Week 9: Musculoskeletal System and Conditions (Ch 30)
1/123
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
124 Terms
Fracture
break or disruption in continuity of bone
complete fracture
bone is divided into two distinct sections
incomplete fracture
bone not broken into two sections, break is only through of the bone
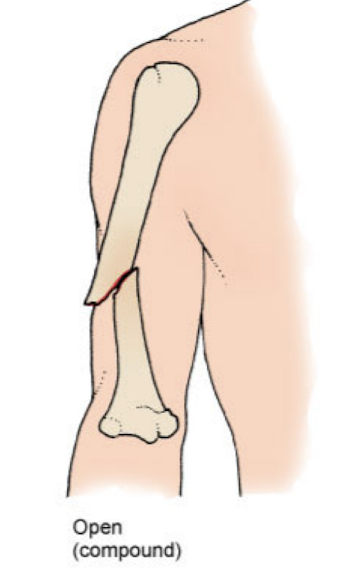
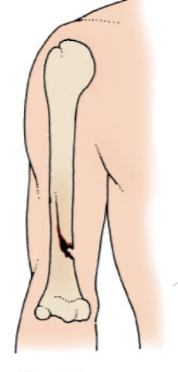
open/compound fracture
skin surface over the broken bone is compromised
infection risk
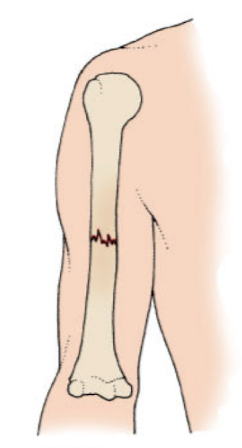
closed/simple fracture
does not extend through the skin, no visible wound
pathological/spontaneous fracture
minimal or no trauma
weak bones from disease (osteopenia/cancer)
fatigue/stress fracture
repetitive excessive stress on a bone
seen with athletes
compression fracture
force on long axis of bone
seen in vertebrae in pt w osteoporosis
comminuted fracture
bone shattered

Displaced fracture
bone fragments are separated and not aligned.

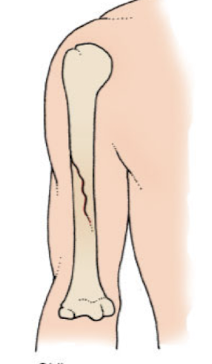
oblique fracture
A fracture that occurs at an angle across the bone, typically due to a sharp angle of force
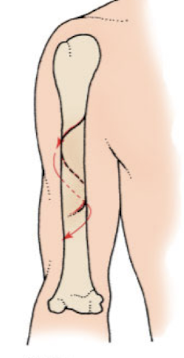
spiral fracture
A type of fracture that occurs when a twisting force is applied to the bone, resulting in a ragged break that encircles the bone.
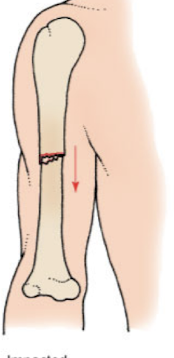
impacted fracture
A fracture where one bone fragment is driven into another, often due to compressive forces.
greenstick fracture
seen in children
bone bends and partially breaks (break not through)
acute complications of fractures (6)
vte, infection, acute compartment syndrome, crush syndrome, hemorrhage/hypovolemic shock, fat embolism syndrome
acute compartment syndrome
a broken bone impacts muscle, swelling increases pressure, decreasing ciruclation to area, crushing nerves potenailly leading to necrosis
severe pain
what is the first intervention to acute compartment syndrome? other interventions/treatment?
