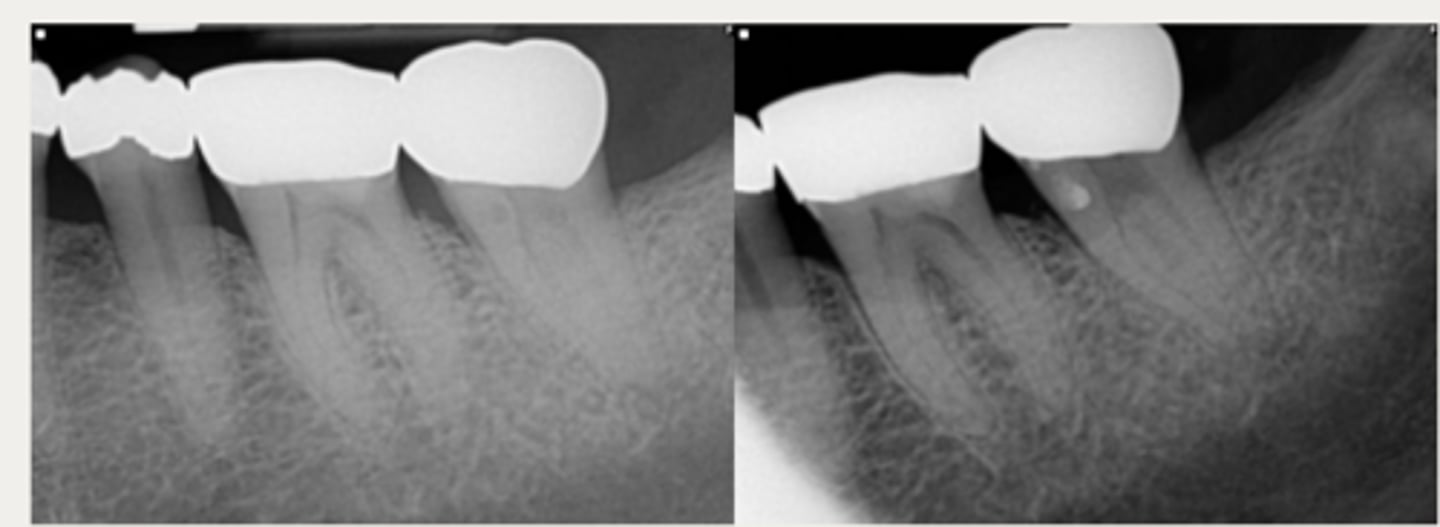
External Replacement Resorption/Ankylosis
Which type of resorption?
External Replacement Resorption/Ankylosis
Which type of resorption?
- Fusion of cementum or dentin with alveolar bone
External Replacement Resorption/ankylosis
Which type of resorption>
- Damage to PDL ⇒ stimulus for surrounding bone to activate osteoclasts and begin resorbing cementum/dentin and replacing it with bone tissue
- Almost always due to trauma (luxation, intrustion, avulsion, replantation)
- Can be progressive or self-limiting
20%
(May be reversed if less than 20% of the root surface is involved)
External Replacement Resorption can occur if over ___% of the root surface becomes damaged
External Replacement Resorption/ankylosis
ID the type of resorption:
CLINICAL
- Characteristic metallic sound on percussion
