4 - Selected Lumbar Pathology
1/50
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
Osteoarthritis - age demographic
most common in pts 45+
Osteoarthritis - pts typically have Hx of
LBP
Osteoarthritis - presentation
- stiff in AM, pain inc during day
- pain not well localized (cant pinpoint)
- does not radiate to leg (past buttock)
OA - observations
postural changes consistent w overall degeneration
~ arthritis affects facet joints --> loading with inc extension painful = flattened lordosis
OA - neuro findings
none usually present
OA - function
reduced overall motion with exception to flexion
- may req repeated motions to provoke symp if not in acute exacerbation
~ flex is reserved bc nothing is compressed
OA - palpation
palpable degenerative changes
~ abnormal/bumpy
OA - special tests
non-specific
- compression may be positive
OA - segmental mobility
consistently reduced throughout region
degenerative spinal stenosis - age demographic
most common in 65+
degenerative spinal stenosis - Hx of
LBP
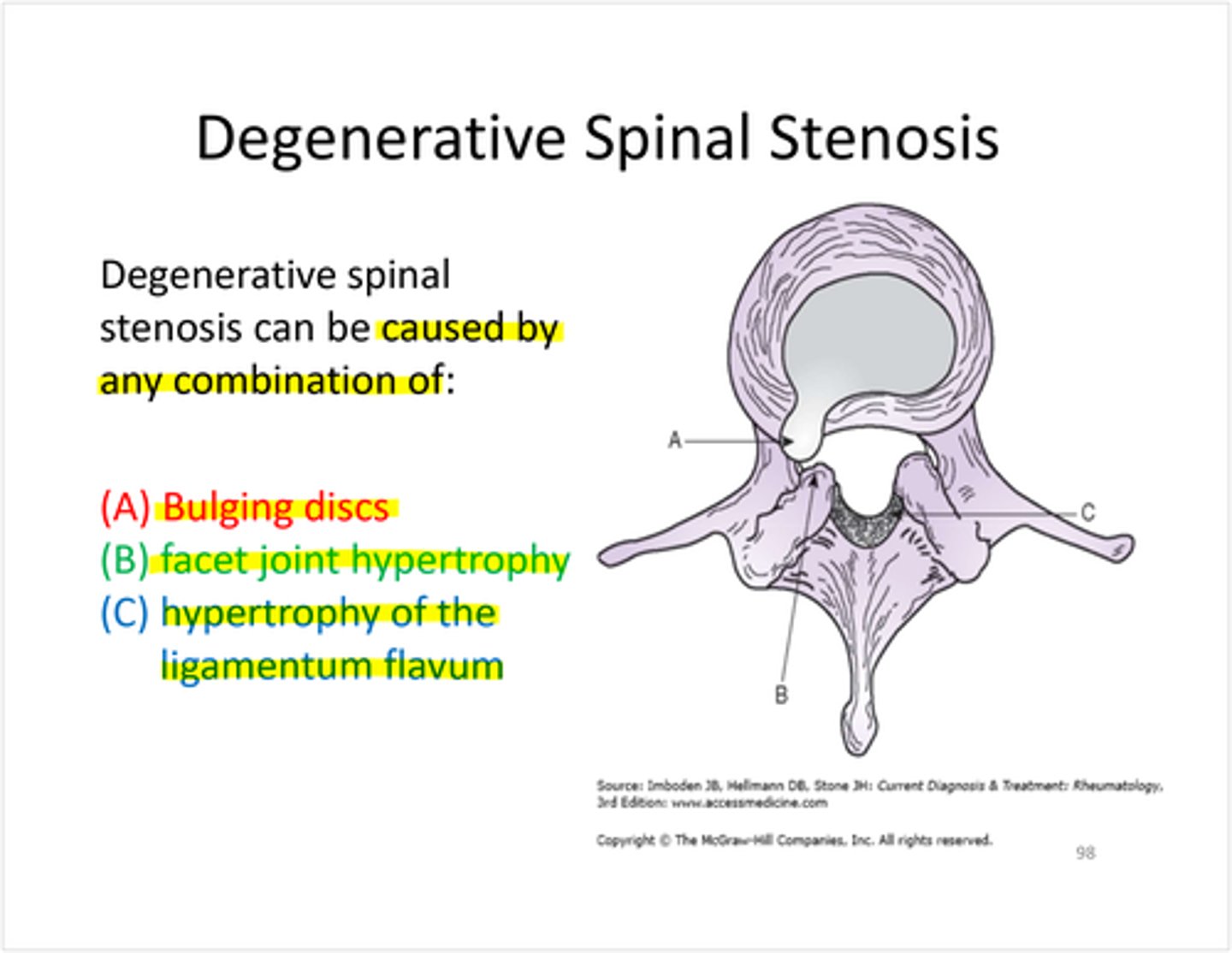
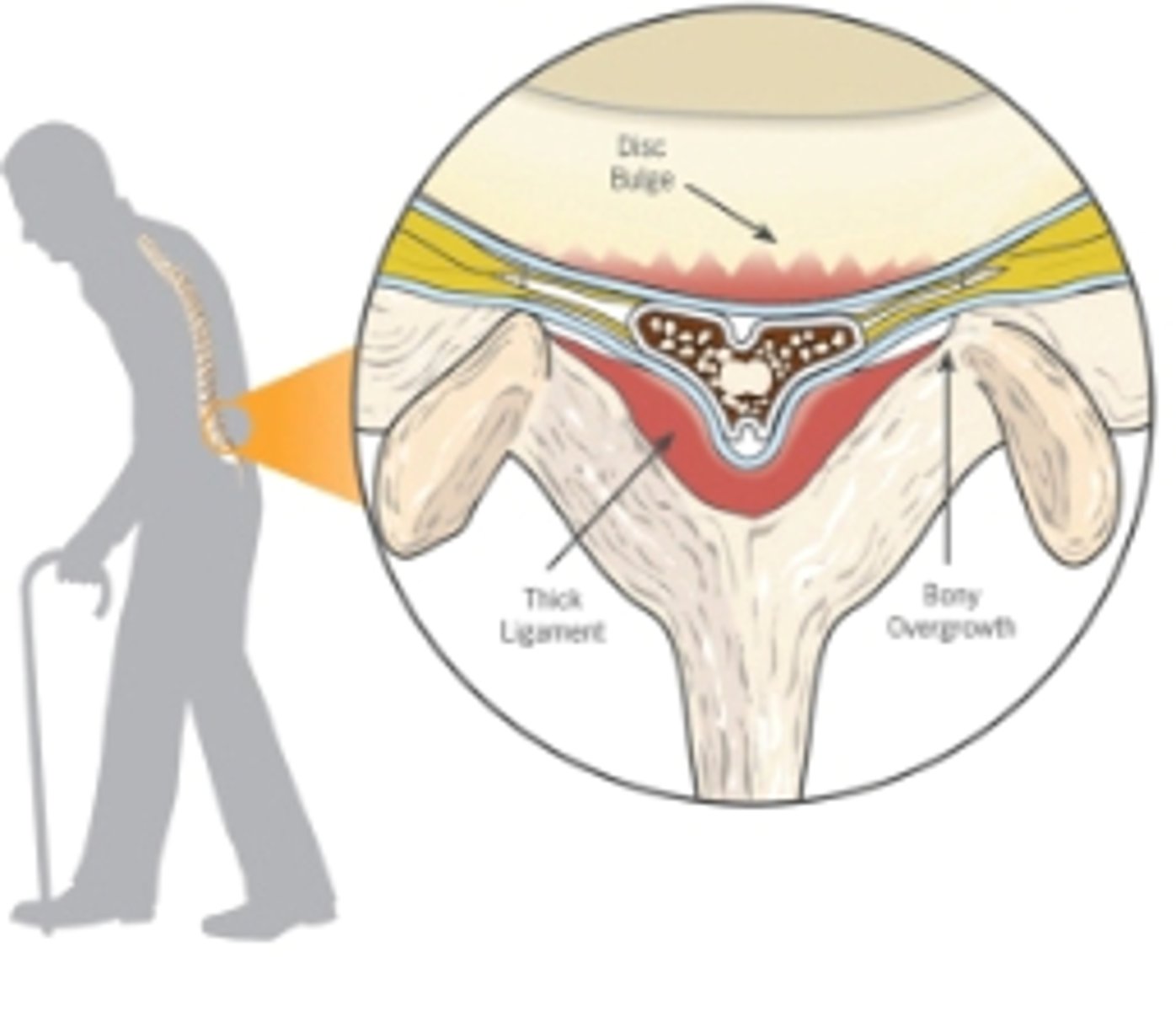
what structures are often involved in degenerative spinal stenosis?