elevate limb to return blood flow
call doctor to perform a fasciotomy (scalpel to release pressure)
crush syndrome
broken bone damages BV resulting in severe bleeding, inc pressure, hemorrhage
fat embolism syndrome
inside bones contain fat globules
a fracture releasees these into circulation
may get stuck resulting in a PE or stroke
chronic complications of fractures- complex regional pain syndrome
dysfunction of the CNS/PNS that leads to severe, persistent pain
results from fractures or other traumatic ms injury and commonly occurs in the feet and hands
avascular necrosis
death of bone tissue from decreased bf
health promotion and matinence of fractures (4)
osteoporosis screening= dexiscan
fall prevention, home safety
dangers of drinking/driving
helmets, seatbelts
history assessment of fractures (3)
determine cause, events leading up to injury
substance use (opioids)
occupational/recreational activities
physical/psychosocial assessment of fractures (4)
check for trauma to other body systems (distractor), assess all body systems
check urine for blood
swelling, skin color, peripheral pulses
coping, support, accessibility of house
physical assessment- imaging for fractures
x rays- where fracture is
CT- for complex areas like hip/pelvis/spine
MRI- soft tissue injuries
labratory assessment of fractures
hbg/hct (low if bleeding)
ESR- nonspecific inflammation marker (high)
WBC- high with bone/skin inf
serum Ca2+ and phosphorus- high as broken pieces of bone are reabsorbed into blood
analyze cues for fractures (4)
acute pain, muscle spasms, edema/swelling
decreased mobility
potentional for neurovascular comp, impaired perfusion
potentional to inf due to wound firom open fracture
interventions for fractures (2 actions, 2 steps to prevent)
managing acute pain
increase mobility
prevent/monitor neurovacular compromise (swelling—> check cap refill, temp, pulse)
prevent infections (open fracture, cover w sterile dressing and antibiotis)

closed reduction devices- action, use, duration
immobilize bone to heal in partial breaks
wear 24 hours a day, remove to shower
typivally used for 6 wks
closed reduction devices- fiberglass synthetic cast
full break
placed in ER, doc office, OR
immonilize bone to heal
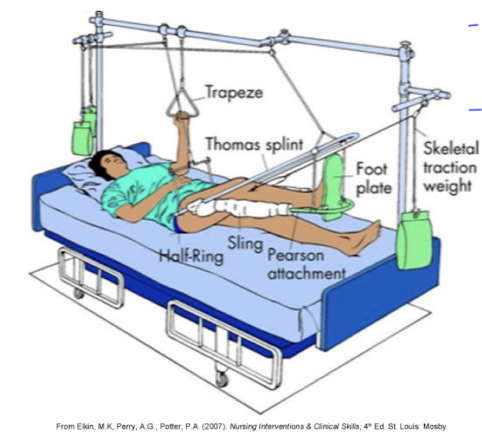
skeletal traction- for? action? result?
hip or femur fracture
pulling force to a part of the body
allow alignment
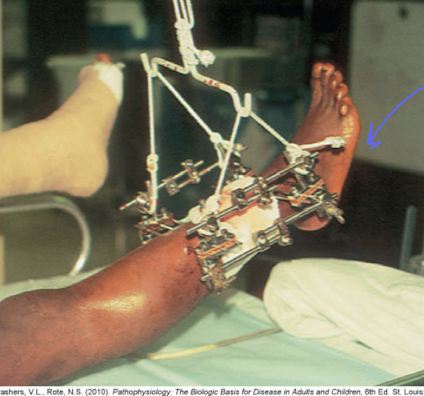
fixation devices (2)
operative procedure
internal- open reduction, metal pins/screws/rods/plates/prosthetic inside body
external- closed reduction, when pt have soft tissue injury (open fracture), pins/wires thru skin/bone, then connected to an external frame to stabilize, care w iodine at site
preventing/monitoring neurovascular compromise (fractures)
perform neurovascular assessments
be aware of s/s of acute compartment syndrome
6 P’s
6 P’s of fractures
pain
pressure (skin taight)
paralysis
paresthesia
pallor
pulselessness
preventing infection of fractures
use aspetic technique for dressing changes/wound irrigation
monitor vs, wound appearance/drainage
notify provider if inflammation, purulent drainage noted
pt may need antibiotics, VAC system
care coordination/transition management for fractures
home care- stairs, driving, bathroom access, scatter rugs, shower tub
self management education- verbal/written instructions, wound care, recognize s/s, nutrition, follow up care
health care resources- home health nurse
evaluation of fractures
adequate pain control 2-3 on 0-10 scale
free inf
adequate bf
free of conseuqnces of dec mobility
osteoporosis definition
chronic disease of cellular regulation
osteoporosis patho (3)
bone loss= decreased density (fracture risk), fragility fracture from osteoporosis (women over >50 from dec estrogen)
decreased BMD (bone mineral density)
loss in height (as much as 6 in)
osteomalacia
soft bones from lack of vit d
osteopenia
loss of bone mass
dowager’s hump
abnormal curvature of the spine resulting from osteoporosis, leading to a stooped posture
osteoporosis etiology (2)
genetic, lifestyle, environmental factors (non modifiable)
nutrition- lack of calcium and vit d, protein deficiency
osteoporosis health promotion/disease prevention (5)
teach women appropriate health/lifestyle practices
remind men >50 and menopause women of hearly t score screening
nutrition- vit d
stop smoking, acoid alcohol, limit carbonated beverafes
lose weight, exercise (weight bearing)
what foods should people with osteoporosis eat? what major factor contributes?
