CPE Part 3: Restorative Dentistry Concepts, Outline form, Dental Materials, Liners & pulp caps, tooth anatomy
1/228
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
229 Terms
Abrasion
- wear of teeth due to mechanical process (tooth brushing)
- commonly occurs in cervical third of tooth (Class V)
- Notch/ V shaped notches
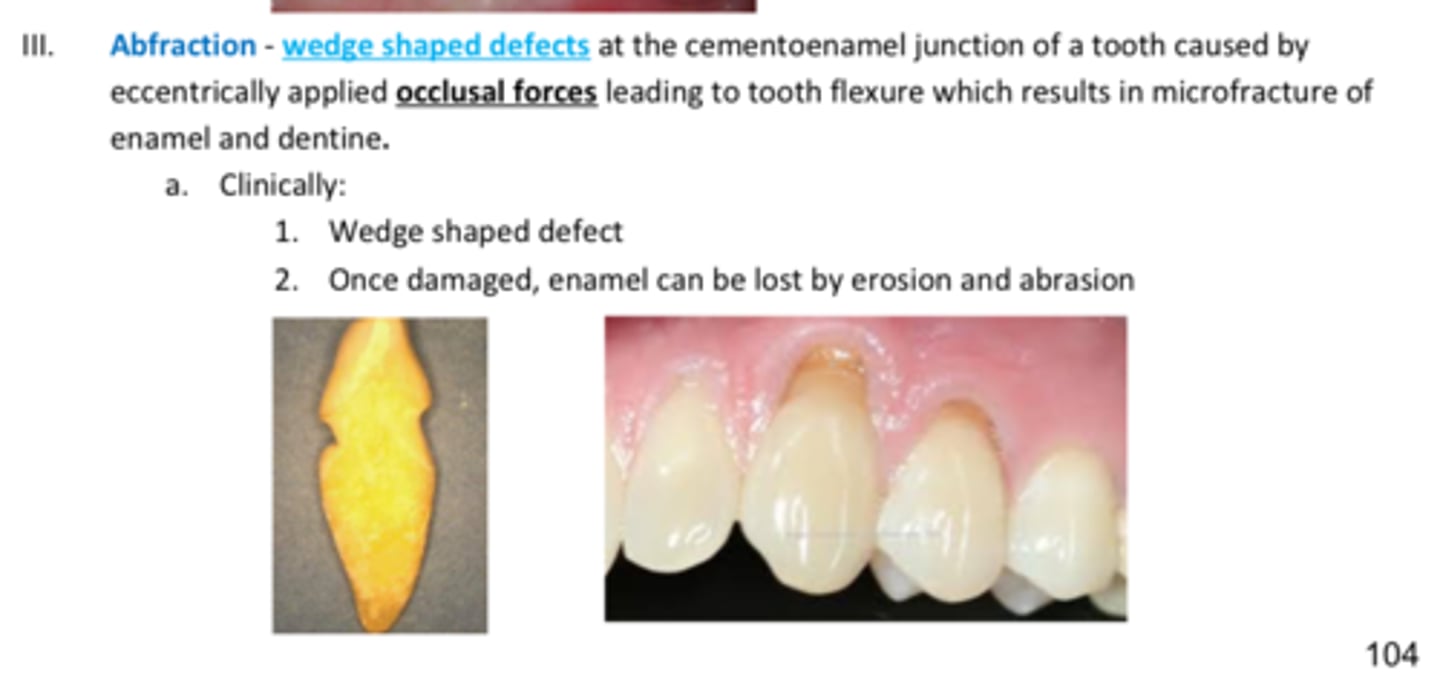
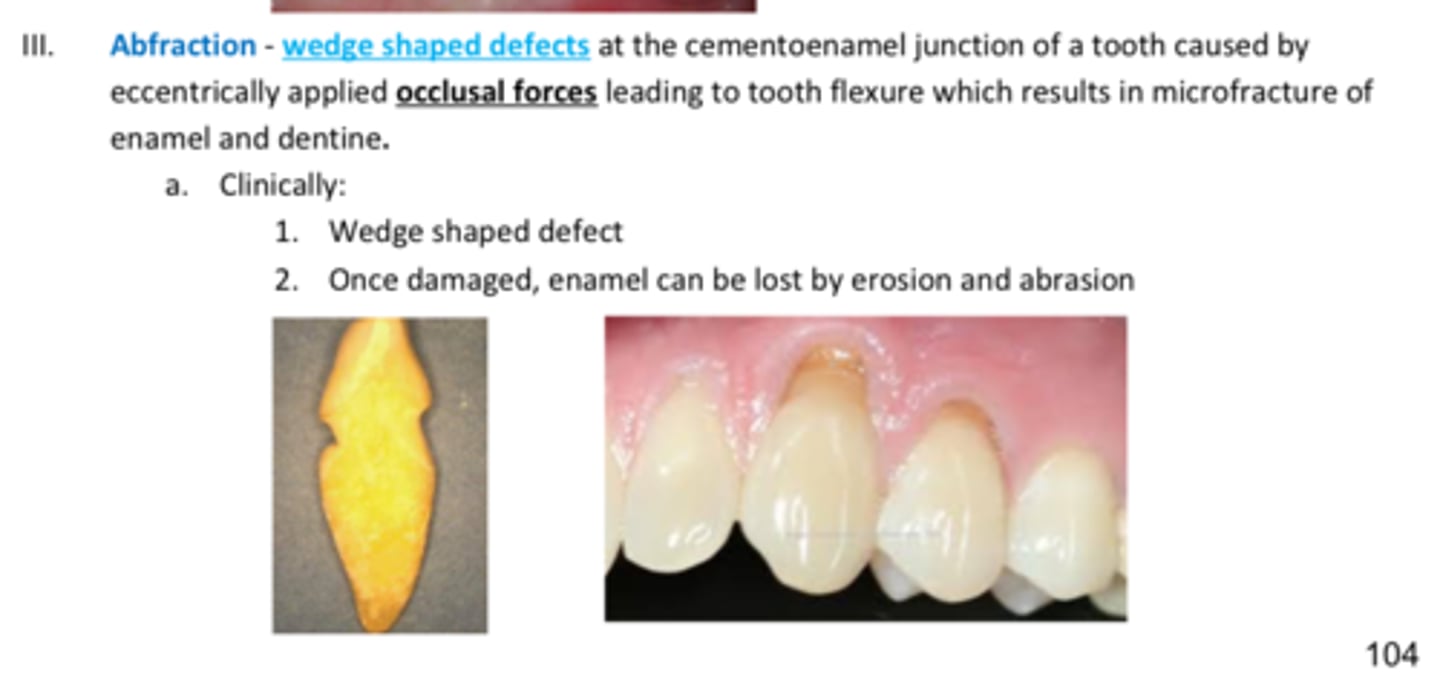
Abfraction
- wear of teeth @ CEJ causes by excessive occlusal forces
- Wedge shaped defects
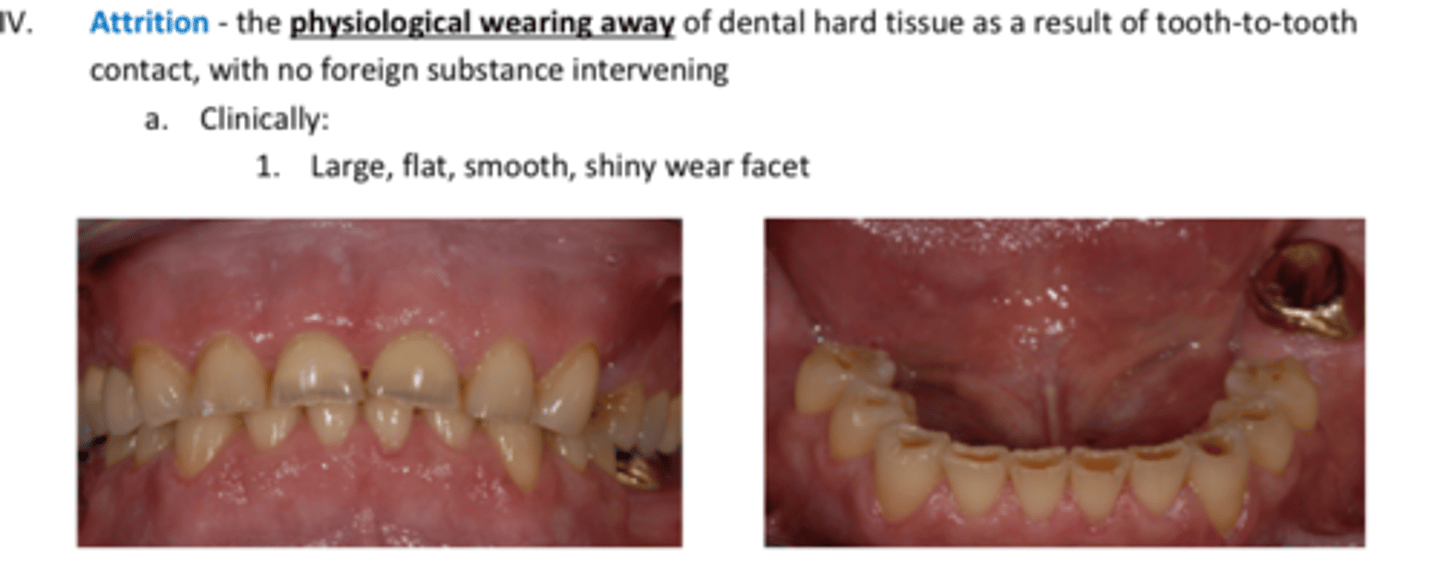
Attrrition
- wear of teeth due to tooth-tooth contact
- flat teeth
Abrasion=
Abfraction=
Attrition=
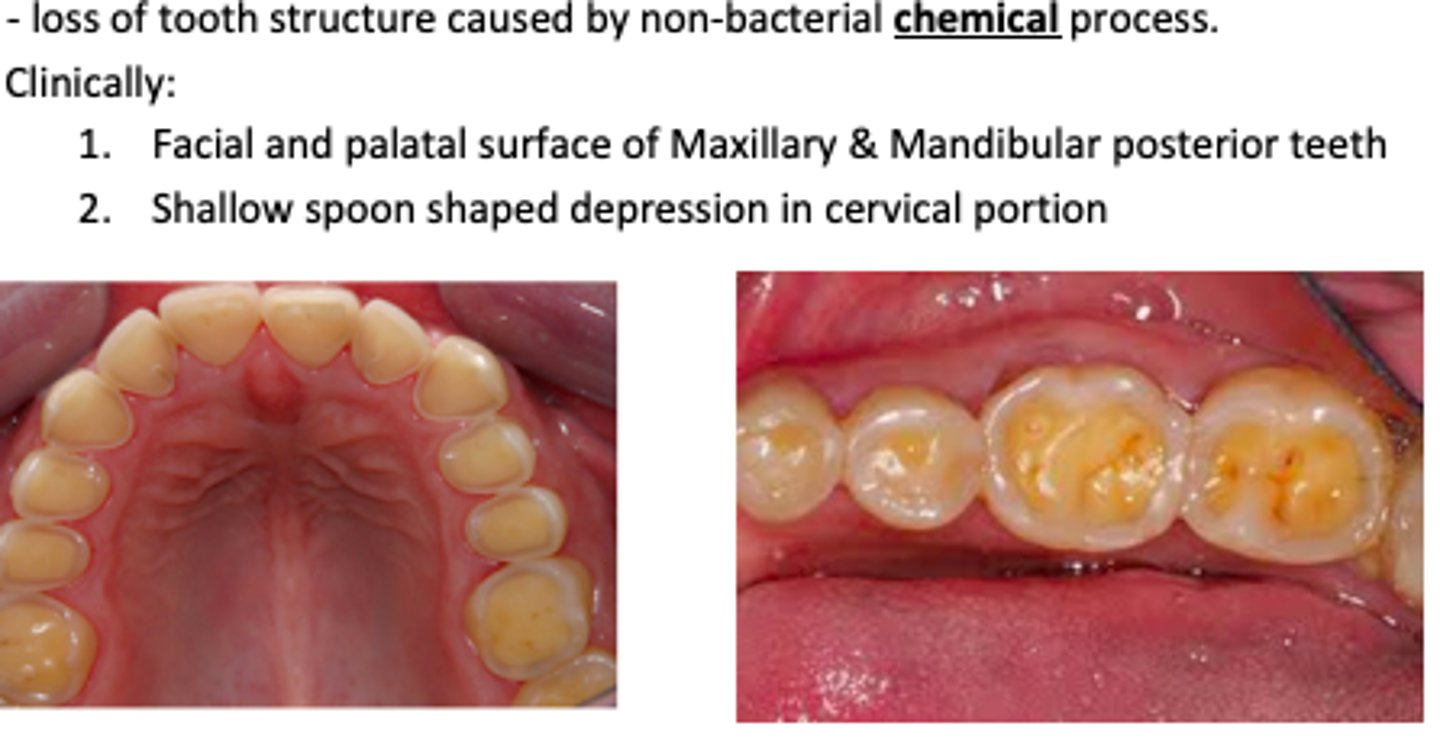
Erosion
Loss of tooth structure caused by non-bacterial chemical process (acid)
Clinically:
Facial and palatal surface of Maxillary & Mandibular posterior teeth
Shallow spoon shaped depression in cervical portio
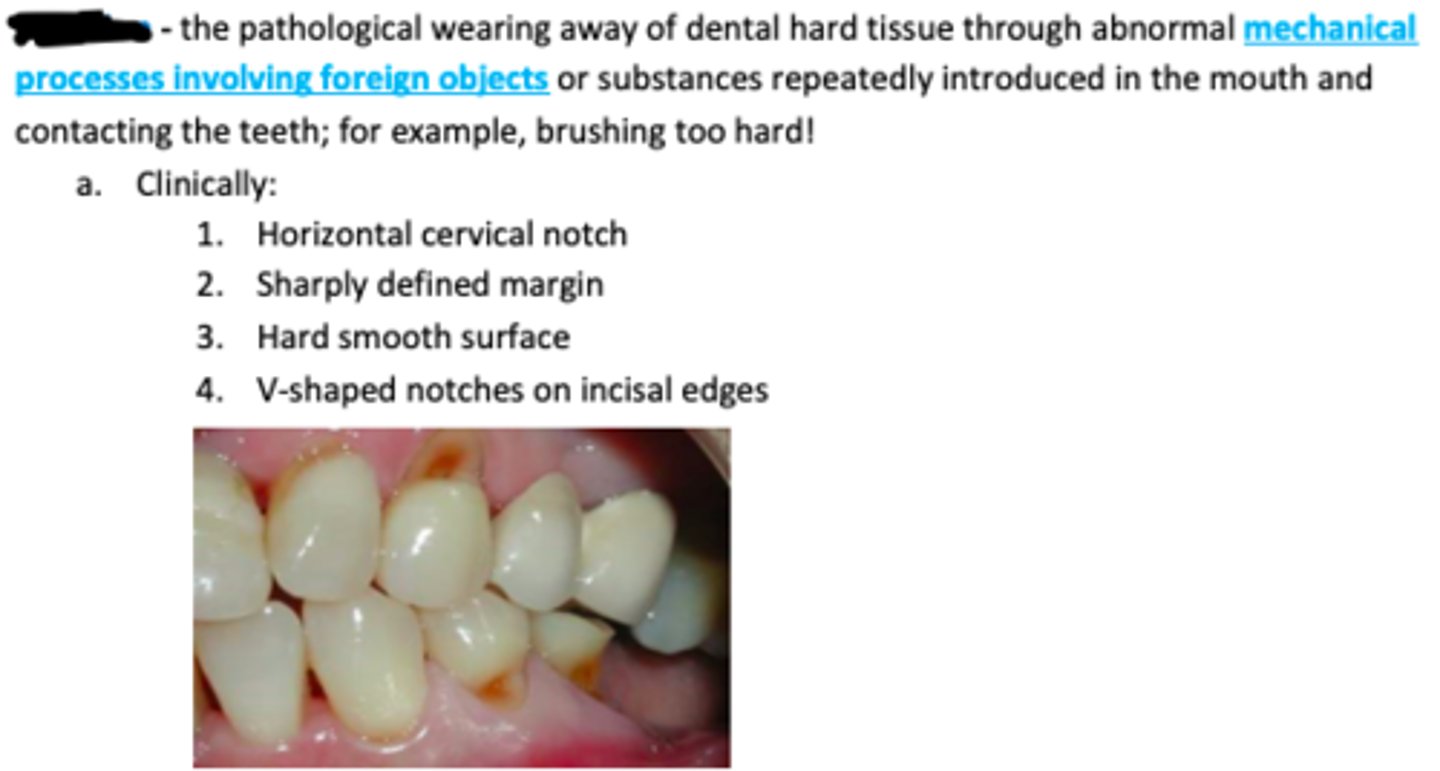
Abrasion
The pathological wearing away of dental hard tissue through abnormal mechanical processes involving foreign objects or substances repeatedly introduced in the mouth and contacting the teeth; for example, brushing too hard!
Clinically:
Horizontal cervical notch
Sharply defined margin
Hard smooth surface
V-shaped notches on incisal edges
Abfraction
Wedge shaped defects at the cementoenamel junction of a tooth caused by eccentrically applied occlusal forces leading to tooth flexure which results in microfracture of enamel and dentine.
Clinically:
Wedge shaped defect
Once damaged, enamel can be lost by erosion and abrasion
Attrition
The physiological wearing away of dental hard tissue as a result of tooth-to-tooth contact, with no foreign substance intervening
Clinically:
Large, flat, smooth, shiny wear facet
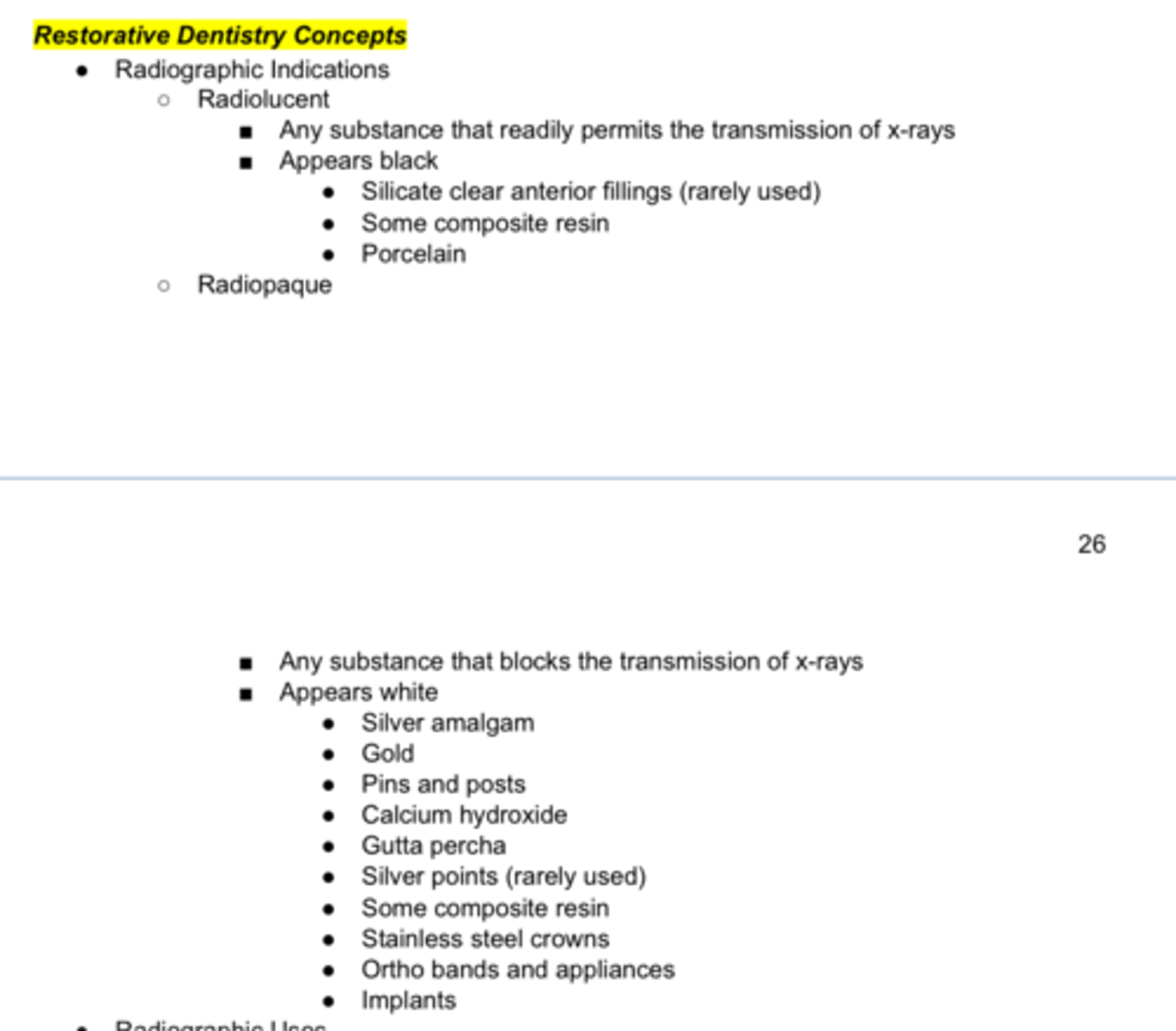
Permits the transmission of X-rays
Appears black:
- composite resin
- procelain
Any substance that blocks the transmission of x-rays
Appears white:
- silver amalgam
- gold
- CaOH
- pins & posts
- Gutta percha
- SSC
- implants
Radiolucent=
Radiopaque=
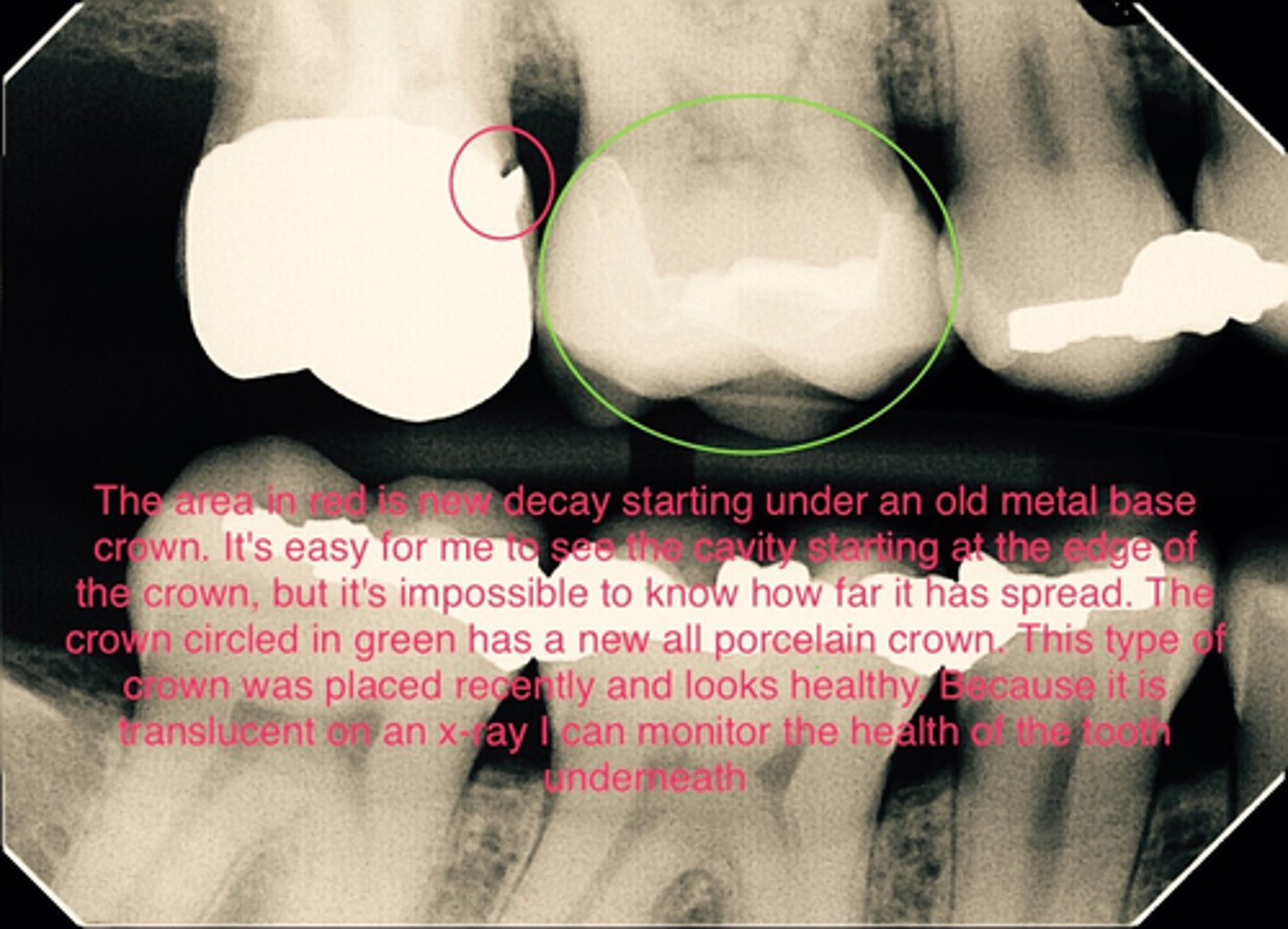
Radiolucent
Porcelain shows up (radiolucent/radiopaque) on a radiograph
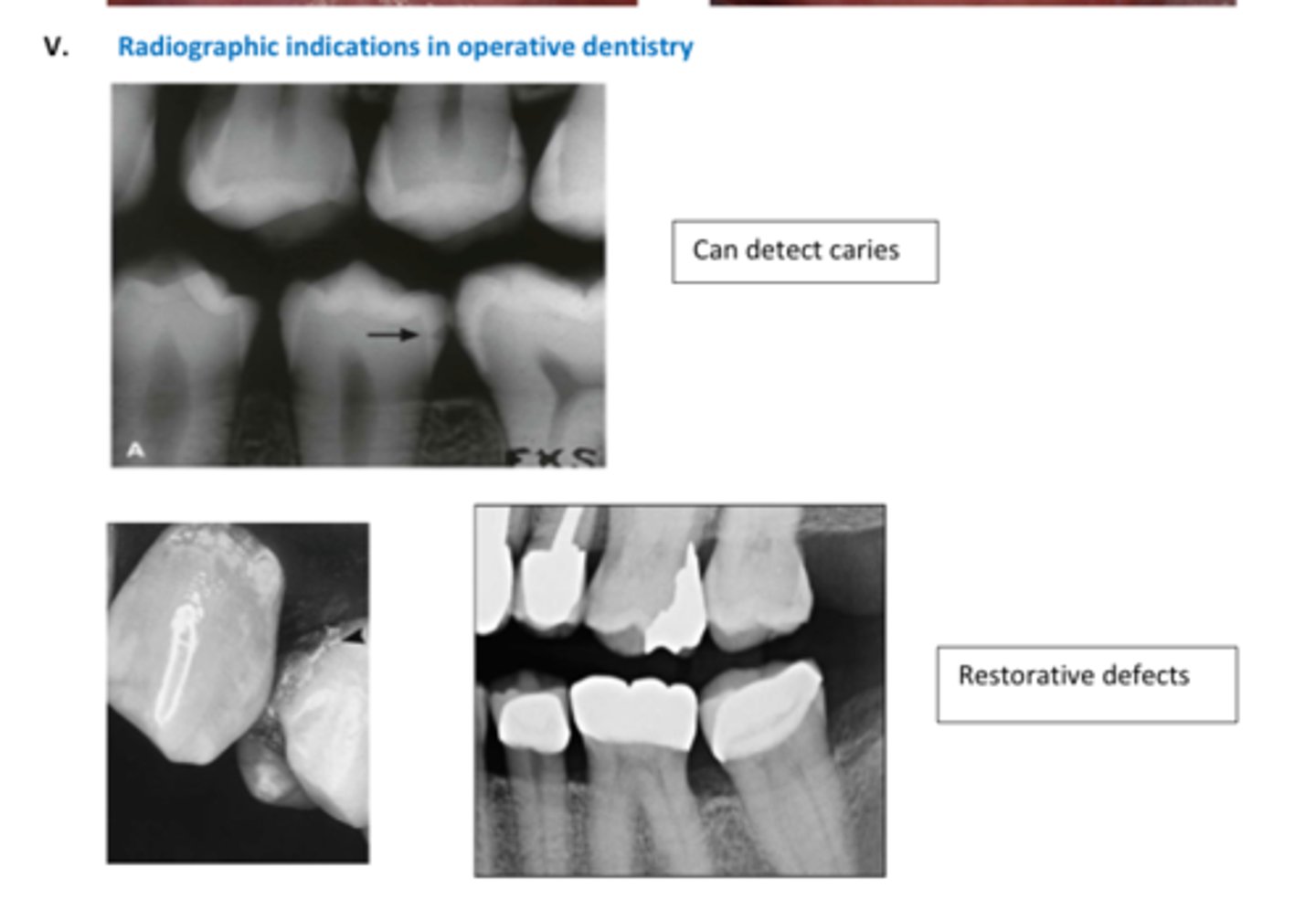
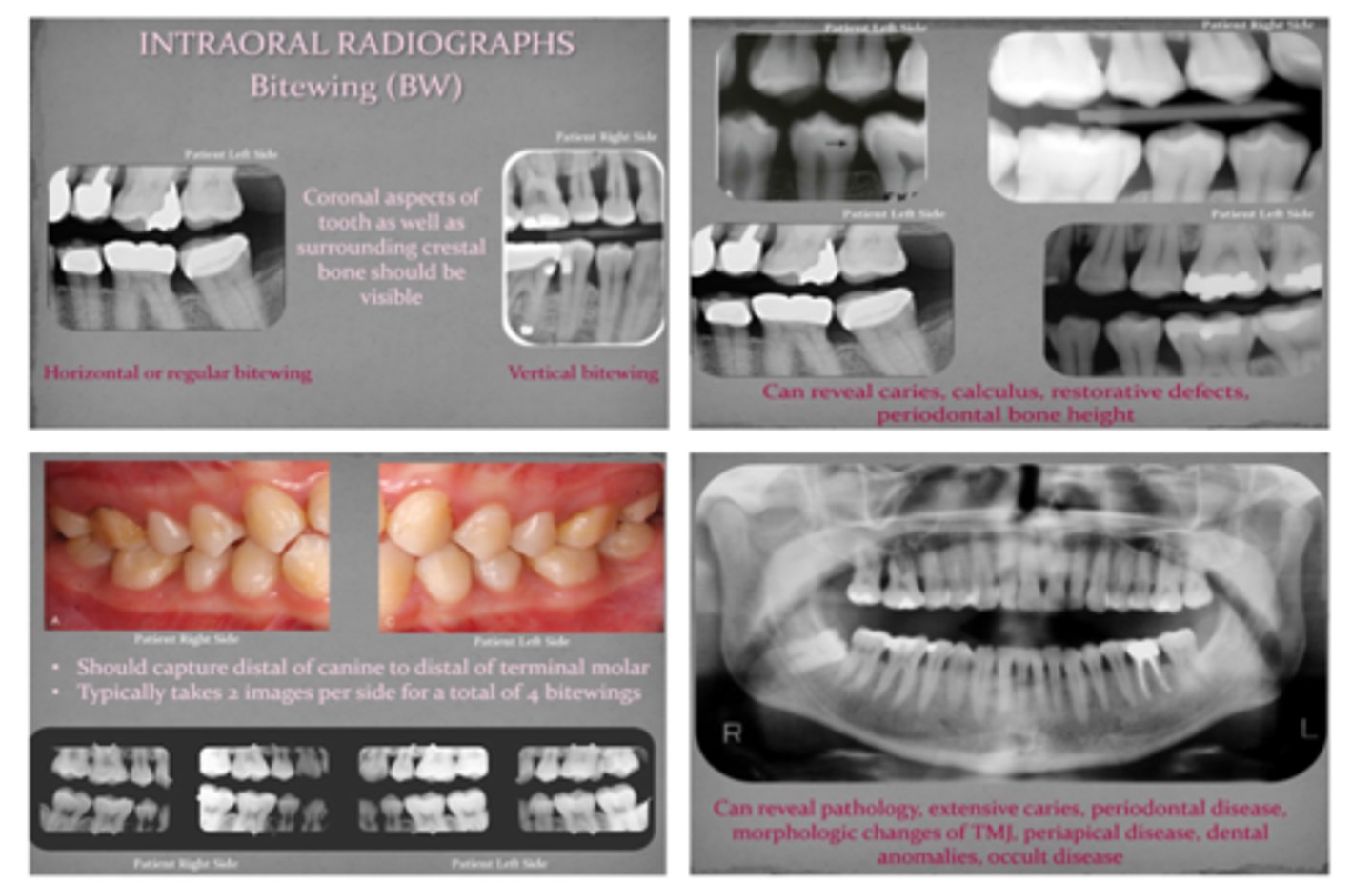
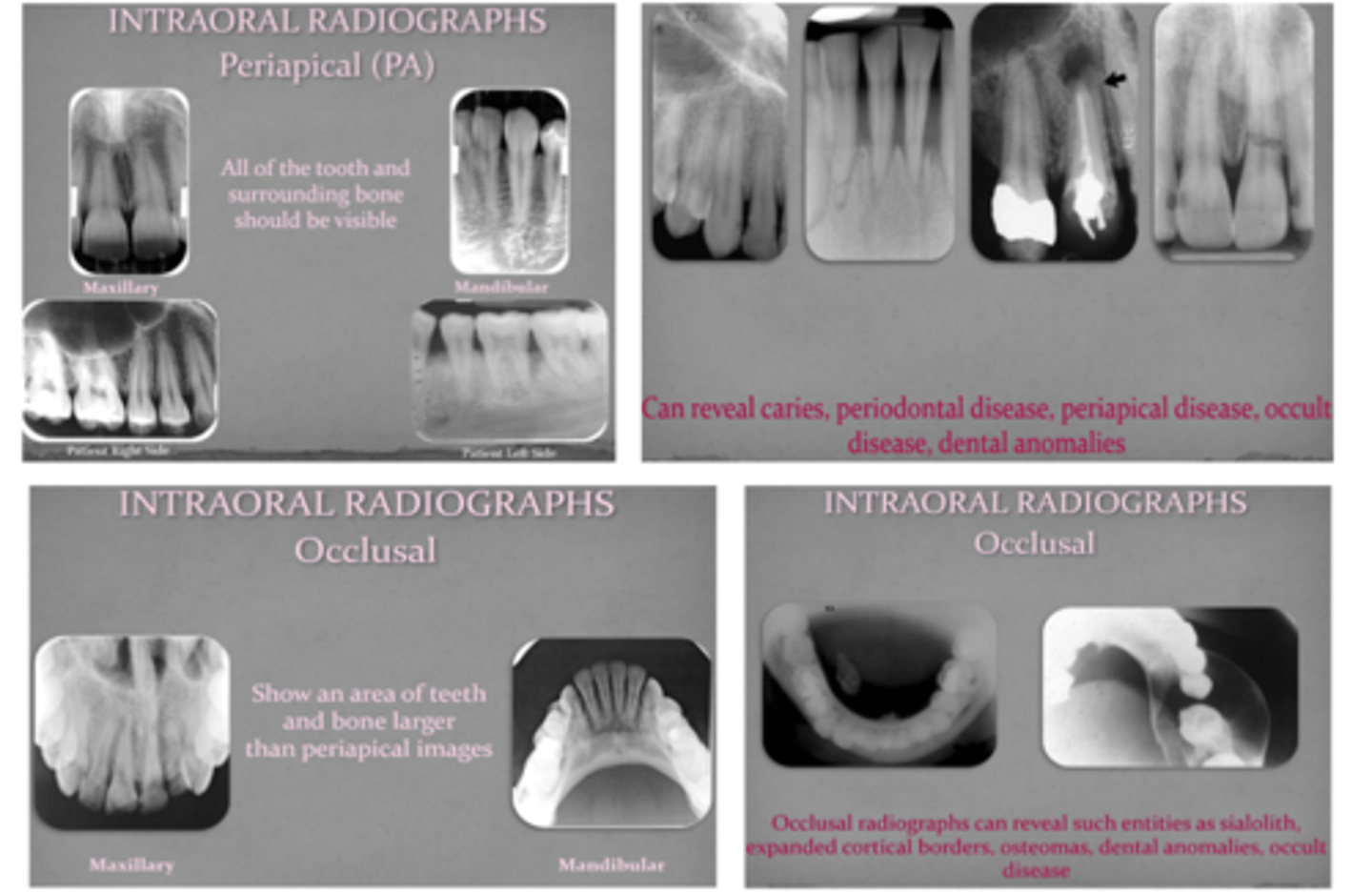
4 Types of Radiographs:
BW
PA
Panoramic
Occlusal
- already covered in Part 1 quizlet
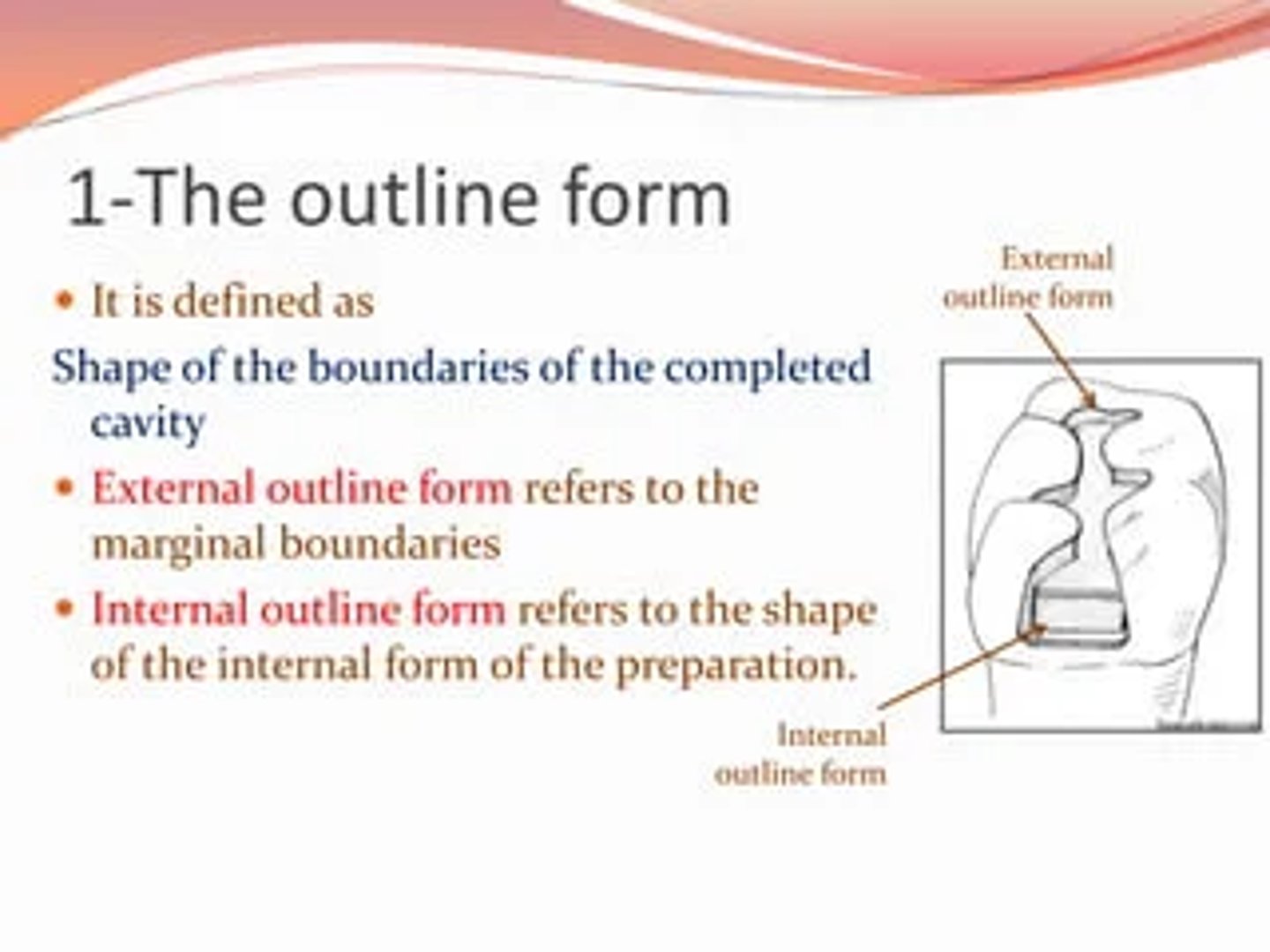
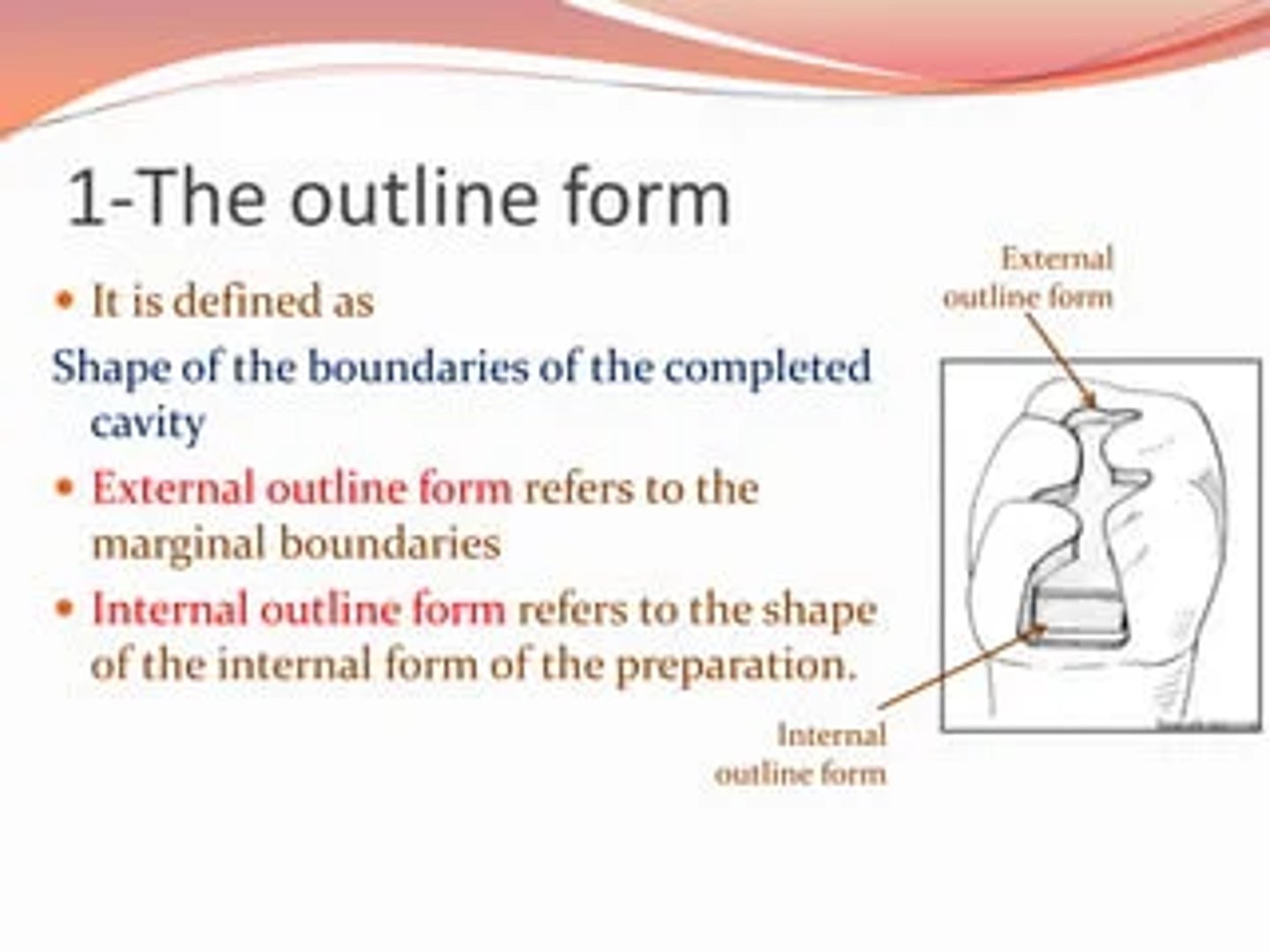
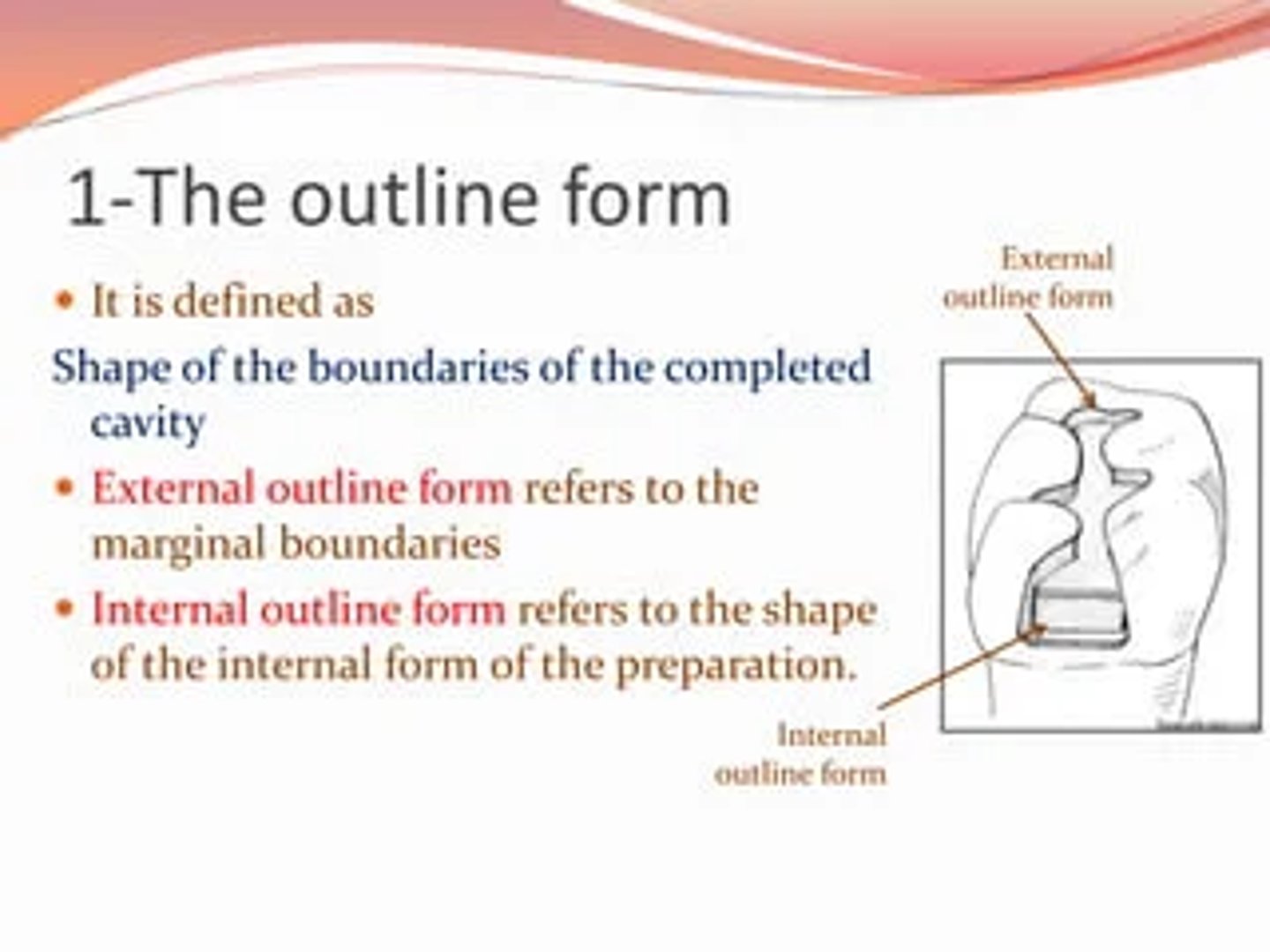
Internal outline form
– includes the inner dimensions, depth, and details of the preparation
- Location and direction of internal (i.e., axial, pulpal) and external (i.e., buccal, lingual, proximal) walls
External outline form
- the form of the area of the tooth surface to be included within the finished preparation