- May appear infraoccluded in developing dentition
- Lacks physiologic mobility of normal teeth
- May not respond to sensibility testing
RADIOGRAPHIC
- Absence of lamina dura/PDL
- Bone trabeculation occupying previous root surface
- CBCT is often helpful to assess the full extent
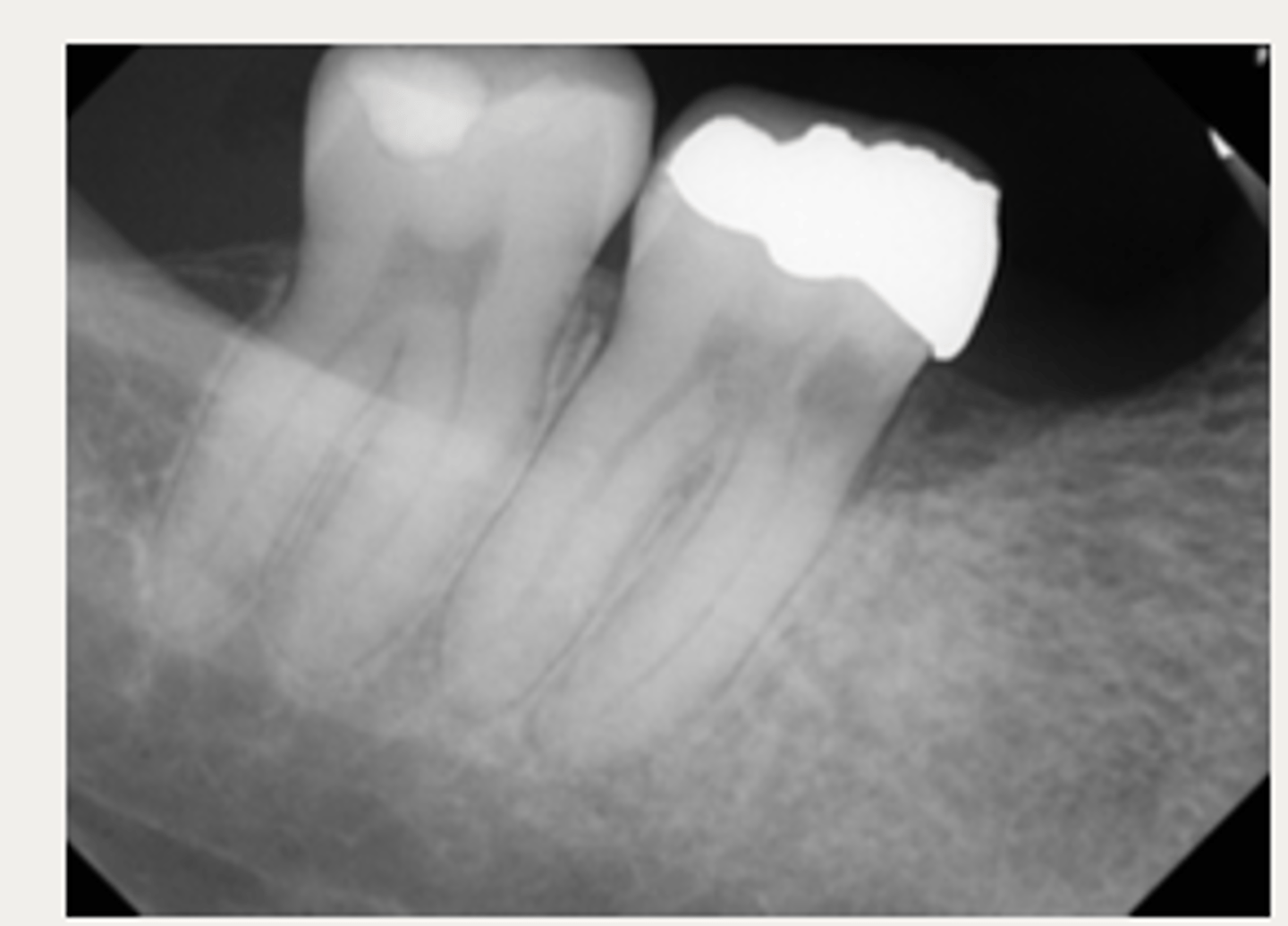
External Replacement Resorption/ankylosis
Patient presents with a metallic sound on percussion, infraoccluded appearance in developing dentition and may not respond to sensibility testing. What is the most likely diagnosis?

External Replacement Resorption/ankylosis
Patient presents with these radiographic findings. What is the most likely diagnosis?
- Absence of lamina dura/PDL around lesion.
- Bone trabeculation occupying previous root surface.
Monitoring
(No effective management)
