KAAP310 EXAM 2 - Respiratory Content
1/58
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
59 Terms
functions of respiratory system
gas exchange, communication, olfaction, acid-base balance, blood pressure regulation, platelet production, blood/lymph flow, blood filtration, expulsion of abdominal contents
conducting zone
consists of passages that serve only for airflow
from nostrils to major bronchioles - walls of passages are too thick for adequate oxygen diffusion from air to blood
respiratory zone
consists of alveoli and other gas exchange regions of distal airway
upper respiratory tract: airway from nose to larynx
lower respiratory tract: trachea through lungs
nasal cavity epithelia
begins with vestibule - stratified squamous
past vestibule, ciliated pseudostratified columnar epithelium with ciliated cells and goblet cells
small area has olfactory epithelia which have immobile cilia
oral cavity epithelia
stratified squamous epithelia (mostly nonkeratinized, but can be keratinized in hard palate and gingiva)
protects against mechanical stress from chewing and food
pharynx epithelia
nasopharynx: pseudostratified columnar epithelium to filter/humidify air
oropharynx and laryngopharynx: stratified squamous epithelium to protect against abrasion
larynx epithelia
above vocal cords: stratified squamous epithelium to protect cords from mechanical stress
below vocal cords: pseudostratified columnar ciliated epithelium to move mucus and debris
trachea epithelia
pseudostratified ciliated columnar with goblet cells to move mucus upward toward pharynx to clear inhaled particles
cell types of alveoli
squamous type I alveolar cells, great type ii cells, and alveolar macrophages (dust cells)
squamous type i cells
cover 95% of surface area and allow for rapid gas diffusion
great type ii cells
cover 5%, round to cuboidal shape
repair alveolar epithelium when squamous cells are damaged
secrete pulmonary surfactant that prevents alveolar/bronchiole collapse when exhaling
alveolar macrophages
wander lumens of alveoli and CT between them and phagocytize dust particles that escape entrapment by mucus
pulmonary blood vessels and alveoli relationship
pulmonary arteries carry deoxygenated blood to lungs - branch extensively and form networks around each alveolus
capillary walls and alverolar walls form respiratory membrane - thin membrane allowing for rapid gas diffusion
structure of respiratory membrane
barrier between alveolar air and blood
squamous alveolar cell, squamous endothelial cell of capillary, and shared basement membrane
diameter of single erythrocyte
actions of respiratory muscles during inspiration
sternocleidomastoid elevates sternum
scalene fix/elevate ribs 1-2
external intercostals elevates ribs 2-12 and widens thoracic cavity
pectoralis minor elevates ribs 3-5
internal intercostals aid in elevating ribs
diaphragm descends and increases depth of thoracic cavity
actions of respiratory muscles during expiration
internal intercostals depress ribs 1-11 and narrows thoracic cavity
diaphragm ascends and reduces depth of thoracic cavity
rectus abdominis depresses lower ribs, pushes diaphragm upwards by compression abdominal organs, assisted by external oblique
