lumbar mobilization
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
fryette's first law
- in neutral
- SBing and rotation occur to opposite sides
*if lumbar spine side bends to the right, it rotates to the left
fryette's second law
- in flexion or extension
- SBing and rotation occur to the same side
*in flexion, if the lumbar spine side bends to the right, it also rotates to the right
fryette's third law
when motion is introduced in one plane, it will decrease motion in the other two planes
when should you do combined motions?
when straight plane movements don't provocate symptoms
indication for manipulation
- no sxs distal to the knee
- recent onset of sxs (<16 days)
- low FABQ score (<19)
- hip IR ROM >35 for at least 1 hi[
combined motions - opening restriction
limitation in flexion, SBing, and rotation AWAY from the painful side
combine motions - closing restriction
limitation in extension, SBing, and rotation TOWARD the painful side
lateral stenosis will have pain with max
closing
disc herniation will have pain with max
opening
PPIVM/PAIVM mobility categorization
- normal
- excessive/hypermobile
- reduce/hypomobile
with PAIVM you're looking for
end feel!
- normal
- abnormal (spasm, soft, hard/capsular)
PPVIM/PAIVM is most reliable for
pain provocation and finding the most hypomobile segment
lumbar forward/backward bending PPVIM
- pt side-lying, with hips and knees flexed
- support pt leg with one arm and palpate between SPs with the other
- gradually flex and extend the pts trunk via the hips by shifting your weight laterally
- should feel space between SPs "opening"/"closing" as SPs separate
lumbar SBing PPVIM sidelying
- pt side-lying, hips and knees slight flexed
- IR/ER pts hips to induce passive sidebending
- compare motion betweeen segments and with contralateral motion
lumbar SBing PPVIM prone
- pt prone with pillow under stomach
- abduct pts leg to induce sidebending
(left hip abd = left SBing)
central PAIVM
- pt prone with pillow under abdomen
- use thumb or pisiform to apply pressure to target SPs
- assess end-feel, mobility, and pain
unilateral PAIVM
- pt prone with pillow under abdomen
- use thumb or pisiform to apply pressure to target TPs
- apply a gentle, anterior force toward the table
- assess end-feel, mobility, and pain
when doing unilateral PAIVM, if the patient has pain and hypomobility when pressing on L TP then what may be the problem
- closing problem on the L (extension, L SB, L ext quadrant)
- opening problem on the R (flexion, L SB, L flexion quadrant)
mobilization dosing
- initial: 2-3x per week
- session: 3-5 mob sets per restricted segment
central vs unilateral PA mobilization
- central assists with sagittal plane motion of forward and backward bending
- unilateral enhances rotation and SBing
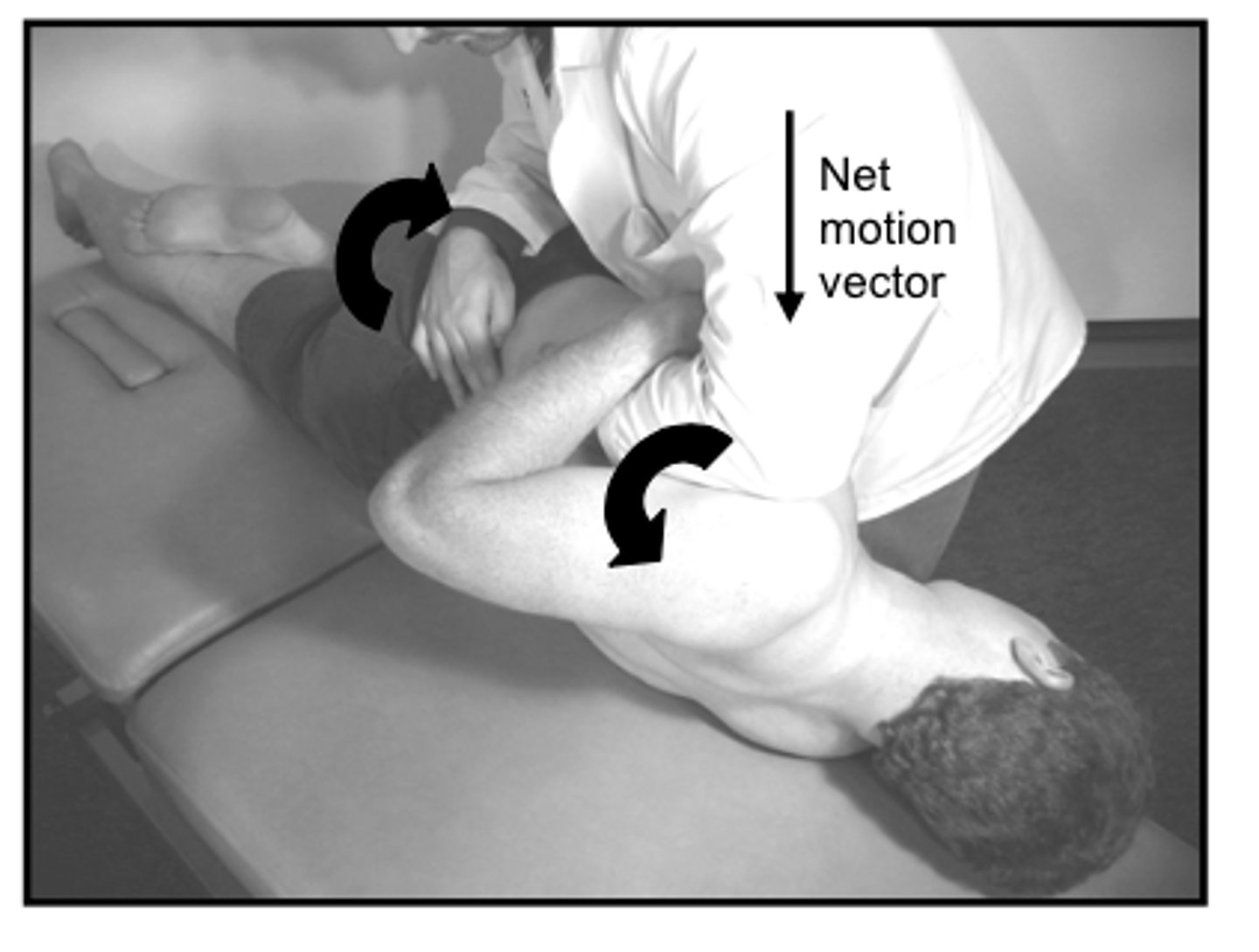
rotation gapping
- hand closest to their head goes under their arm --> then rotate their shoulder anteriorly
- other hand rotates their pelvis until slack is taken up (then back out a little)
- thumb of hand closest to head pushes superior vertebrae up
- 2 and 3 fingers of other hand pushes inferior vertebrae down
- continue rotating torso and pelvis