With external replacement resorption, what is usually the treatment of choice since there is no stimulation to remove?
Decoronation
(- Remove all canal contents: vital, necrotic, previous filling - Induce bleeding into canal until clot forms - Decoronate tooth to bone level - Suture and let bone/gingiva heal over - Root gradually replaced by bone while maintaining alveolar width/height)
With external replacement resorption, in developing teeth, what is a possible treatment to preserve the alveolar ridge and allow more optimal conditions for a later prosthetic solution?
True
T/F: Extraction of a external replacement resorption may be difficult
No cure, but the process can be very slow and self-limiting; can take years to decades to completely resorb a root
Is there a cure for external replacement resorption?
Optimizing replacement strategies
(Early diagnosis and replacement or maintenance of bone until age allows implant placement)
Treatment of external replacement resorption is usually aimed at what?
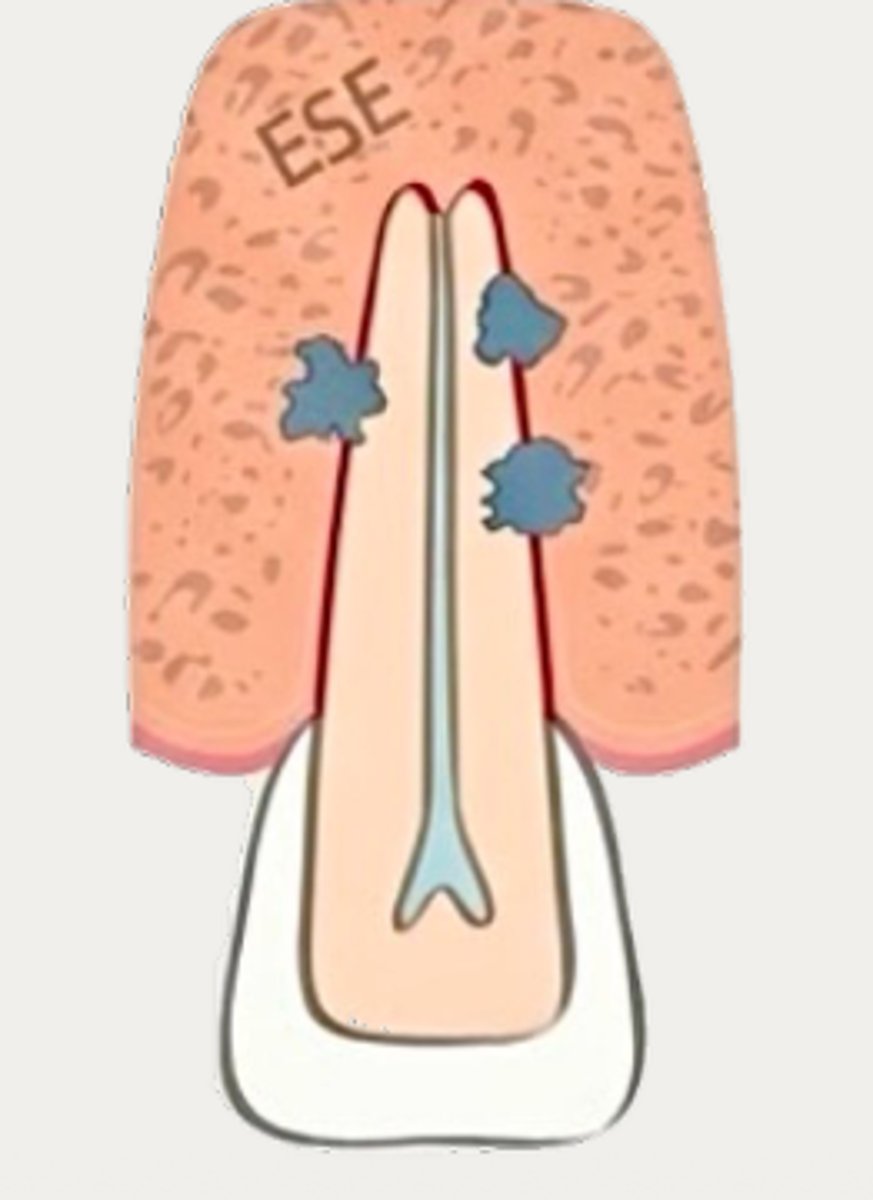
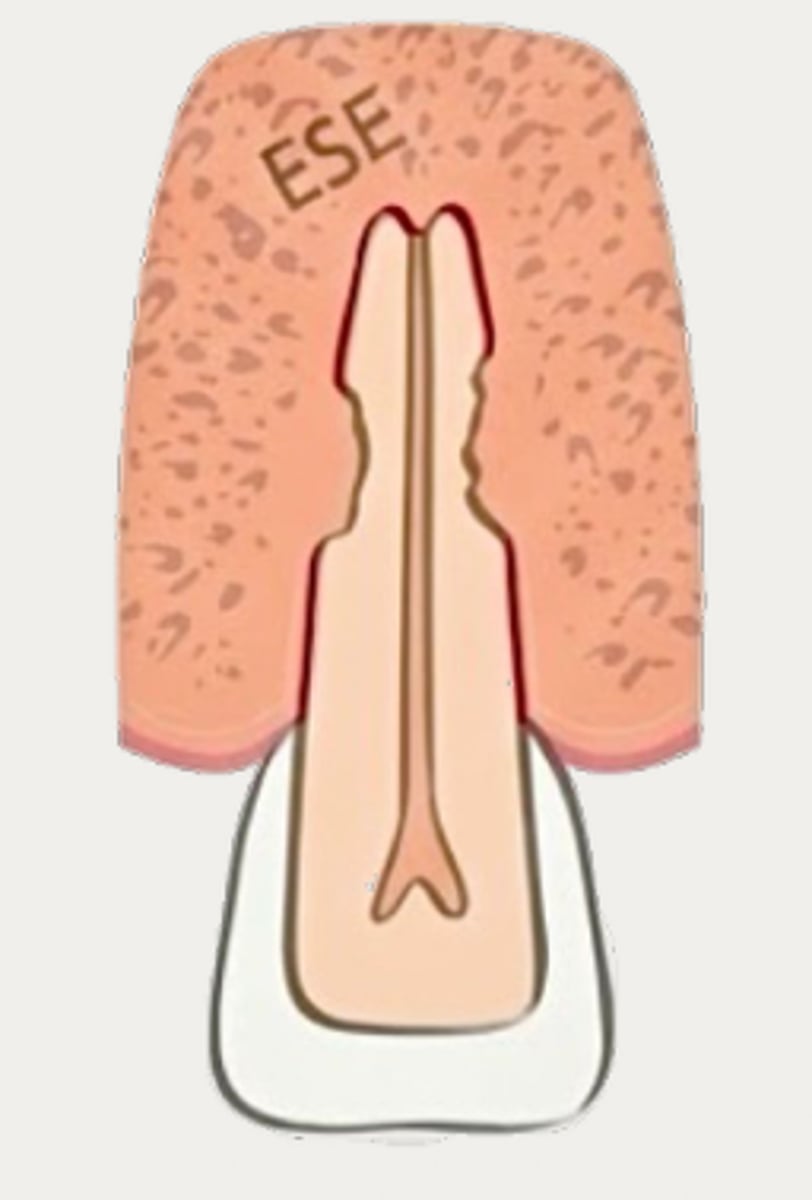
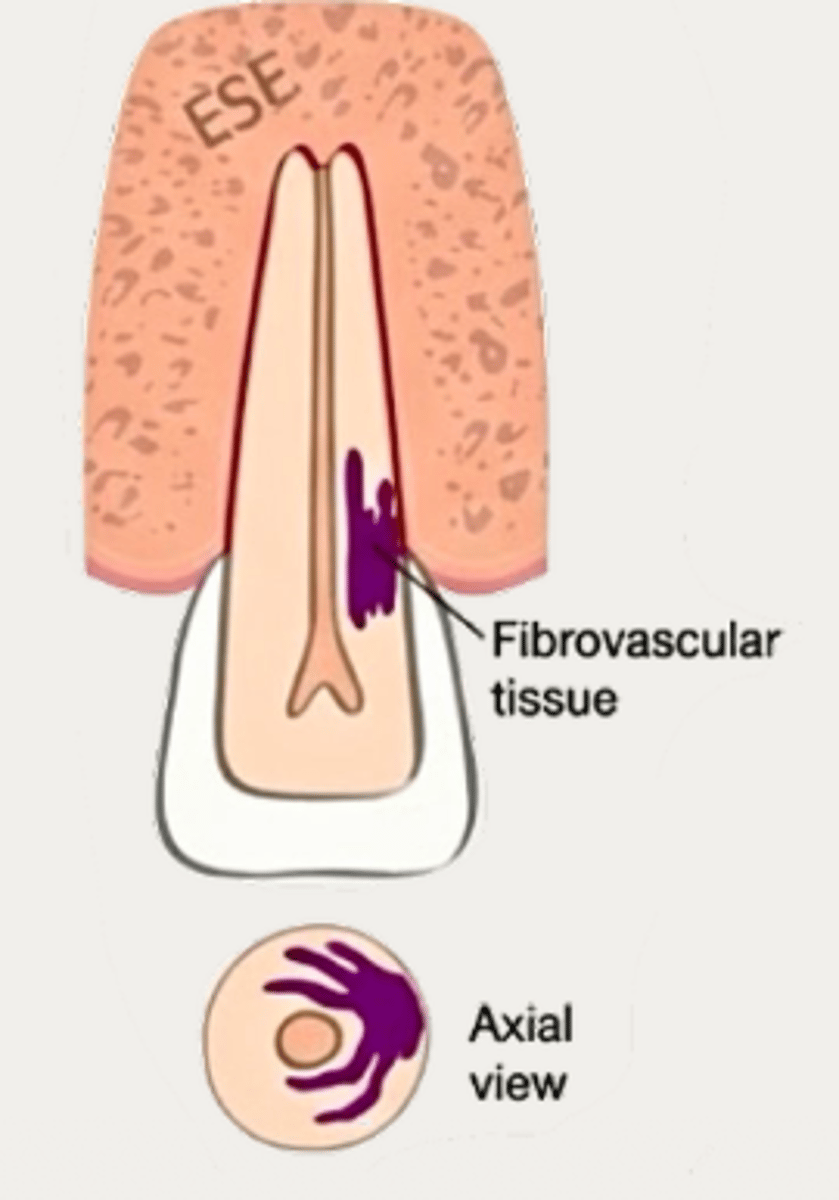
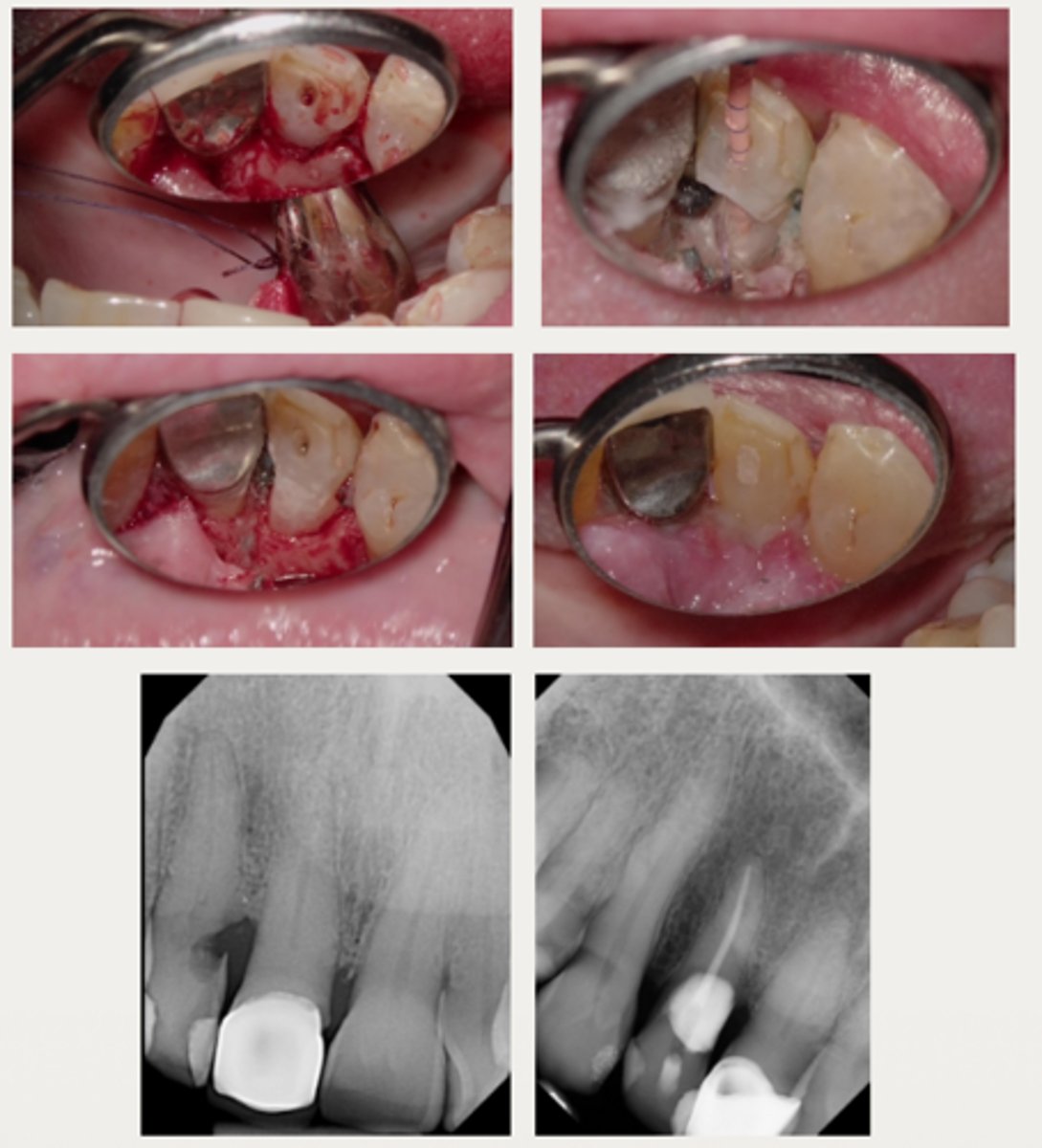
External cervical resorption (Invasive Cervical Resorption)
Which type of resorption?
Invasive Cervical Resorption
What is external cervical resorption also known as?
External cervical resorption (Invasive Cervical Resorption)
Which type of resorption?
- Loss/absence of subepithelial precementum layer in cervical region of tooth causes osteoclasts from periodontium to invade exposed root surface
Subepithelial precementum
In external cervical resorption, the loss of what causes osteoclasts from periodontium to invade the exposed root surface?