- Defines the external boundary or perimeter of the preparation
- Location and placement of cavosurface margins
Internal outline form=
External outline form=
Internal outline form
– includes the inner dimensions, depth, and details of the preparation
- Location and direction of internal (i.e., axial, pulpal) and external (i.e., buccal, lingual, proximal) walls
External outline form
- the form of the area of the tooth surface to be included within the finished preparation
- Defines the external boundary or perimeter of the preparation
- Location and placement of cavosurface margins
Outline form
These are all factors affecting (Internal/External) Outline Form
● Location and size of carious lesion, defect or fracture
● Restorative material planned
● Proximity of the lesion to other defects and restorations
● Relationship of adjacent teeth
● Occlusal relationships!!
● Esthetic considerations
Resistance form
Features of the preparation that enable the restoration and the remaining tooth structure to withstand the stresses of mastication and lateral (shear) forces
Features of the preparation that resist fracture of the restoration itself or fracture of remaining tooth structure
- features of the prep that allow the tooth/restoration to resist occlusal forces
Resistance Form
Principles of ______ ________ of a Cavity Preparation:
(1) Flat pulpal and gingival walls perpendicular to occlusal forces
(2) Keep prep as small as possible to maintain strong cusps and ridges
(3) Rounded internal line angles to reduce stress concentration in tooth structure
(4) Extend prep to remove weak tooth structure, such as unsupported enamel, to prevent or resist fracture
(5) Provide adequate thickness of restorative material
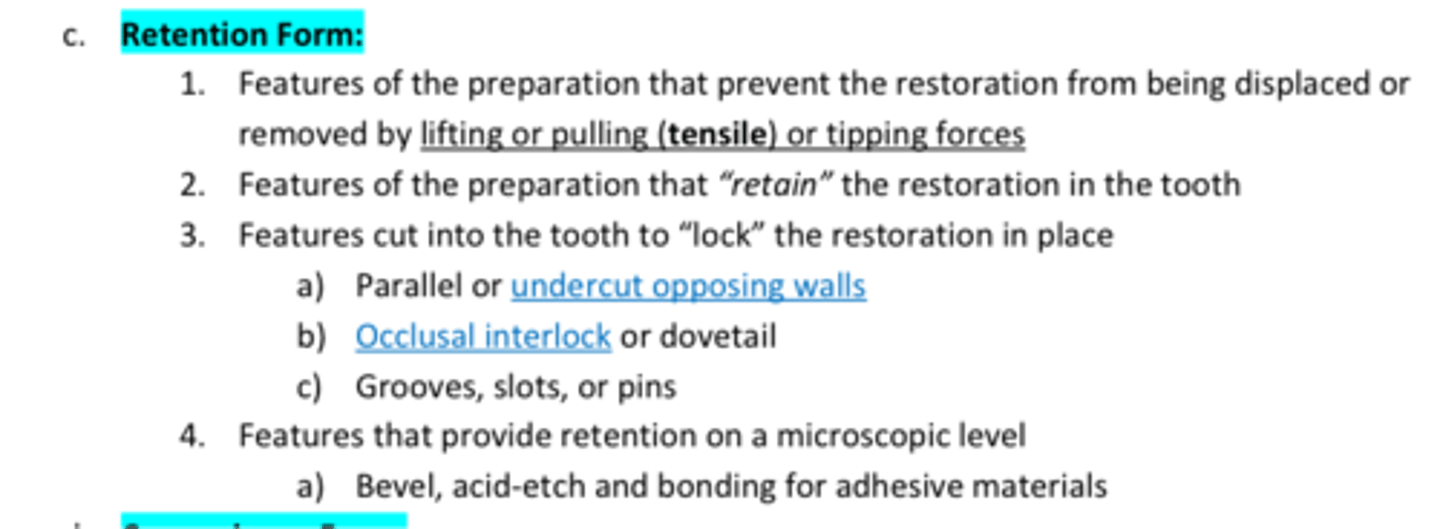
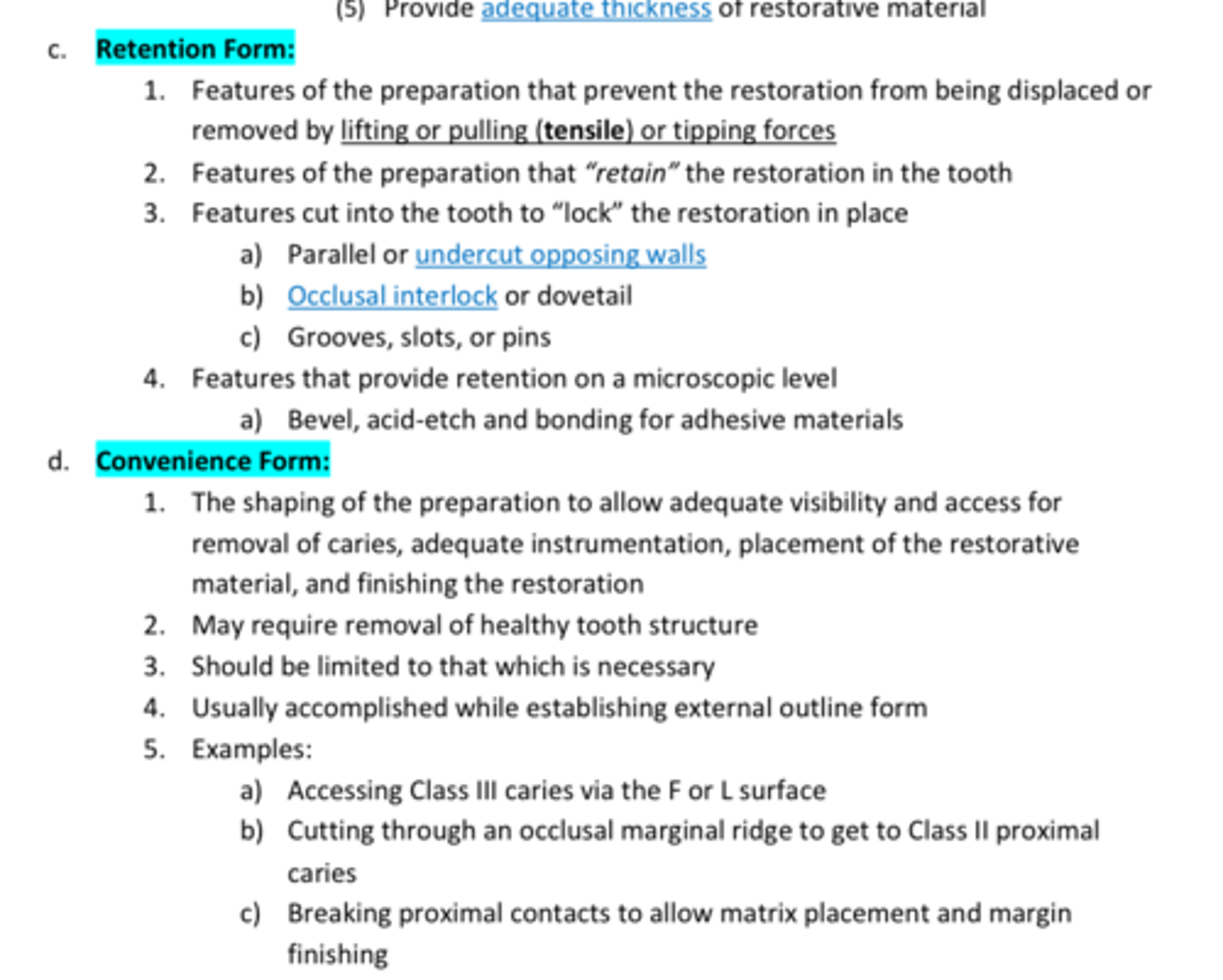
Retention Form
Features of the preparation that prevent the restoration from being displaced or removed by lifting or pulling (tensile) or tipping forces
Features of the preparation that “retain” the restoration in the tooth
review 4
Convenience form
The shaping of the preparation to allow adequate visibility and access for removal of caries, adequate instrumentation, placement of the restorative material, and finishing the restoration
2. May require removal of healthy tooth structure
3. Should be limited to that which is necessary
4. Usually accomplished while establishing external outline form
5. Review examples in photo!
Proper Understanding of isolation
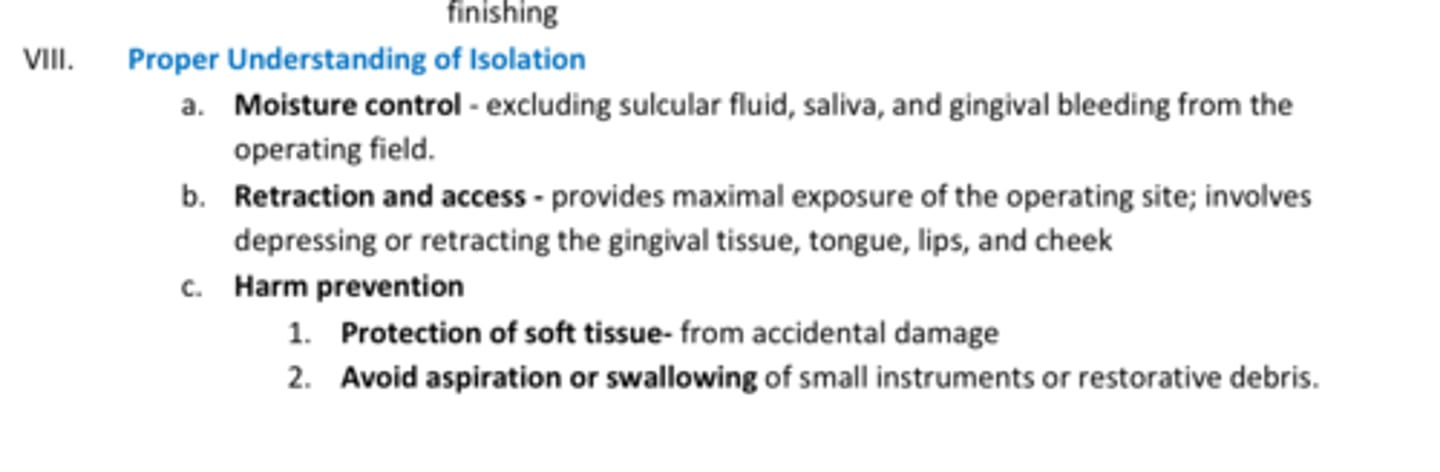
Review Isolation techniques
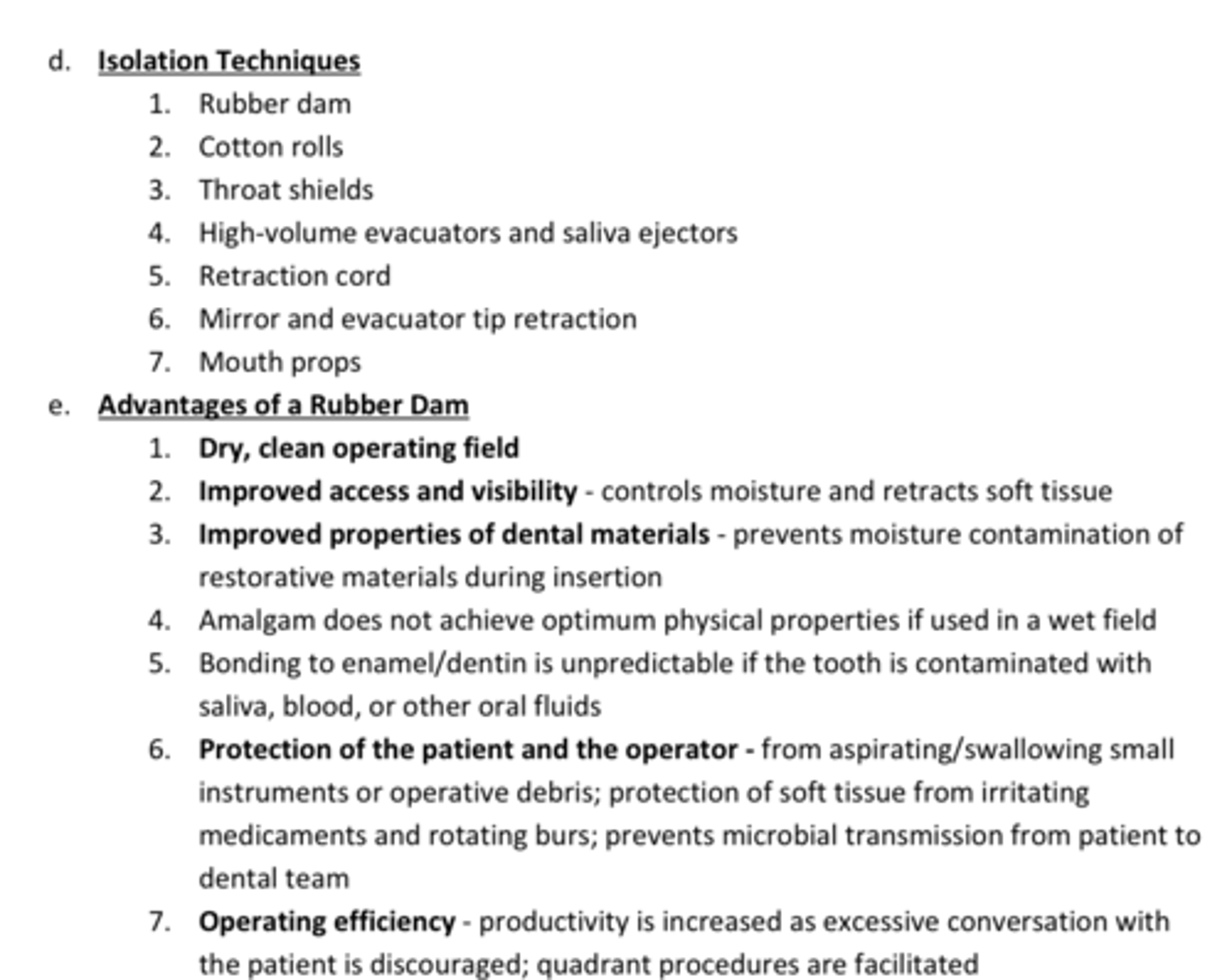
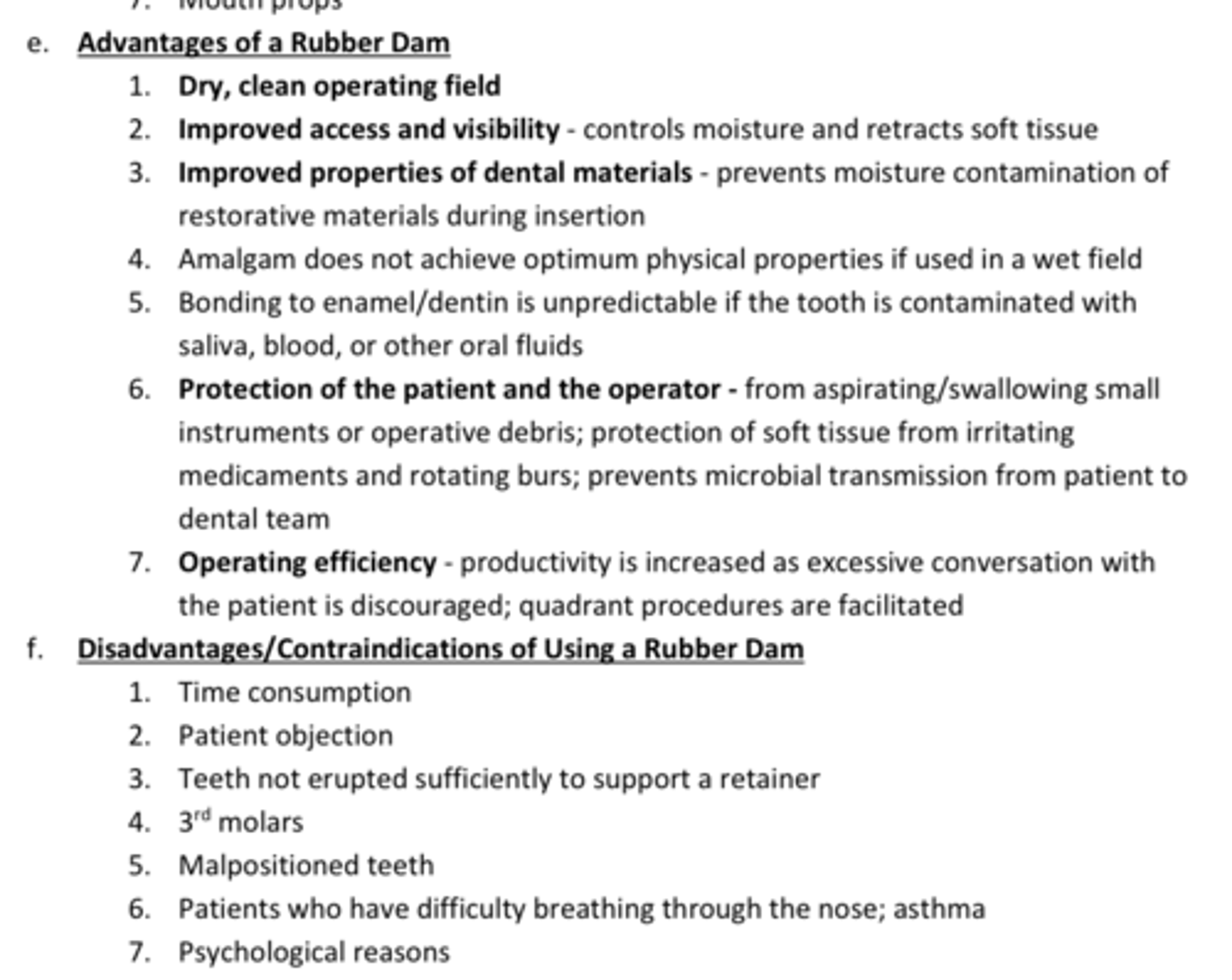
Dry, clean operation field
Improved access & visibility
Protection for pt & dentist
List 3 advantages of using a Rubber Dam for Isolation
