psychopathology test 3 miller
1/220
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
221 Terms
hallmark of Bulima
Binge- eating excess amounts of food
eating is perceived as uncontrollable
associated medical features of bulimia
most are within 10% of normal weight
purging can result in severe medical problems
erosion of dental enamel, electrolyte imbalances
kidney failure, cardiac arrhythmia, seizures, intestinal problems, permanent colon damage
associated psychological features of bulimia nervosa
most are overly concerned with body shape
fear gaining weight
between binges, individuals typically restrict calories and avoid high fat foods and "trigger" foods
high comorbidity- anxiety, mood, and substance abuse
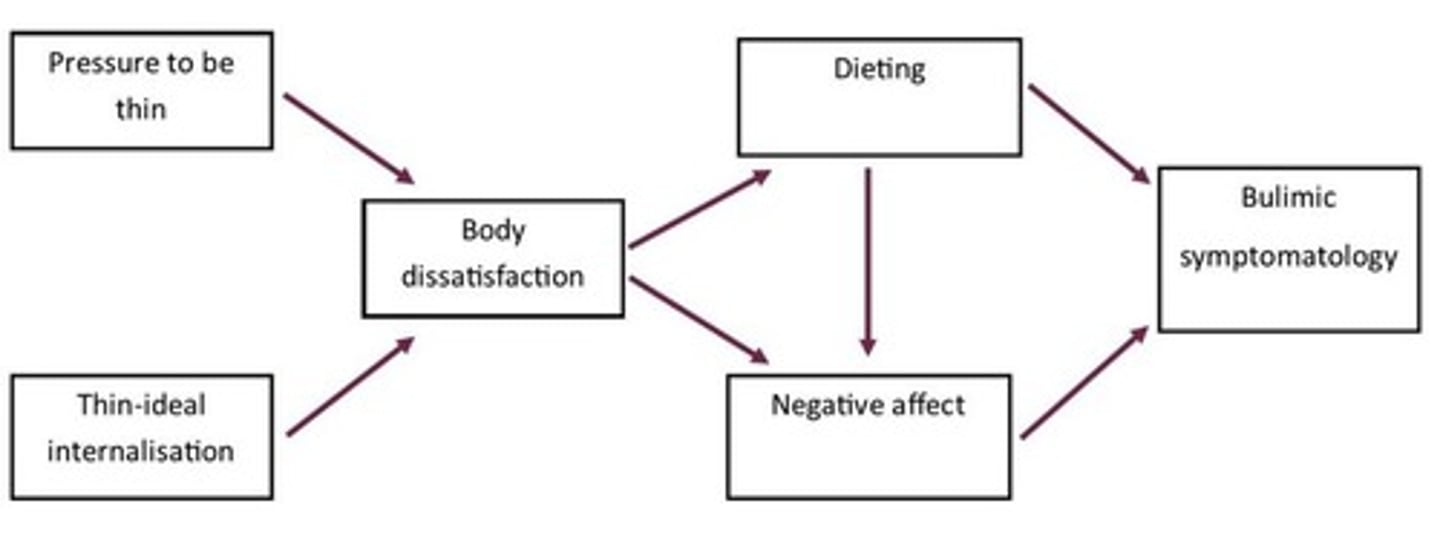
***Stice's dual pathway model of bulimic pathology***
distal to more proximal
longitudinal module
hallmark of anorexia
successful weight loss
anorexia nervosa defining features
restriction of energy intake relative to requirements that leads to significantly low body weight in context of age, sex, developmental trajectory, and health
-defined as 15% below expected body weight (DSM- IV; DSM-V doesn't say this)
often begins with dieting
intense fear of obesity
disturbance in way one's body shape is perceived; denial of seriousness of the problem; large impact on self-evaluation
DSM-5 subtypes of anorexia
restricting subtype
binge-eating-purging subtype
restricting subtype
limit caloric intake via diet, fasting, and excessive exercise
binge-eating-purging subtype
like bulimia but with significant weight loss
associated features of anorexia nervosa
marked disturbance in body image
high comorbidity with other psychological disorders
weight loss methods have life threatening consequences
never satisfied with weight- need continuous loss to feel comfortable
medical consequences of anorexia nervosa
amenorrhea (women not having regular periods)
dry skin
brittle nails and hair
sensitivity to cold temperatures
lanugo- downy hair on limbs and cheeks
cardiovascular problems
psychological consequences of anorexia
depression, withdrawal, anxiety, irritability, reduced sex drive
-may be secondary to starvation
binge-eating disorder: overview and defining features - appendix of DSM-IV-TR; "full" diagnosis in DSM-5
engage in food binges without compensatory behaviors
perceived loss of control during binges
binging associated with: eating more rapidly until uncomfortable fully; when not hungry; feeling embarrassed about intake; feeling disgusted/guilty afterwards
distressed about binge eating
1 a week for at least 3 months
binge-eating disorder associated features
many are normal weight/overweight or obese
often older than bulimics and anorexics
more psychopathology vs. non-binging obese people
concerned about shape and weight
binging used as a coping mechanism
no major difference across gender or cultural/racial groups (unlike anorexia and bulimia) -- this used to not be true
bulimia facts and statistics
-Majority are female - 90%+
-Onset typically in adolescence (16-19)
-Lifetime prevalence is about 1.1% for females, 0.1% for males
-6-8% of college women suffer from bulimia at some point
-Tends to be chronic if left untreated
-childhood obesity and early pubertal onset risk factors
anorexia facts and statistics
Majority are female from middle- to upper-middle-class families
Usually develops around age 13 or early adolescence
More chronic and resistant to treatment than bulimia
bulimia and anorexia are found in westernized cultures
immigrants from other countries often develop symptoms
lower rates in African American and Asian females
integrative model ~ causes of bulmia and anorexia
media and cultural considerations
-being thin= success, happiness
-cultural imperative for thinness translates into
dieting
- media standards of the ideal are difficult to
achieve
-"playmates"
- peer groups may act as a transmission path
for body image concerns and coping
behaviors (e.g., dieting, exercise)
-cultural differences USED TO serve as protective
factors
-now equivalent rates across ethnic groups
in US
- LGBTQ+ at risk, Food insec. at risk
biological considerations for bulimia and anorexia
50% due to genetic factors (not clear what is inherited)
common fears for ED
fear of judgement (weight gain, fear of eating in social situations, disliking how body feels due to weight gain, feeling tense around food
medical treatment for bulimia
