327 Exam 1 Pharmacotherapy of HTN
1/101
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
102 Terms
Goals of Hypertension
Reduce CVS and overall morbidity and mortality. Use of non-pharmacologic and pharmacologic therapy that has been demonstrated in large-scale clinical trials to reduce the long-term morbidity and mortality associated with hypertension. Address, Incorporate, Prevent, Simplify, Promote, Maintain and Improve
Difference between clinical BP and Ambulatory BP
Both cause mortality and CV mortality but masked HTN is more strongly associated with all-cause mortality than sustained HTN
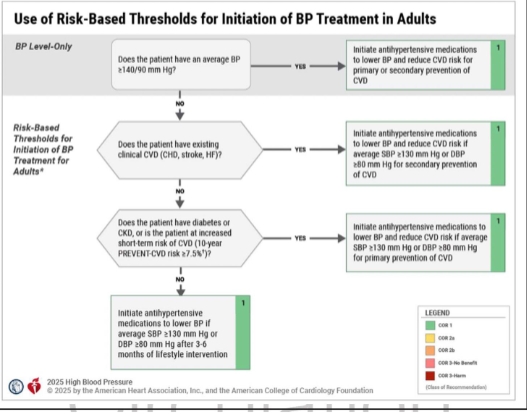
Risk Based Thresholds for Initiation of BP Treatment in Adults
General Lifestyle Modifications
Weight reduction, DASH diet, decrease dietary sodium, increase physical activity, stress reduction, and moderate alcohol consumption
DASH Diet
Dietary Approaches to Stop Hypertension: 8-10 Servings a day of fruits and vegetables, 2-3 servings of low far dairy products, a diet which is low in saturated fats and cholesterol, increase potassium to 4.7 grams per day
Potassium-based salt
Recommended for patients w/ and w/o HTN. Contraindicated in patients with CKD and on meds that reduce potassium secretion (ACEI, ARBs, Potassium-sparring diuretics)
Exercise Recommendations
3-4 Sessions per week, on average lasting 40 minutes per session with moderate to vigorous intensity. Or exercising 160 minutes per week of moderate to vigorous exercise
Glutamic Acid
Vegetable protein, Inverse relationship to lowering BP, animal proteins may increase BP
Red and Blue berries
Contain antioxidants known to help lower blood pressure
Napping and Hypertension
Midday naps had a noticeable drop in BP. On average 5mm Hg drop in blood pressure
Dietary factors of unknown or controversial benefit
fish oil, fiber, calcium, magnesium, carbohydrate, saturated fats, omega-6 polyunsaturated fats, monounsaturated fats
Strategies to Dosing Antihypertensive Medications
Start one drug, titrate to max dose and then add a second drug
Start one drug and then add a second drug before achieving max of the initial
Begin with 2 drugs at the same time, either as 2 separate pills or a single pill combination especially if Stage 2 hypertension
Risk Estimation of BP Treatment Threshold
Does the patient have an average BP >140/90
Does the patient have existing CVD
Does the patient have diabetes or CKD or is the patient’s short-term risk of CVD
Is the SBP >130mm Hg or DBP >80 mmHg after 3-6 months of lifestyle interventions
PREVENT Risk Score
Ages 30-79, Uses more recent data, used additional risk factors, 10-30 year risk estimates, tends to be lower than ASCVD risk score, most likely more accurate but less used
ASCVD Risk Score
Ages 40-79, used data from 1960-1990, traditional risk factors such as age, sex, BP, cholesterol, 10 year risk estimates
Goal BP
<130/80
Initial Monotherapy
Initiation with 2 first line agents of different classes, either as separate agents or in a fixed dose combination is recommended with stage 2 HTN an average BP of >20/10 the fixed target
First-line HTN Medications
Thiazide diuretics, Calcium Channel blockers, ACE inhibitors, ARBs
Examples of Thiazide Diuretics
HCTZ, chlorthalidone, indapamide, metolazone
Examples of Loop diuretics
Furosemide, bumetanide, torsemide
Examples of Potassium sparing diuretics
Triamterene, amiloride
Examples of Aldosterone Antagonists
Spironolactone, eplerenone
Thiazide Diuretics
Preferred over loop when CrCl >30 ml/min, they are all equally effective, and have ancillary benefits (reduced CV events, lower HF)
Side Effects of thiazide diuretics
Hypokalemia, hyperglycemia, hyperlipidemia, hyperuricemia, polyuria, and photosensitivity (sulfonamide)
Loop Diuretics
Not directly used for HTN, preferred for people whose CrCl <30 ml/min
Side effects of loop diuretics
Similar to thiazide, usually dose related, hypocalcemia (blocks Na and Ca reabsorption)
Potassium sparing diuretics
Help prevent the loss of potassium and magnesium that normally occur with thiazide or loop diuretics. They are weak antihypertensives but are additive in effect in combination with a thiazide or loop. Many drug interactions.
