CNS drugs, clinical trials and BBB
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
what are CNS drugs used for
they act on CNS to alter mood, behaviour, perception or consciousness
what are the main categories of CNS drugs
depressants
stimulants
analgesics
antipsychotics
antidepressents
anxiolytics
why are CNS disorders increasing
due to aging population and increased life expectancy
examples of CNS disorders associated with aging
Alzheimer’s disease
Parkinson’s disease
stroke
depression
epilepsy
why is drug delivery to brain difficult
due to blood brain barrier which restricts entry of most drugs via oral or IV injection
100% of all proteins and nucleic acids and 98% of small molecules cannot enter CNS
what structures contribute to CNS drug delivery barriers
BBB
cerebrospinal fluid (CSF)
systemic dilution of drugs in circulation
the CNS is extremely sensitive - what is BB designed to do
protect against toxins
maintain stable environment
strictly control what enters the brain
why is the BBB so selective
tight junctions prevent paracellular diffusion
only selective transport or passive diffusion allowed
how do most drugs cross BBB and what are the features that the drug must have
passive diffusion across cell membranes
therefore drug must be:
small
lipophilic
non-polar
why is high blood concentration important for CNS drugs
because brain and blood concentrations reach equilibrium → enough drug must be in blood to reach receptors
what are the strategies to improve CNS drug delivery
intracranial delivery
BBB disruption (temporary)
modify P-glycoprotein transport
intranasal delivery
nanotechnology
what structural feature makes the BBB so restrictive
tight junctions between endothelial cells
prevent paracellular (between-cell) diffusion
force substances to go through cells, not between them
how is BBB permeability different from intestinal permeability
there is poor correlation between Caco-2 (intestinal) permeability and BBB transport
how does drug solubility affect BBB penetration
drug solubility depends on:
molecular structure
distribution of polar vs non-polar regions
intermolecular forces in solid form
how does systemic distribution affect CNS drug delivery
drugs are diluted throughout the body - only a fraction reaches the brain
what happens if the BBB is disrupted
because it can be neurotoxic and damage brain protection systems
Lipinski’s rule of five: what are the parameters for poor absorption/permeation of the drug
poor absorption/permeation if compound has:
more than 5H-bond donors (sum of OHs and NHs)
more than 10H-bond acceptors (sum of Ns and Os)
MW>500
LogP>5
Lipinski’s rule of five: what are the parameters for CNS penetration of drug
CNS penetration likely if:
MW<400
LogP<5 or equal to
H-bond donors <3 or equal to
H-bond acceptors <7 or equal to
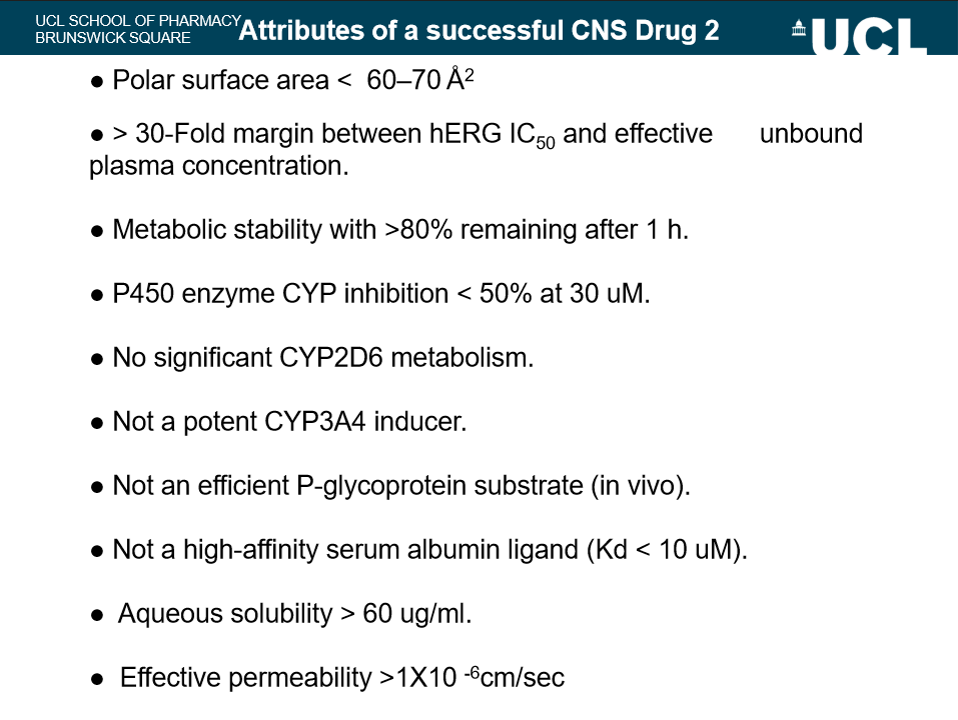
summary of a successful CNS drug parameters
potent activity is low
highly selective
MW < 450
minimal hydrophobicity (clogP < 2.5)
H-bond donors < 3
H-bond acceptors < 8
pKa 7.5-10.5 (avoid acids, keep neutral or basic)
H-bonds < 8
plus all the ones of the slide
why are CNS clinical trails difficult compared to other areas
because:
CNS diseases involve complex brain functions
outcomes are hard to measure objectively
many drugs fail to show clear improvement over existing therapies
the first major challenge in CNS clinical trails: achieving measurable improvement in cognitive function - why?
aim is to improve cognition by counteracting brain damage caused by disease
but this depends heavily on disease stage
why is disease stage critical in CNS trails
mild cognitive impairment → improvement possible
severe neurodegeneration → structural brain damage too advanced
why are early-stage patients considered ‘good experimental subjects’
brain structure less damaged
cognitive decline is still reversible or modifiable
so drug effects easier to detect
why are elderly patients with advanced disease ‘poor-experimental subjects’
often have multiple conditions (e.g. dementia and depression)
cognitive performance varies significantly
improvements may be indirect (e.g. mood, motivation) rather than true cognitive change
what is the second major challenge in CNS trials
interpreting whether observed changes are truly due to drug
why must CNS trials be conducted in ‘neutral environment’
to eliminate external factors that affect cognition like mood, motivation, arousal levels
how can side effects interfere with trials
improvements in cognition may actually be due to:
increased alertness
reduced anxiety
improved mood
why do many CNS drugs fail in clinical trials
Difficulty achieving measurable endpoints
Poor trial design
Inappropriate patient selection
Indirect or confounded effects
many compounds fail to show significant benefit over current therapy