- review photo for rest
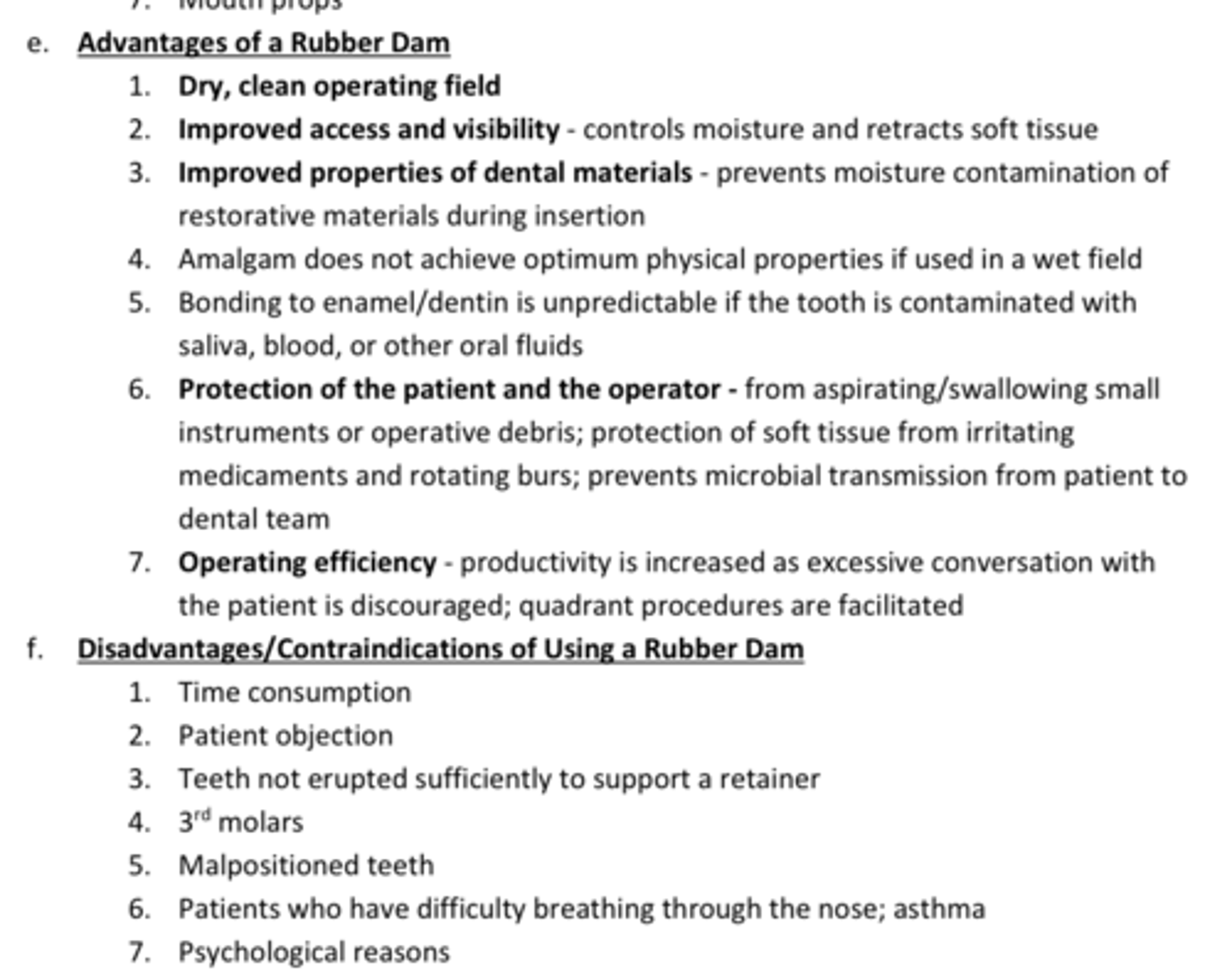
Pt objection
3rd molars
Pts who have difficulty breathing through nose; Asthma
List 3 disadvantages of using a Rubber Dam for Isolation
- review photo for rest
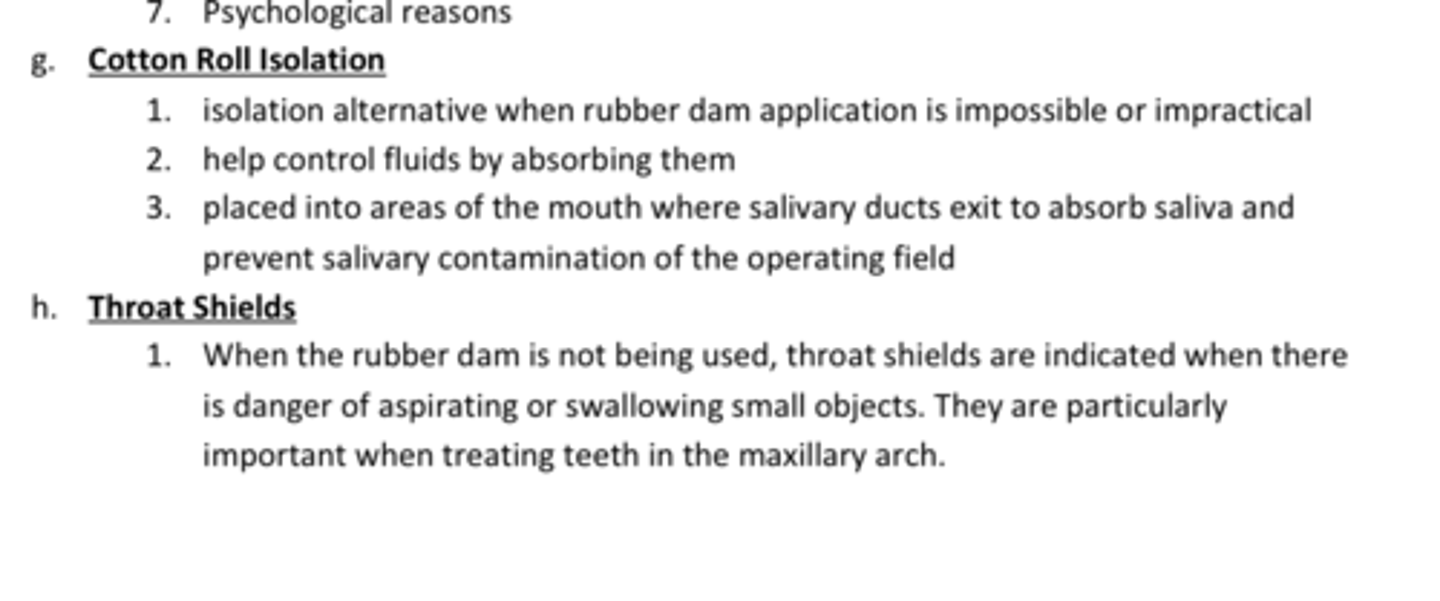
Cotton roll
_____ ____ isolation can be used as an Isolation alternative when rubber dam application is impossible or impractical
- Help control fluids by absorbing them
- Placed into areas of the mouth where salivary ducts exit to absorb saliva and prevent salivary contamination of the operating field
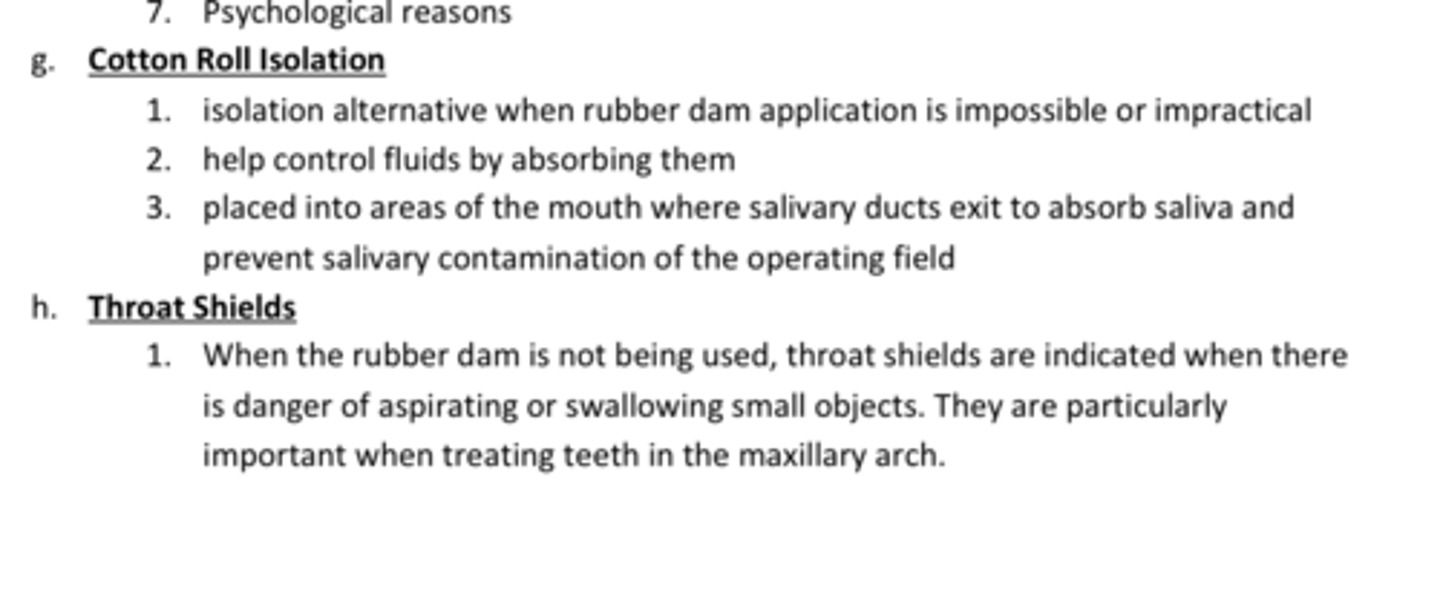
Throat shield
What type of isolation:
Used when the rubber dam is not being used, are indicated when there is a danger of aspirating or swallowing small objects (esp when treating MX teeth)
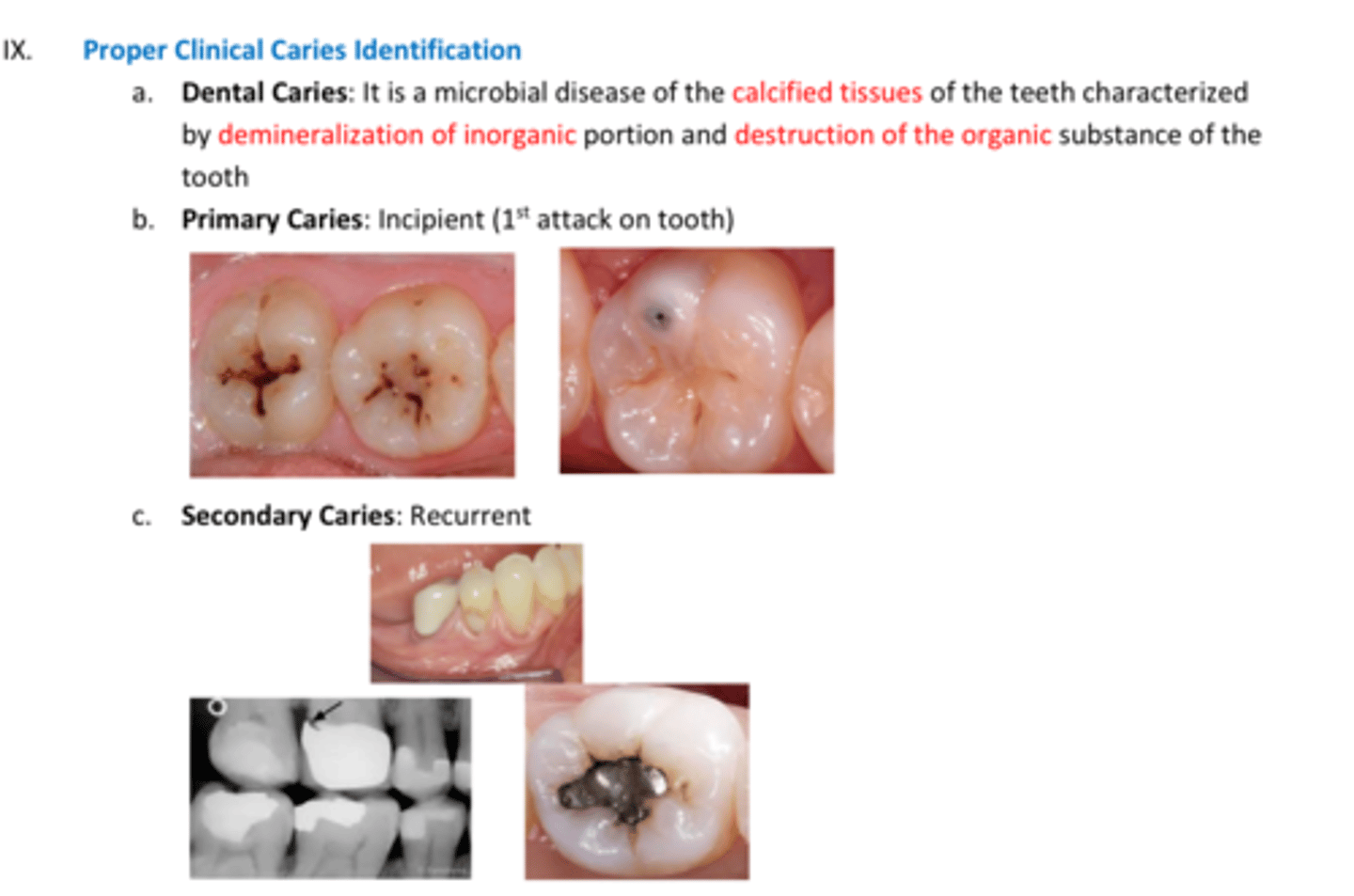
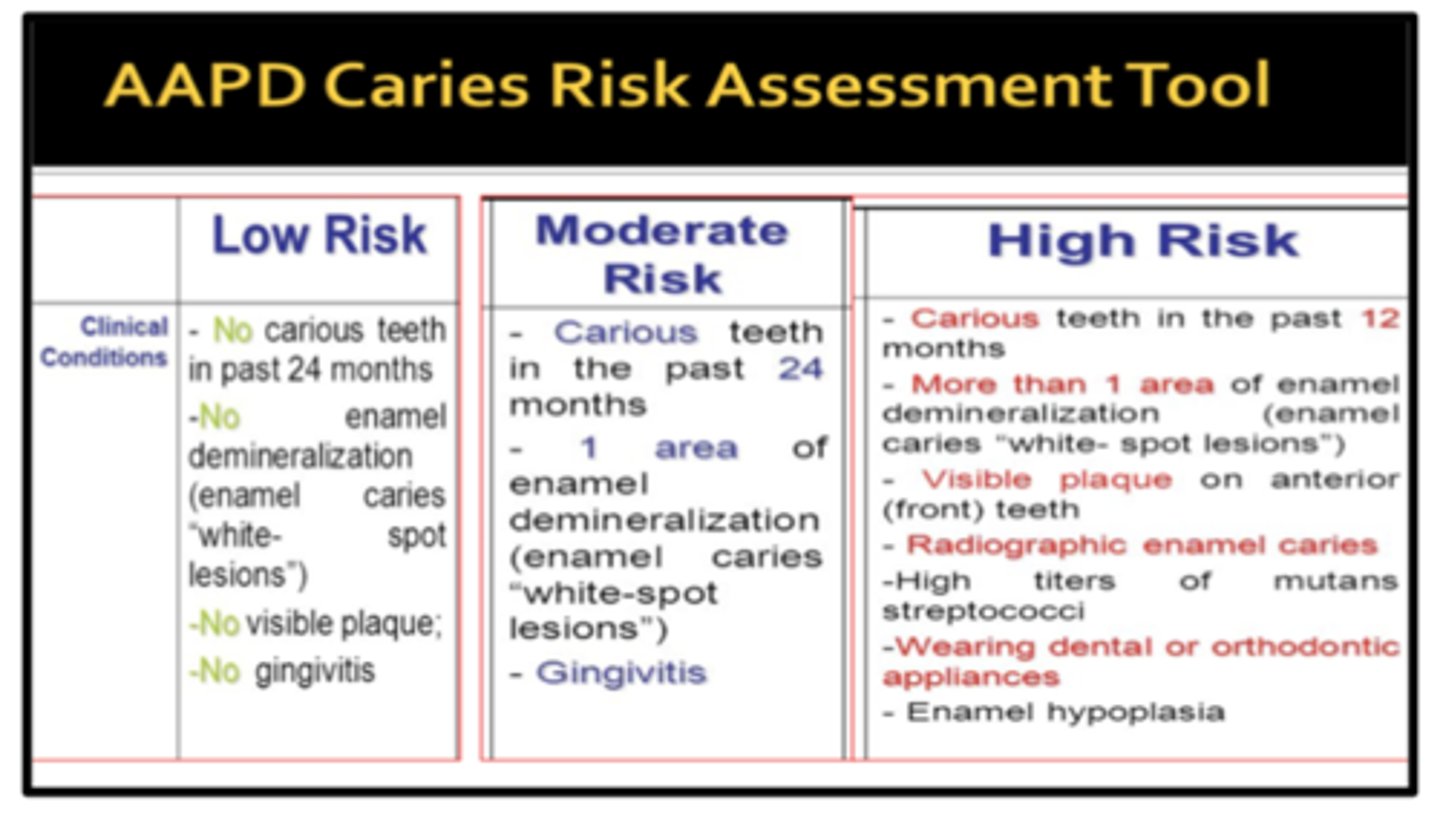
Dental caries
Microbial disease of the calcified tissues of the teeth characterized by demineralization of inorganic portion and destruction of the organic substance of the tooth
5.5
- if a pts saliva pH gets below 5.5= HIGH risk for caries
- pH below 5.5= BAD
Critical pH of caries!!!
Incipient caries (haven't reached dentin yet)
Recurrent caries
Primary caries=
Secondary caries=
review Nature
■ Critical pH: 5.5
■ Primary Caries (incipient)
■ Secondary caries (recurrent)
■ Xylitol inhibits formation of plaque
True
T/F: Xylitol inhibits formation of plaque
White spot lesions
First sign of caries
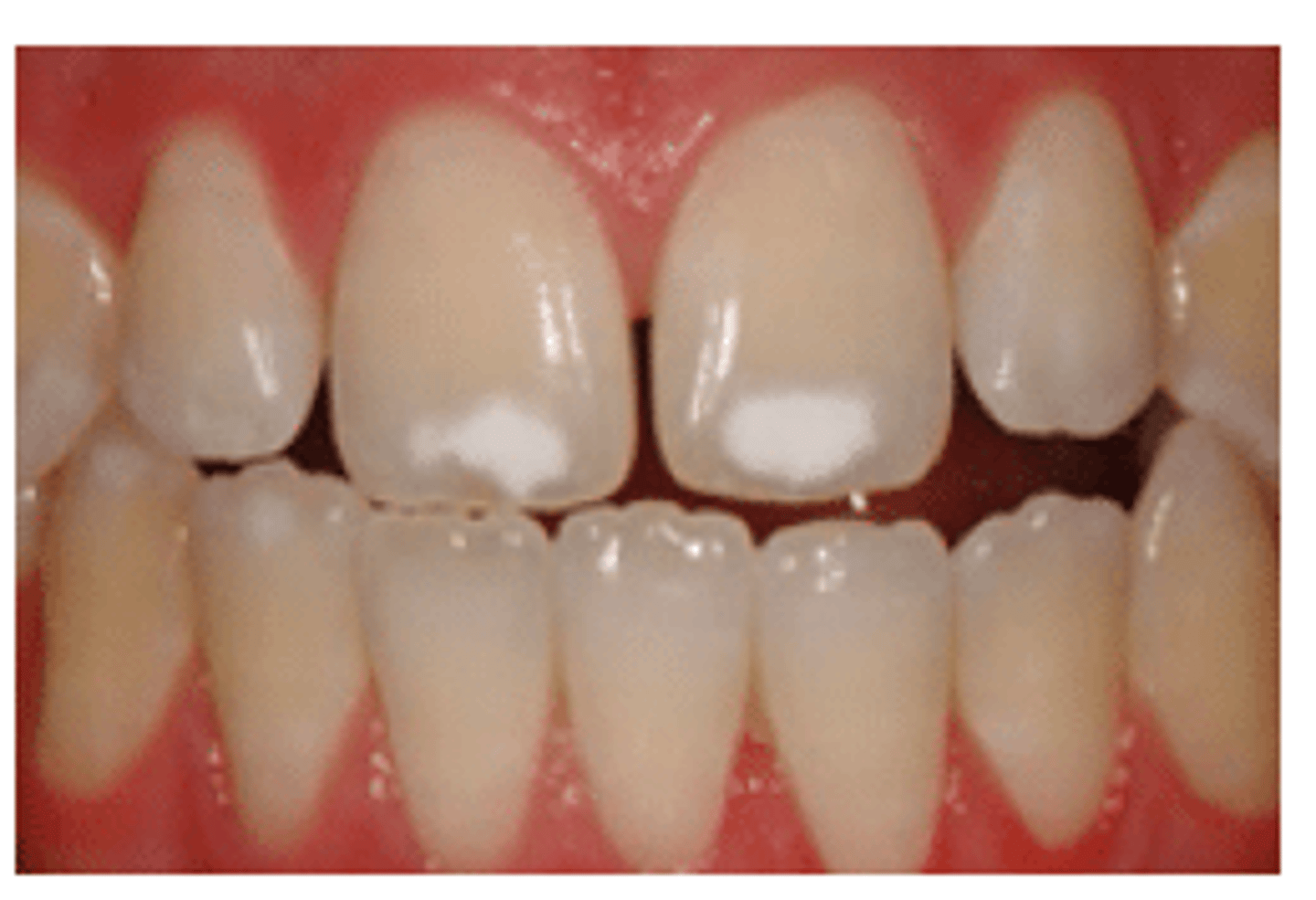
early sign
White Spot Lesions are an ____ ____ of Caries
-Surface layer with mineral content lower than sound enamel
- Higher mineral content than underlying body of lesion
Tactile sensation
- Texture/hardness of the dentin/cavity
Is the MOST IMPORTANT indicator in caries detection
Julias- just review
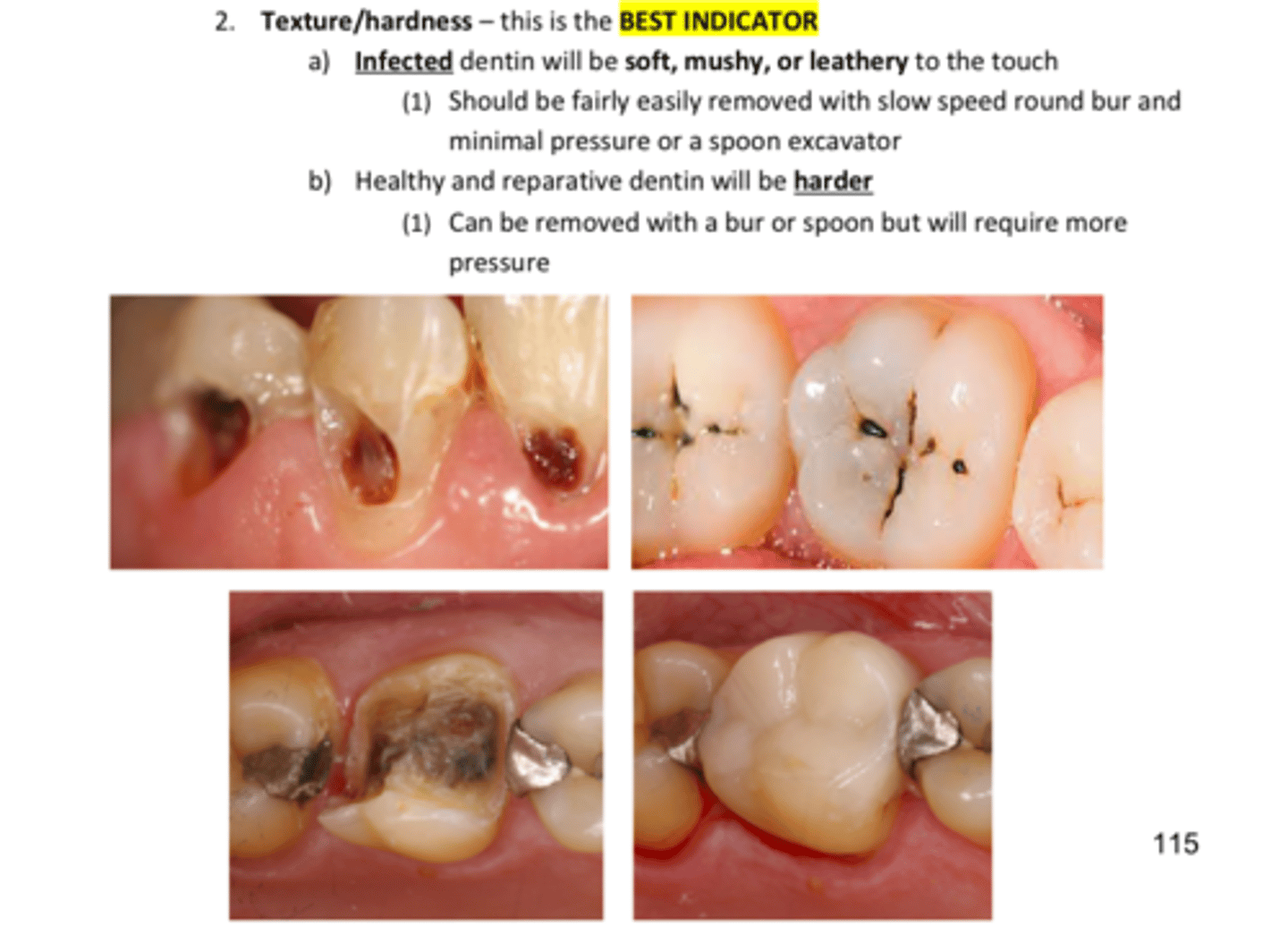
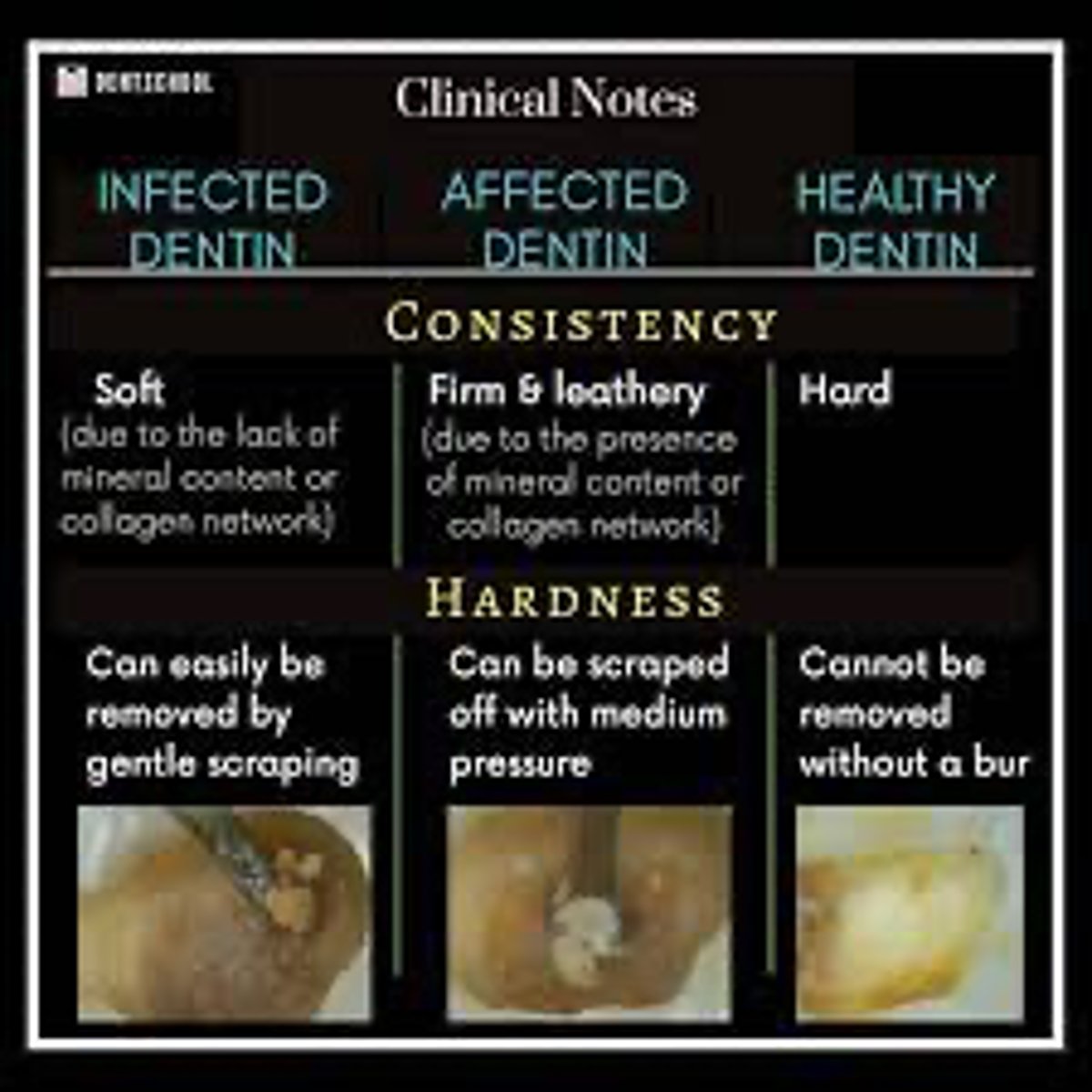
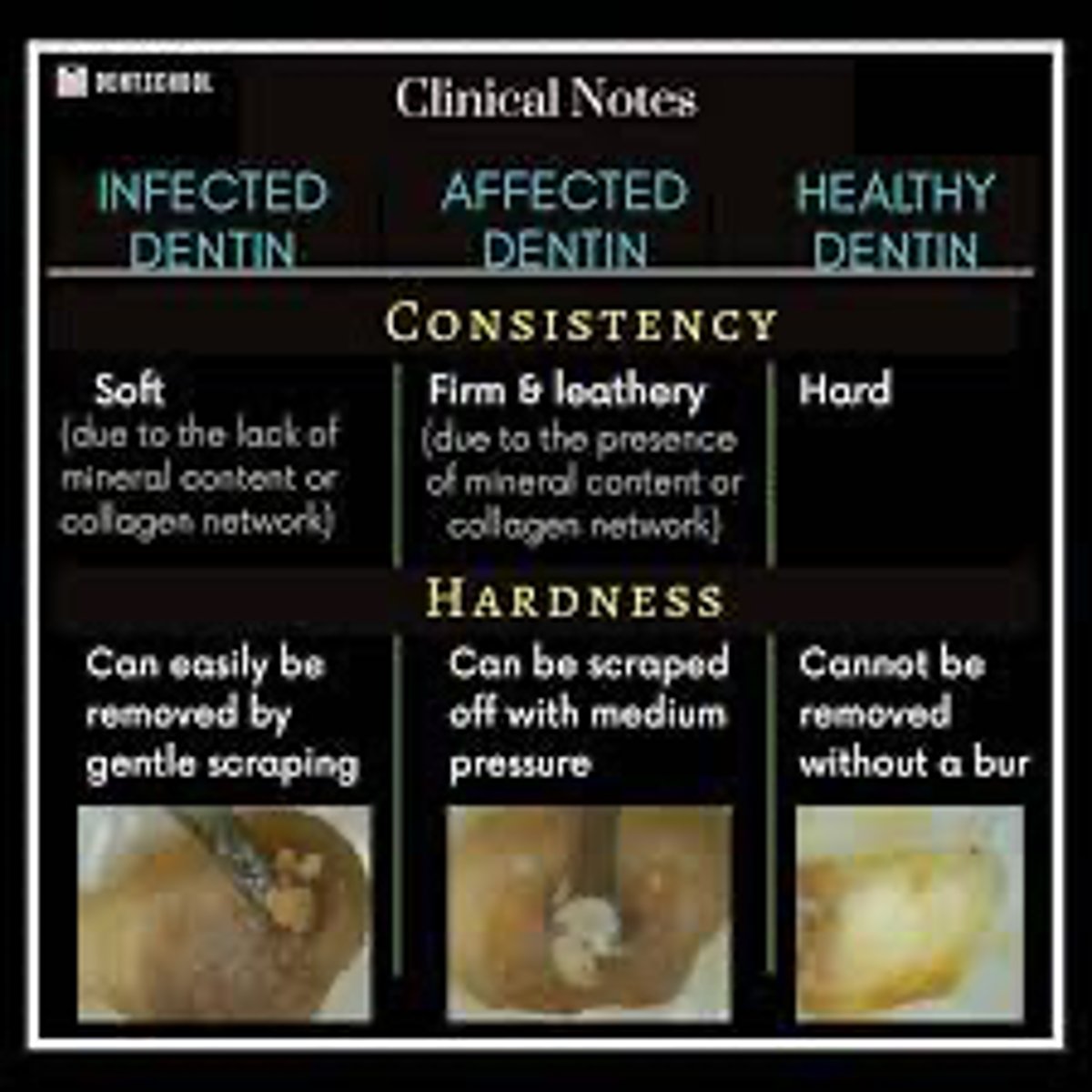
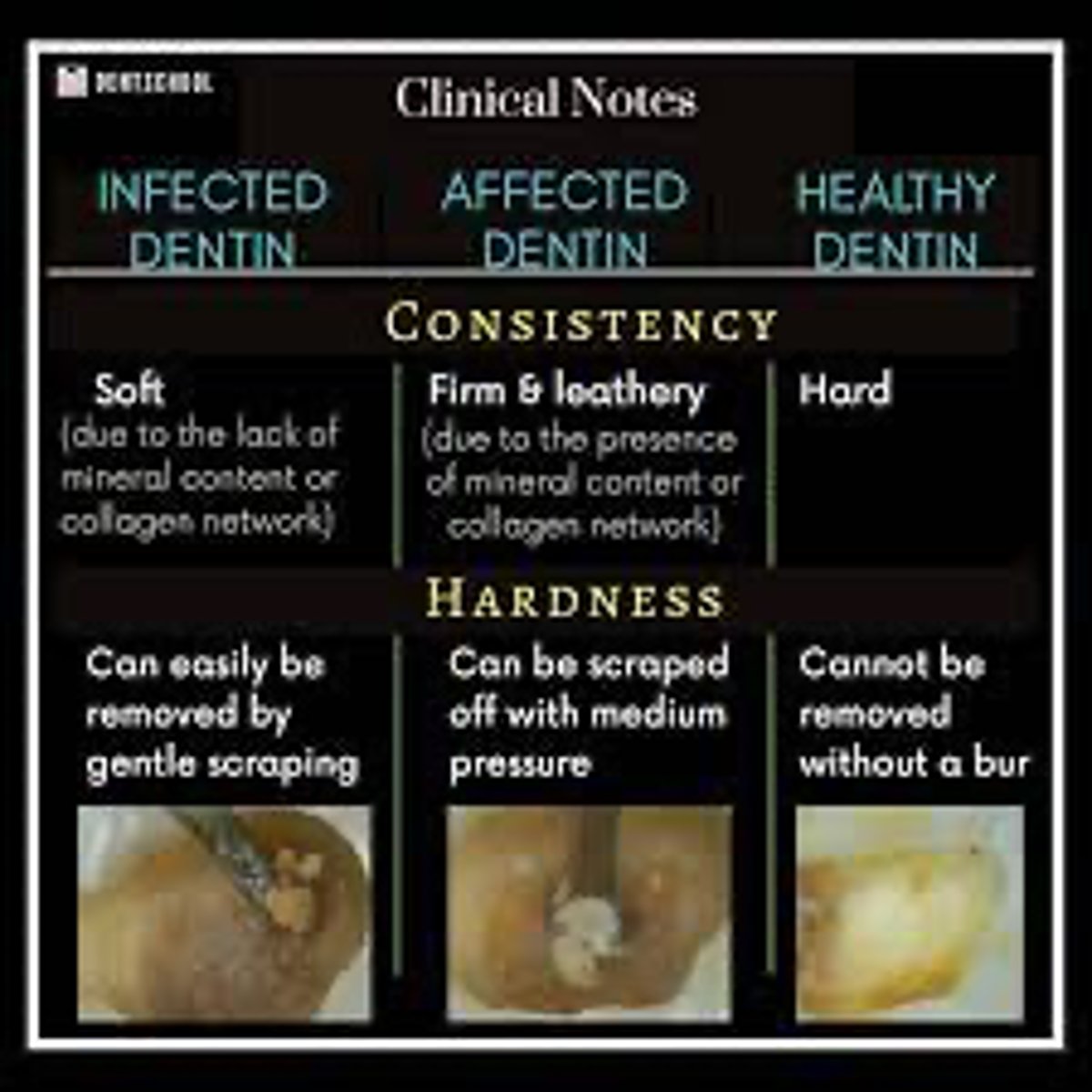
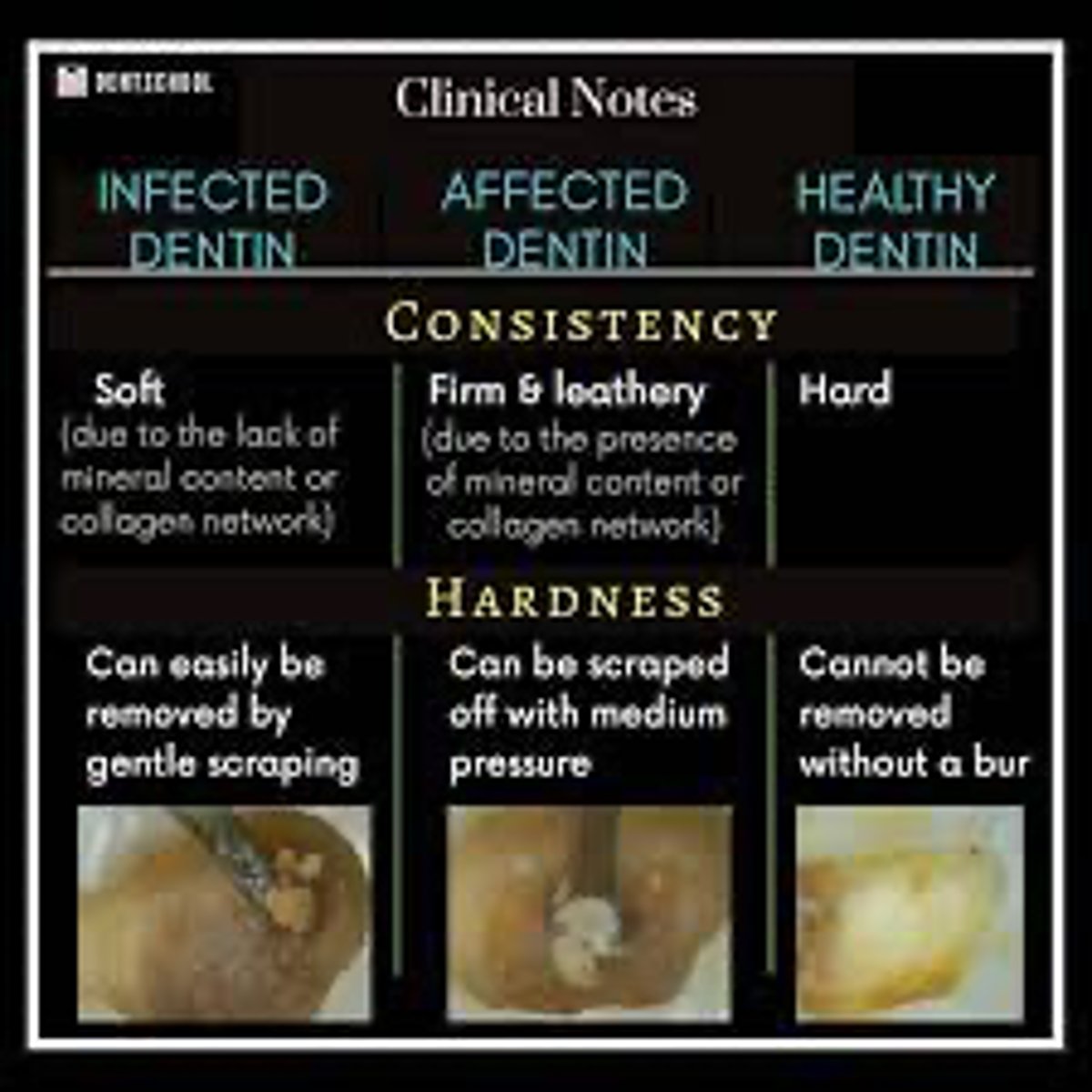
Infected Dentin
- Bacteria present
- Surface level
- NOT remineralizable, must be removed
- Soft and able to scoop
- Wet/mushy
Affected Dentin
■ NO bacteria
● Deeper into the cavity preparation (middle)
■ Re-mineralizable, should be preserved
■ Moist to dry
■ Leathery and firm (two types)
● Leathery does not deform as easily with a hand instrument but can still be pliable, whereas firm resists the pressure of pushing with a hand instrument
Sound Dentin
■ Completely dry
■ HARD
■ Deepest level
■ Need sound dentin left on the periphery of cavity prep
Zones of Dentinal Caries:
Infected Dentin=
Affected Dentin=
Sound Dentin=
Infected Dentin
What type of Dentin:
- Bacteria present
- Surface level
- NOT remineralizable, must be removed