Side effects of potassium sparing diuretics
Hyperkalemia
Aldosterone Antagonists
Additive hypotensive effects when used in combination with thiazide or loop agent. Inspira is indicated for mono or combination therapy for hypertension
Spironolactone Dosing and Side effects
Min 25mg, max 400 mg, usually 25-50 mg max 2x/day. May decrease mortality in HF, associated with gynecomastia
Eplerenone (Inspra)
Min 25mg, usually 50mg up to 2x/day. Four weeks for full effect. Selective Aldosterone Receptor Antagonist. Broad range of interactions are likely.
What is eplerenone cleared through
CYP3A4 isozymes
Eplerenone (Inspra) Adverse effects
HA/Dizziness/GCT elevations, little evidence of gynecomastia, breast tenderness, menstrual irregularities. Avoid use if CrCl <50ml/min
ACE inhibitors
All are equally effective, differ in duration and tissue penetration, drug interactions are similar, can slow progression of HF, they are beneficial post MI, and they slow the progression of diabetic nephropathy.
ACEI side effects
Avoid in pregnancy due to teratogenicity, acute renal failure and death in neonates; Renal insufficiency, hyperkalemia. Hypotension (common in Na or volume depleted individuals), Cough, rash, RF (stop or reduce dose if CrCl inc. 35%), angioedema
Angioedema
Can occur in the face, larynx, and GI tract. Facial, airway, and tongue swelling. Can occur due to cross reactivity with other ACEI and ARBs
What is a major risk factor for the development of hyperkalemia with ACEIs?
Presence of renal dysfunction
Angiotensin II Receptor Blockers (ARBs)
Flat-dose response relationship. Monitor renal function while in use. Slight favor to ARBs over ACEI
Side effects of ARBs
Avoid in pregnancy (teratogenicity, acute renal failure in neonates), orthostatic hypotension, renal insufficiency, hyperkalemia, angioedema (less likely than ACEI), cross reactivity with ACEIs
ARB Monitoring
Monitor hyperkalemia: baseline is 102 weeks after initial dose or changes made. Monitor blood pressure lowering affects
Why should ACE inhibitors and ARBs not be used together
Combining them does not improve health outcomes but instead increases the risk of serious side effects like hyperkalemia and renal failure
Direct Renin Inhibitor
Newer class of antihypertensive. Drug is poorly absorbed, and high fat meals further reduce absorption. Available in 150mg or 300mg tablets, dose changes not necessary for renal or hepatic impairment. Generic name is Aliskiren and brand name is Tekturna.
Indication for Aliskiren
Treatment of HTN as monotherapy or in combination. Caution: angioedema and severe hypotension has been reported
Side effects of Aliskiren
Dose related GI effects, Rash, elevated uric acid levels, renal stone, single episode tonic-clonic seizures. <1% reported nasopharyngitis, dizziness, fatigue, upper respiratory infection, back pain, cough
Calcium Channel Blockers
All equally effective but use dihydropyridines over non-dihydropyridines. Differ in pharmacodynamic properties. Decreases risk of stroke but not as strongly as ARBs, no benefit to HF or CHD.