brainstem respiratory centers
ventral respiratory group, dorsal respiratory group, pontine respiratory group
ventral respiratory group
primary generator of respiratory system
elongated neural network in medulla
In quiet breathing, the I neuron circuit fires for about 2 seconds at a time to contract muscles to enlarge thoracic cage and cause inspiration - once I neurons stop firing, E neurons begin firing
eupnea
normal respiration, about 12 breaths per minute
dorsal respiratory group
modifies basic respiratory rhythm, extends length of medulla between VRG and canal of brainstem
modulates the VRG's activity by receiving input from several sources (PRG, chemosensitive center in medulla, chemoreceptors in major arteries, stretch/irritant receptors in airways, higher brainstem centers)
pontine respiratory group
receives input from higher brain centers and issues output to DRG and VRG
hastens or delays transition from inspiration to expiration - adapts to circumstances like sleep, exercise, vocalization, or emotional responses
central chemoreceptors
brainstem neurons that respond to changes in pH of CSF
on each side of medulla
ensures stable CO2 level
peripheral chemoreceptors
in carotid and aortic bodies of large arteries that respond to O2, CO2, and pH content
glossopharyngeal (carotid bodies) and vagus (aortic bodies) nerves enter medulla and synapse with DRG neurons
stretch receptors
found in smooth muscle of bronchi, bronchioles, and visceral pleura
respond to inflation of lungs and signal DRG by vagus nerves
excessive inflation triggers the inflation reflex, which strongly inhibits the I neurons and stops inspiration
irritant receptors
nerve endings amid epithelial cells of airway
respond to irritants
transmit signals via vagus to DRG, and DRG returns signals to respiratory and bronchial muscles, resulting in protective reflexes such as bronchoconstriction, shallow breathing, apnea, and coughing
neural pathway for voluntary control of respiration
originates in motor cortex
output neurons send impulses down corticospinal tracts to integrating centers in spinal cord, bypassing brainstem centers
holding one's breath raises CO2 level of blood until breaking point is reached when automatic controls override
relationship between airflow, pressure, and resistance
airflow is directly proportional to pressure difference
airflow is inversely proportional to resistance
how and why do intrapulmonary pressures change relative to atmospheric pressure during inhalation
during inspiration, diaphragm contracts and flattens, increasing volume of lungs which decreases intrapulmonary pressure
because air flows from high to low, pressure difference causes air to flow into lungs (atmospheric pressure - 760 mmHg, intrapulmonary pressure 758 mmHg)
boyle's law
the pressure of gas is inversely proportional to its volume
if lung volume increases, intrapulmonary pressure decreases and vice versa
charles's law
the volume of gas is directly proportional to its absolute temperature
inhaled air is warmed to 37C by the time it reaches the alveoli, and the inhaled volume will expand and contribute to the inflation of the lungs