dairy, leafy green veggies, sun exposure
osteoporosis physicsal/psychosocial assessment (3)
kyphosis/dowager’s hump
bone density tests, fracture history
psychosocial- body image
osteoporosis laboratory assessment
serum calcium and vit d3
osteoporosis imaging assessment
x rays of spine/long bones
DXA scan= T score
QCT scan
vertebral imaging
MRI
DXA Scan- bone mineral density T Score of +1 to -1
normal bone density
DXA Scan- bone mineral density T Score of -1 to -2.5
osteopenia
DXA Scan- bone mineral density T Score of more than -2.5
osteoporosis
what can combat the effects of decalcification of bone?
exercise, calcium, meds
osteoporosis interventions (3)
nutrition therapy- fruits, veggies, low fat, high dairy, low caffiene
lifestyle changes- resistance/cardio
drug- biphosphonates, calcium (4,000/day max), vit d
biphosphonates- exemplar, action, pt teaching
alendronate
slow bone resorption
take on empty stomach in AM w full glass of water (8oz) once a week
take before at least 30 minutes before the first food and remain upright
osteoporosis evaluation
follow up w DXA screening
makes lifestyle changes
no bone fragility fracture
osteomalacia
soft bones because of vit d deficiency
osteomyelitis- define, types
infection in bony tissue caused by bacteria, virus, fungi
exogenous (open fracture/surgery), endogenous (inf in blood)
osteomyelitis physical s/s
bone pain, fever
erythema and heat in area of inf bone
osteomyelitis labs
elevated wbc
ESR may elevate later in disease
osteomyelitis chronic s/s
foot ulcers w localized pain
osteomyelitis nonsurgical management
meds
iv antibiotics
pain meds
antipyretics
osteomyelitis surgical management
debriedment w antibiotics
IND (incision/drainage)
osteoarthritis- note, define, sign
most common arthritis
joint pain and loss of function characterized by progressive deterioration and loss of cartilage
osteophytes
osteophytes
bone spurs that form in response to cartilage degeneration or osteoarthritis
cause pain, reduced mobility, and nerve compression
osteoarthritis patho
cartilage degenerates, bone/cartilage float into joint= crepitis
osteoarthritis primary and secondary risks
primary- aging and genetics
secondary- joint injury, obesity, repetitive stress to joints
what are the most common joints affected by osteoarthritis?