Examples of dihydropyridine
Amlodipine, felodipine, nifedipine
Examples of non-dihydropyridine CCB
Diltiazem, Verapamil
Dihydropyridine side effects
Reflex tachycardia, dizziness, flushing, headache, peripheral edema, drowsiness
Non-dihydropyridine side effects
Bradycardia, affects AV conduction, contraindicated in patients with AV block, dizziness, flushing, headache, peripheral edema
General Calcium Channel Blocker Side effect
Lower extremity edema (which is why it is not used in HF pts.), constipation, gingival hyperplasia
Important Counseling Points for CCBs
Report weight gain and peripheral edema to prescriber. May use stool softener if constipation occurs
Diltiazem Dosing
Usual: 180-240mg
Min-Max: 120-540mg
Once daily
Verapamil Dosing
Usual: 180-240mg
Min-max: 120-540
Once daily
ARB compared to CCB
ARB resulted in a 3-5% absolute lower rate of new onset diabetes than CCB. No difference in overall mortality. `
Beta Blockers
All BBs are equally effective in HTN. Useful post MI decreases both morbidity and mortality in HF pts. Lower HR but that may cause more MIs and increase CV deaths. Some are cardio selective and are safer in patients with asthma, PVD, and DM
Cardio selective BBs
Metoprolol, atenolol, bisoprolol. Cardioselectivity is dose related and variable
Non-cardioselective BBs
Propranolol, timolol
Side effects of Beta Blockers
Hypotension, bradycardia, fluid retention, fatigue
Contraindicated in pts with HR < 60 and SBP <100 mmHg
Proceed with caution in pts. with asthma/COPD
Increases triglycerides and decreases HDL-C
Weight Gain
Decreases exercise endurance
Little effect on LVH regression
BB Counseling
Monitor HR and BP. Use caution with positional changes, especially with initiation of medication. Initial fatigue may occur but may occur with time and steady state levels of medication. Do not stop abruptly taper over 10-14 days, can cause unstable angina, MI, or death.
Intrinsic Sympathomimetic Activity
No one uses these. But in theory it is better for patients with sinus bradycardia and PVD. Examples: pindolol, penbutolol, carteolol, acebutolol. Have alpha blocking activity as well as membrane stabilizing action.
Nebivolol
Brand name is Bystolic. It is a Beta-1 selective agent with nitric oxide vasodilating properties. Can cause HA, dizziness, diarrhea, and fatigue. It maintains systemic flow and blood flow to target organs; it lowers vascular resistance and supposedly have very little metabolic adverse effects. Comes in 2.5, 5, and 10mg doses
Losartan Intervention for Endpoint (LIFE) reduction study
Primary composite outcome with losartan, lower risk of fatal and nonfatal strokes, slightly lower risk of CVD, similar risk of myocardial infarction
Selective Alpha-1 Blocker
Should not be used strictly for hypertension, they lower BP but have a lot of potential side effects and inferior CV outcomes. Use cautiously in elders. Have adverse effects on morbidity and mortality. Add multiple drugs and it will increase the risk of HF.
Ancillary benefits of Alpha-1 Blockers
Benefit for benign prostatic hypertrophy. Also used for off label conditions such as PTSD, nightmare, Raynaud’s. It is lipid and glucose neutral.
Side effects of Selective Alpha 1-blockers
First dose hypotension, dizziness, palpitations, and possible syncope with changing positions. Usually happen with first dose and increased dose.
Alpha-1 Blockers Counseling points
Tell pts. to take at bedtime, orthostatic hypotension
Zilebersian
Is an RNA interference agent that inhibits hepatic angiotensin synthesis. In pts. with 200mg dose BP decreased 10/5 mmHg. Results were similar with high salt diets and with irbesartan. Side effects: Headache and injection site reaction
Obj of Medication in Research
To determine whether treatment with a CCB and/or an ACEI lowers the incidence of CHD or other CVD events vs treatment with a diuretic
Why is research in medicine so important
Very large population of people have HTN, must check for irregularities across the board. Looks to maximize safety across all pops. Can show that changes in recommended doses need to be made.
Main Outcome Measures
Primary outcome was fatal CHD or nonfatal MI. Secondary: mortality, stroke, combined CHD (Coronary revascularization procedures, angina, and hospitalization), combined CVD (stroke, angina, heart failure, and PAD)
ALLHAT Summary
No difference between chlorthalidone, amlodipine, and lisinopril in primary outcome and all-cause mortality. Amlodipine has a higher than of HF than chlorthalidone, and lisinopril vs chlorthalidone found a higher rate of HF, stroke, and combined CVD with lisinopril
SPRINT Trial
Tested whether a treatment strategy aimed at reducing systolic BP to <120 or <140 will reduce the occurrence of cardio-vascular disease. Found that CVD rates will be lower in the interventive intervention arm.
Central alpha-2 agonists
Clonidine, guanabenz, guanfacine, methyldopa. Can cause rebound hypertension.
Direct Vasodilators
Hydralazine and Minoxidil
Clonidine
.1, .2, and .3mg tablets or transdermal patch. Gradually DC over 1 week for oral therapy. Do not use in the elderly. Abrupt stop can cause rebound hypertension.