- bulging disc anteriorly
- facet hypertrophy posterioly
- thickening of ligamentum flavum
- spinal cord is compressed overtime bc less space in canal
degenerative spinal stenosis is commonly preceded by:
activities that involved extension
what are activites that aggravate degenerative spinal stenosis? relieves?
- aggravated by walking; standing for long periods of time can worsen symp
- relieved by sitting
why is degenerative spinal stenosis "seasonal"?
Often involves an activity that aggravates the condition
- Ex: going backpacking on vacation = Inc anterior tilt bc of inc stride length can create enough repeated pressure --> inc symptoms
- Ex: gardening --> In spring --> constantly reaching up (extension) in quadruped position
- Can create enough sustained extension to agg. condition
how does walking aggravate degenerative spinal stenosis?
epeated anterior pelvic tilt --> closes space
- Long stride length is often the problem
how does sitting relieve degenerative spinal stenosis?
puts you in neutral/post tilt (stops anterior pelvic tilt)
what is a hallmark for degnerative spinal stenosis?
neurogenic claudication
~ Ex: prolonged walking --> legs start to hurt bc of cord compression
~ Bilateral leg pain
~ Happens bc of neuro problem
degenerative spinal stenosis - observation
- flattened lumbar lordosis accompanied by adaptive changes
degenerative spinal stenosis - posture overtime
- Sequence of decreased --> reversed lordosis
- Increased flexion
degenerative spinal stenosis - neuro findings
- Neurogenic claudication
- May have other neurologic symptoms consistent with compression of SC or nerve roots depending on severity.
degenerative spinal stenosis - function
extension reproduces symptoms
- grossly reduced extension
- SB sometimes reproduces sx