bronchodilation
widening of bronchi
increases airway diameter -> decreases resistance to airflow -> improves ventilation
triggered by sympathetics such as epinephrine during exercise or stress
bronchoconstriction
narrowing of bronchi
increased airway resistance -> decreased ventilation
triggered by parasympathetics, allergens, irritants
pulmonary compliance
the lung's ability to stretch and expand
high compliance -> lungs inflate easily -> better ventilation
low compliance -> lungs are stiff -> reduced ventilation
can be affected by age, disease, or structural lung tissue damage
alveolar surfactant
lipid-protein mixture produced by type ii alveolar cells that reduce surface tension inside alveoli
prevents alveolar collapse -> increases compliance and reduces work of breathing -> better ventilation
not enough surfactant -> alveoli collapse -> poor ventilation
composition and partial pressures of atmosphere
Nitrogen - 78.6%, 597 mmHg
Oxygen - 20.9%, 159 mmHg
Carbon dioxide - 0.04%, 0.3 mmHg
Water - 0.5%, 3.7 mmHg
total pressure = 760 mmHg
dalton's law
total atmospheric pressure is a sum of the contributions of these individual gasses (partial pressures)
i.e., average atmospheric pressure is 760 and oxygen is 20.9%... 0.209 x 760 = 159 mmHg <- pp of oxygen
alveolar air
lower nitrogen, lower oxygen, higher water, and higher carbon dioxide
alveolar air is humidified, so water is higher
freshly inspired air is combined with leftovers, so oxygen is diluted and CO2 is enriched
alveolar air exchanges O2 and CO2 with blood, so O2 is lower and CO2 is higher
gas exchange and water solubility
air in alveoli is in contact with the film of water covering the alveolar epithelium, so for oxygen to get into the blood, it must dissolve in water and pass through the respiratory membrane
diffusion only works for dissolved substances
four variables determining rate of oxygen loading and carbon dioxide unloading
partial pressure gradients of the gasses, solubility of the gasses, thickness of respiratory membrane, surface area of respiratory membrane
partial pressure gradients of the gasses
O2: higher pp in alveoli (100mmHg) vs lower in capillaries (40 mmHg) so O2 diffuses into the blood
CO2: higher in capillary blood (45 mmHg) than alveoli (40 mmHg) so CO2 diffuses out of the blood
greater gradient = faster diffusion
solubility of the gasses
CO2 is 20x more soluble in water than O2, so O2 needs a steeper pressure gradient to move effectively
thickness of respiratory membrane
thicker membrane slows diffusion
thin=faster exchange
normally 0.5 um thick
surface area of respiratory membrane
if SA decreases, gas exchange efficiency drops
more surface area = more exchange opportunities
ventilation-perfusion coupling
lungs adjust ventilation so that air is directed to best-perfused parts of lungs
if part of lung is poorly ventilated, oxygen would have a low pp, which stimulates vasoconstriction and reroute the blood to better-ventilated areas to pick up more oxygen
increased ventilation raises the local blood oxygen pp, and stimulates vasodilation, increasing blood flow to that region