Combined Antihypertensive Therapy
For aggressive BP goals. Monitor effectiveness with added drugs.
Treating stable Ischemic Heart Disease
Target BP <130/80. First line meds: BBs, ACEIs/ARBs for pts. with previous MI or stable angina. Follow up with dihydropyridines, CCBs, mineralocorticoid receptor antagonists
Treating HTN with HF
Target is <130/80. Nondihydropyridines CCBs are not recommended for pts. with HF. Adults with HF and HTN after management of volume overload should be treated with ACE or ARB plus beta blocker plus other medications to goal
Treating HTN with patients with chronic kidney disease
Pts. with HTN and CKD (stage 3 or higher) treat with ACE inhibitors or ARB. After a kidney transplants treat with CCB to improve GFR and kidney survival
Treating HTN for secondary Stroke prevention
Should include thiazide, ACE, or ARB, or a combo of thiazide + ACE
Patients with Diabetes and Hypertension
Can use all first line: diuretics, Ace Inhibitors, ARBs, CCBs. ACE and ARBs should be considered in the presence of albuminuria
HTN in Black Adults
Can start thiazide or CCB. Can add ACE and ARB if necessary.
Women with HTN
Oral contraceptives can increase BP. Hormone replacement therapy does not raise BP. Consider other forms of contraception if necessary
Pregnant women with HTN
Use Nifedipine XR and/or labetalol. ACEI, ARBs, and direct renin inhibitors are contraindicated in pregnancy. Also avoid atenolol, nitroprusside, and Potassium sparing Diuretics. Can be counseled for low dose Aspirin to reduce the risk of preeclampsia for high-risk preeclampsia patients. Goal is to reduce <140/90 before 20 weeks gestation.
Urgent BP Control in Pregnancy
SBP is >160 and DBP is >110. Labetalol IV, Hydralazine IV or IM, Nifedipine (immediate release) orally
Elderly and HTN
Thiazide diuretics and long acting CCB. Start with small initial dose. ACEI is good choice if MI, HF, or CKD present. BB only if another condition warrants it. Avoid peripheral alpha blocker or central alpha agonists
Very Elderly and HTN
>80 years old. Lowering BP may delay dementia
Complementary medicine for HTN
Danshen, grape seed extract, cocoa, Astralagus, black tea, blueberry powder, beetroot juice, vitamin D
Resistant Hypertension
BP that remains above goal despite being on 3 different medications, ideally ne medication should be a diuretic. Screening for primary aldosteronism is recommended regardless of whether hypokalemia is present. See if a medication is possibly causing it. Consider renal denervation treatment
Causes of Resistant Hypertension
Poor BP technique, adherence, genetic factors, white coat effect, obesity, alcohol, dietary salt, drug related causes.
Treatment of Resistant Hypertension
Eplerenone and spironolactone are preferred in primary aldosteronism and resistant hypertension. Can be added as fourth agent. Avoid potassium supplements or potassium sparing diuretics in people with severe renal dysfunction. If K-sparring meds cannot be tolerated try BBs, ABs, or direct vasodilators
Renal Denervation
A procedure that disrupts the renal sympathetic nerves via ablation. Goal is to reduce sympathetic activity and reduce blood pressure. Considered for patients with true resistant hypertension after excluding a secondary cause, optimizing medical therapy, and confirming adherence.
Promoting Adherence
Build patient trust, increase motivation. Consider beliefs and attitudes. Both clinician and patient must agree on BP Goals
Strategies to promote adherence
Education, patient and family involvement, regular communication, discussion of progress, link drug administration to daily activities, minimize number of daily doses, use of combo of products, reminder strategies, medication affordability and access
BP Readings at home vs in clinic
Are usually 10/5 mmHg higher in clinic than ambulatory at home
Large cuff on small arm
Falsely low BP
Small Cuff on Big arm
falsely high blood pressure
Pharmacist Roles in CVD Risk Reduction
Collaborative practice agreements - can initiate and modify pharmaceutics
Systems approach - CVD risk reduction is challenging in a busy primary care practice, so technology is helpful
LVH
Left ventricular hypertrophy. Is the thickening of the left ventricular myocardium in response to chronic pressure overload or volume overload
Severe hypertension
>180/120. In emergencies admit to ICU and continue monitoring for organ damage. Reduce by oral or IV meds by no more than 25% in the first hour. Then no less than 160/100 in the next 2-6 hours. Then <130 over the next 24-48 hours