- flexion relieves symptoms
degenerative spinal stenosis - palpation
may note degenerative changes
degenerative spinal stenosis - special tests
- compression positive
- Van Gelderens test for diff neurogenic vs vascular claudication
Van Gelderens test
- Bicycle in upright until sx appear.
- Cont bicycling in flexed position
- Symptoms will resolve in case of neurogenic claudication
neurogenic claudication is
positional - bilateral leg pain
vasular claudication is
based on oxygen demand - bilateral leg pain
- Creating enough O2 demand in LE for blood (inc exercise) --> vascular system can't supply it (requirement cant be met) --> pain in LE muscles
- Occurs when there is a blockage higher in chain (between heart and LE)
- Serious problem --> want to refer immediately to physician
degenerative spinal stenosis - segmental mobility (PPIVMS)
globally reduced segmental mobility consistent w degenerative conditions
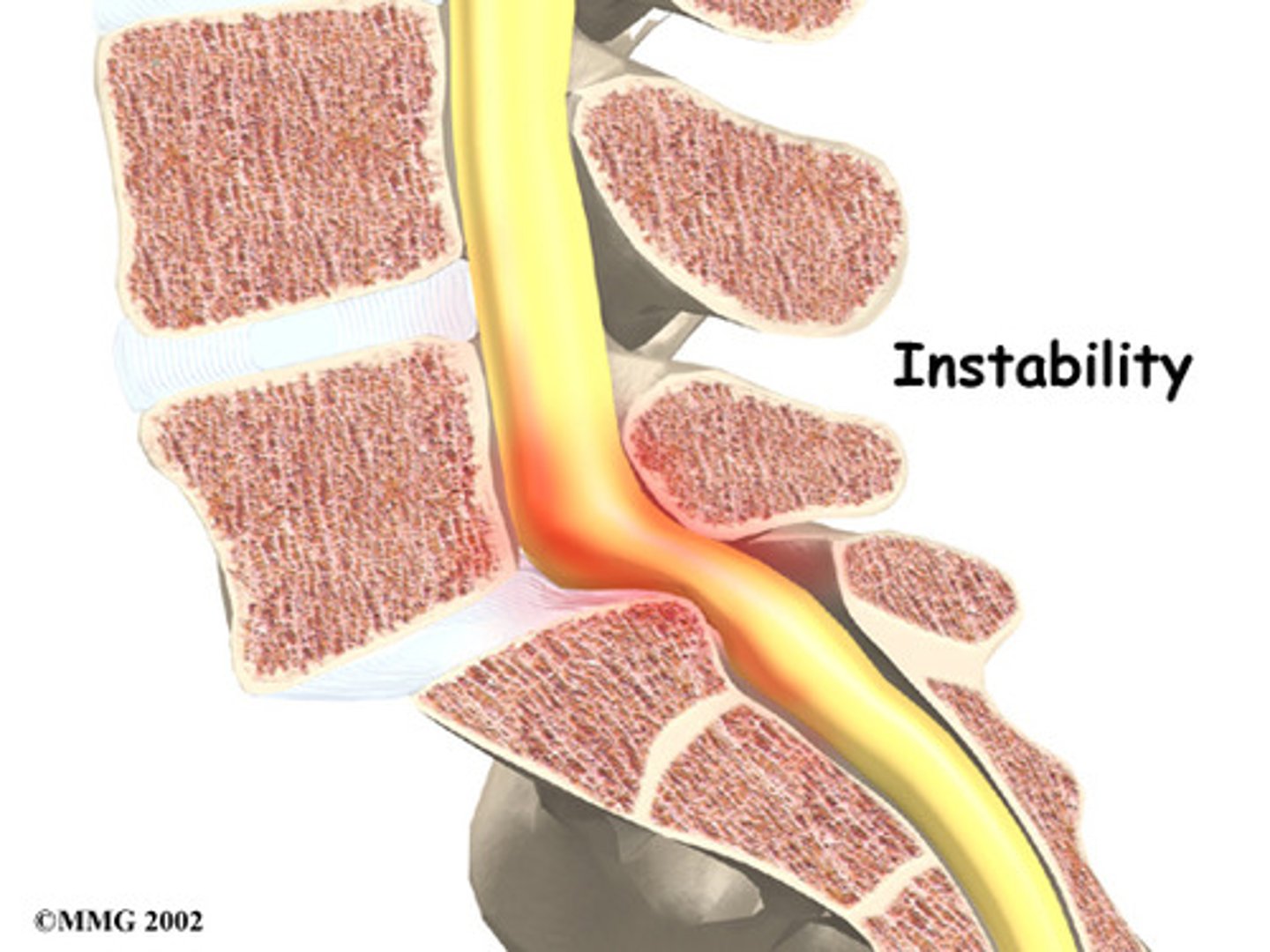
Clinical/Segmental Instability - symptoms
- inconsistent symptoms
- repeated episodes of feeling unstable
- minor aching after episodes
- clicking/cluncking
Clinical/Segmental Instability - observation
hinging or wedging may be present
Clinical/Segmental Instability - function
excessive active ROM
- inability to return from full flexion normally
~ Flexion past end ROM (flexing too far at that segment) --> will walk up their thighs w hands
~ Will relieve moment arm
~ Tries to be in closed packed position before coming up (inc lordosis)
Clinical/Segmental Instability - palpation
pressure during palpation may generate symptoms
Clinical/Segmental Instability - special tests
nonspecific
Clinical/Segmental Instability - segmental mobility present
- shearing may be present
- may note hypermobilities