two modes of oxygen transport in blood
98.5% of O2 is bound to hemoglobin, and each hemoglobin can carry up to 4 O2 molecules
1.5% of O2 is dissolved in blood plasma, but is the only portion which contributes to pp of oxygen, which drives diffusion
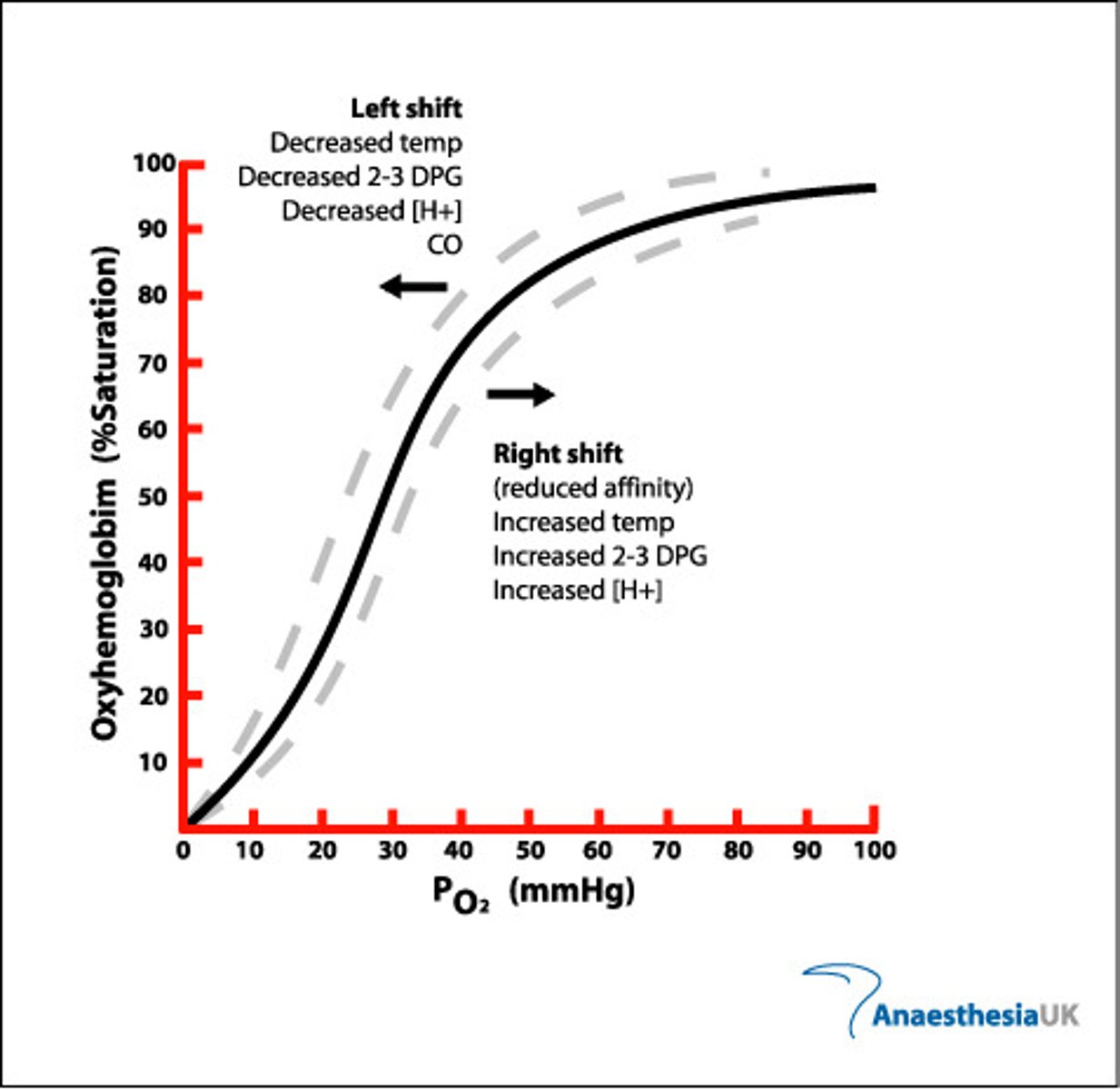
oxyhemoglobin dissociation curve
at low PO2, the curve rises slowly, then there is a rapid increase in oxygen loading as PO2 rises
-when the first heme group binds O2, hemoglobin changes shape that facilitates uptake of second, third, and fourth, which explains the rising midportion of curve
at high PO2 levels, the curve levels off because the hemoglobin reaches 100% saturation
three modes of CO2 transport
90% is hydrated to form carbonic acid, which dissociates into bicarbonate and hydrogen
5% binds to amino groups of plasma proteins and hemoglobin to be transported
5% is carried in blood as dissolved gas
carbaminohemoglobin
hemoglobin bound to carbon dioxide on its polypeptide chains
how carbonic anhydrase and chloride shift help load CO2
CO2 enters RBCs from tissue fluids
CAH converts CO2 + H2O -> H+ and HCO3-
Bicarbonate is transported out of RBC into plasma to avoid buldip
Chloride ions move into RBC as bicarbonate exits to maintain electrical neutrality -> keeps reaction going by removing its products and ensuring continued CO2 uptake
H+ binds to hemoglobin as well, which prevents dangerous pH drop
-Bohr effect - low pH + high CO2 = more O2 unloading
four mechanisms that adjust amount of oxygen unloaded by hemoglobin
lower PO2 in tissues, higher temperature, Bohr effect, and BPG
lower PO2 in tissues
lower PO2 in tissues -> more O2 unloading from hemoglobin
oxygen diffuses from high to low, so more active tissues creates a steeper gradient, pulling in more O2
higher temperature
higher temperature = more O2 unloading
active tissues generate heat -> hemoglobin releases O2 more readily
Bohr effect
lower pH reduces hemoglobin's affinity for O2 -> more O2 release in acidic environments where cells are metabolically active
BPG
BPG is produced by RBCs when tissues are active (hypoxia, fever, high altitude)
BPG binds to hemoglobin and reduces its affinity for O2 -> promotes O2 unloading
three factors that stimulate chemoreceptors
CO2 levels, pH levels, and O2 levels
CO2 and chemoreceptors
high CO2 -> both central and peripheral chemoreceptors -> increases breathing rate and depth
pH levels and chemoreceptors
low pH -> both central and peripheral chemoreceptors -> increases breathing rate and depth to expel CO2 and reduce acid
O2 levels and chemoreceptors
low O2 -> mainly peripheral chemoreceptors -> increases breathing rate and depth
how exercise increases respiration
Increased CO2 decreases pH, which trigger chemoreceptors to send signals to respiratory centers to increase breathing rate and depth
Increased O2 demand increases ventilation -> PO2 in lungs decrease due to increased consumption in muscles, which is sensed by peripheral chemoreceptors and increase RR and TV
Epinephrine increases ventilation by stimulating b-adrenergic receptors in smooth muscle of airways, leading to bronchodilation