True
T/F: The etiology of external cervical resorption is not entirely understood/unclear but Potential predisposing factors are orthodontics, trauma, internal bleaching, diabetes, antiresorptive medication use, feline virus transmission, bacteria, periodontal surgery, orthognathic surgery, restorative work, malocclusion, wind instrument use, parafunctional habits, and idiopathic causes
Orthodontics
What is the most common sole predisposing factor of external cervical root resorption?
- Initiation
- Resorption
- Repair
What are the three stages of the mechanism responsible for the development and progression of external root resorption?
Resorptive
Which stage of external cervical resorption?
- Dentin and cementum are progressively replaced by fibrovascular lesion
Repair
Which stage of external cervical resorption?
- Fibrovascular lesion ultimately becomes calcified to develop into fibro-osseous tissue
False - NOT self-limiting (usually exhibits a prolonged resorption phase)
T/F: The process of External cervical resorption (Invasive Cervical Resorption) is self-limiting
Pericanalar resorption resistant sheet (PRRS)
An external cervical resorption lesion will not involve the pulp until the very end stages due to the __________ of predentin adjacent to the pulp tissue
External cervical resorption (Invasive Cervical Resorption)
ID the type of resorption:
- Often asymptomatic until late stages, and may be misdiagnosed as caries
- Possible pink spot in the cervical aspect of the tooth, near gingival margin
- Often hemorrhagic on probing
- Feels hard and scratchy when probed (unlike subgingival caries which feels sticky)
External cervical resorption (Invasive Cervical Resorption)