Facet Joint Dysfunction - onset is often described as
"locking up"
- associated w flexion activity & onset of acute pain when return to upright
Facet joint dysfunction: pain
- constant and severe after onset
- slowly decreases w time
Facet joint dysfunction: Hx
of similar episodes in the past
Facet joint dysfunction: MOI
- Hypermobile segment stretches facet joint capsule
- During flexion: facet joint capsule is fully elongated
- return to standing: capsule does not "retract" with sufficient elasticity to reposition capsular structures, structures are extruded or entrapped
facet joint dysfunction - observation
possible spasm, lack of willingness to move
facet joint dysfunction - neurological
not usually present
- pseudo-radiculopathy may be present
facet joint dysfunction - function
all mvmt painful
- patten varied
- resisted motions increase pain
facet joint dysfunction - palpation
spasm often in paraspinal and multifidus
facet joint dysfunction - special tests
none specific
facet joint dysfunction - segmental mobility
- hypomobile bc of spasm
- FOLLOWED by hypermobility segmentally when sx resolve
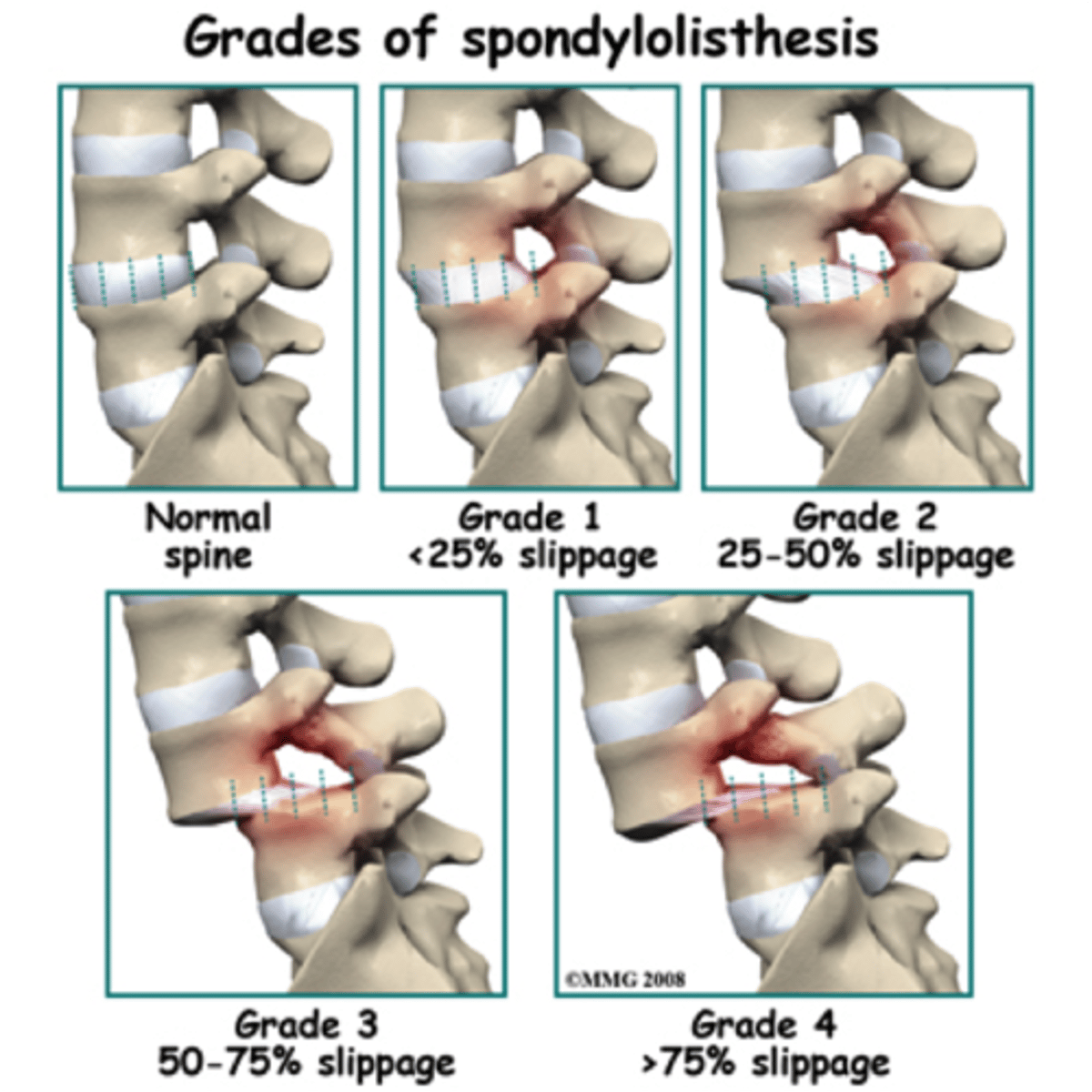
Spondylolisthesis is most common at what segment?
L5/S1
Spondylolisthesis - age demographic
- adolescents 15-20
- degenerative older population
Spondylolisthesis is most common in what gender?
Women > Men
Spondylolisthesis - palpation
step may be palpated
- Palpate - one spinous process "steps up"
- Spinous process of L5 is left behind but body is slipped anteriorly
- L4 spinous process moves anteriorly
Spondylolisthesis - what motion exacerbates symptoms?
extension
Spondylolisthesis - when does neural signs show?
if neurological structures compromised
Spondylolisthesis - shearing
is excessive