- Soft and able to scoop
- Wet/mushy
Affected Dentin
What type of Dentin:
- NO bacteria
- Deeper into the cavity preparation (middle)
- Re-mineralizable, should be preserved
- Moist to dry
- Leathery and firm (two types)
- Leathery does not deform as easily with a hand instrument but can still be pliable, whereas firm resists the pressure of pushing with a hand instrument
Sound dentin
What type of Dentin:
- Completely dry
- HARD
- Deepest level
- Need sound dentin left on the periphery of cavity prep
Just for review
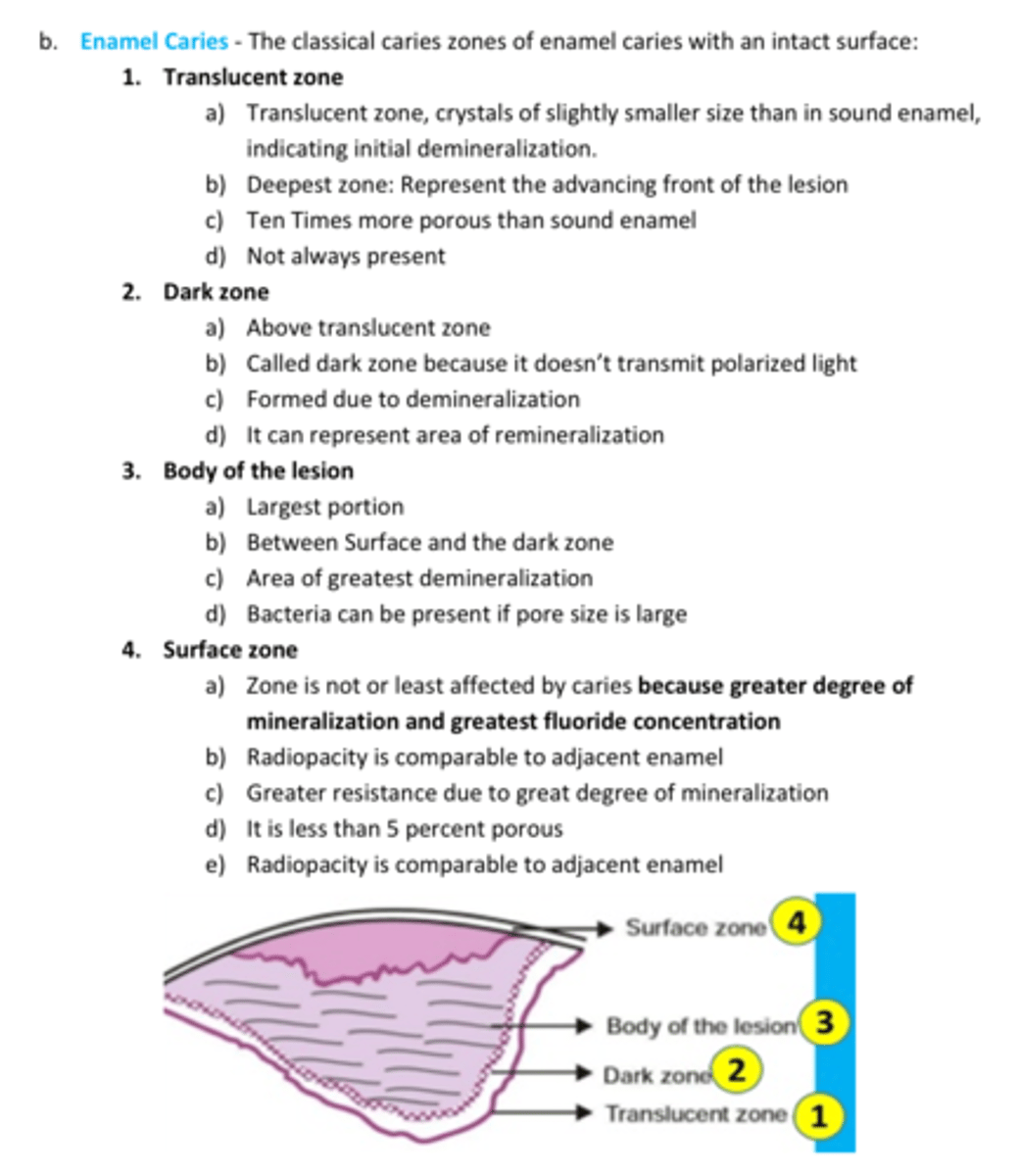
Zones of Enamel Caries
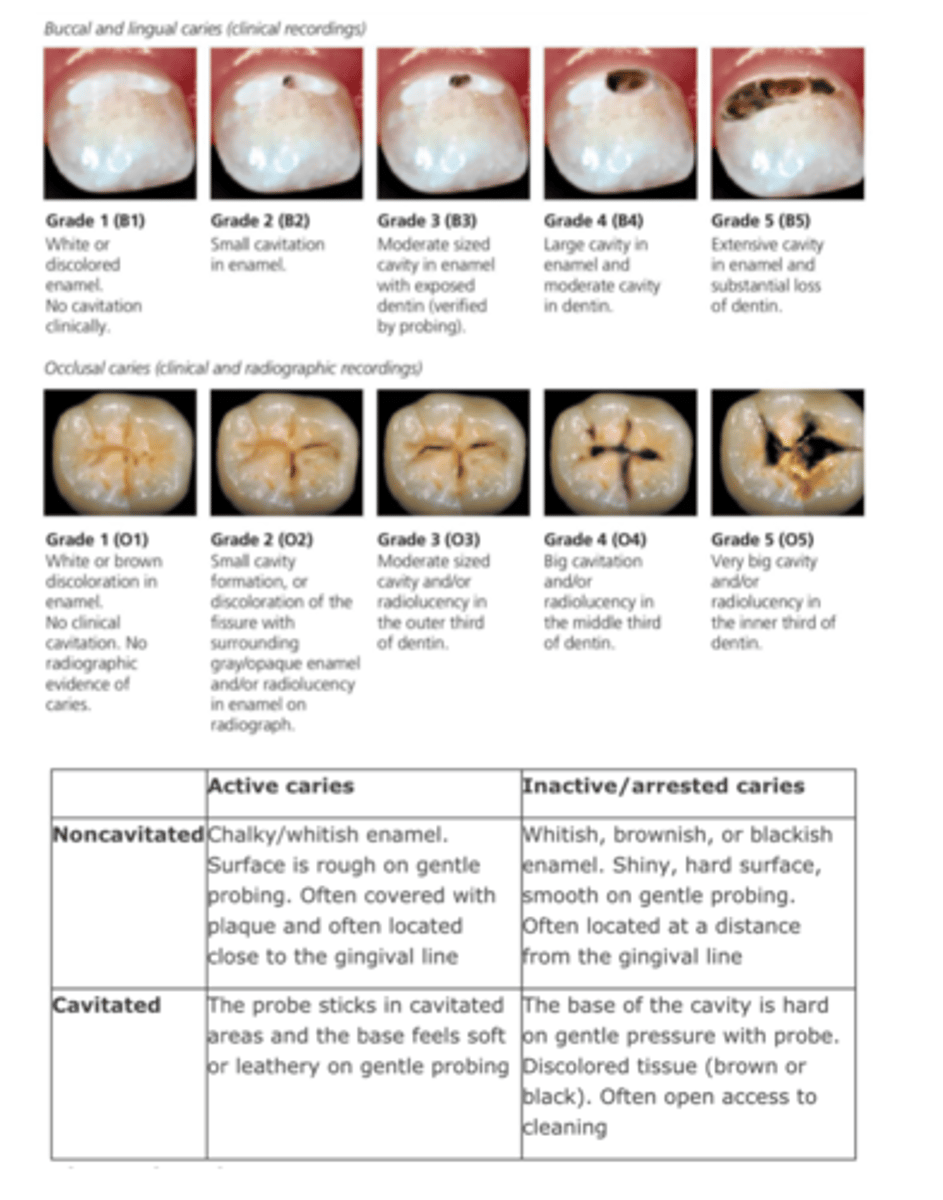
review Cavitated/Non-cavitated Caries chart
Root caries
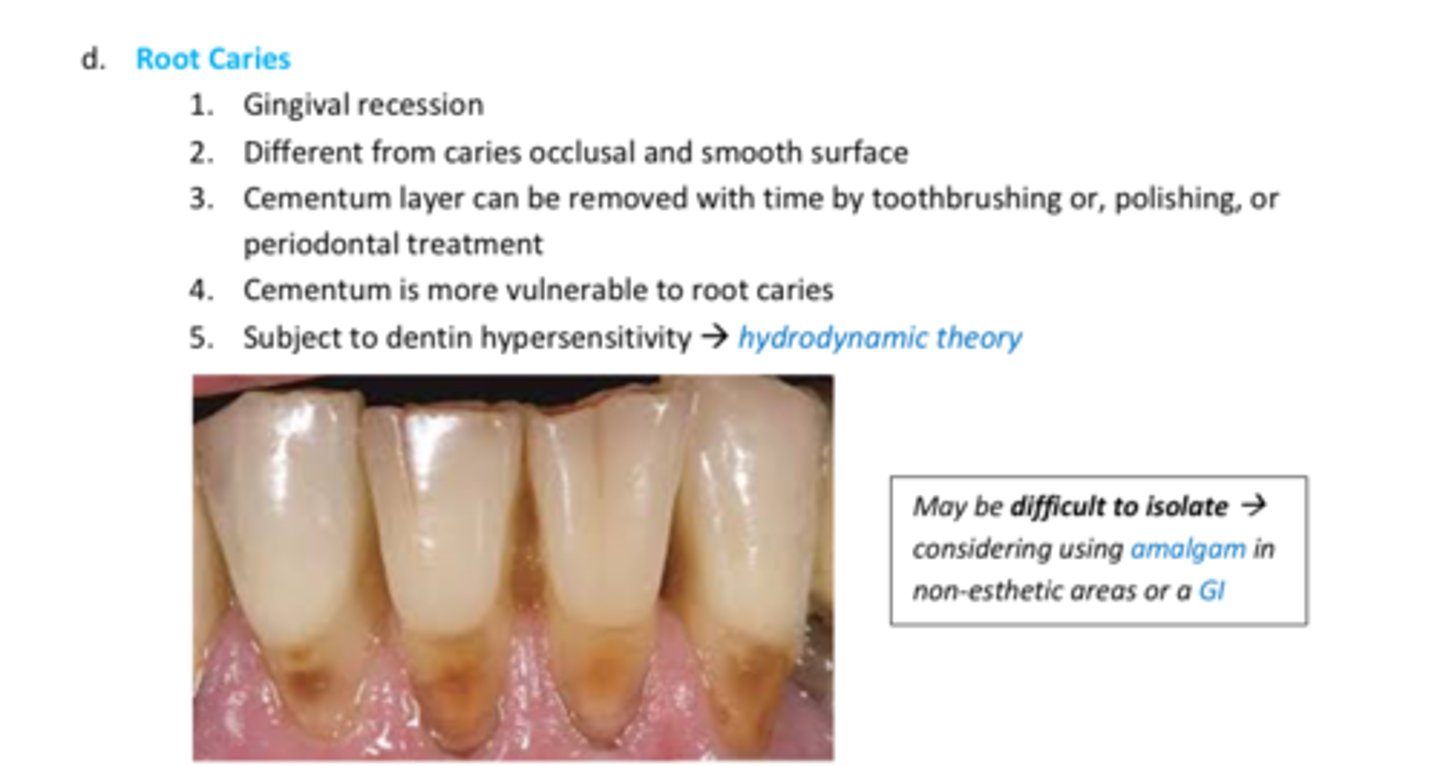
Class V Caries (at CEJ) or Root caries
- use GI/RMGI bc of moisture contamination
- Fuji II (RMGI)
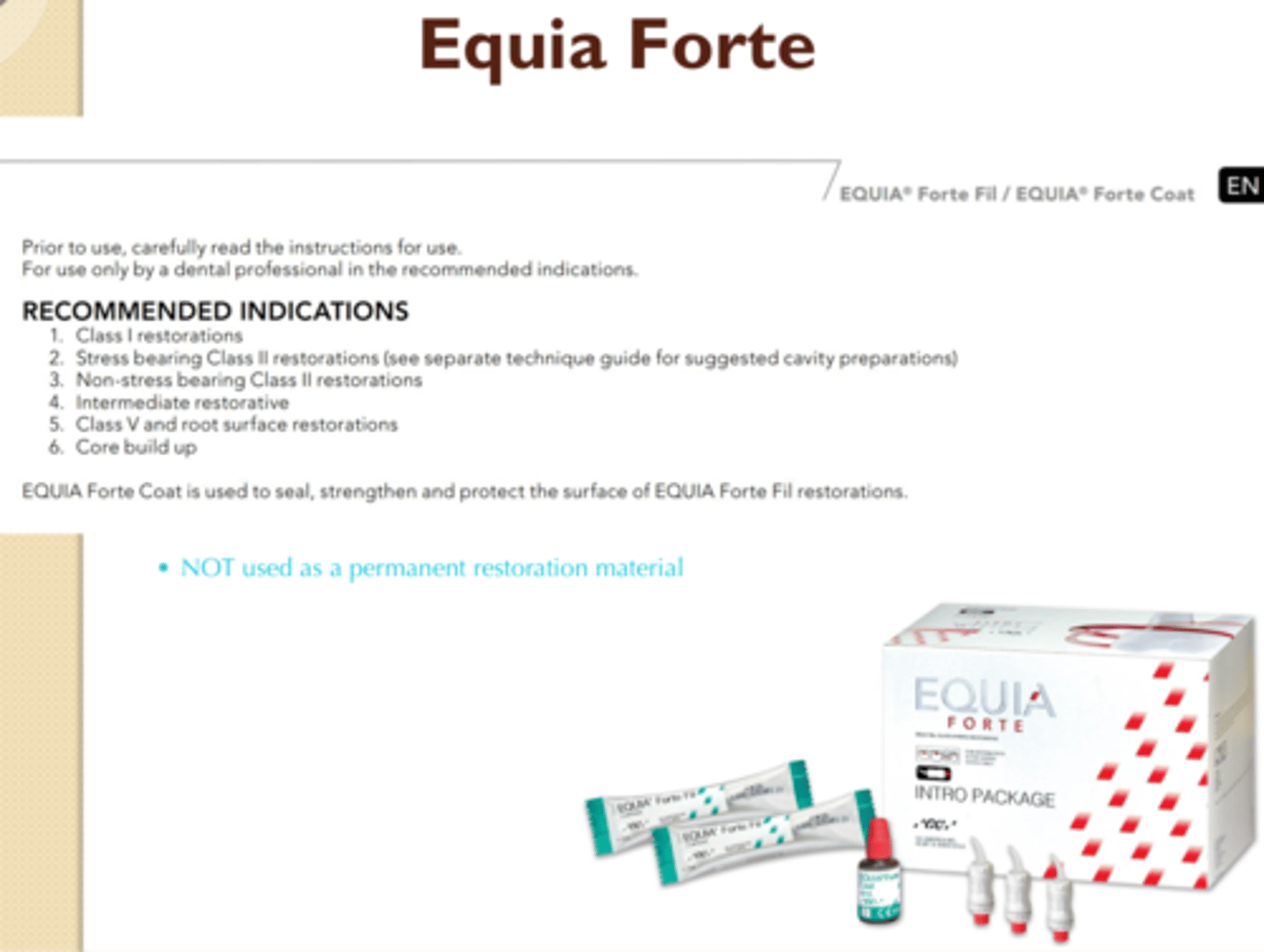
- Equia Forte??
- check this
Consider using a GI or Amalgam (in non-esthetic areas) for what type of caries?
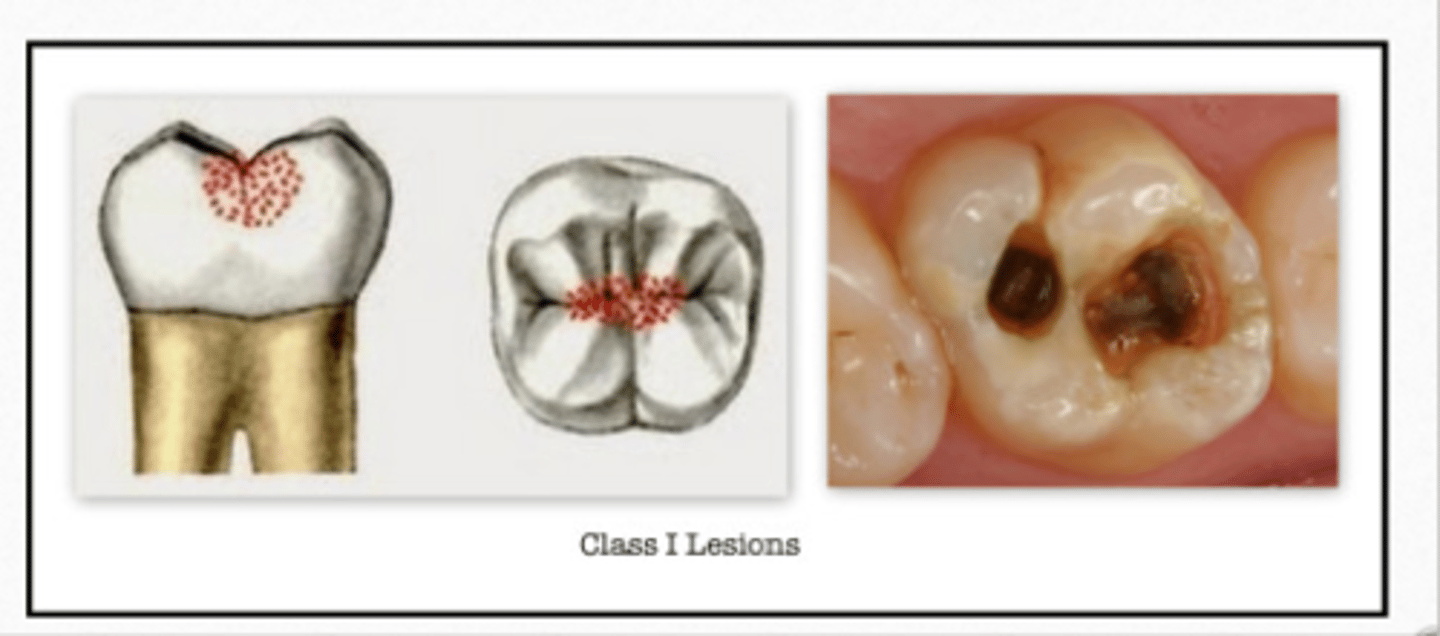
Class I
- Pits/ fissures on the L surfaces of anteriors and on the occlusal, B & L of posteriors
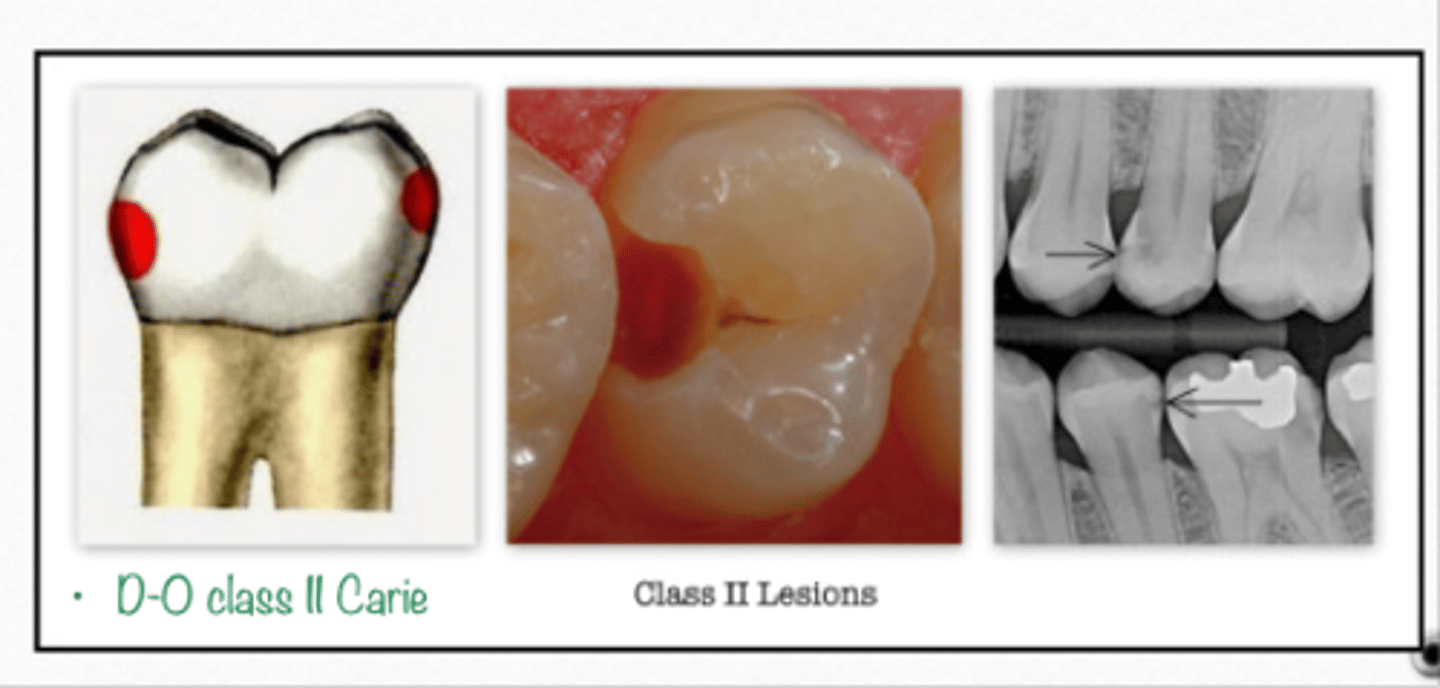
Class II
- Interproximal surfaces of posteriors
- Drop a BOX
Class III
- Interproximal surface of anterior teeth
- Does NOT include the incisal edge
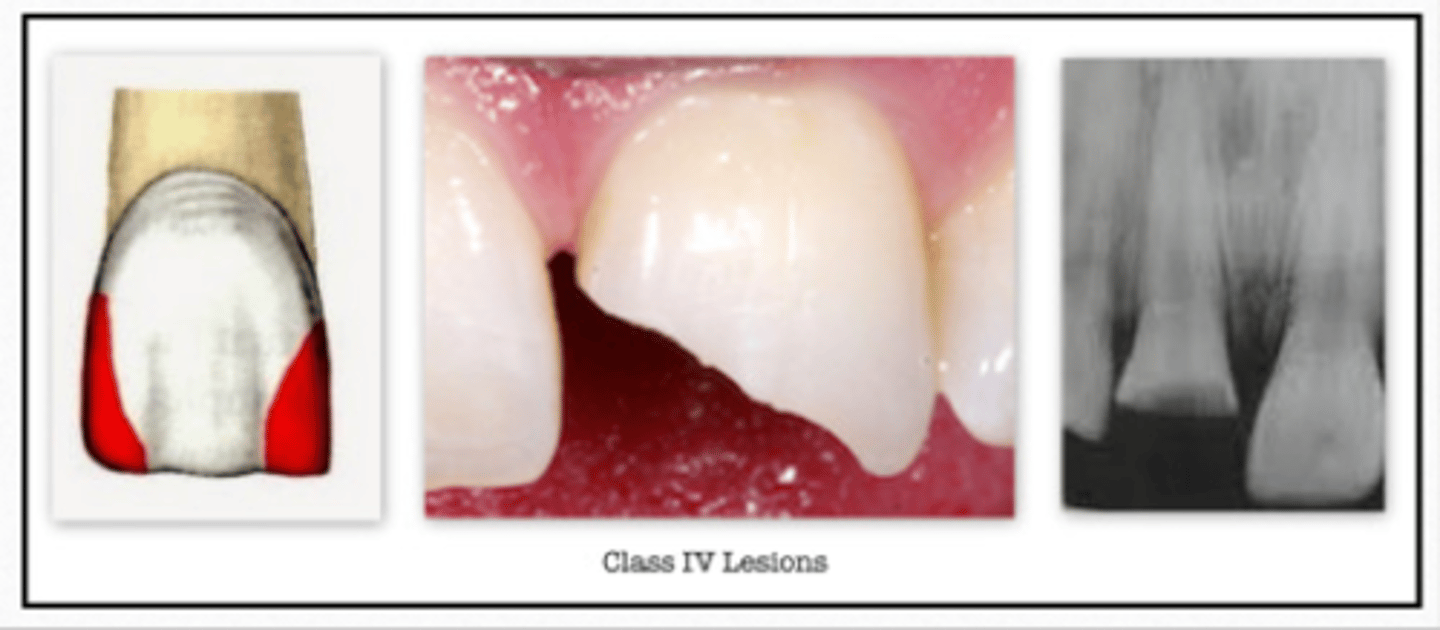
Class IV
- Interproximal surface of anterior teeth
- DOES includes the incisal edge
Class V
- Gingival 1/3
- B or L surface of all teeth
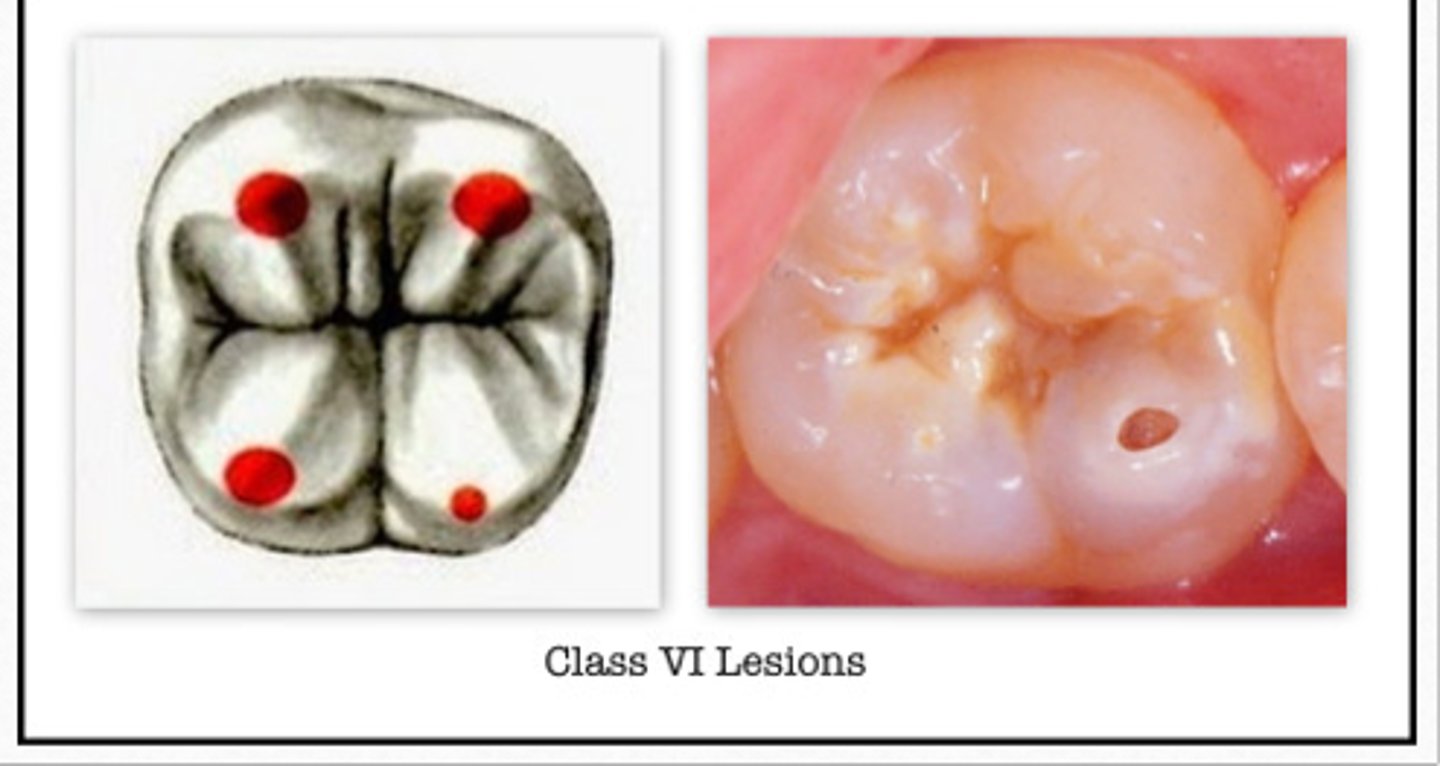
Class VI
- Incisal edges of anterior teeth
- or occlusal cusp tips of posterior teeth
GV Black Classification of Caries:
Class I
Class II
Class III
Class IV
Class V
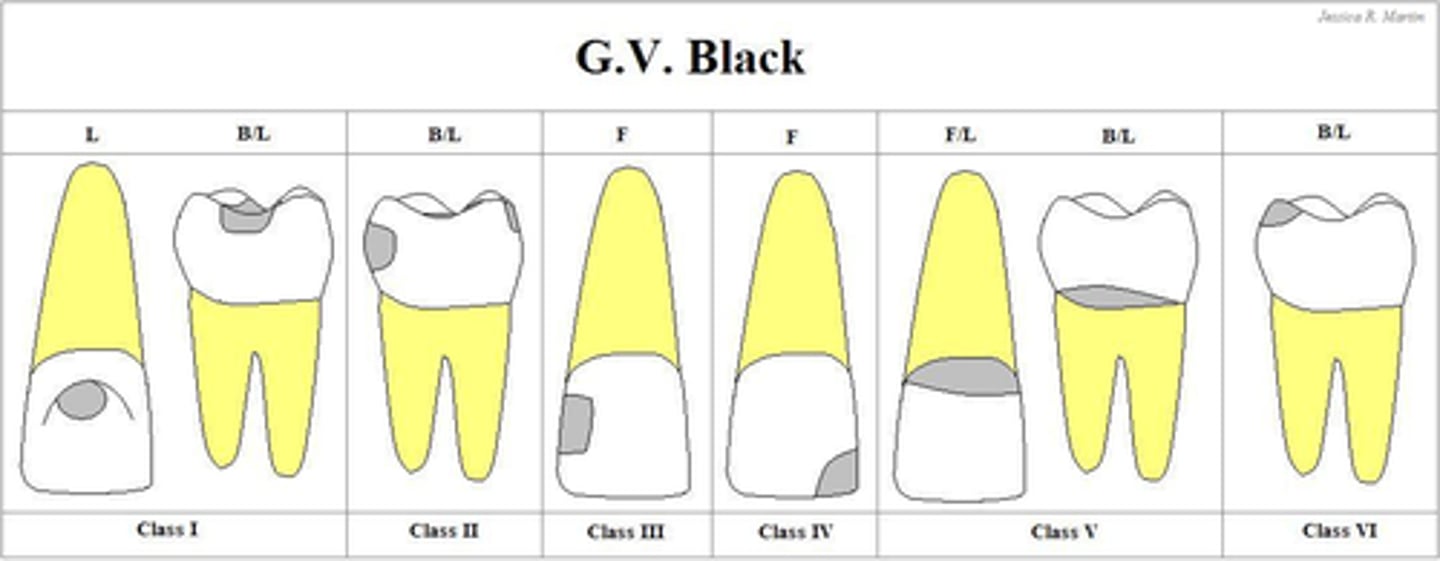
Class I caries
GV Black Classification of Caries:
- Pits/ fissures on the L surfaces of anteriors and on the occlusal, B & L of posteriors
Class II caries
GV Black Classification of Caries:
- Interproximal surfaces of posteriors
- Drop a BOX
Class III caries
GV Black Classification of Caries:
- Interproximal surface of anterior teeth
- Does NOT include the incisal edge

Class IV caries
GV Black Classification of Caries:
- Interproximal surface of anterior teeth
- DOES includes the incisal edge
Class V caries
GV Black Classification of Caries:
- Gingival 1/3
- B or L l surface of all teeth

Class VI caries
GV Black Classification of Caries:
- Incisal edges of anterior teeth
- or occlusal cusp tips of posterior teeth
- ONLY cusp tips
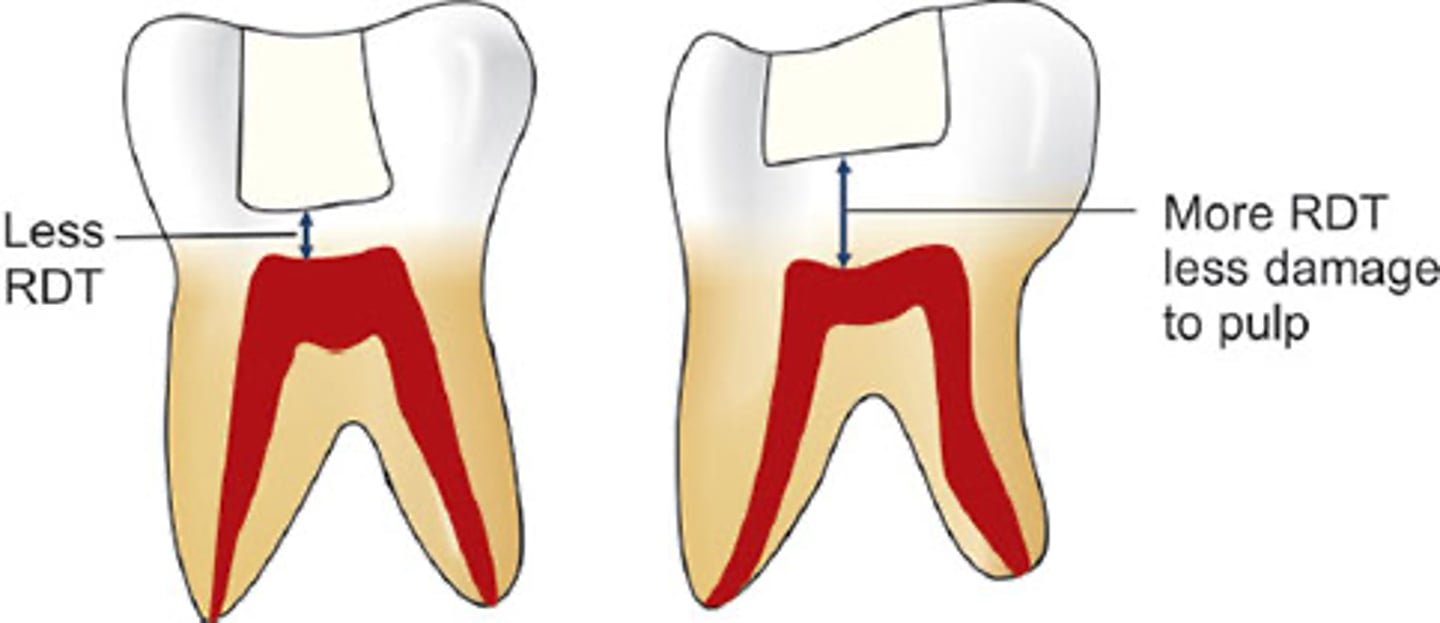
- Amount of tooth structure you have from the depth of cavity prep to the pulp
- single most important factor in protecting the pulp from insult/damage
- the pulp is MOST safe if there is at LEAST 0.5-2mm of structure btw prep & pulp
What is the Remaining Dentinal Thickness?
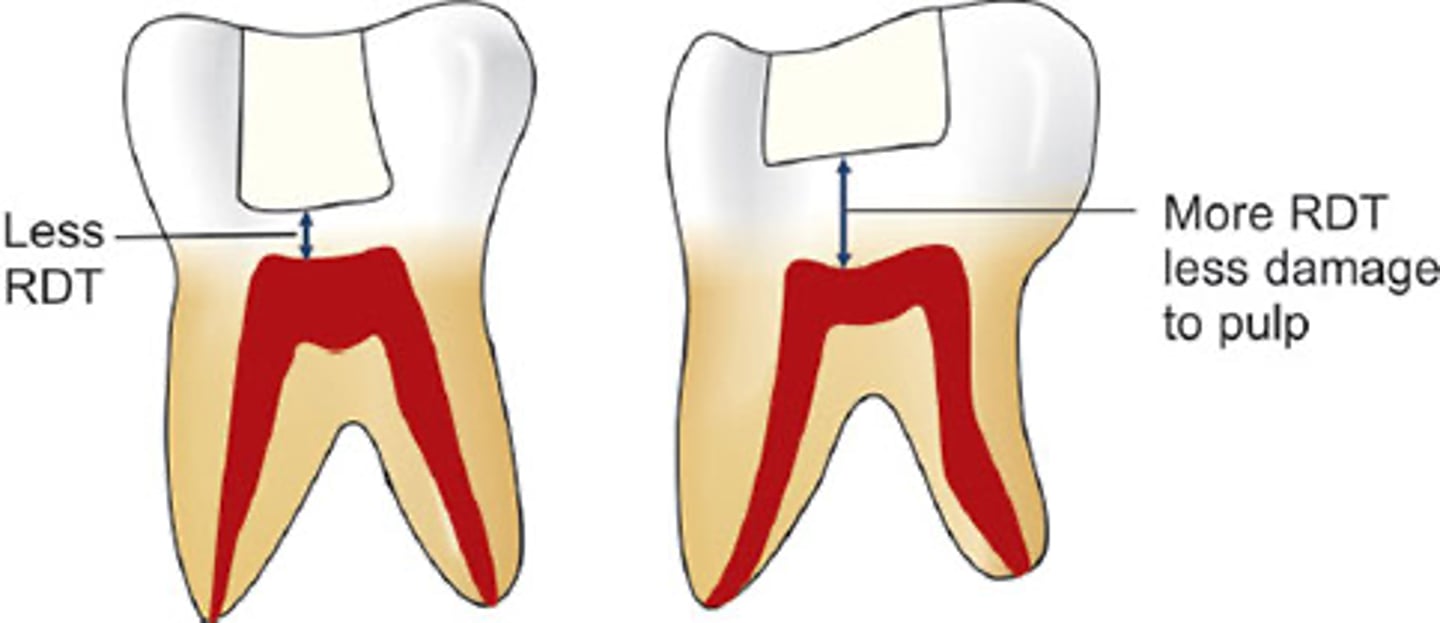
Remaining Dentinal Thickness (RDT)
Goes from the depth of the cavity preparation to the pulp
is the single most important factor in protecting the pulp from insult/damage
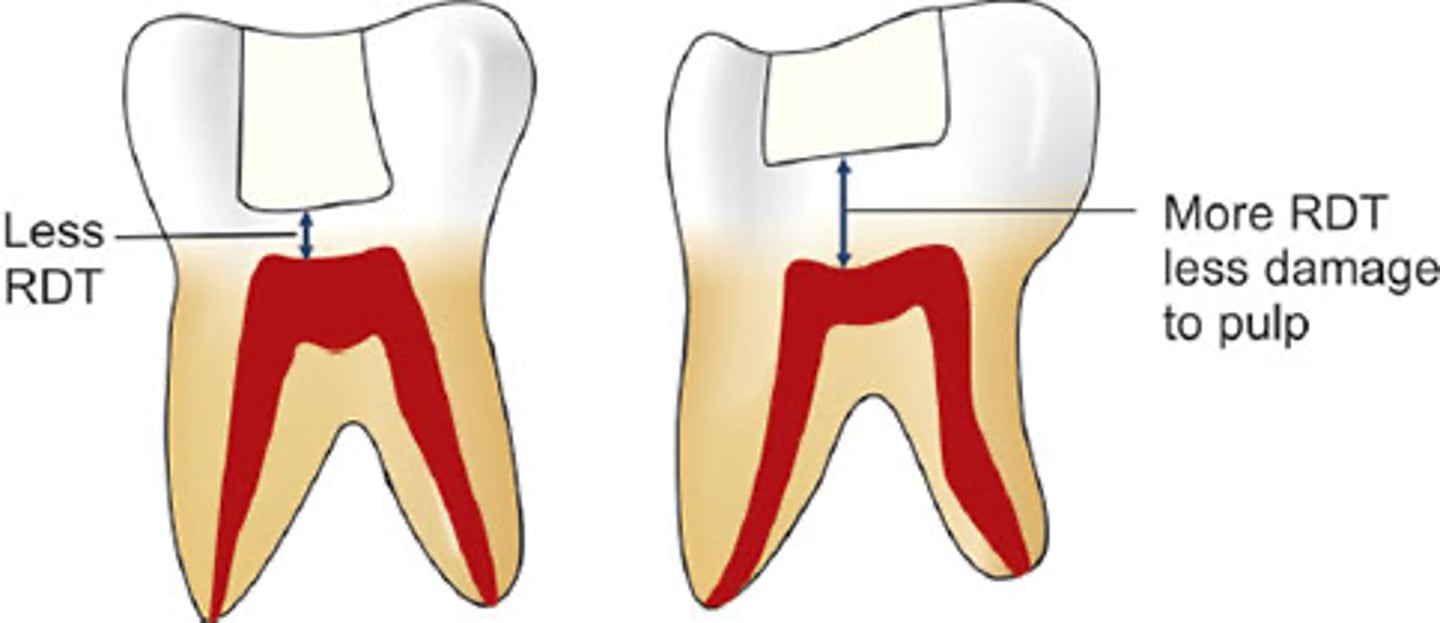
Remaining Dentinal Thickness (RDT)
Single most important factor in protecting the pulp from insult/damage
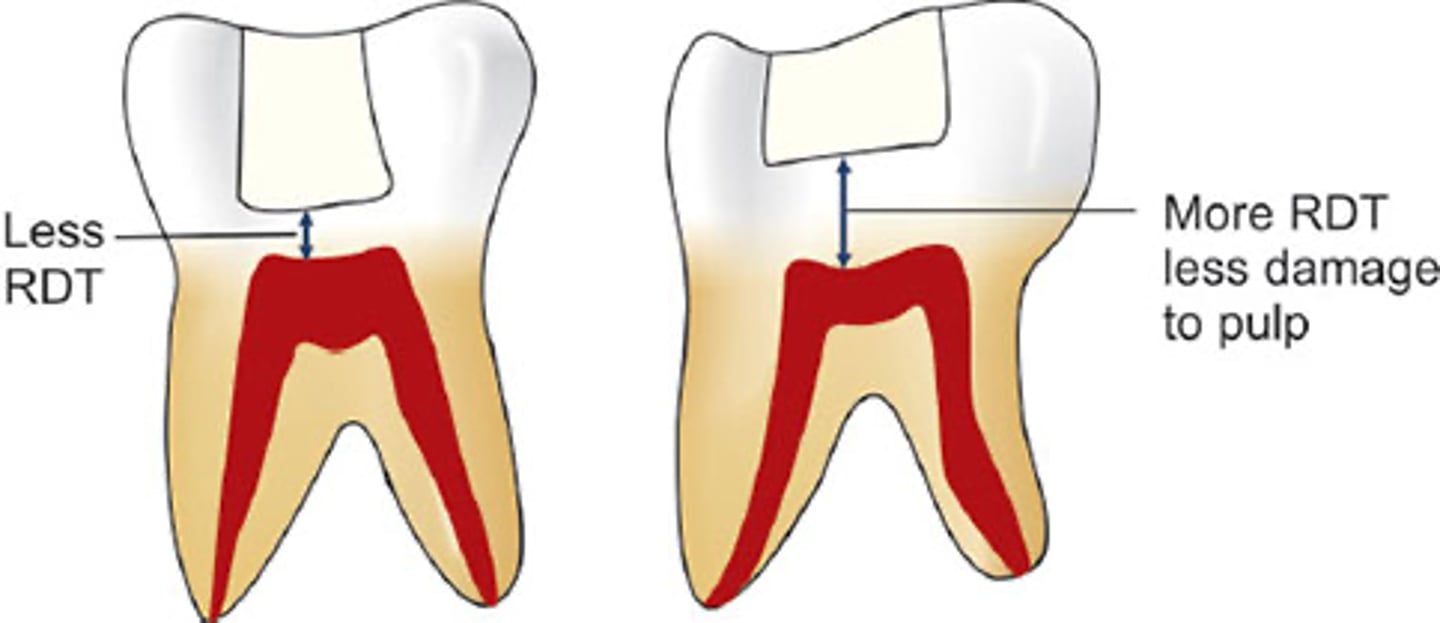
0.5
2.0
RDT is the single most important factor in pulpal protection:
____ mm thickness of dentin protects pulp by 75%
1.0 mm thickness of dentin protects pulp by 90%
Little pulpal reaction occurs when there is an RDT of ____
mm or more!!!
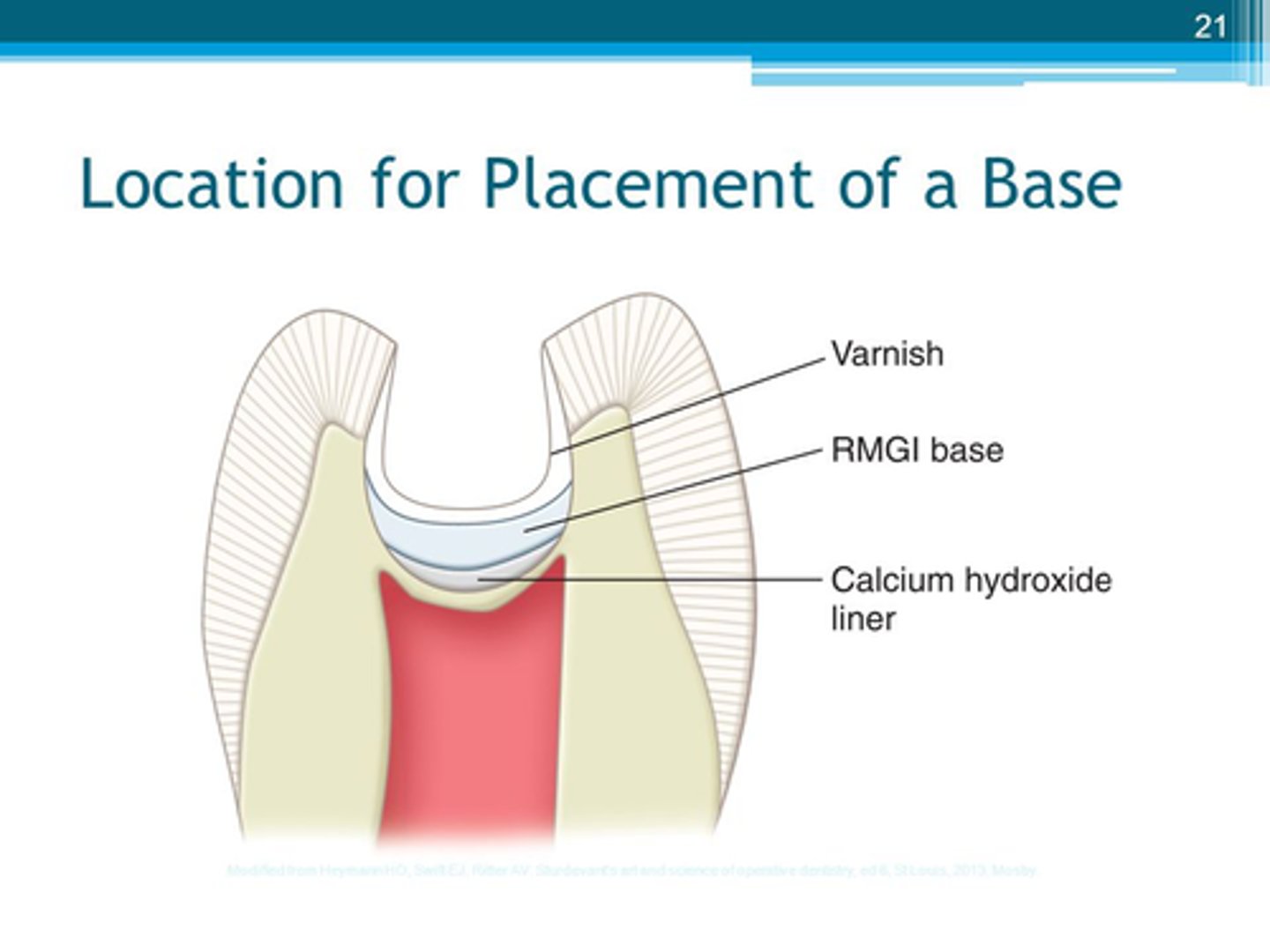
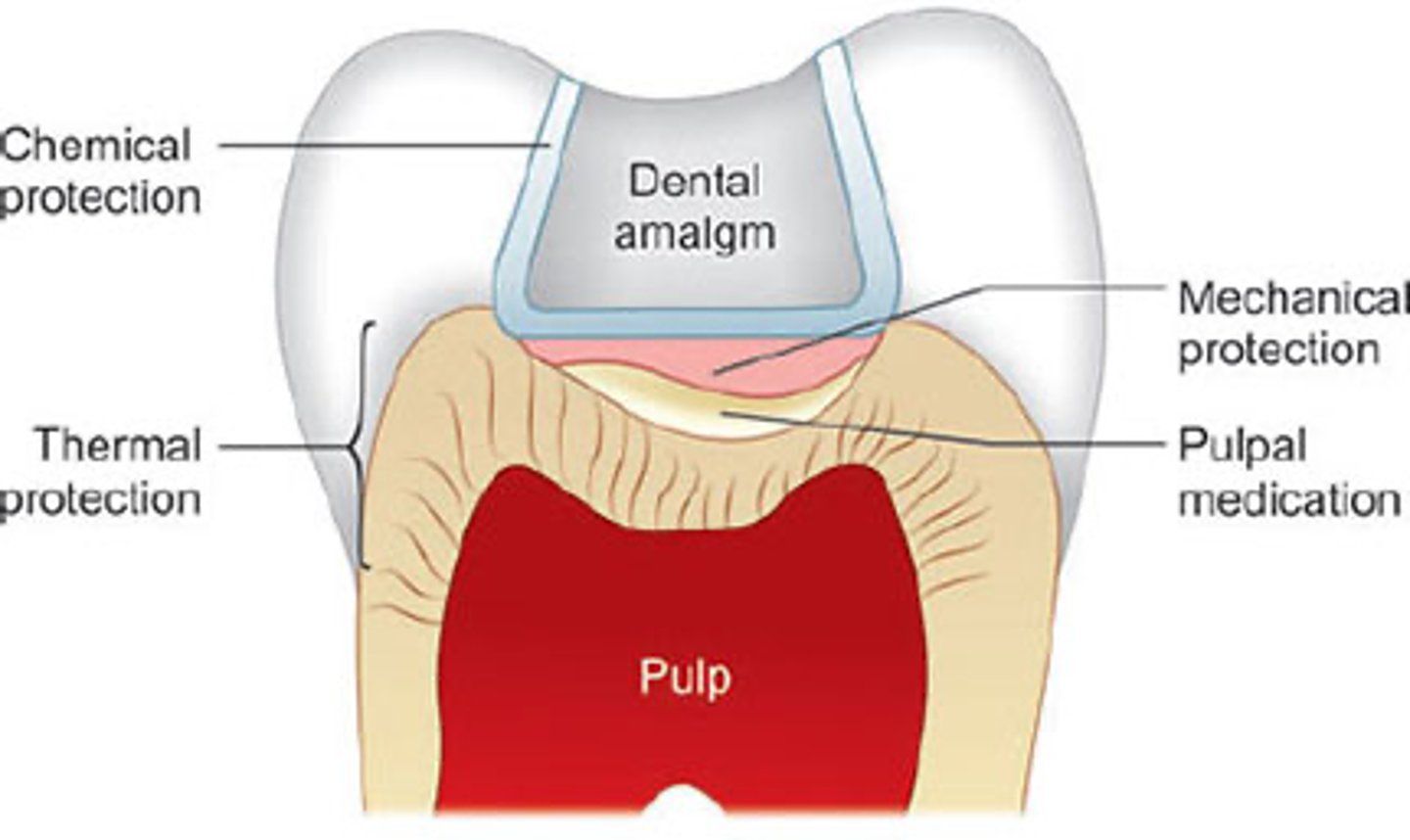
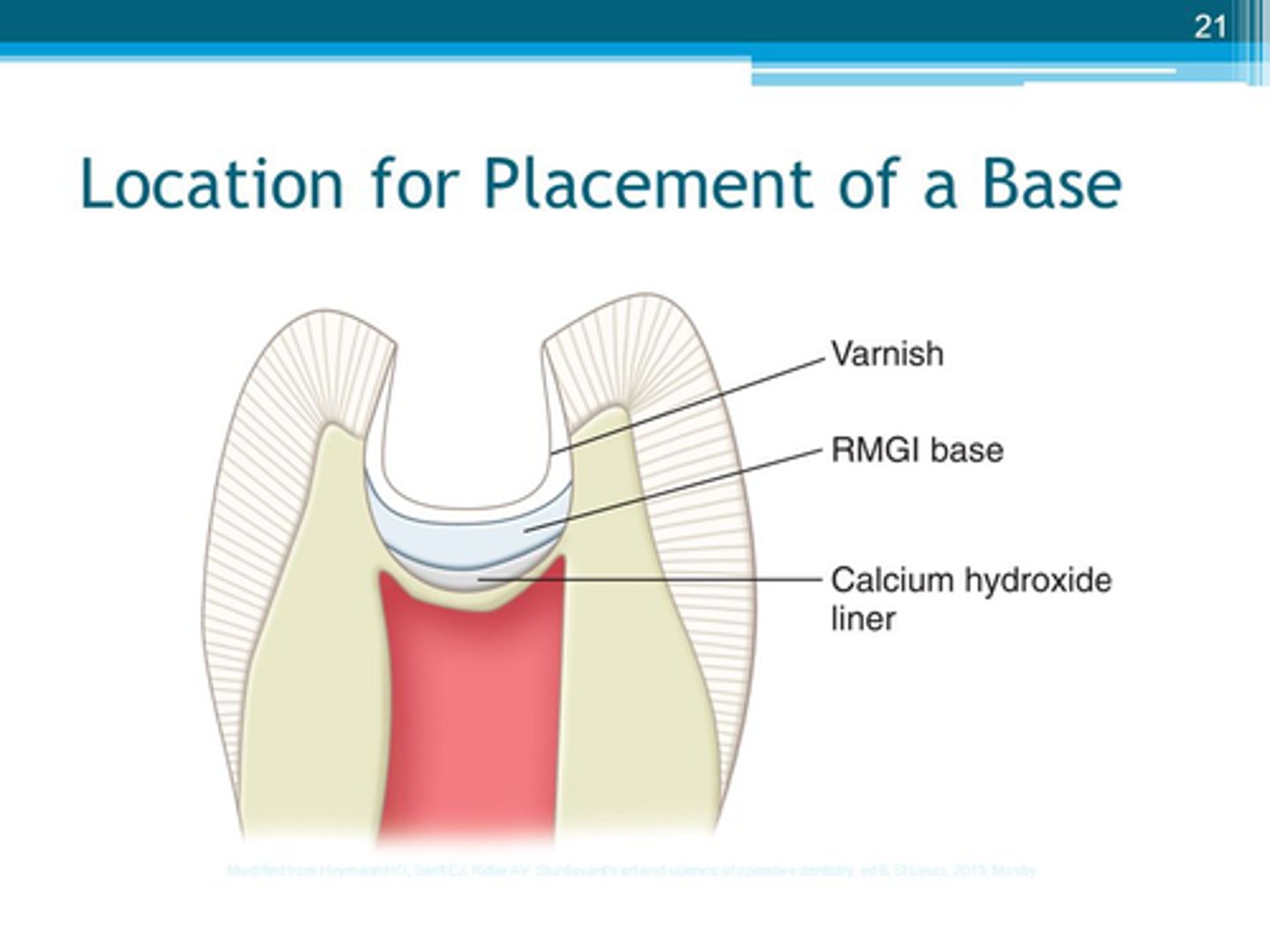
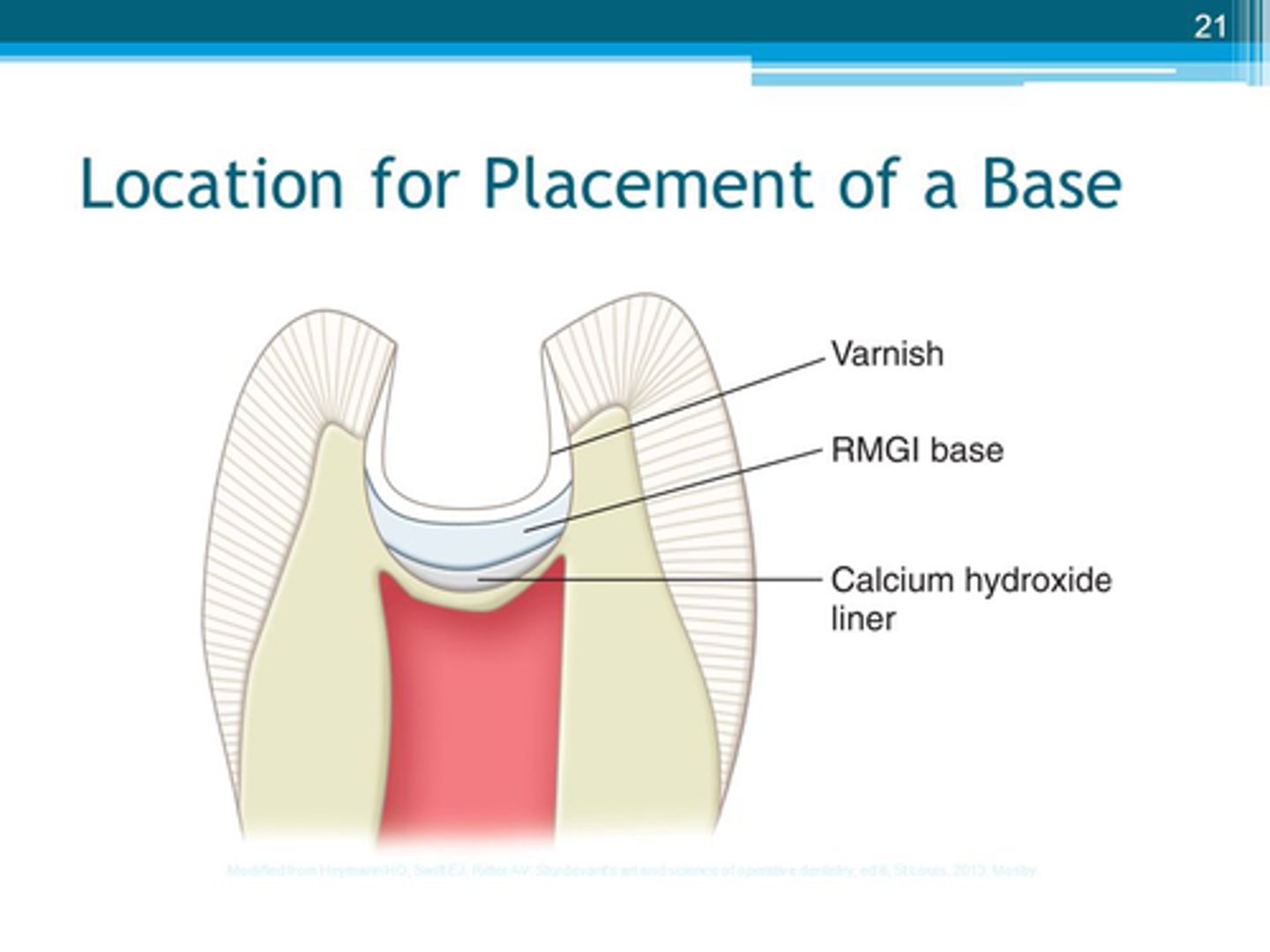
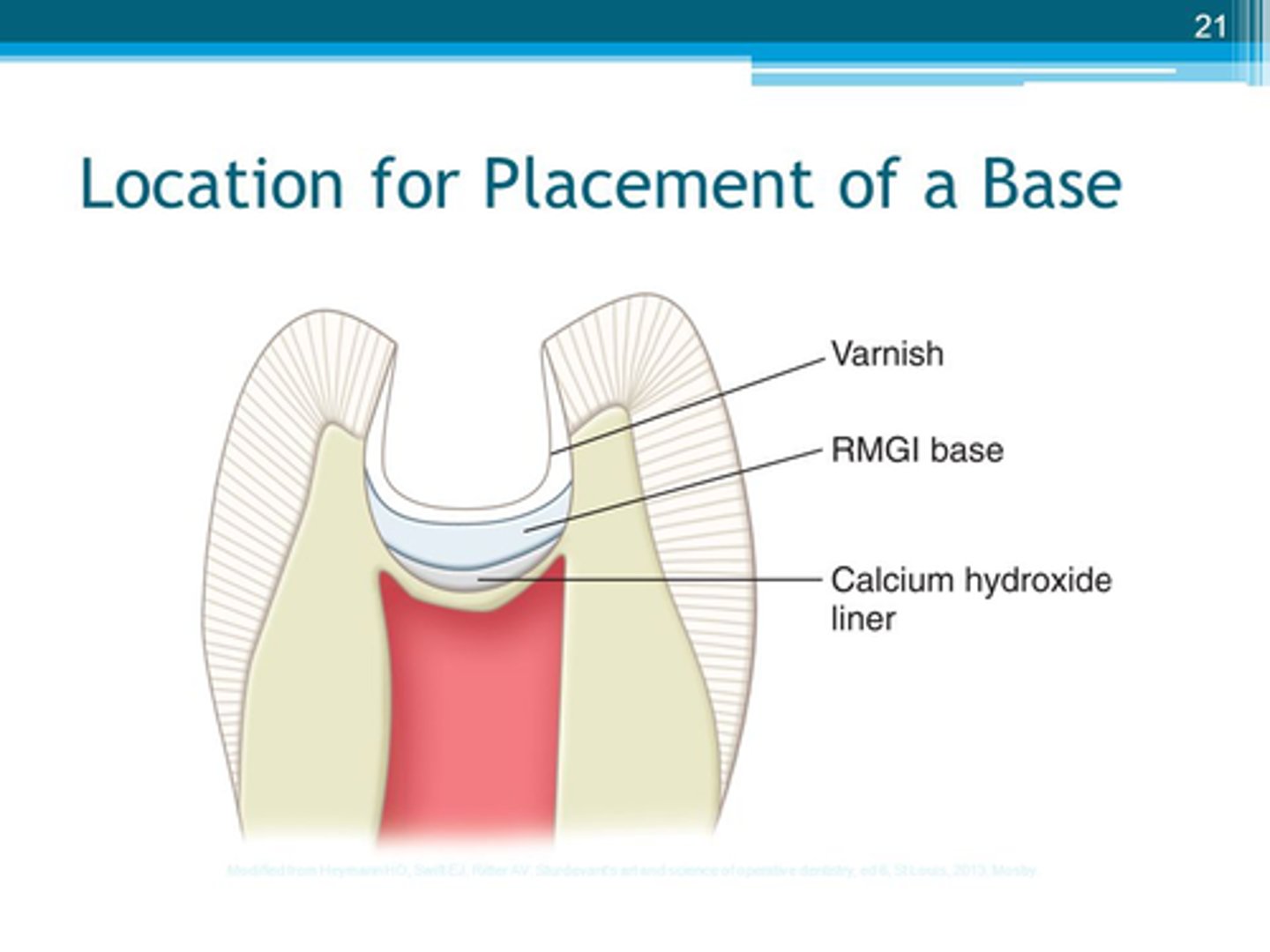
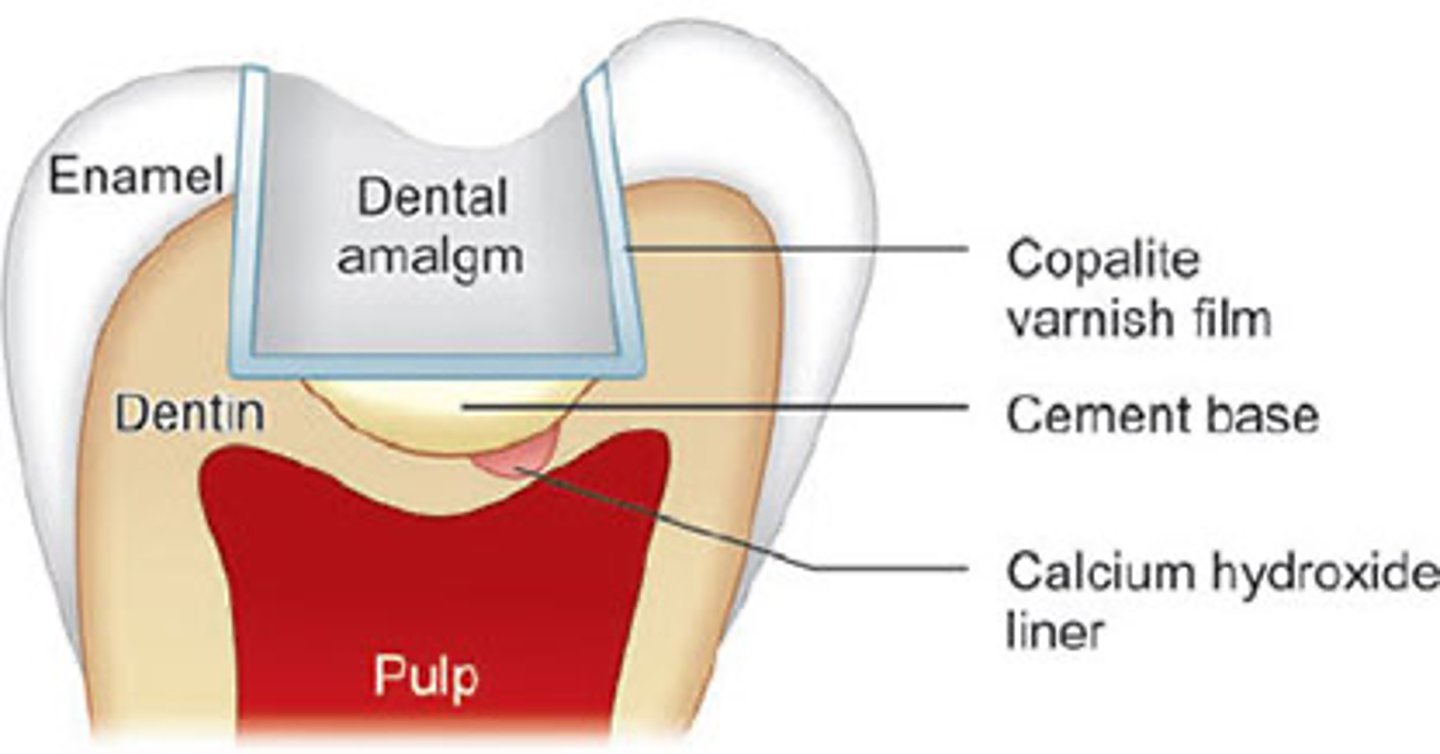
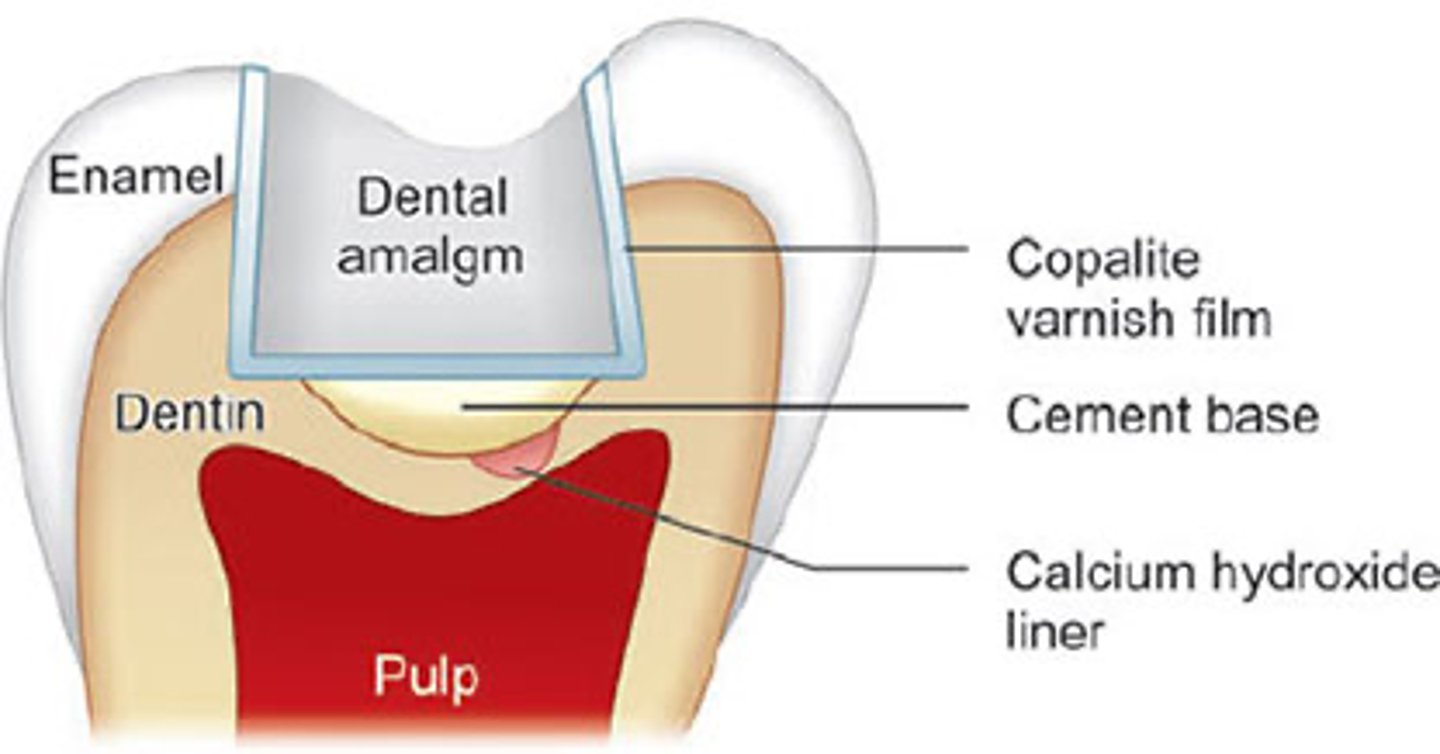
Cavity liners
- used to protect the pulp from the effects of restorative materials
- this is why they are usually applied to dentin NEAR the pulp (to protect it)
- Indicated for= Sensitivity
ex:
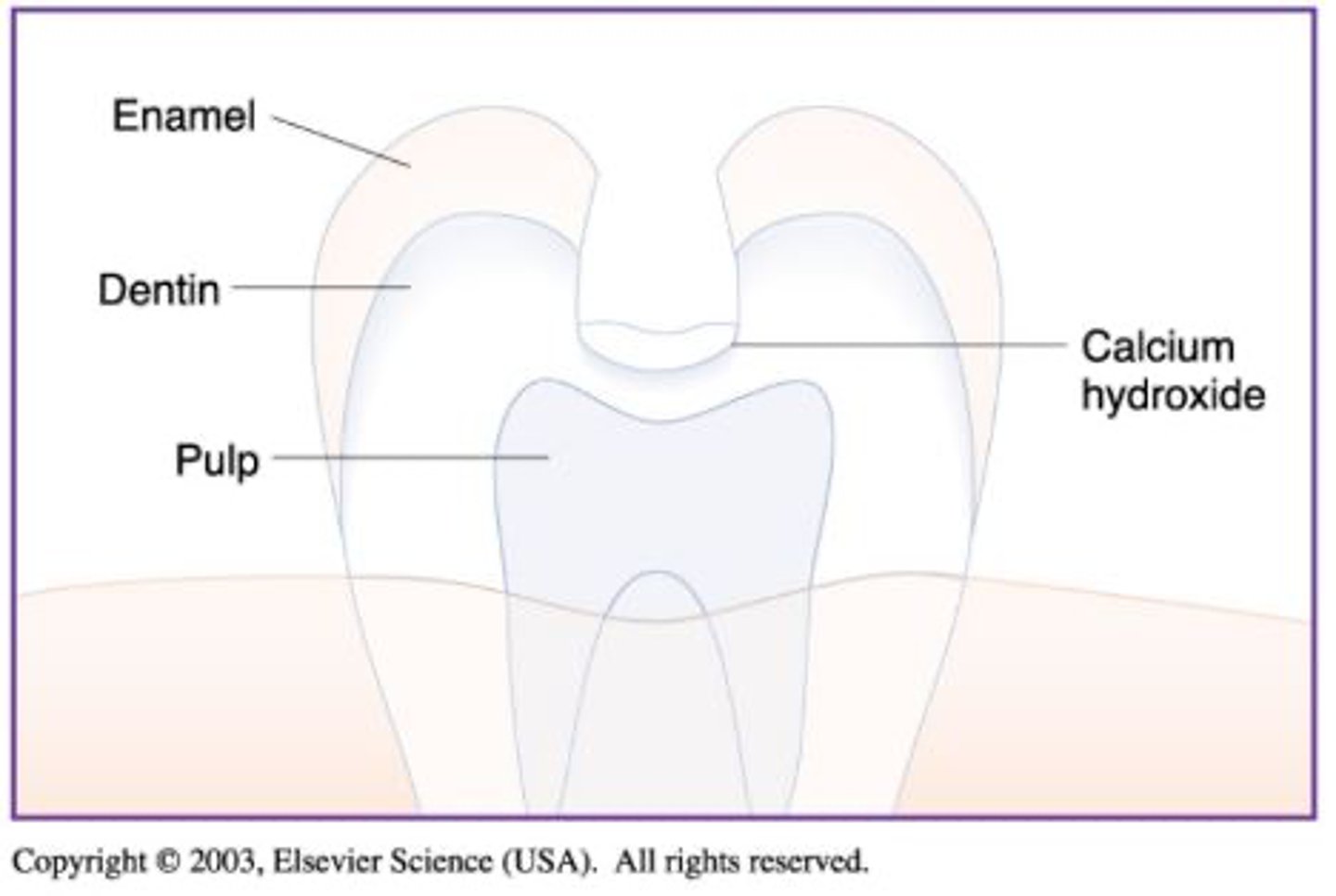
- Calcium Hydroxide (CaOH)
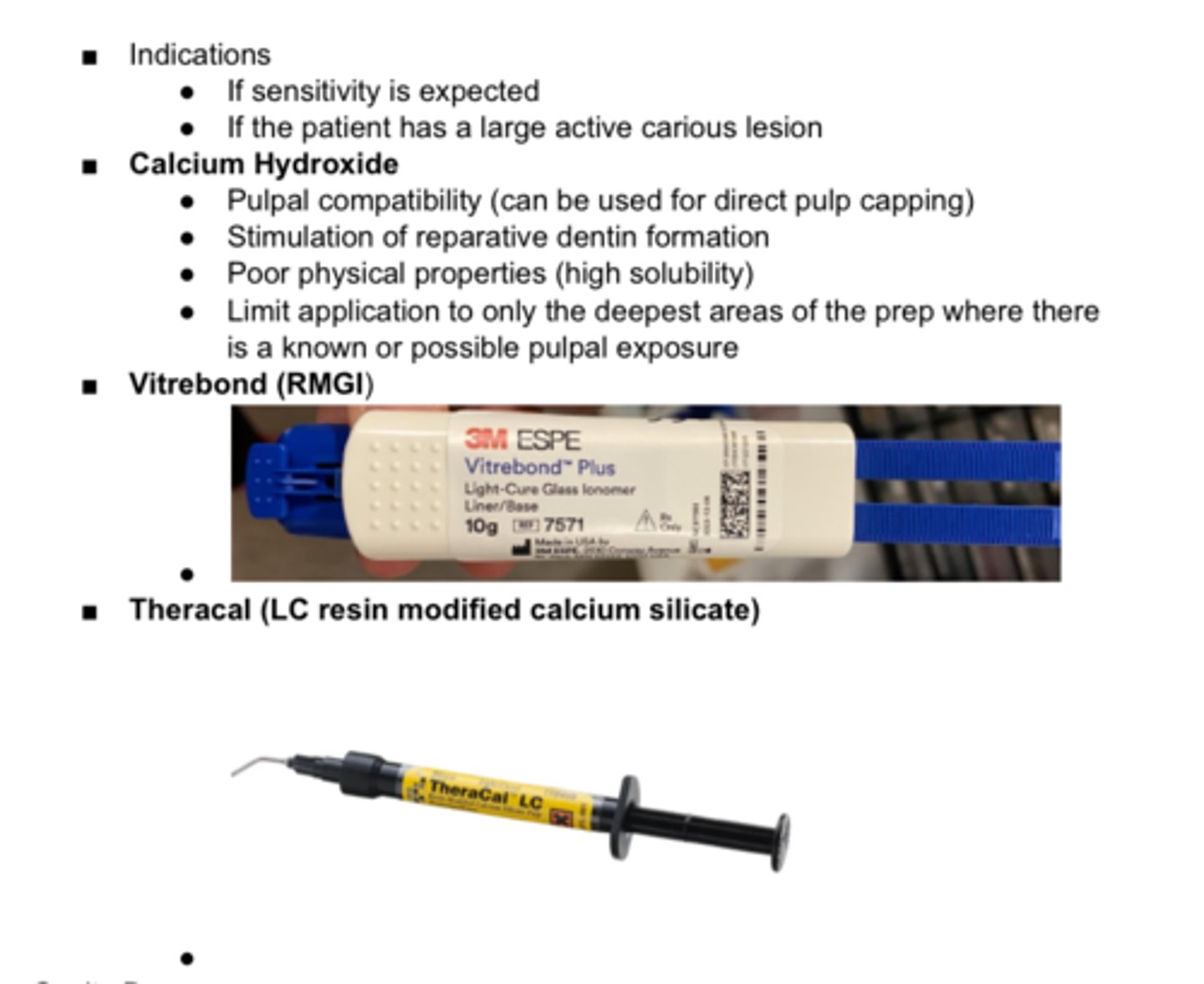
- Vitrebond (RMGI)
- Theracal
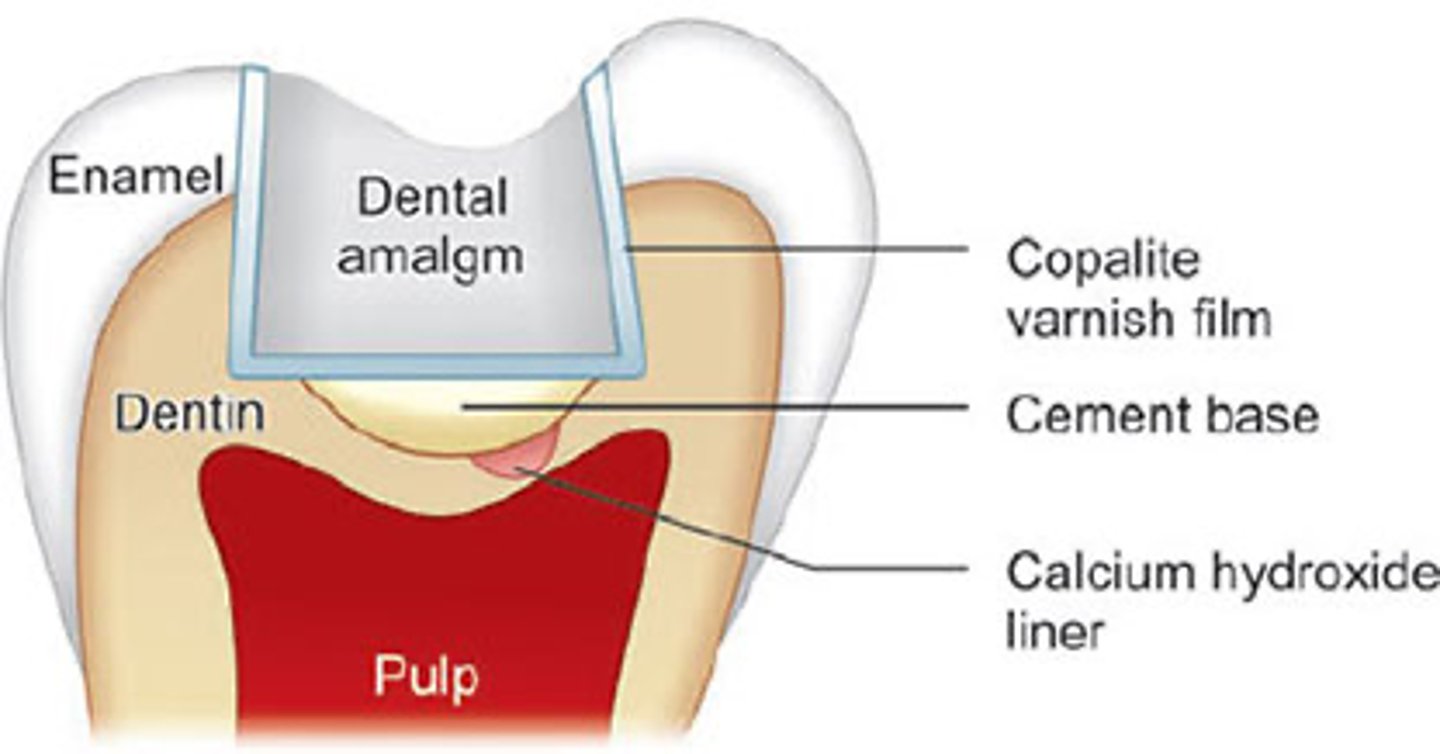
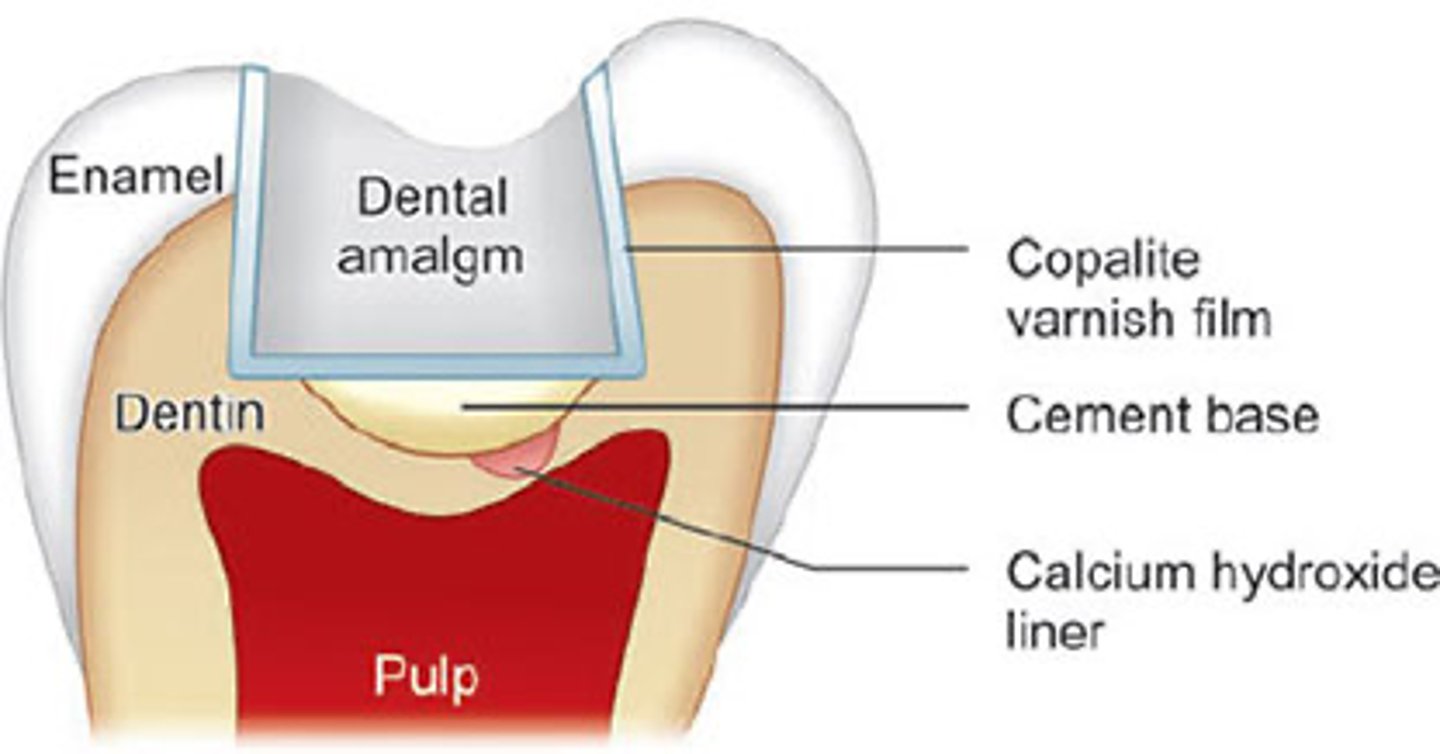
Cavity bases
- used to replace missing dentin/is placed on the dentin in the floor of a prep
- protects the pulp by providing thermal insulation due to temp changes & through absorbing occlusal forces
ex:
- Zinc oxide- Eugenol & Zinc phosphate cements
(good thermal insulation)
- Glass Ionomers (Equia)
- Vitrebond (RMGI)
- Theracal
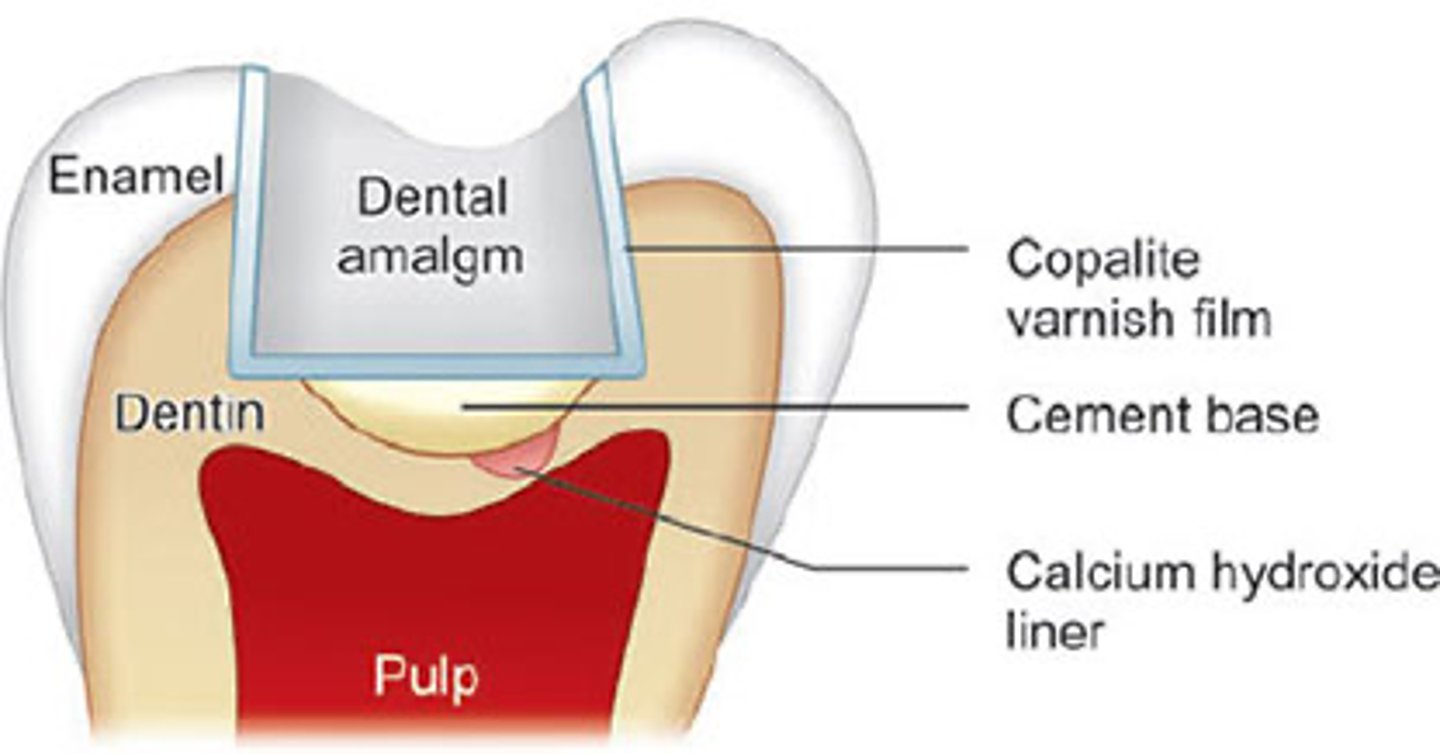
Cavity sealers
- Protective coating placed on all WALLs of a prep to prevent leakage & seal the restoration
ex:
- Cavity Varnish (ONLY applied b4 placing amalgam!!!)
- NEVER used w adhesive materials (comp resin, GI ect bc it interferes w bonding)
Restorative materials & their functions:
Cavity liners= (3)
Cavity bases= (4)
Cavity sealers= (1)
-know
- Cavity liners & bases are used to protect & recent damage the pulp
Cavity liners
Indications for _____ ____
- If sensitivity is expected
- If pt has large active carious lesions that could affect the pulp
pulp
Cavity liners & bases are used to protect & prevent damage to the _____
Cavity Liner
- used to protect the pulp from the effects of restorative materials
- this is why they are usually ONLY applied to dentin NEAR the pulp (to protect it)
- Indicated for= Sensitivity
ex:
- Calcium Hydroxide (CaOH)
- RMGI (Vitrebond)
- Theracal
Cavity liners
- bc they protect the pulp from restorative materials
are usually ONLY applied to dentin NEAR the pulp
Cavit liners
- vitrabond= is a RMGI liner/base material
These are?
- Calcium Hydroxide (CaOH)
- Vitrebond (RMGI)
- Theracal
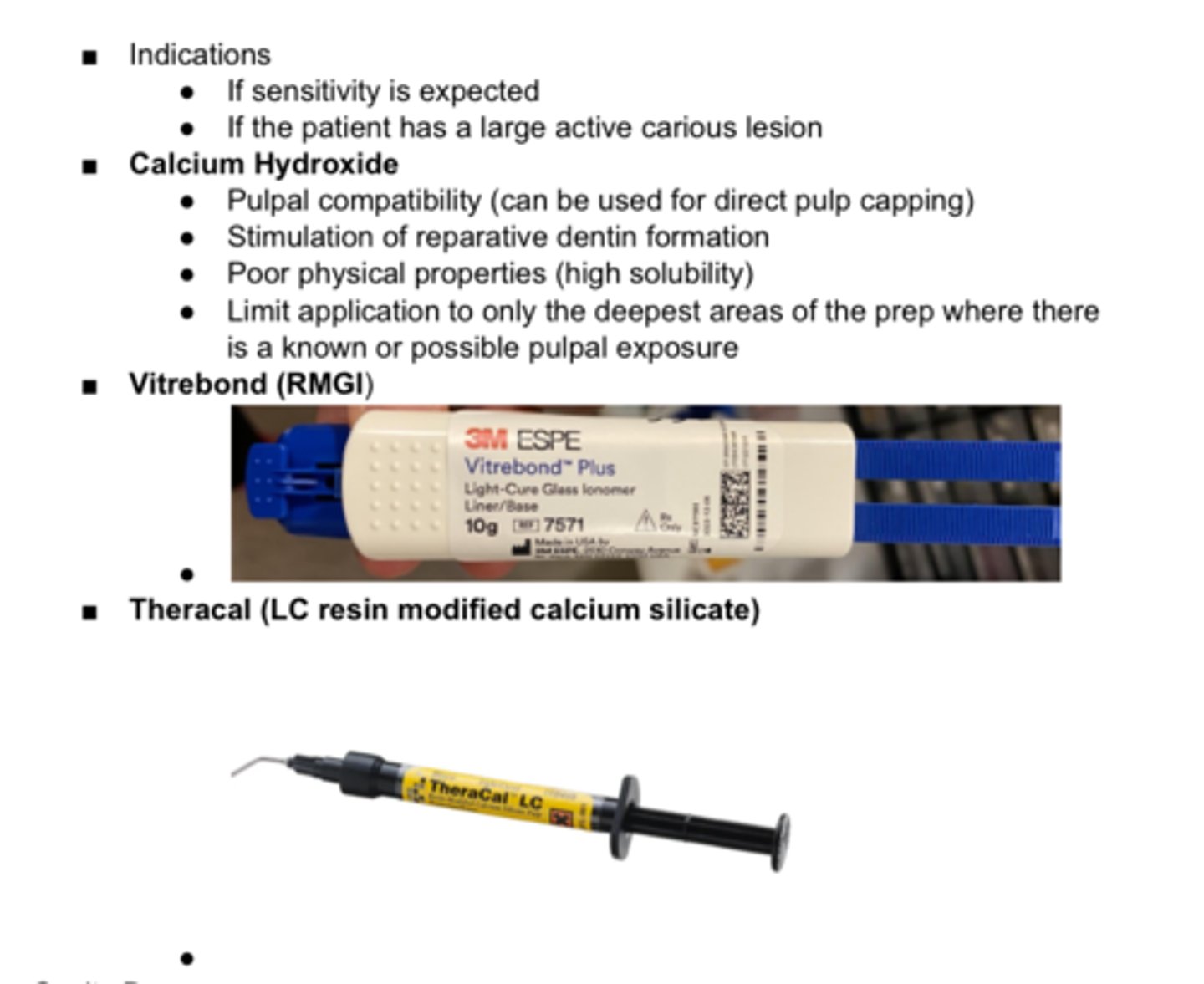
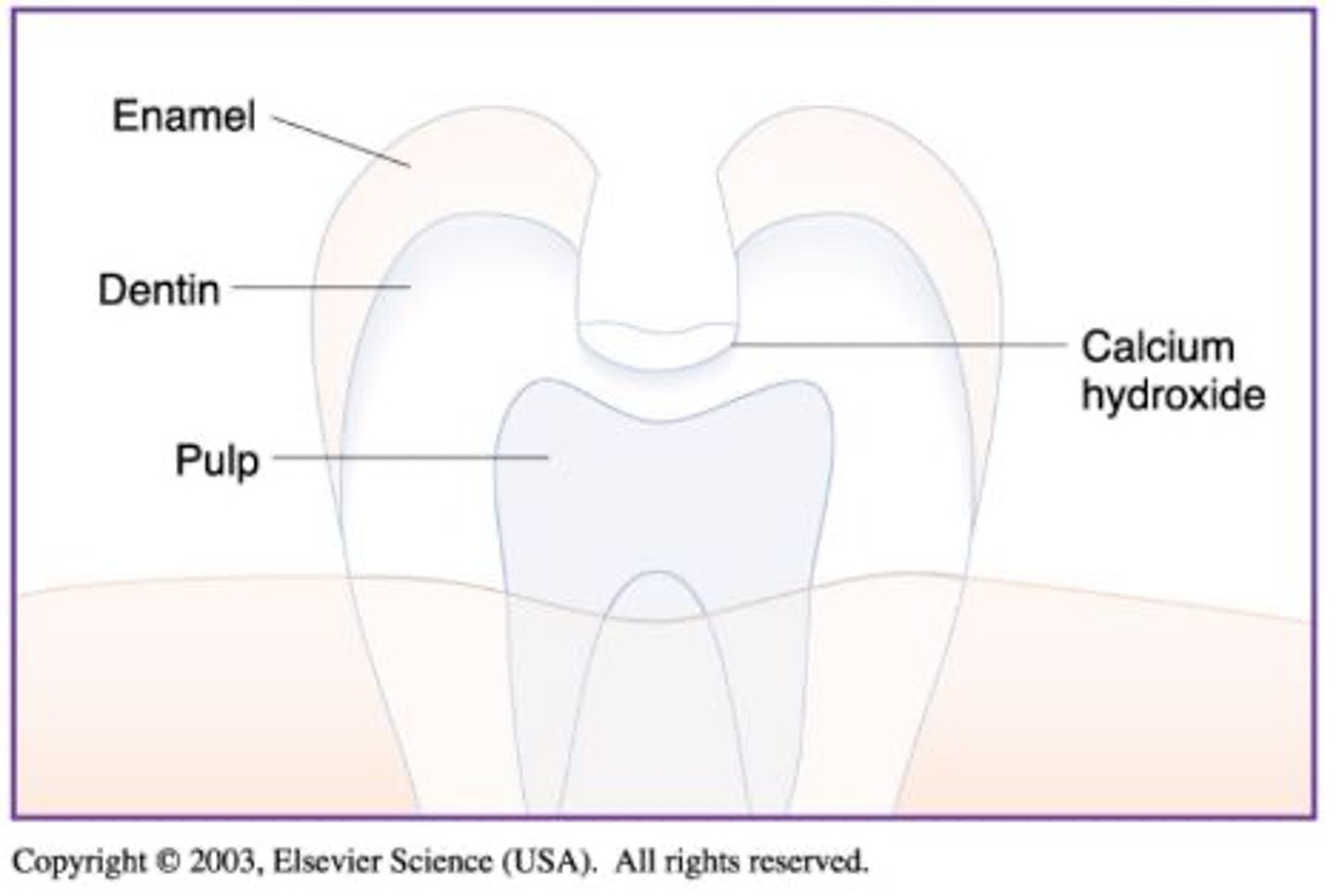
Calcium Hydroxide
Indications for which Cavity liner:
Pulpal compatibility (can be used for direct pulp capping)
Stimulation of reparative dentin formation
Poor physical properties (high solubility)
Limit application to only the deepest areas of the prep where there is a known or possible pulpal exposure
Cavity Bases
- used to replace missing dentin/is placed on the dentin in the floor of a prep
- protects the pulp by providing thermal insulation due to temp changes & through absorbing occlusal forces
ex:
- Zinc oxide- Eugenol & Zinc phosphate cements
(good thermal insulation)
- Glass Ionomers (Equia)
- Vitrebond
- Theracal
- Zinc oxide- Eugenol & Zinc phosphate cements
(good thermal insulation)
- Glass Ionomers (Equia)
- Vitrebond (RMGI)
- Theracal
List 4 Cavity Bases
- that can be used to provide thermal insulation to the pulp
- are usually RMGI
Cavity bases
These are?
- Zinc oxide- Eugenol & Zinc phosphate cements
(good thermal insulation)
- Glass Ionomers (Equia)
- Vitrebond
- Theracal
- Cavity Varnish (ONLY applied b4 placing amalgam!!!)
- NEVER used w adhesive materials (comp resin, GI ect bc it interferes w bonding)
List 1 example of a Cavity Sealer
- used to prevent leakage
Cavity sealer
(cavity varnish)
- Protective coating placed on all WALLs of a prep to prevent leakage & seal the restoration
ex:
- Cavity Varnish (ONLY applied b4 placing amalgam!!!)
- NEVER used w adhesive materials (comp resin, GI ect bc it interferes w bonding)
Cavity sealer
(cavity varnish)
This is a?
- Cavity Varnish (ONLY applied b4 placing amalgam!!!)
- NEVER used w adhesive materials (comp resin, GI ect bc it interferes w bonding)
Cavity varnish
- type of cavity sealer
Is ONLY applied b4 placing amalgam!!!