antidepressants- help reduce binging and purging
antidepressants are not efficacious in the long term
psychological treatment for bulimia
Cognitive behavior therapy
-Treatment of choice
didactics (consequences of binging and purging; ineffectiveness)
scheduled eating (5-6 meals; short interval between meals)
challenge automatic and dysfunctional thoughts
monitoring purges and graduates plan for decreasing them; use new coping skills or distraction to handle urges to purge
interpersonal psychotherapy- gains similar to CBT but doesn't work as fast
binge eating disorder medical treatment
sibutramine (Merida) -used to control hunger
binge eating psychological treatment
CBT for bulimia
Interpersonal psychotherapy has been as effective as CBT
there is some evidence to suggest self-help books/ techniques are also effective
treatment for anorexia nervosa
medical- none exist with demonstrated efficacy
psychological treatment:
- weight restoration: primary initial goal
- if below 70% of weight, inpatient treatment
preferred
- weight gain is often easiest part
- understand that they are not going to
be made overweight
- use numerous, small meals
- eat under supervision
- reinforcements provided
- confront self-defeating behavior
psychoeducation- food, weight, nutrition, health
behavioral and cognitive interventions
-treatment likely to be unsuccessful without
cognitive restructuring
treatment often involves family
long-term prognosis- poorer than bulimia
schizophrenia vs psychosis
psychosis- broad term (e.g., hallucinations, delusions)
schizophrenia- a type of psychosis
psychosis and schizophrenia are heterogeneous
lots of ways and reasons for psychosis
different "types" of schizophrenia
disturbed thought, emotion, behavior
Emil Kraepelin
father of psychiatric classification
used the term dementia praecox (premature dementia)
-focused on subtypes of schizophrenia (paranoid;
catatonic)
-recognized it as a "disease of the brain"
-recognized that several distinct symptoms
appeared to be part of a broader syndrome
-differentiated "dementia praecox" from manic-
depressive illness
Eugen Bleuler
introduced the term "schizophrenia"
"splitting of the mind"; inability to keep a consistent train of thought
described "positive" and "negative" symptoms
characteristics of schizophrenia
two (or more) of the following, each present for a significant portion of time during a 1 month period (or less if successfully treated)
1. delusions
2. hallucinations
3. disorganized speech (frequent derailment or incoherence)
4. grossly disorganized or catatonic behavior
5. negative symptoms (affect flattening, alogia, avolition)
criteria for schizophrenia
social/occupational dysfunction
continuous signs of disturbance for at least 6 months
not schizoaffective or mood disorder
positive symptoms of schizophrenia
active and obvious manifestations of abnormal behavior
excess or distortion of normal behavior
delusions
distortion in thought content
erroneous beliefs that usually involve a misinterpretation of perception or experiences. Beliefs are typically held very strong
gross misrepresentations of reality
types of delusions
persecutory (most common)
referential
erotomanic
somatic
nihilistic
grandiose
"bizarre delusions"
persecutory delusion
"FBI is after me"
most common
referential delusions
"when madonna waves at the audience, she was really waving at me"
erotomanic
madonna is in love with me
somatic
my liver is dead and rotting inside me
nihilistic
the world is ending
grandiose
i am the president of the entire world
bizzare delusions
false beliefs that could not possibly be true, given what is known about the world
Hallucinations
experience of sensory events without environmental input
can experience in any sensory
(auditory, visual, olfactory, gustatory, tactile)
most common hallucination
auditory "voices"
scary form~ "command" hallucinations
2 or more voices running commentary are considered highly characteristic of SZ
delusions and hallucinations may have a congruent theme
findings of imaging studies
subtle structural damage in parts of brain associated with auditory processing
-thinner cortex
in fMRI studies, activation of auditory regions during auditory hallucinations
negative symptoms
absence or insufficiency of normal behavior
spectrum of negative symptoms
Avolition (or apathy) - lack of initiation and persistence
Alogia - relative absence of speech
Anhedonia - lack of pleasure, or indifference
