The Cervix
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
Cervix
can be assessed clinically w/ a digital exam for dilation, position, consistency, and length
is subjective
Transabdominal or transperineal approach can be used
What type of U/S is best able to accurately determine cervical length?
Transvaginal
Transvaginal Cervical U/S
have pt empty bladder
lithotomy position
insert trdx or have pt insert
align trdx w/ endometrial stripe in longitudinal plane
obtain a sagittal view of the cervix, w/ the long axis view of echogenic endocervical musoca along the length of the canal
lengthen out the cervix and measure from internal os to external os
observe cervix for dynamic changes
fundal pressure?
Incompetent Cervix
premature opening or shortening of the cervix that may lead to fetal loss
may “funnel” (dilation of the internal os)
sign of cervical incompetence
dilation of the internal part of the cervical canal and reduction of the cervical length
>50% funneling before 25 weeks is associated w/ approx. 80% risk of preterm delivery
measure:
% funneling → funnel length(functional cervical length + funnel length)
depth and width of funnel length
shape:
U or V shaped funneling

What changes might we see w/ an Incompetent Cervix?
changes in length and degree of funneling over the course of the ultrasound exam
cervical changes occur in the absence of uterine contractions
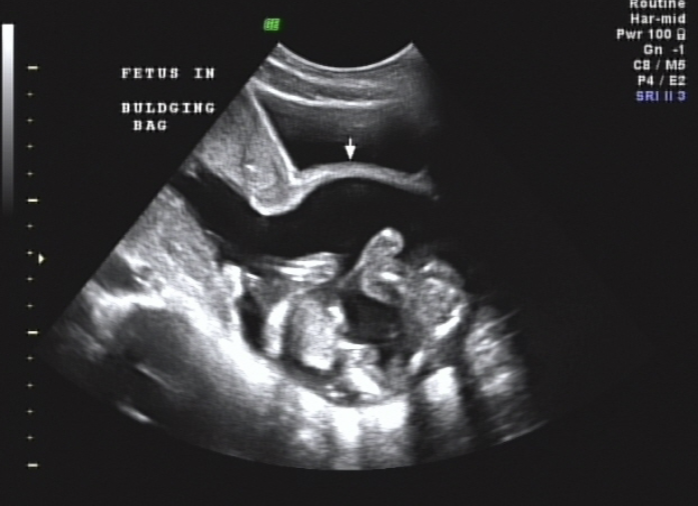
Incompetent Cervix
cervix may open and allow fetus to pass into vaginal canal → Bulging Bag (BBM)
Hour-glassing
If enough cervix remains, a cerclage may be put in place to “stitch” the cervix closed in effort to prevent Preterm delivery (PTD)
would not place cerclage in the presence of major fetal anomaly, PROM, infection or placental abruption
Cerclage U/S:
confirm that the cerclage is intact by visualizing both sides of the string on either side of the cervical canal
measure cervical length
note any funneling and measure the funnel width and length
PROM (Premature Rupture of Membranes)
prior to term (37 weeks)
once the membranes rupture, delivery is recommended when the risk of ascending infection outweighs the risk of prematurity
PROM Risk Factors:
PROM in a prior pregnancy
Illicit drugs (cocaine)
Anemia
Low body mass index (BMI <19.8 kg/m²)
Nutritional deficiencies (copper + ascorbic acid)
Uterine Overdistension (polyhydramnios, mutliples)
Intra-amniotic infection (chorioamnionitis)
Invasive procedure (Amniocentesis, CVS, fetoscopy, cerclage placement)
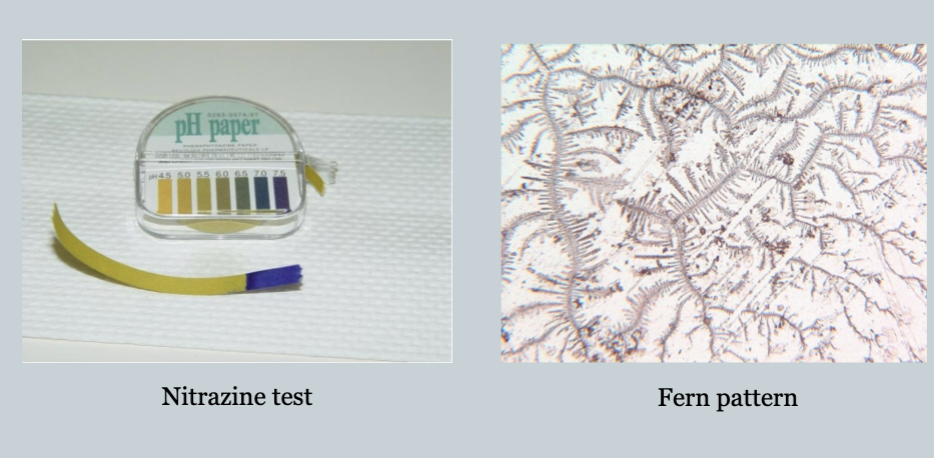
PROM is predominantly a clinical diagnosis:
watery vaginal discharge
visual pooling of clear fluid in the posterior fornix of the vagina or leakage of fluid from the cervical area
an alkaline pH of th cervicovagial discharge, which is tyically demonstrated by seeing whether the discharge turns yellow nitrazine paper to blue (nitrazine test)
microscopic ferning of the cervicovaginal discharge on drying
evidence of diminished amniotic fluid
PROM U/S findings:
oligohydramnios
anhydramnios

Preterm Labor (PTL)
preterm birth is the leading cause of perinatal mortality and morbidity
maternal risk scoring fails to detect up to 70% of infants who are delivered spontaneously before term
PTL risk factors:
previous PTL
cervical incompetence
smoking
nonmedical drug use
multiple GA
polyhydramnios
vaginal bleeding
uterine anomalies
excessive uterine contractions
PTL Detection
cervical changes
fetal fibronectin
is there PROM?
PTL Treatment
corticosteroids for baby’s lung development
best rest if mild
pregesterone gel or tablets
cerclage
antibiotics may be given if bacteria is suspected as a cause of PTL
Tocolytic Meds ( to attempt to stop contractions)
Tocolytic Meds
often only work for a short period of time
Indomethacin - can cause premature closure of DA w/ prolonged use
Magnesium sulfate can cause the pt to be lethargic, dizzy, and weak
many others meds may be used
Fetal Fibronectin (Ffn)
fFN is produced by decidual cells and is a glycoprotein
“Glue” in utero-placental junction
Normally absent from vaginal secretions from 24-36 weeks
an fFN test is a safe, reliable, non-invasive test to tell if the cervix may be getting ready for delivery
not useful for predicting labor in women at risk for preterm labor
The fFN test should only be used for those who:
have intact amniotic membranes
have a cervix that has not dilated >3cm
have only slight vaginal bleeding
do not have cervical cerclage
Negative fFN test result:
very accurate
shows that labor has not started and is unlikely to occur within the next 14 days
Positive fFN test result:
may show that labor has started
but false-positives are common
False-positive fFN test result:
can occur if a woman has recently had:
a pelvic exam
to reduce risk of a false positive, it’s important that a fFN test be done after a manual pelvic exam
sexual intercourse
uterine contractions
vaginal bleeding