A patient presents asymptomatic with a pink spot in the cervical aspect of the tooth, near the gingival margin. Upon probing, the pocket is hemorrhagic and feels hard/scratchy. What is the most likely diagnosis?

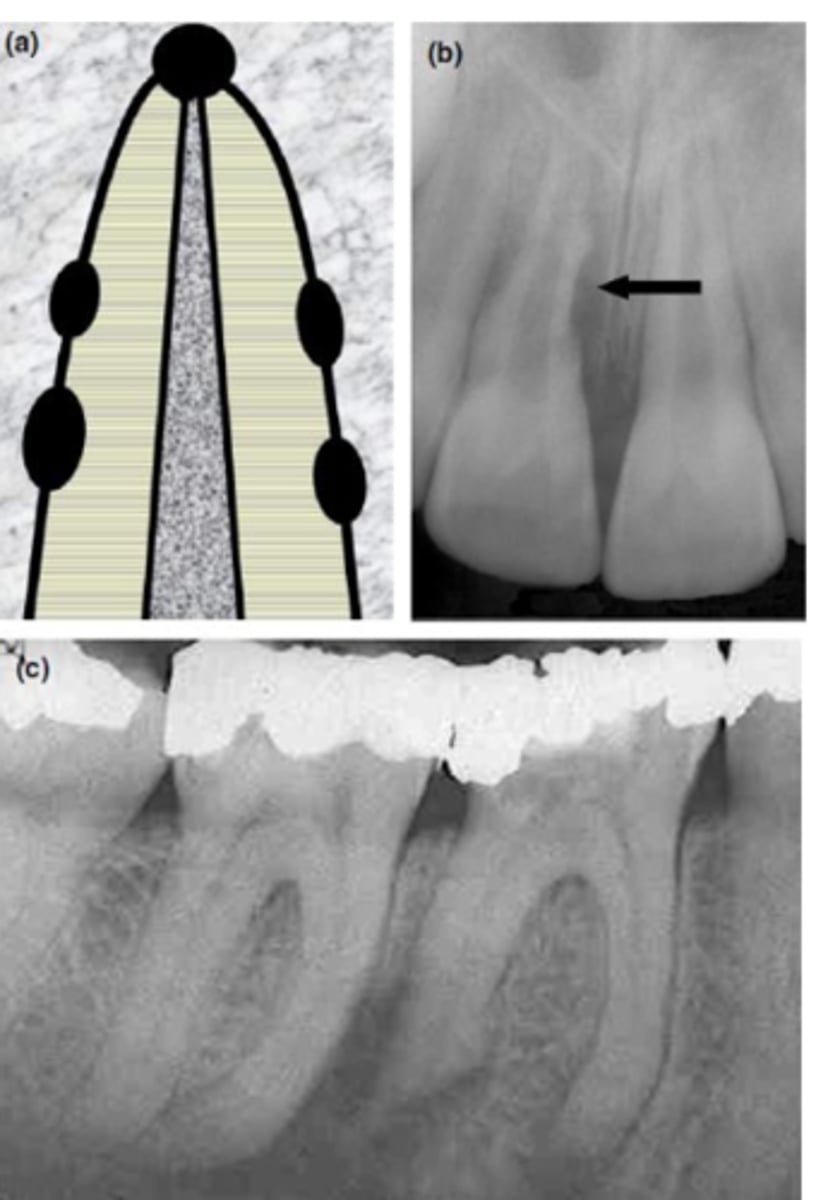
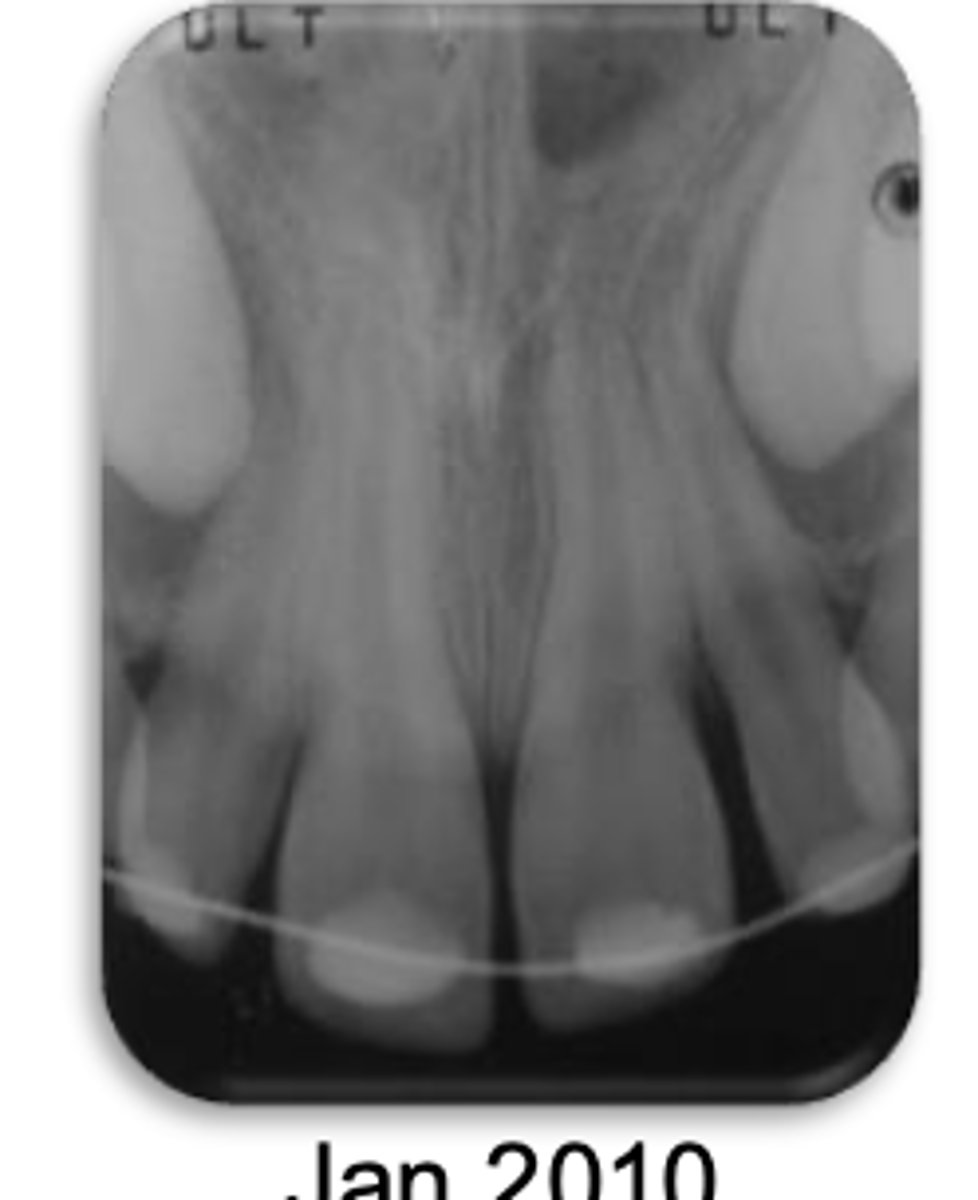
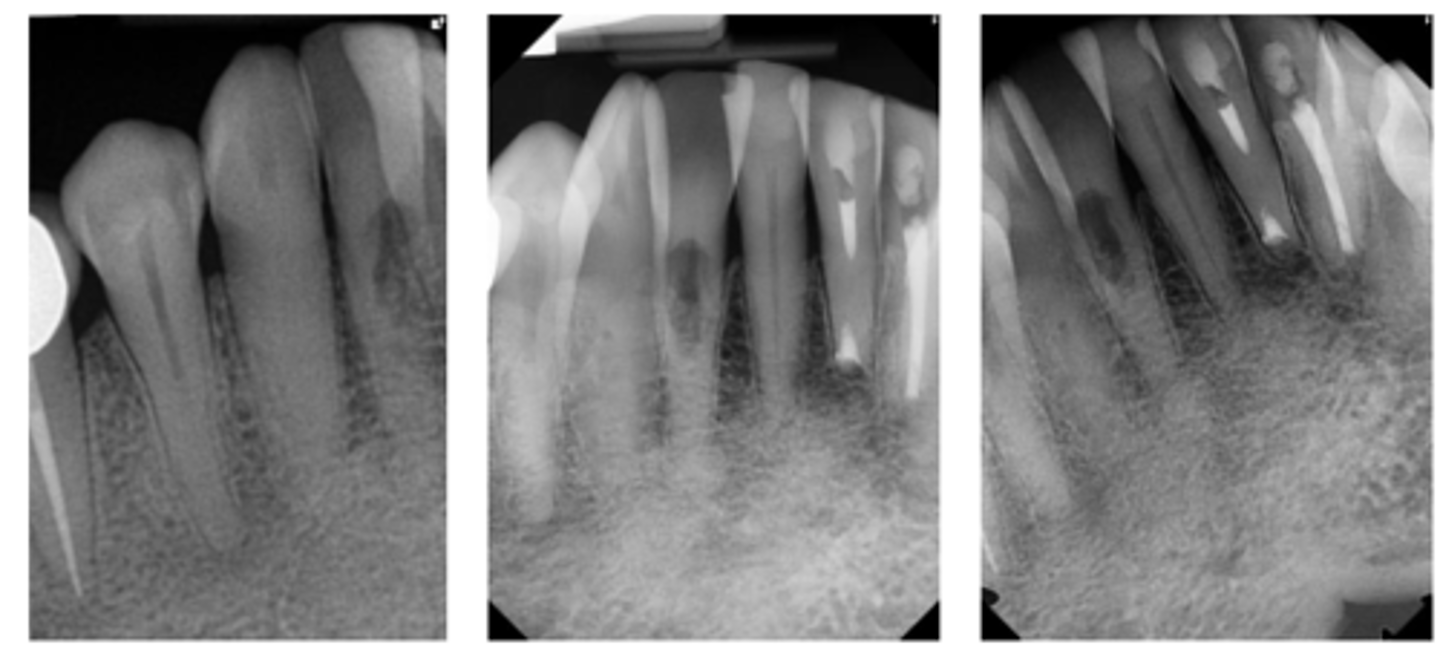
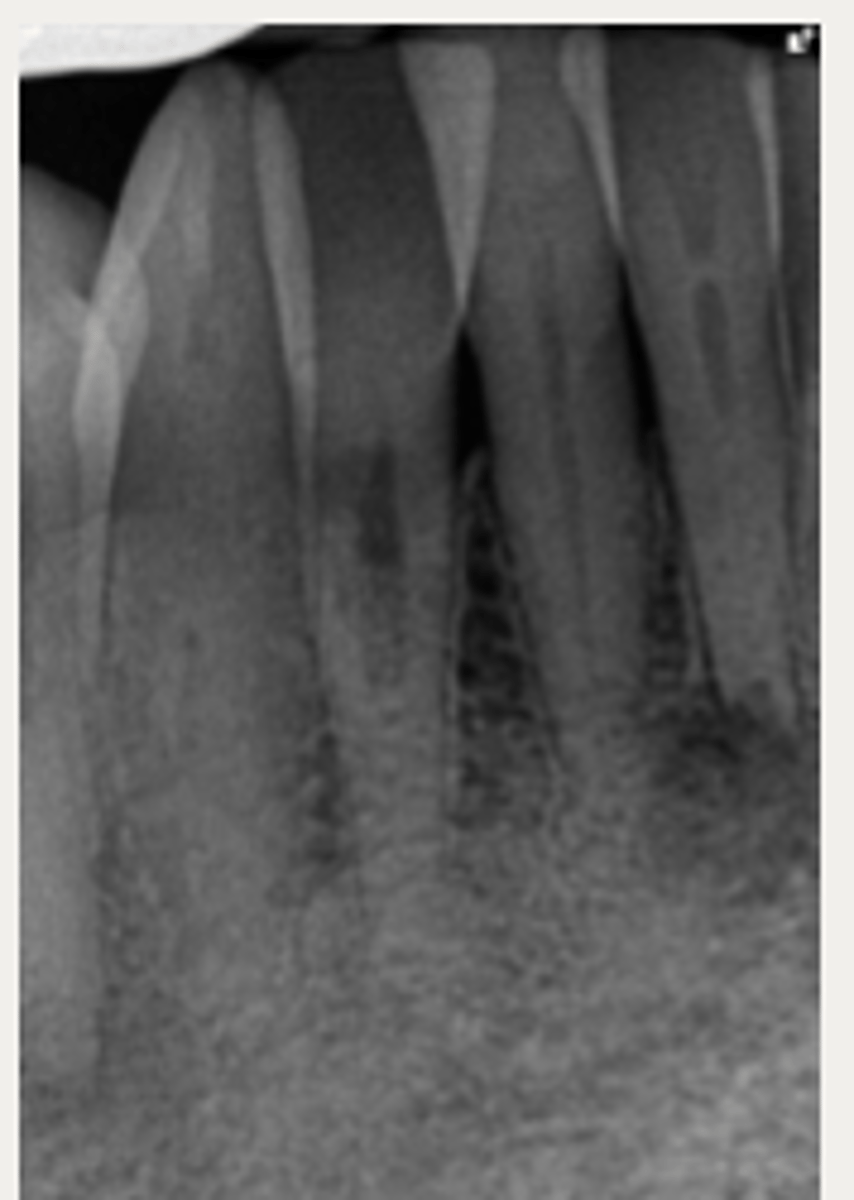
External cervical resorption (Invasive Cervical Resorption)
ID the type of resorption:
- Usually an incidental radiographic finding, especially for less advanced lesions
- Variable appearances; may be a well-defined or irregular radiolucency around the cervical aspect of the tooth
- A portal of entry is always present in the cervical region of the tooth
- The chamber/canal outline is often visible as the innermost layer of predentin around the chamber is not resorbed
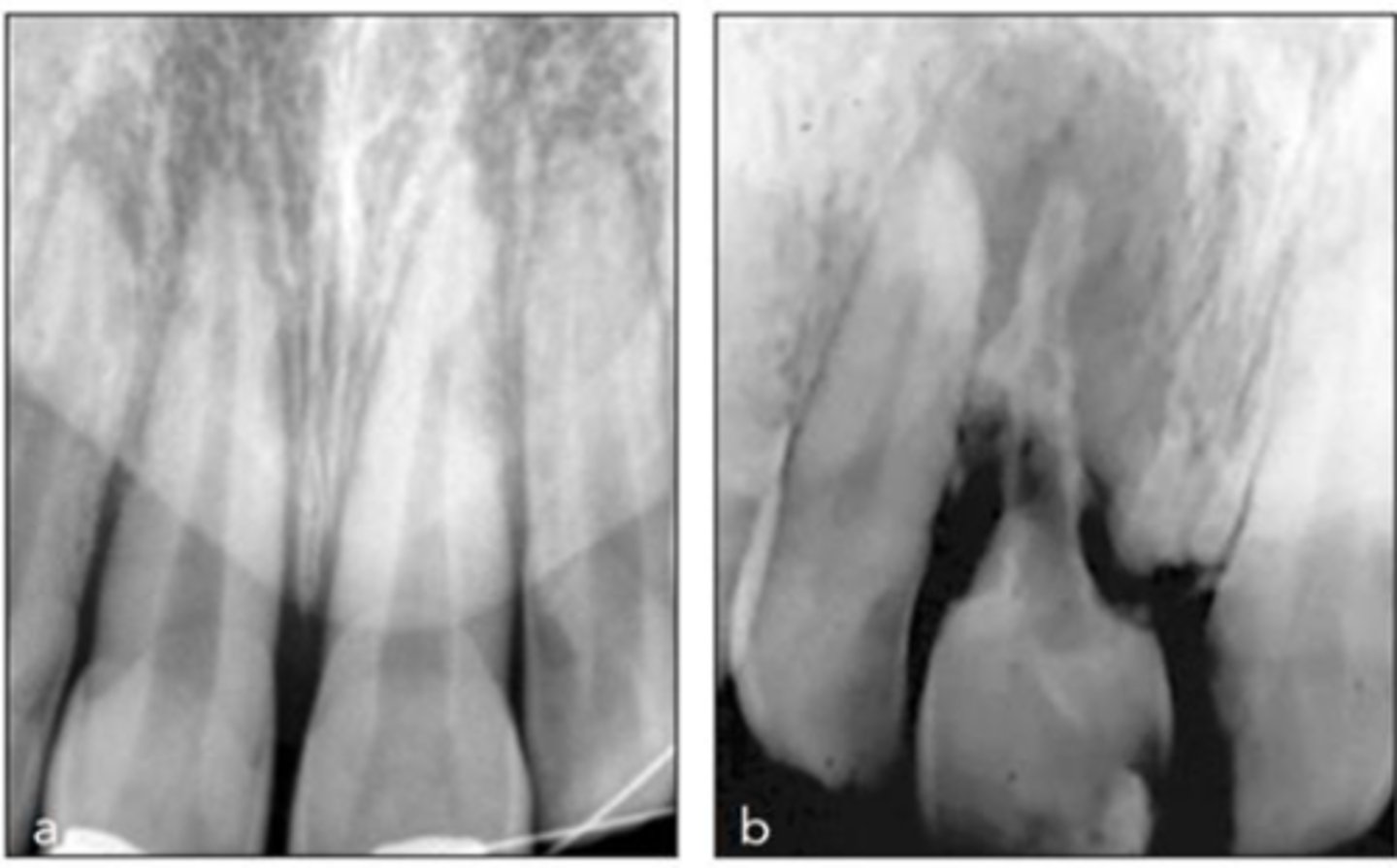
External cervical resorption (Invasive Cervical Resorption)
Patient presents with these radiographic findings, what type of resorption?
- Incidental finding
- Radiolucency around cervical aspect of tooth
- Portal of entry present in cervical region
- Chamber/canal outline is visible
External cervical resorption (Invasive Cervical Resorption)
What type of lesion is similar to internal resorption but is distinguished by taking an off-angle PA in which the lesion moves?
Internal inflammatory resorption
If you take an off-angle PA and the lesion does NOT move, what do you suspect?
CBCT
What is the gold standard for diagnosis and treatment planning of External Cervical Resorption (ECR) lesions?
Heithersay Classification for External Cervical Resorption