Affective flattening - little expressed emotion
-prodromal symptoms (first seen)
-face immobile and unresponsive
-may not be indicative or experienced emotion
-flat affect may appear before others
Disorganized symptoms
include severe and excess disruptions in speech, behavior, and emotion
nature of disorganized speech
tangentiality-"going off on a tangent"
cognitive slippage/loose associations- conversation in unrelated directions
word salad; neologisms (make-up new words)
nature of disorganized behavior
includes a variety of emotional behavior
(disheveled; odd appearance; inappropriate or unpredictable behavior)
Nature of disorganized affect
inappropriate emotional behavior
-behavior not consistent with context (e.g., smiling when talking about death)
catatonia
disorganized behavior
wild agitation, waxy flexibility, immobility
schizophreniform disorder
schizophrenic symptoms for a few months (less than 6; more than 1)
impaired functioning not required
some never progress on to schizophrenia but more do (schizoaffective disorder)
schizoaffective disorder
Symptoms of schizophrenia and a mood disorder
Both disorders are independent of one another
Prognosis is similar for people with schizophrenia
Such persons do not tend to get better on their own
Need to have delusions and/or hallucinations that are present for at least 2 weeks in the absence of the mood disorder
bipolar type schizoaffective disorder
if mania is part of the presentation
Depressive Type of Schizoaffective Disorder
if only major depressive episodes are part of the presentation
delusional disorder
presence of one or more delusions that persist for 1 month or more
lack other positive and negative symptoms
disorganization is not present
types include:
- erotomanic-someone else is in love with this person
-grandiose
-jealous
-persecutory
-somatic-involves bodily functions or sensations
-bizarre
brief psychotic disorder
-one or more positive symptoms of schizophrenia
-delusions, hallucinations, disorganized behavior/speech
-lasts at least 2 days, but not longer than 1 month
-not due to substance use
-usually precipitated by extreme stress or trauma
-tends to remit on its own
schizotypal personality disorder
may reflect a less severe form of schizophrenia
Process vs. Reactive Distinction
-Process - insidious onset, biologically based, negative symptoms, poor prognosis
-Reactive - acute onset (extreme stress), notable behavioral activity, best prognosis
good vs. poor premorbid functioning in schizophrenia
-focus on functioning prior to developing schizophrenia
-no longer widely used
type 1 vs type 2 distinction
type 1- positive symptoms, good response to medication, optimistic prognosis, and absence of intellectual impairment
type 2- negative symptoms, poor response to medication, pessimistic prognosis, and intellectual impairments
paranoid type of schizophrenia
presence of prominent hallucinations and delusions (usually persecutory or grandeur) but have relatively intact cognitive skills and affect. Organized around coherent theme
do not show disorganized behavior (speech, thought or affect)
later onset
the best prognosis of all subtypes
disorganized type (hebephrenic)
-Marked disruptions in speech and behavior
-Flat or inappropriate affect
-Hallucinations and delusions, if present, tend to be fragmented (unlike paranoid type)
-Develops early, tends to be chronic, associated with a continuous course without remissions
catatonic-type schizophrenia
show unusual motor responses and odd mannerisms
- immobility
-excessive motor activity
-motor negativism (resistance to instructions or attempts to be moved)
-waxy flexibility
tends to be severe and quite rare
examples include echolalia (mimic or repeat words) and echopraxia (mimic movements)
undifferentiated type schizophrenia
Wastebasket category
Major symptoms of schizophrenia
Fail to meet criteria for another type
residual type of schizophrenia
past diagnosis of schizophrenia
absence of prominent delusions, hallucinations, disorganized speech and behavior
continue to display less extreme residual symptoms
-presence of negative symptoms common
-or, attenuated positive symptoms (weird beliefs, eccentric behavior)
cant talk about personality disorders without
personality
funder
Personality is "an individual's characteristic patterns of thought, emotion, and behavior, together with the psychological motivations behind those patterns."