- NEVER used w adhesive materials (comp resin, GI ect bc it interferes w bonding)
true
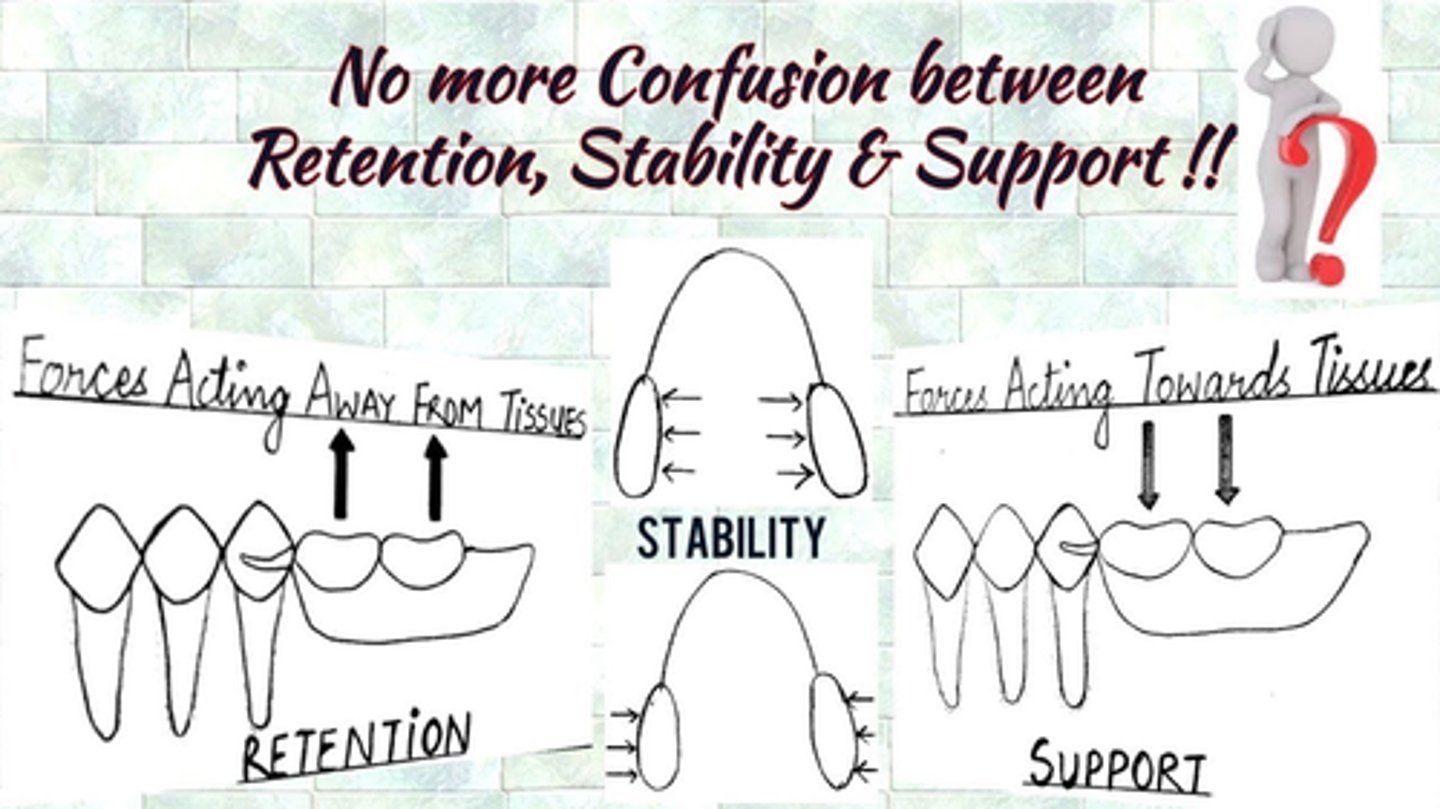
T/F: These are these are the backbone of Prosthodontics
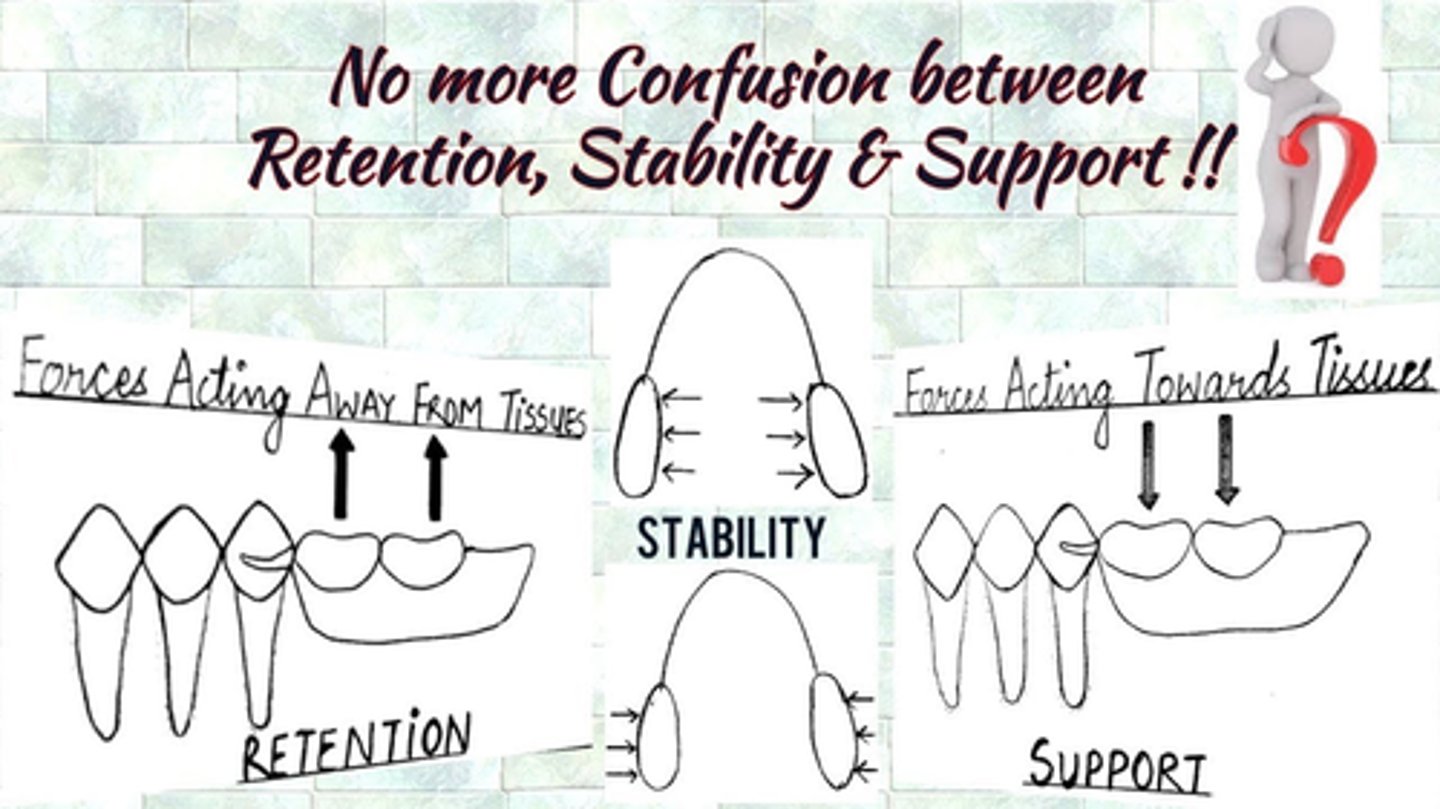
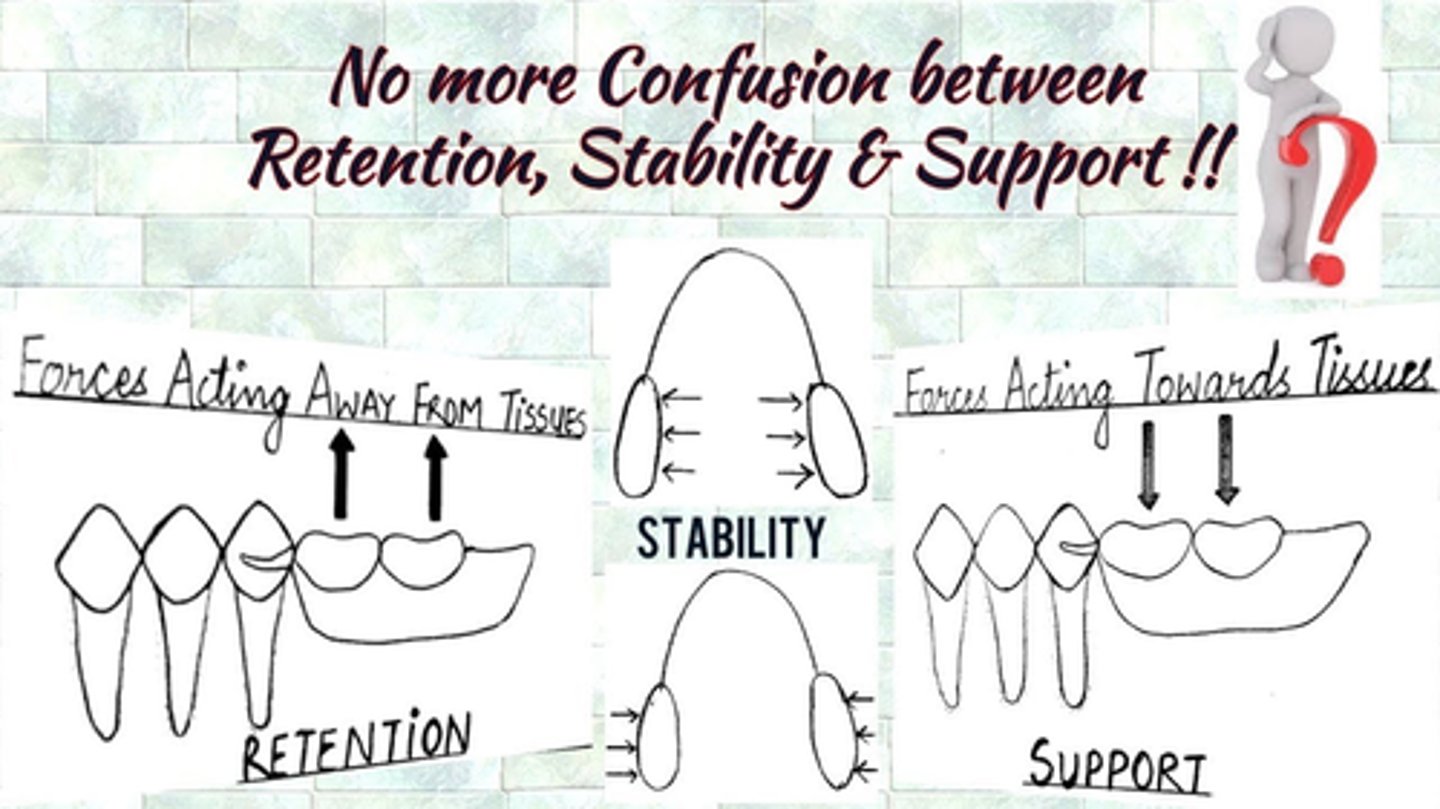
Retention
Stability
Support
Retention
- the quality of the denture to resist displacement along the path of insertion
- Resistance to vertical displacement of the denture away from the denture bearing surface (tissues) during function.
Stability
- quality of the denture to resist dislodgement due to lateral movement during function
Support
- quality of denture to resist the displacement toward the tissue surface
- Resistance to vertical forces of occlusion
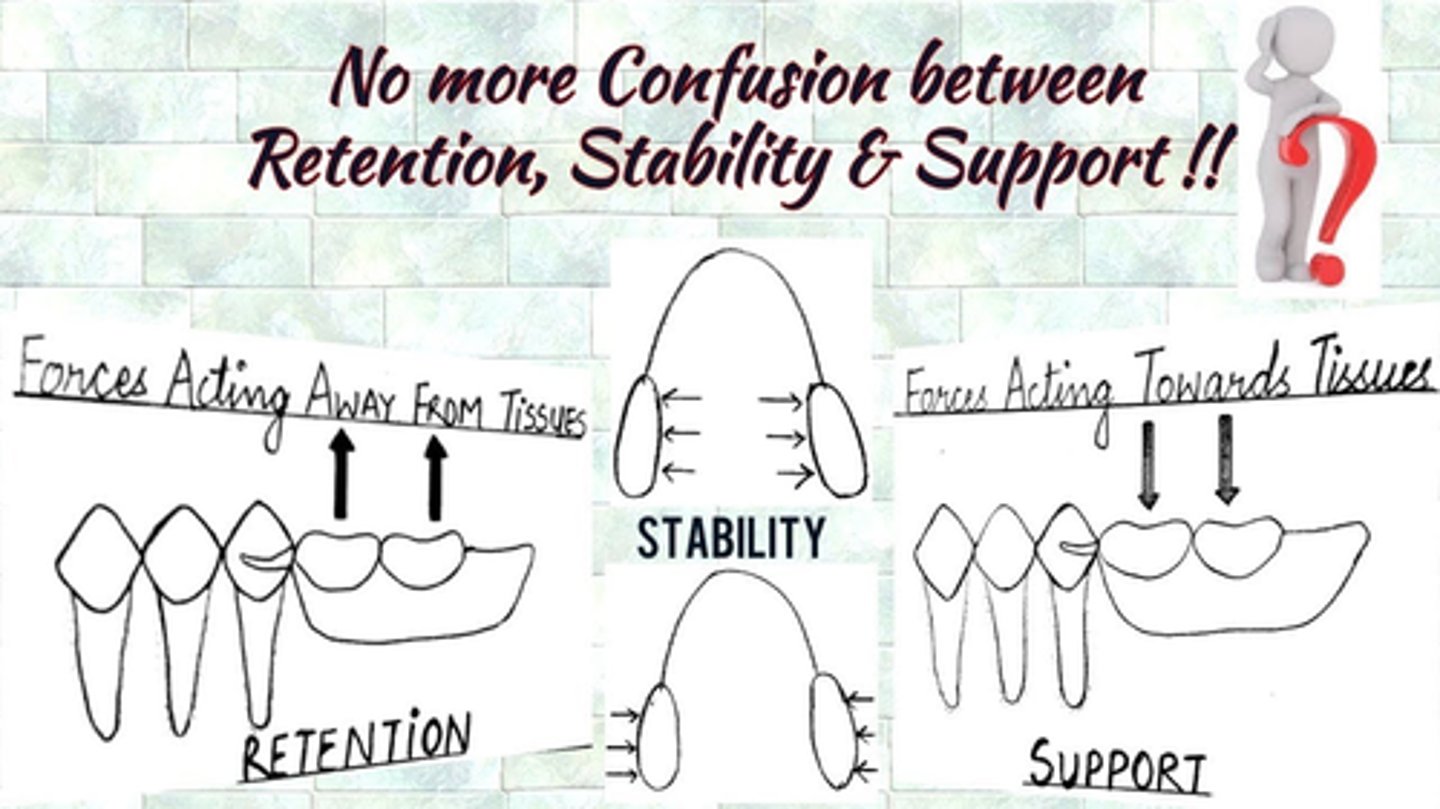
Prosth:
Retention
Stability
Support
Retention
- the quality of the denture to resist displacement along the path of insertion
- Resistance to vertical displacement of the denture away from the denture bearing surface (tissues) during function.
Stability
- quality of the denture to resist dislodgement due to lateral movement during function
Support
- quality of denture to resist the displacement toward the tissue surface
- Resistance to vertical forces of occlusion
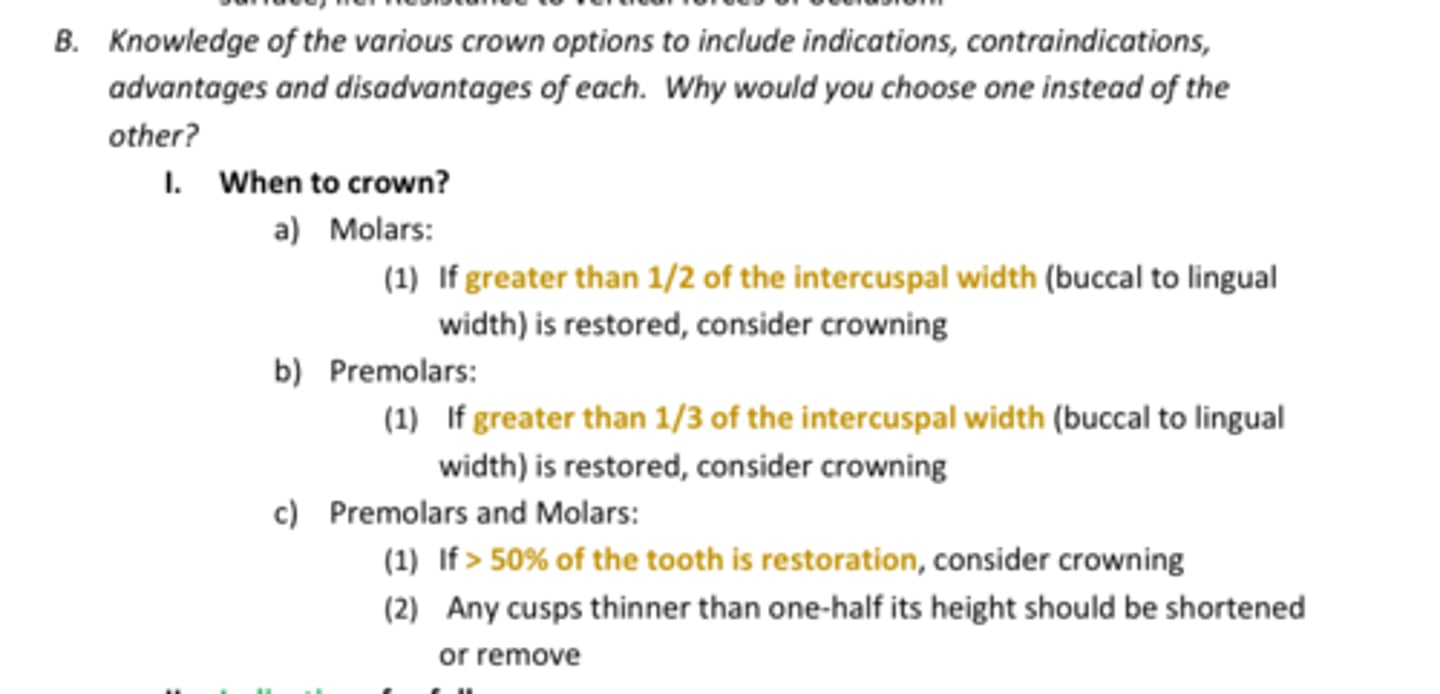
1/2
When to crown?
Molars:(1) If greater than _____ of the intercuspal width (buccal to lingual width) is restored, consider crowning
- REVIEW photo for rest
REVIEW DENTAL ANATOMY BASICS:
- Slides 116-120
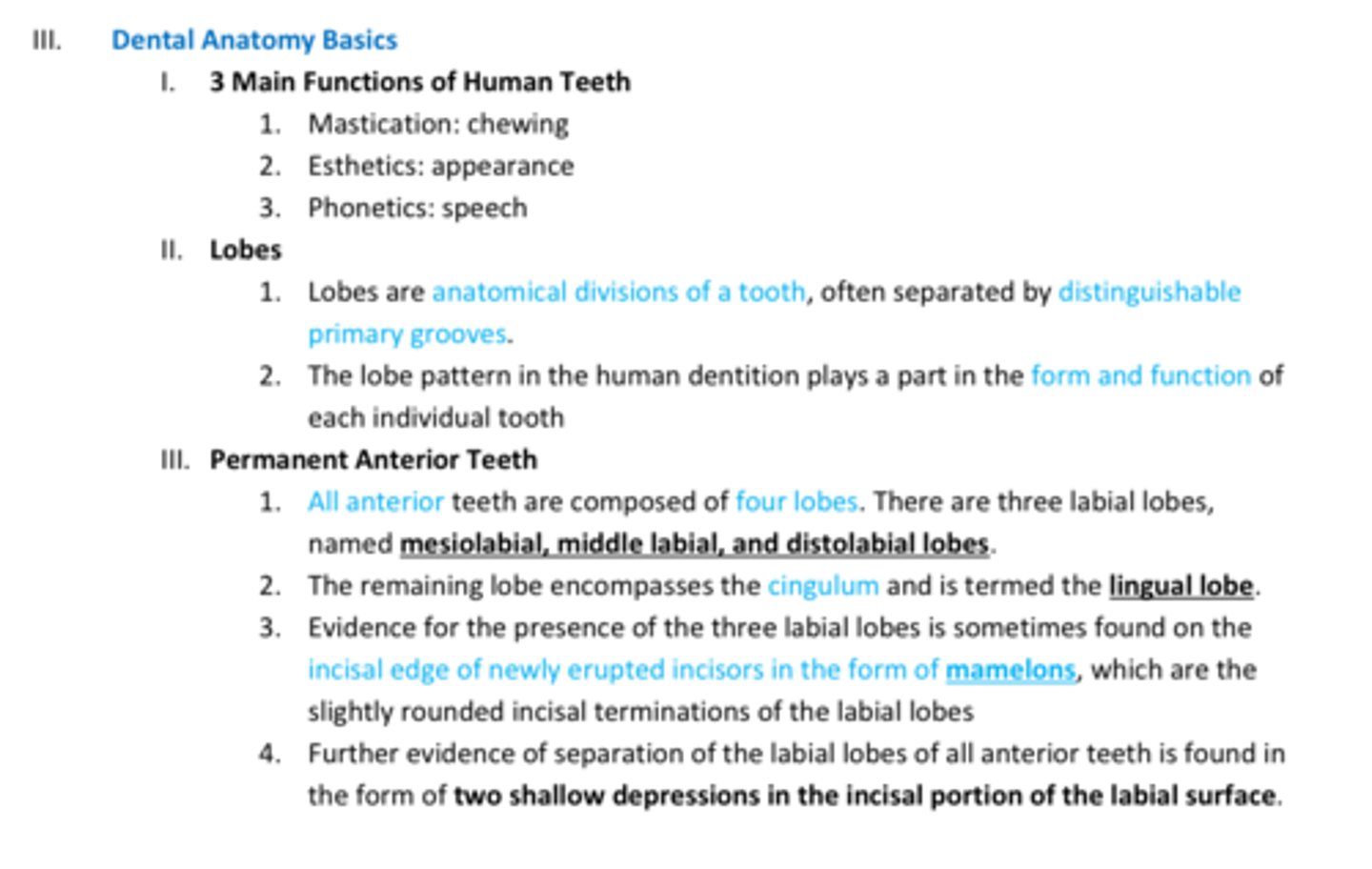
4
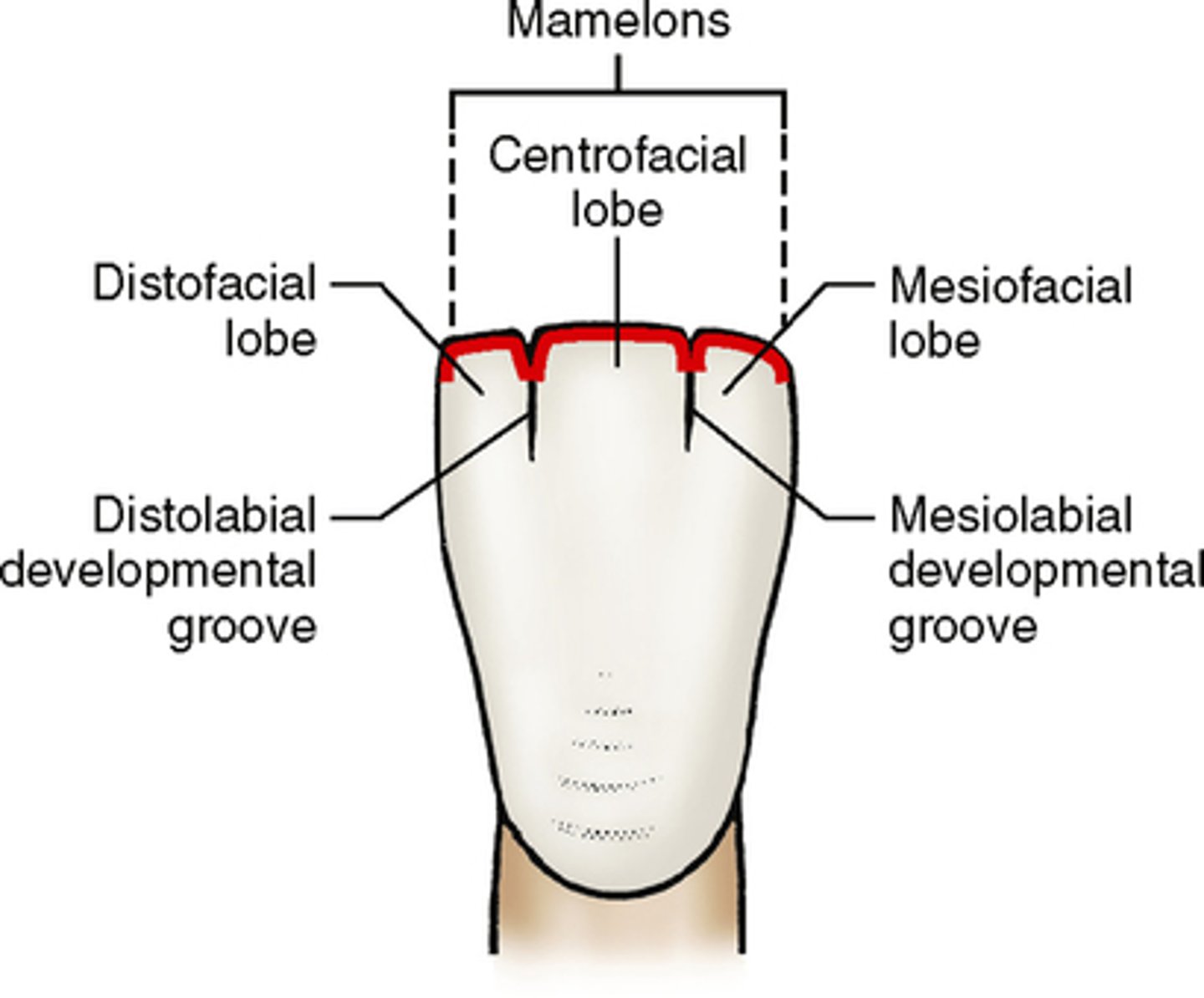
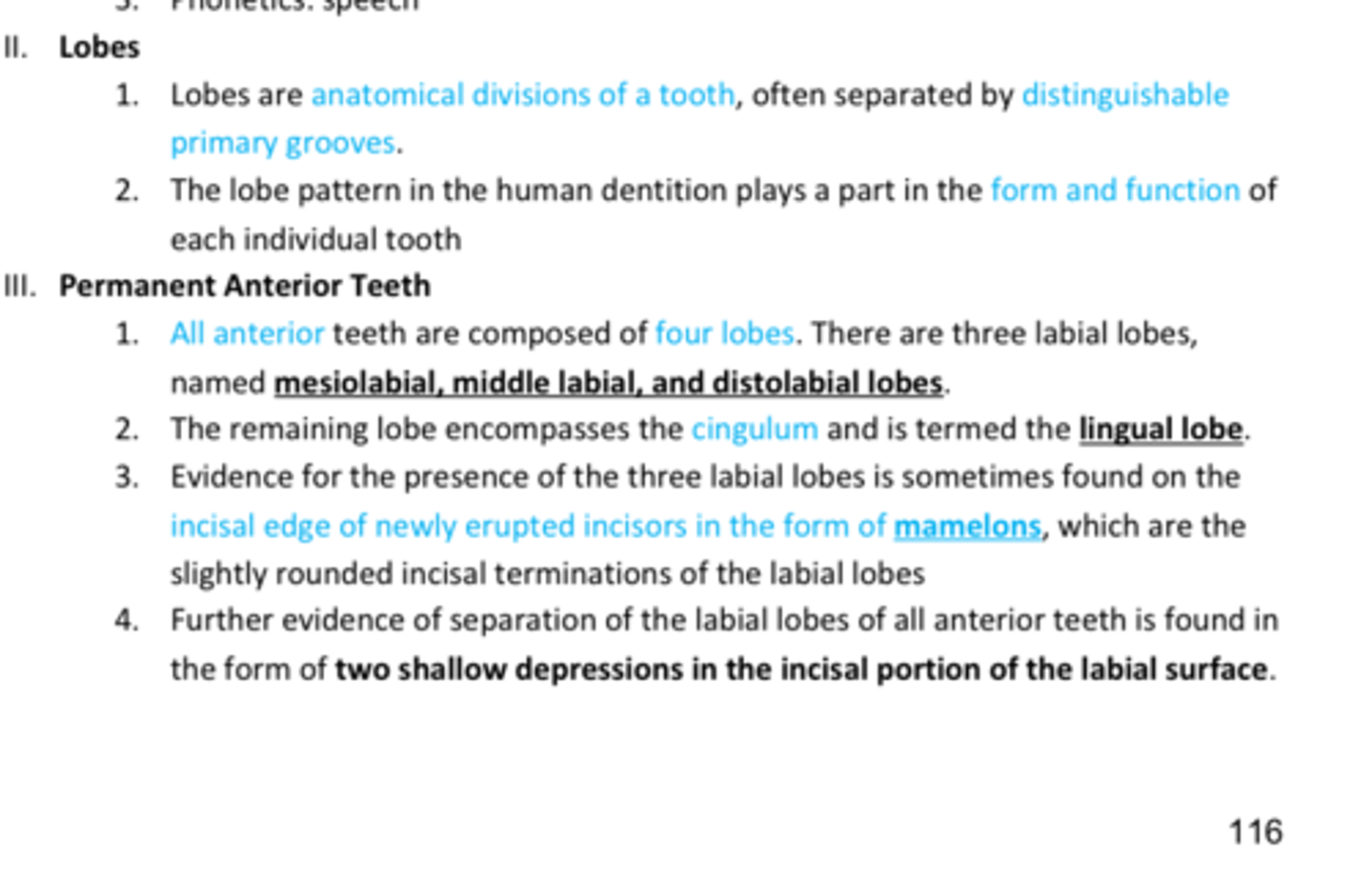
Anterior teeth are composed of ____ Lobes
- named mesiolabial, middle labial, and distolabial lobes.
REVIEW DENTAL ANATOMY BASICS:
- Slides 116-120
REVIEW DENTAL ANATOMY BASICS:
- Slides 116-120
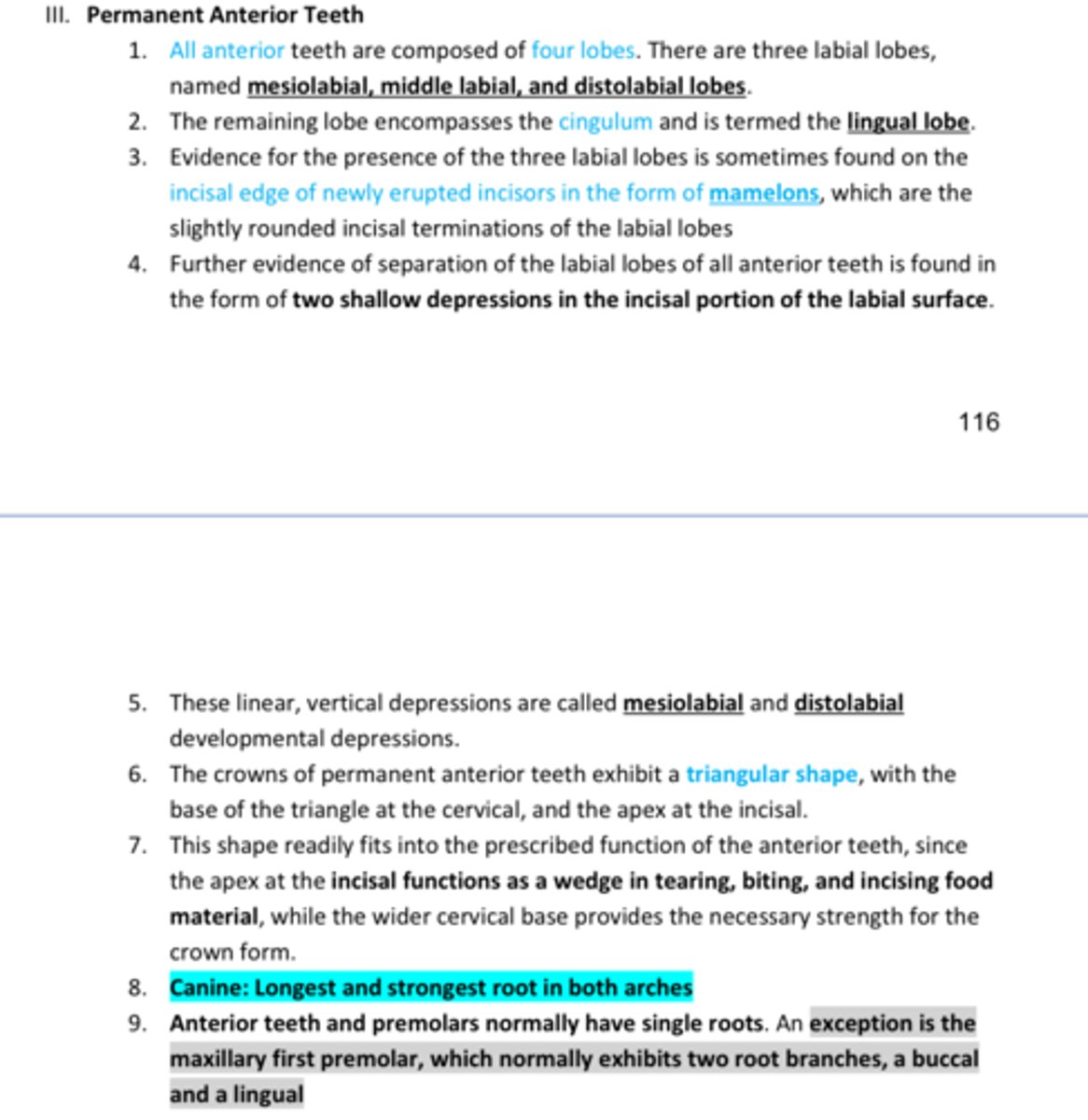
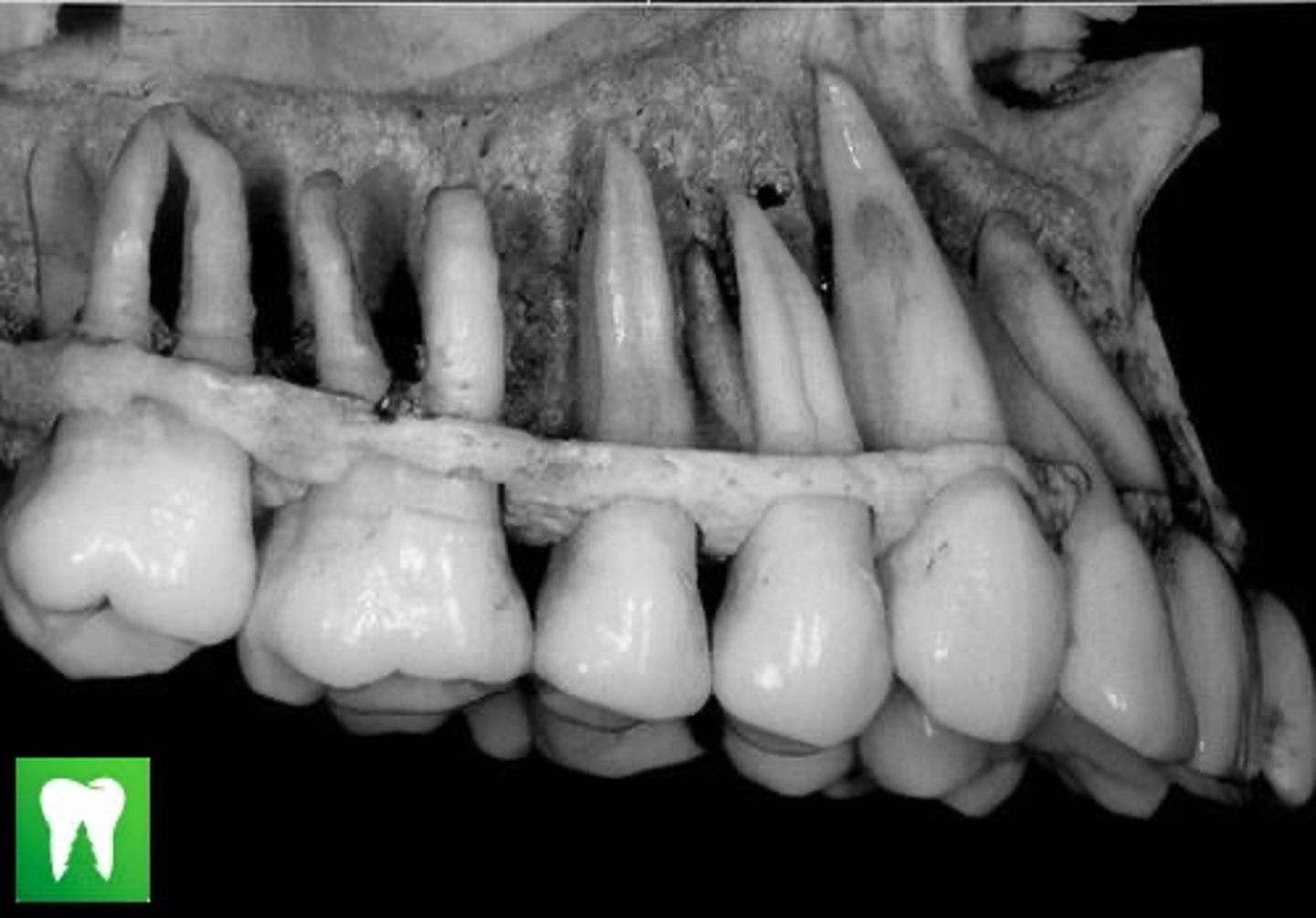
Canine
Longest and strongest root in both arches
Maxillary 1st Premolar
Anterior teeth and premolars normally have single roots.
An EXCEPTION is the ____ ____ ____ which normally has 2 roots: B & L root branches
4
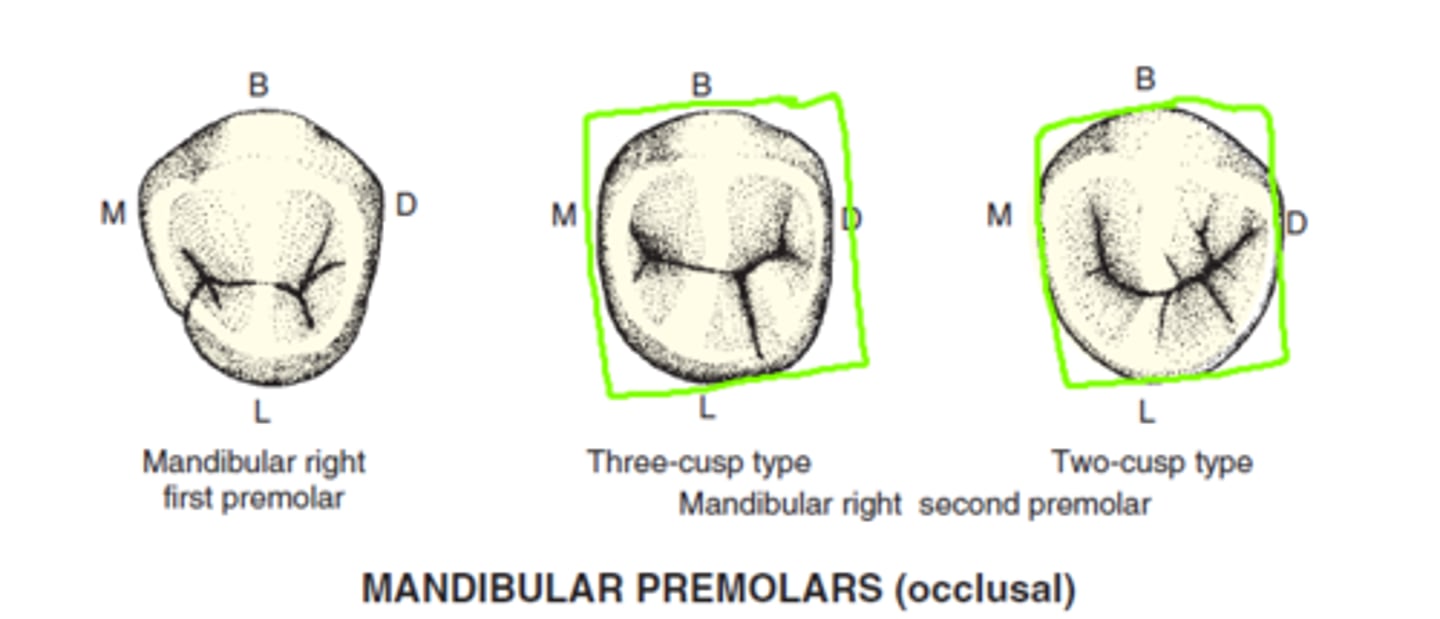
Mandibular 2nd Premolar
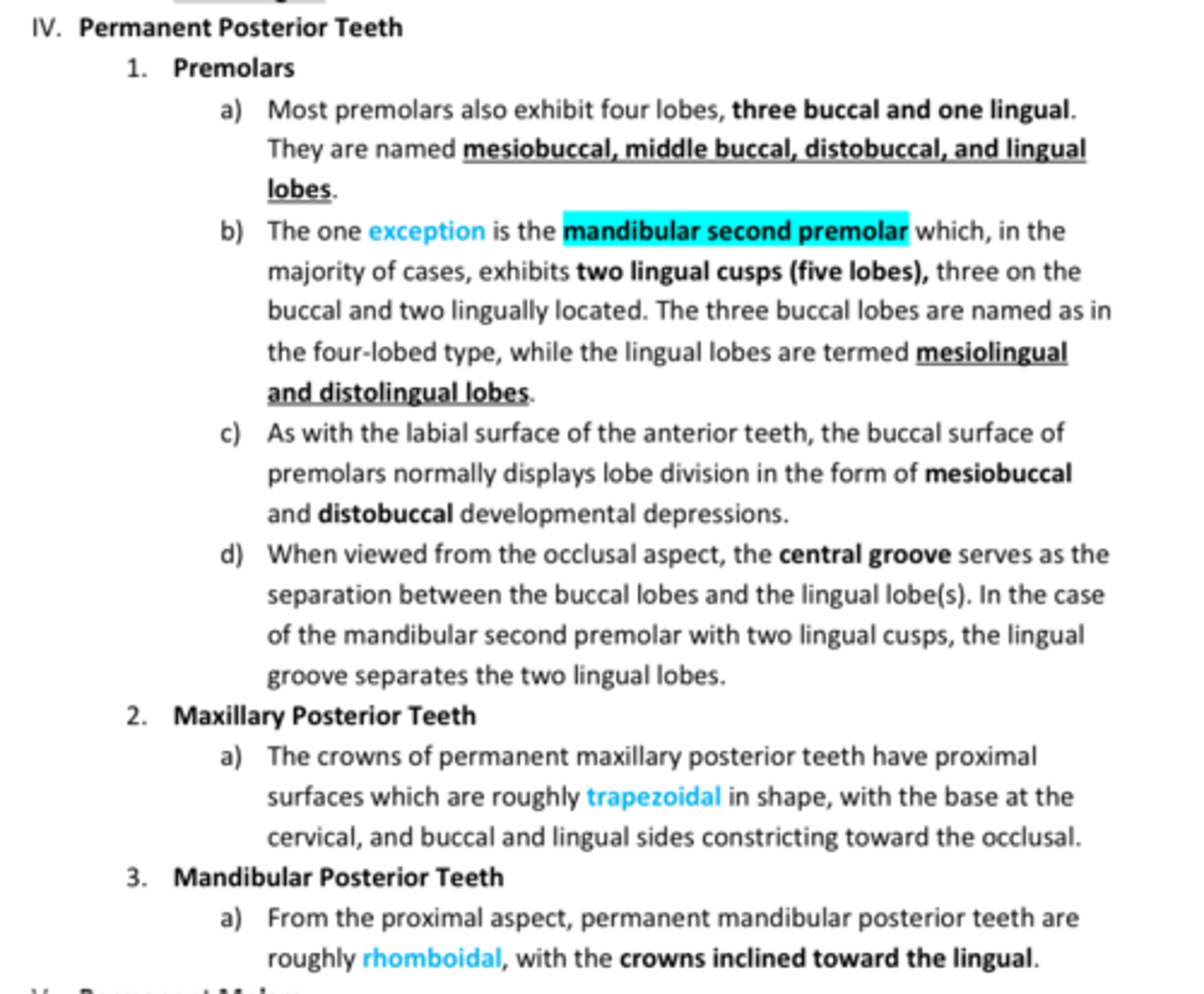
Most Premolars have ____ lobes.
Named: mesiobuccal, middle buccal, distobuccal, and lingual lobes.
The EXCEPTION is the ____ ___ ____ bc it has TWO lingual cusps= 5 lobes
REVIEW DENTAL ANATOMY BASICS:
- Slides 116-120
True
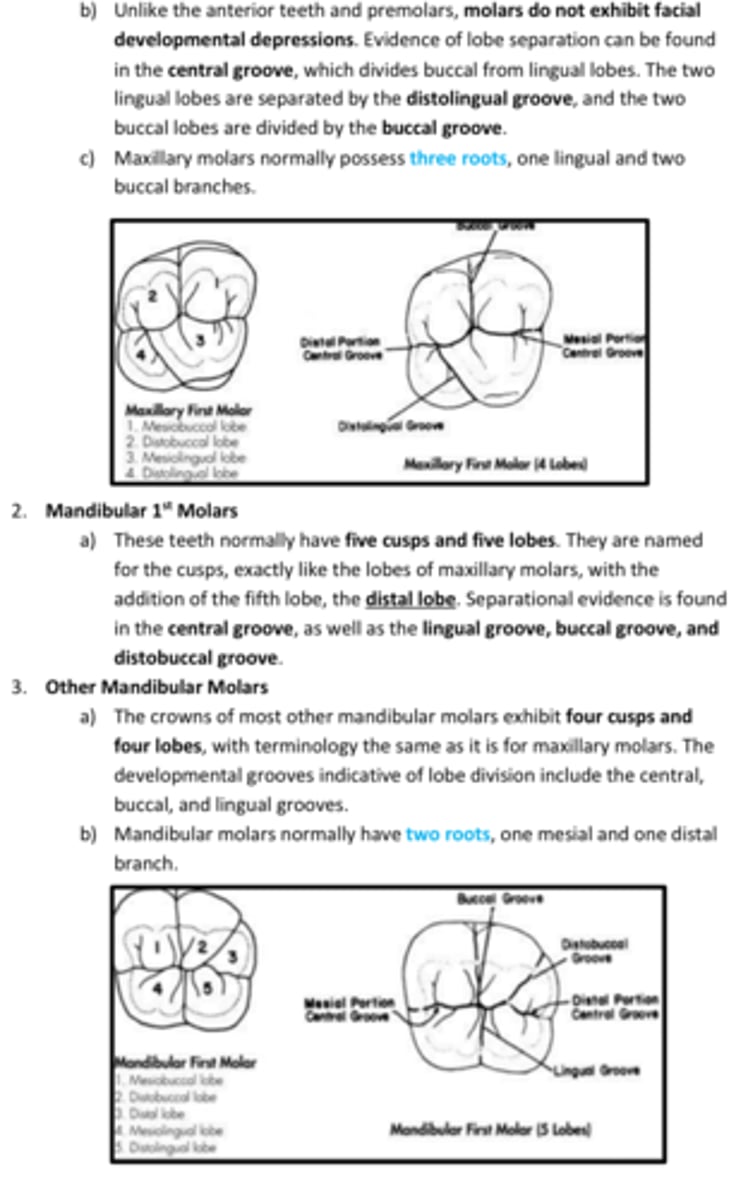
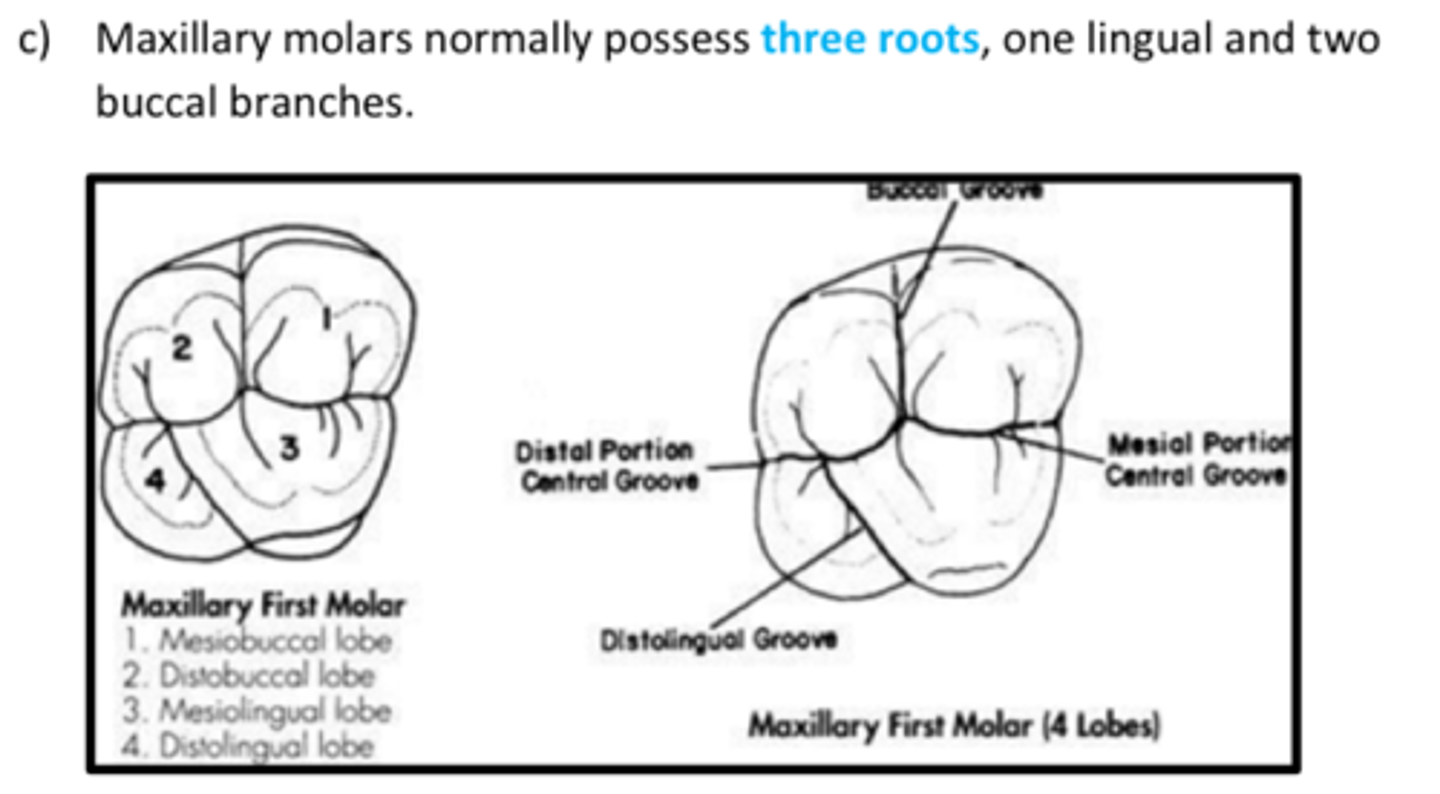
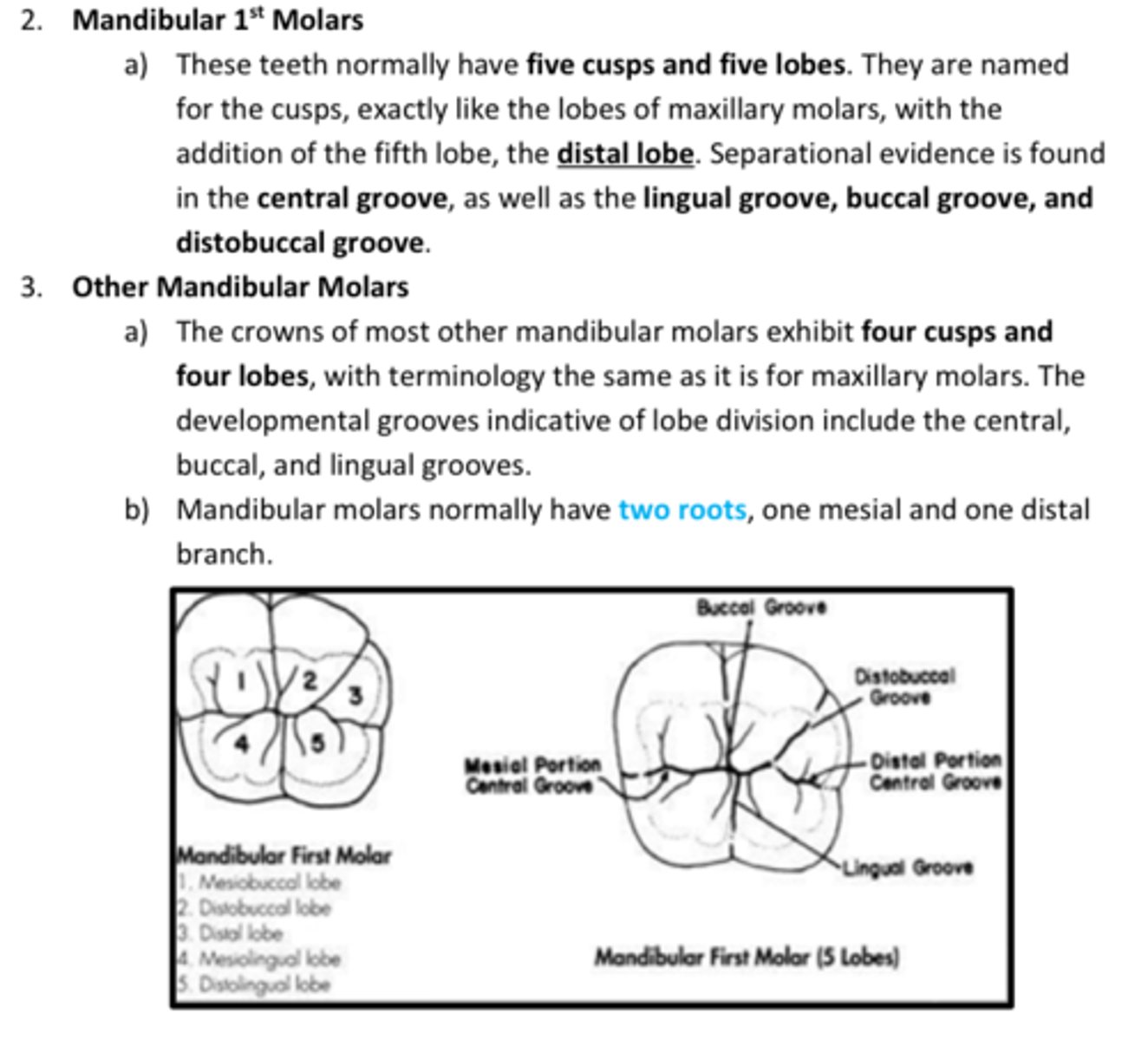
T/F: Unlike the anterior teeth and premolars, molars do not exhibit facial developmental depressions. Evidence of lobe separation can be found in the central groove, which divides buccal from lingual lobes. The two lingual lobes are separated by the distolingual groove, and the two buccal lobes are divided by the buccal groove.
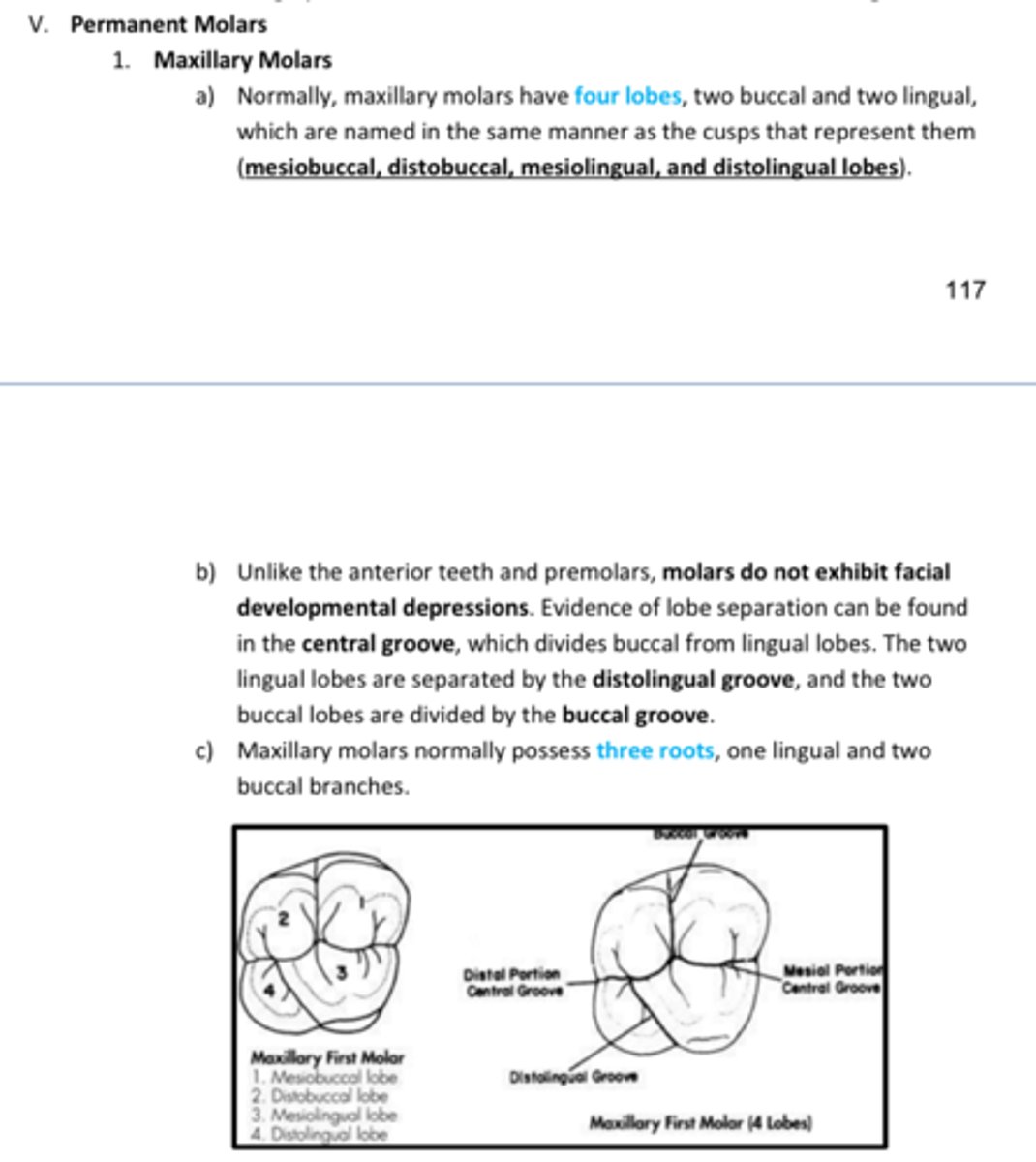
3
2
Max molars have ___ roots
Mand molars have ____ roots
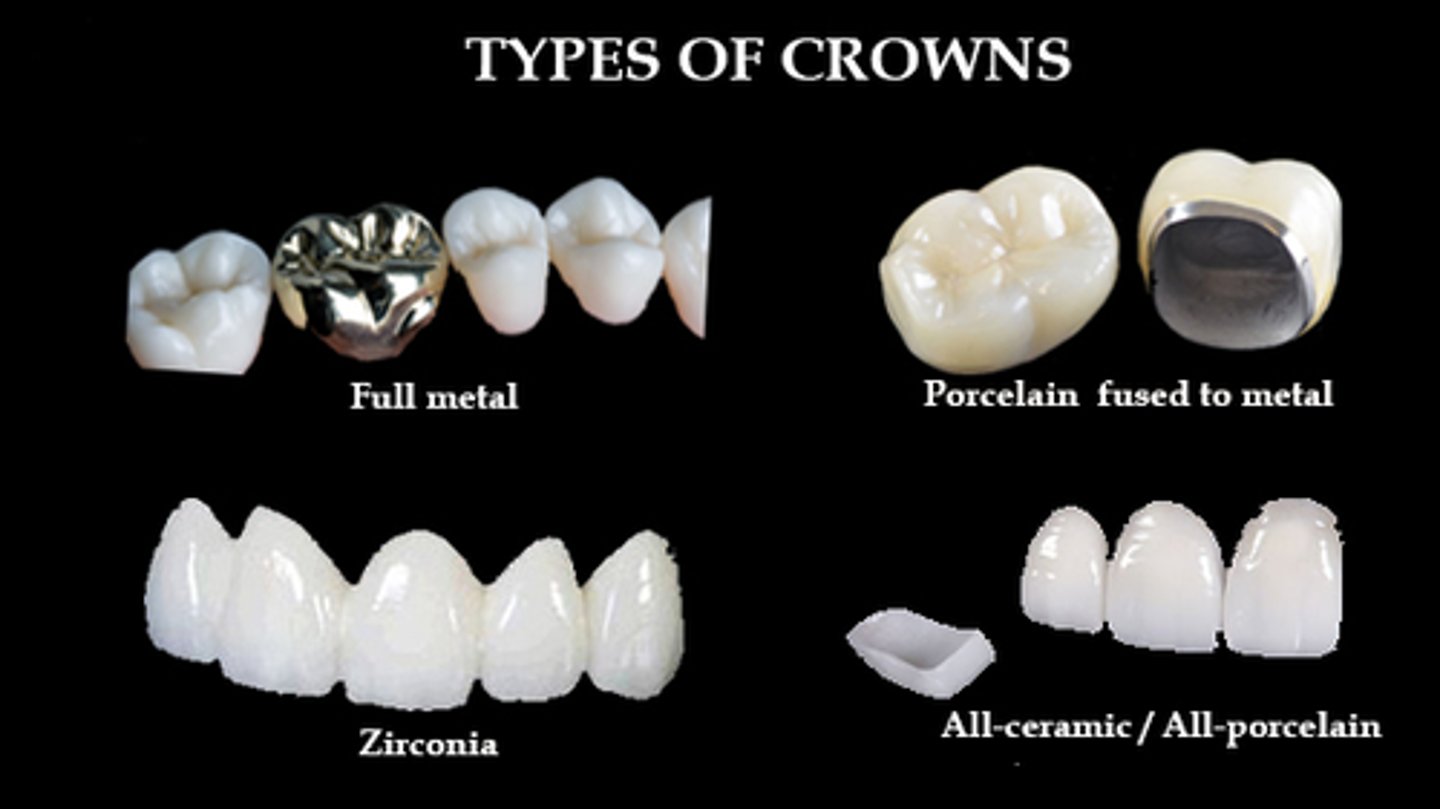
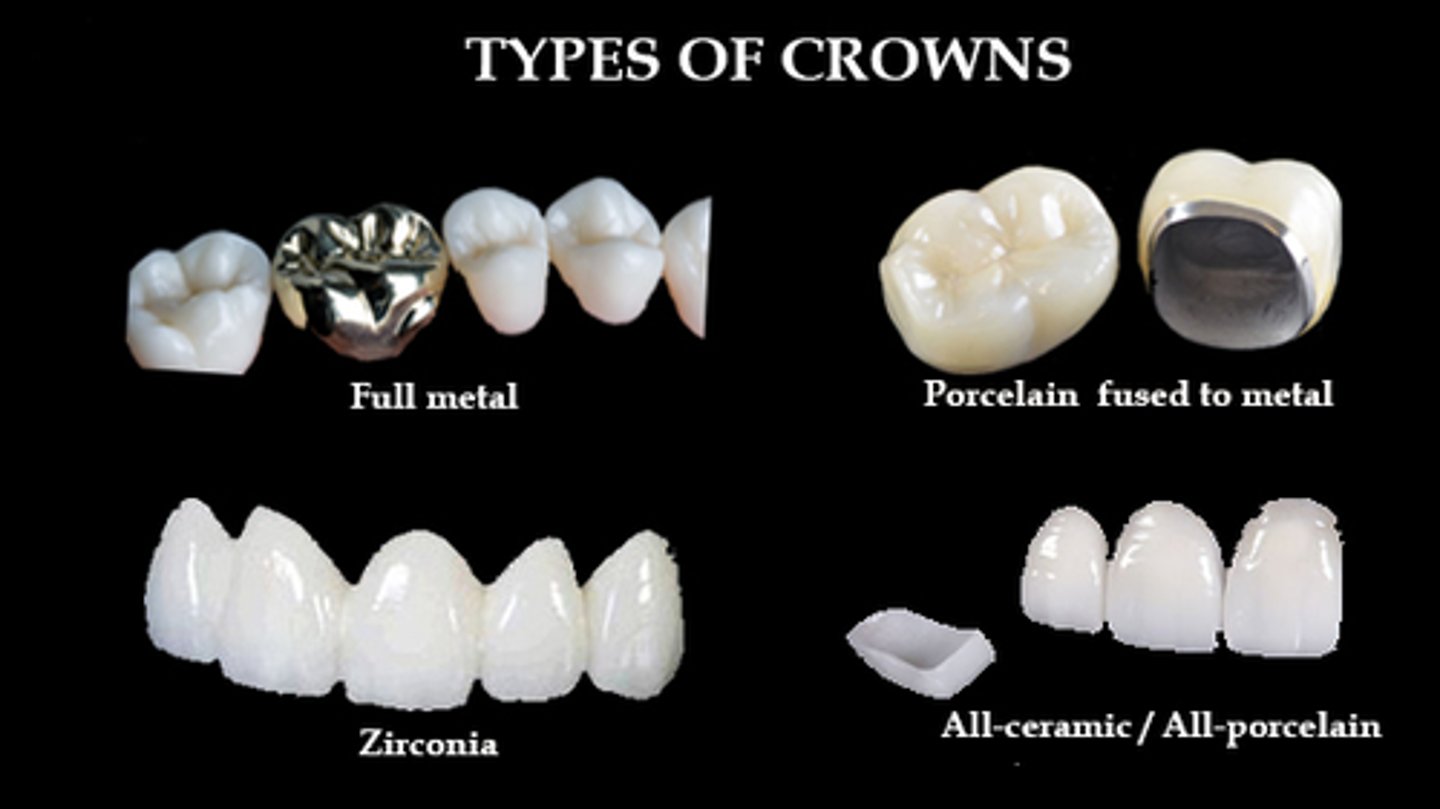
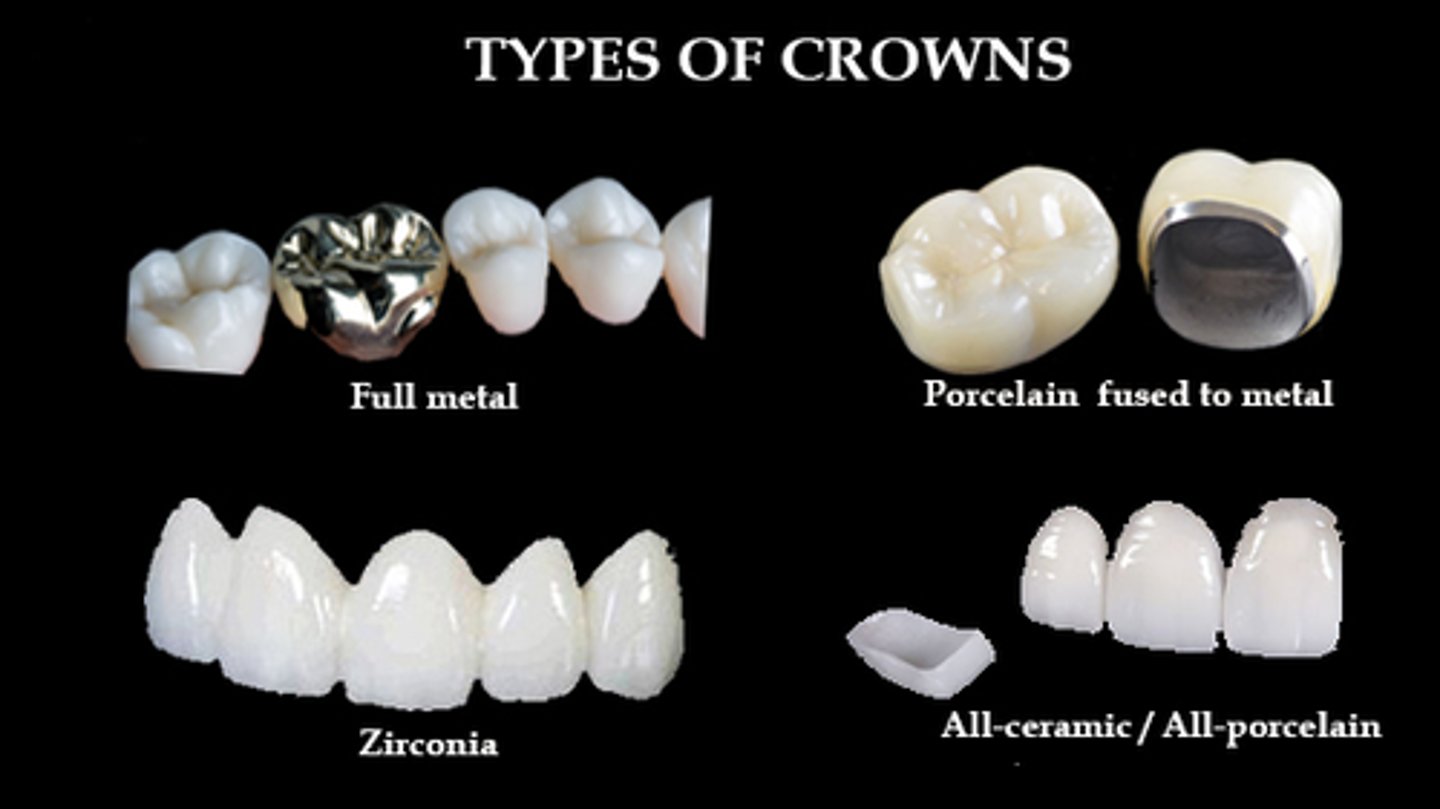
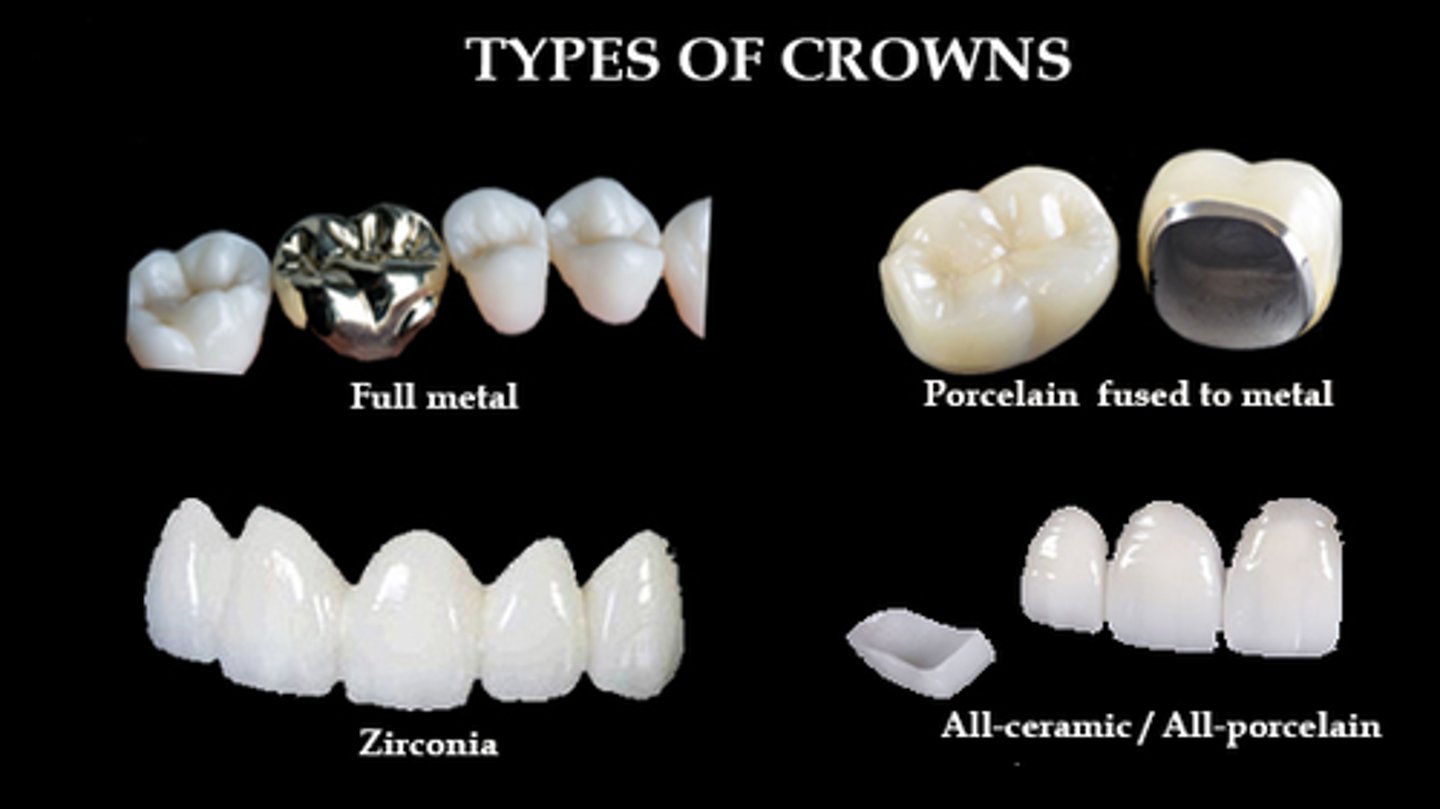
Crowns
These are the 3 types of ____
Full Metal Crowns
- Full gold crowns
- Full silver crowns
PFM Crowns
- Zirconia fused metal crown
- Porcelain fused metal crown
ALL Ceramic Crowns
- Zirconia crowns
- Feldspathic crowns
- Lithium Discilicate (E.Max) crowns
- Zirconia crowns
- Feldspathic crowns
- Lithium Discilicate (E.Max) crowns
List 3 types of All Ceramic Crowns
Full metal crown
What type of crown:
Indications:
- extensive coronal destruction by caries or trauma
- to support a partial removal dental prosthesis
- Endodontically Tx teeth
Contraindications:
- if a more conservative approach can be used
- high esthetics
- active caries/perio disease
Advantages:
- BEST retention
- BEST resistance
- BEST strength
Disadvantages:
- not esthetic
- adverse effect on pulp & periodontium
- cannot perform EPT on vital tooth
**Type of Preparation:**
CHAMFER bur all the way around
- Axially= 0.8-1mm
- Occlusally/Incisial= 1-1.5mm
Cement:
- Anything EXCEPT Light cure resin
- RelyX Unicem or RelyX Luting Plus

Full metal Crown
What type of crown:
Indications:
- extensive coronal destruction by caries or trauma
- to support a partial removal dental prosthesis
- Endodontically Tx teeth
Advantages:
- BEST retention
- BEST resistance
- BEST strength

Full metal crown
What type of crown:
Indications:
- extensive coronal destruction by caries or trauma
- to support a partial removal dental prosthesis
- Endodontically Tx teeth
Contraindications:
- if a more conservative approach can be used
- high esthetics
- active caries/perio disease
Advantages:
- BEST retention
- BEST resistance
- BEST strength
Disadvantages:
- not esthetic
- adverse effect on pulp & periodontium
- cannot perform EPT on vital tooth
Full metal crown
**Type of Preparation:**
CHAMFER bur all the way around
- Axially= 0.8-1mm
- Occlusally/Incisial= 1-1.5mm
Cement:
- Anything EXCEPT Light cure resin
- RelyX Unicem or RelyX Luting Plus