What is a system used to categorize External Cervical Resorption (ECR) based on the extent of the lesion's penetration into the tooth's structure, visualized through periapical radiographs?
- Monitor the lesion
- Intentional replantation
- Extraction
- External surgical repair only
- External surgical repair with RCT
- Internal repair with RCT
What are six treatments for External Cervical Resorption (ECR)?
Monitor the lesion
These are a part of which treatment for External Cervical Resorption (ECR)?
- For lesions that are asymptomatic, but have progressed too far to treat without irreparable damage to tooth, or where the resorptive lesion is inaccessible to treatment
Intentional replantation
These are a part of which treatment for External Cervical Resorption (ECR)?
For inaccessible lesions
- Atraumatic extraction
- Debride and restore lesion +/- RCT
- Replacement of tooth in socket +/- flexible splint
- RCT, if necessary, can be done before, after, or during the replantation
Extraction
These are a part of which treatment for External Cervical Resorption (ECR)?
- For symptomatic, untreatable lesions, or for
patients who wish to be proactive about treatment
External surgical repair only
These are a part of which treatment for External Cervical Resorption (ECR)?
For lesions that are accessible through raising a flap and that are unlikely to have pulpal involvement after removal
- Raise a flap
- Complete debridement of the resorptive lesion
- Tx with 90% trichloroacetic acid (TCA) or 5.25% NaOCl
- Restoration of defect with resin-modified glass ionomer (Geristore) or Biodentine
- Flap closure and suturing
External surgical repair with RCT
These are a part of which treatment for External Cervical Resorption (ECR)?
For lesions with a large portal of entry where the resorptive defect would be accessible by raising a flap without having to remove excessive marginal bone:
- Same as the external repair only approach
- RCT may be completed before or after the repair, if care is taken to prevent canal blockage when restoring the defect first
Internal repair with RCT
These are a part of which treatment for External Cervical Resorption (ECR)?
For lesions with a small portal of entry where the resorptive lesion is in close approximation to the chamber/canals
- Root canal therapy is initiated
- Resorptive lesion is debrided through the access cavity using 90% TCA or NaOCl
- Root canal therapy is completed
- Resorptive defect is restored using RMGI, Biodentine, or Bioceramics (ERRM) depending on the level and extent of the perforation
Classes 1 and 2
According to a study by Heithersay evaluating outcomes of ECR lesions with root canal therapy and surgical defect repair over a period of 3 years, which class(es)?
- 100%
Class 3
According to a study by Heithersay evaluating outcomes of ECR lesions with root canal therapy and surgical defect repair over a period of 3 years, which class(es)?
- 77.8%
Class 4
According to a study by Heithersay evaluating outcomes of ECR lesions with root canal therapy and surgical defect repair over a period of 3 years, which class(es)?
- 12.5%
no treatment (depends on case)
Which treatment has the best prognosis for External Cervical Resorption (ECR)?
External
According to the Mavridou study, do external or internal treatment approaches have better prognosis for External Cervical Resorption (ECR) treatment?