hips, knees, vertebrae, hands
osteoarthiris health promotion
proper nutrition (prevent obestyi)
avoid injury
take work breaks
stay active
osteoarthritis history assessment
localized, unilateral joint pain
secondary to diagnosis
older than 60 yrs
osteoarthritis physical assessment/s/s
persistent join pain/stiffness
crepitus
joint effusions
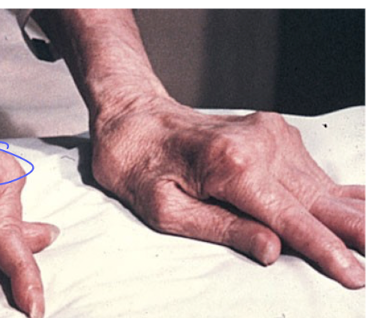
heberden’s nodes/bouchard’s nodes
atrophy of skeletal muscle
psychosocial assessment of osteoarthritis
lifestyle changes
osteoarthritis labs
aspirated join fluid
ESR
hsCRP (non-specific inflammatory marker)
osteoarthritis imaging assessment
xray
mri
heberden’s nodes
distal joint
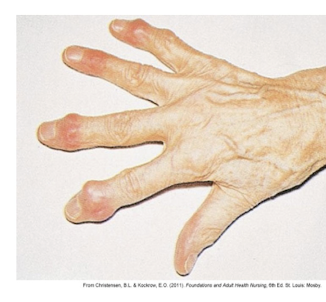
bouchard’s nodes
proximal joint

collaborative problems in pt w osteoarthritis
persistent pain, decreased mobility
osteoarthritis nonsurgical chronic pain management
drugs
rest, immobilization
positioning
thermal (hot/cold)
weight control
integrative therapies- glucosamine, chondroitin
how do heat/cold therapies work
heat vasodilates, inc bf
cold decreases inflam by constricting bv
what drugs can be used for nonsurgical pain management of osteoarthritis?
NSAIDS (advil/ibupro)
acetaminophen (tylenol)
opioids
dyclophenic 1% topical gel (volteran)
surgical management of osteoarthritis
total joint arthroplasty (TJA) / total joint replacement (TJR)
arthroscopy (hole, clean area/remove filling/cartilage)
post op care for TJR
prevent comp
hip dislocation, use abductor pillow
VTE (ambulation), inf
anemia (estimated blood loss), s/s
neurovascular= circ, motor, sensation
hip flexion after total hip replacement
do not flex hips more than 90 degrees


continuous passive motion machine for total knee replacement
constantly bends knee to prevent scar tissue build up, promote ROM
osteoarthritis care coordination/transition management
home care management= environmental safety
self management/education= well balanced diet
health care resources= PT at home, home care nurse
osteoarthritis outcomes
pain 2-3 or level that is acceptable
no complications from total joint arthroplasty
moves/functions in own environment independently w/w out assistive devices
rheumatoid arthritis definition
common ct disease causing destruction to joints
chronic, progressive systemic inflammatory autoimmune disease that primarily impacts synovial joints
remissions and exacerbations
rheumatoid arthritis patho
transformed autoantibodies (rheumatoid factors) form, attack healthy tissue causing infammation
rheumatoid arthritis etiology/genetic risk
combo of environment and genetics
physical/emotional stresses linked to exacerbations
rheumatoid arthritis incidence/prevalence
euro-american caucasians
young-middle aged women 2-3 times more likely than men
rheumatoid arthritis history assessment of symptom stypes
acute/severe, slow and progressive
rheumatoid arthritis general physical assessment
joint and systemic symptoms
generalized weakness and fatigue
morning stiffness
psychosocial assessment
rheumatoid arthritis labs
rheumatoid factor
anti-ccp
ana
esr
hsCRP
serum complement (c3 and c4) (plt ct)
thrombocytosis can occur w late RA
rheumatoid arthritis early signs
joint stiffness
swelling, pain
fatigue, generalized weakness
low grade fvr
rheumatoid arthritis late signs
joints become progessivley inflamed and painful
SQ nodules
rheumatoid arthritis interventions- main goal, 3 things
managing chronic inflammation/pain
drug therapy
promoting mobility
enhancing self esteem
rheumatoid arthritis systemic complications (6)
wt loss, extreme fatigue
exaverbations
sub q nodules
res/cardiac comp
vasculitis (inflamm of bv)
paresthesias, neuropathy
rheumatoid arthritis non pharm interventions
adequate rest, positioning
ice/heat
plasmapheresis (not common)
complementary/alt therapies (hypnosis/acupuncture)
promote self-management, enhance body image
manage fatigue
rheumatoid arthritis drug therapy
DMARs (disease modifying antirheumatic drugs)- methotrexate, hydroxychloroquine
BRMs- biological response modifiers
NSAIDS
glucocorticoids
immunesupressive agents (prednisone)
gout/gouty arthritis definition/types
urate crystals deposit in joints and other body tissues causing infalm (common in big toe)
primary
secondary- hyperuricemia
gout/gouty arthritis incidence/prevalence
men >50, chronic alc, obesity, thiazide diuretics