Millon
a personality trait is "a long-standing pattern of behavior expressed across time and in many different situations"
5 factor model
open to experience
conscientiousness
extraversion
agreeableness
neuroticism
open to experience
tendency to be original, have broad interests, be open to a wide range of stimuli, be daring and take risks
conscientiousness
how dependable, responsible, achievement-oriented, and persistent one is
extraversion
A personality dimension describing someone who is sociable, gregarious, and assertive
agreeableness
how trusting, good-natured, cooperative, and soft-hearted one is
neuroticism
anxiety, insecurity, emotional instability
personality disorders are composed of personality traits that are:
Inflexible
Maladaptive
a significant functional impairment or subjective distress
inflexible
adaptive personality is flexible but not unstable
the nature of personality and personality disorders
enduring and relatively stable predispositions (i.e., ways of relating and thinking)
predispositions are inflexible and maladaptive, causing distress and/or impairment
coded on Axis II of the DSM-IV and DSM-IV-TR
-problems: PD's "neighbor" and reputation
various personality disorders are associated with
-Decreased social functioning
-Decreased occupational functioning
-Increased risk of substance abuse
-Increased risk of depression and anxiety
-Increased risk of schizophrenia
-Increased risk of suicide
-Increased risk of imprisonment
-Increased risk of hospitalization
the DSM-IV/5 gives these general criteria for all personality disorders: (category A)
no one diagnoses on these but he still wants us to know
A. an enduring pattern of inner experience and behavior that deviates markedly from the expectations of an individual's culture. This pattern is manifested in two (or more) of the following areas
Cognition, Affectivity, Interpersonal Functioning, Impulse Control
Christmas | Adds | Interesting Fun | In Children
cognition
i.e., ways of perceiving and interpreting self, other people, and events
affectivity
range, intensity, lability, and appropriateness of emotional response
rest of criteria for personality disorders from DSM
b. the enduring pattern is inflexible and pervasive across a broad range of personal and social situations
c. the enduring pattern leads to clinically significant distress or impairment in social, occupational, or other important areas of functioning
d. the pattern is stable and of long duration, and its onset can be traced back to adolescence or early adulthood
borderline PD: dimensional vs categorical
5 of 9 symptoms have "it"; 4 of 9 do not have "it"
once have "it", presumed to look alike
-126 different ways to have 5 BPD symptoms
- not meeting criteria (e.g., 3-4 symptoms) not the
same as being asymptomatic
cut-offs not empirically derived- don't look different; don't function differently
cause problems with stability and inter-rater reliability
almost unanimous consensus that PDs should NOT be used in a categorial manner
dichotomizing dimensional variables always results in
a loss of information
cause problems with stability and inter-rater reliability
Frances
head of DSM 4; was head of Duke psychiatry for years
"not whether, but when and which"
Comorbidity in Personality disorders
if diagnosed with a PD, likely have more than just 1 personality disorder
gender differences in PD
certain PDs believed to be more common in men vs women
men: paranoid, Schizoid, schizotypal (cluster A), antisocial, narcissistic, OCPD
women: histrionic, borderline, dependent
coverage
most common PD diagnosis in clinical practice - PD NOS (not otherwise specified)
-have a PD not recognized by DSM
-have features or more than one PD but don't meet criteria for any specific PD but features cause distress/impairment
The 10 DSM-5 personality disorders: Cluster A ("the weird")
Paranoid PD (DSM tried to drop )
Schizoid PD (DSM tried to drop)
Schizotypal PD
Please | Stop | Screaming
paranoid PD
is a pattern of distrust and suspiciousness such that others' motives are interpreted as malevolent.
Schizoid PD
a pattern of detachment from social relationships and a restricted range of emotional expression
Schizotypal PD
a pattern of acute discomfort in close relationships, cognitive or perceptual distortions, and eccentricities of behavior
Cluster B (wild) personality disorders
antisocial
borderline
histrionic
narcissistic
A | Baboon | Has | Nothing
antisocial PD
pattern of disregard for and violation of the rights of others
borderline PD
Pattern of instability in interpersonal relationships, self-image, affects, and marked impulsivity.
histrionic PD
pattern of excessive emotionality and attention seeking
DSM tried to drop
Narcissistic PD
grandiosity, need for admiration, lack of empathy
DSM tried to drop these
Paranoid PD
Schizoid PD
Histrionic PD
People | Stopped | Having
Cluster C personality disorders ("the worried")
avoidant
dependent
obsessive-compulsive (OCPD)
A | Dark | Open Casket
avoidant PD
pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation