17 Acuity Limits & Retinal Development
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
What limits visual acuity under normal viewing conditions?
Visual acuity is primarily limited by optical blur, including refractive error (myopia, hyperopia, astigmatism) and optical aberrations of the eye (imperfections in cornea and lens).
What is the Nyquist limit in the context of visual resolution?
The Nyquist limit is the maximum spatial resolution a sampling system can represent without aliasing. In vision, it’s determined by cone photoreceptor spacing in the fovea.
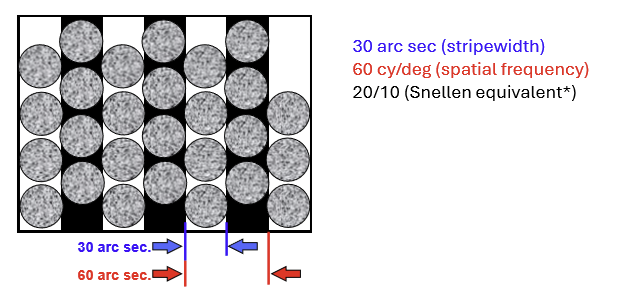
How does cone spacing in the fovea set a theoretical limit on visual resolution?
Foveal cones are spaced ~30 arc sec center‑to‑center.
To resolve a grating:
1 stripe per row of cones, and
2 stripes per cycle (period)
→ yields 1 cycle per 60 arc sec (1 arc min) - 20/10 Snellen equivalent
What does a Nyquist limit of 60 cycles/degree mean anatomically in the fovea?
It reflects cone sampling density:
Foveal cones are spaced ~30 arc sec apart
One stripe falls on one cone
Two stripes (one cycle) require two cones
→ 1 cycle per 60 arc sec (= 60 cycles/degree)
This is the maximum resolution acuity allowed by cone spacing.
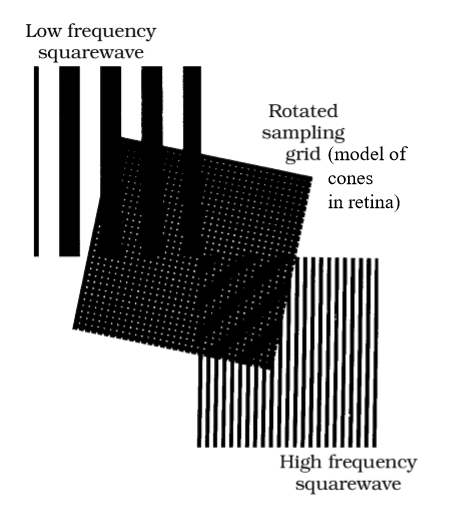
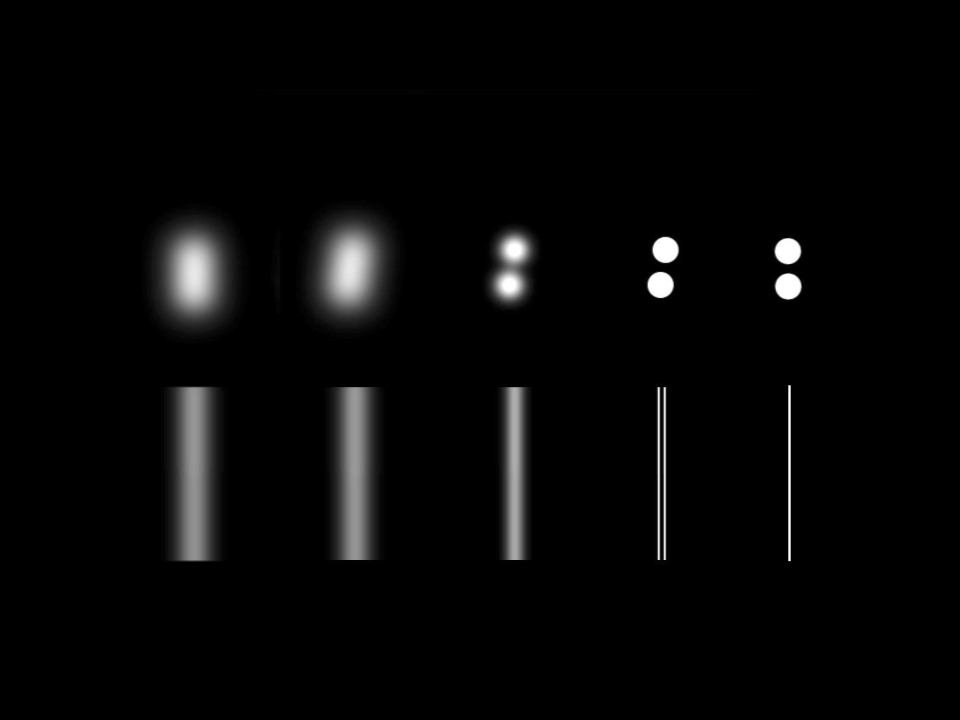
What is aliasing and how does it appear when viewing a high–spatial‑frequency grating?
Aliasing occurs when a grating has very fine spacing, but the visual system samples it too coarsely.
The grating can still be seen, but it looks distorted or abnormal rather than properly resolved.
This can be replicated by viewing fine gratings through a grid of holes with wider spacing, causing a misleading appearance.
Why is the Nyquist limit of the eye difficult to measure experimentally?
Because optical losses in the ocular media reduce image quality before retinal sampling can be tested, masking the true anatomical resolution limit.
What are the main sources of optical loss that degrade fine spatial resolution in the eye?
Defocus (sphere and cylinder → dioptric blur)
Higher‑order aberrations
Scatter in the ocular media and retina
Stray light not absorbed by visual pigments or the RPE
How do optical losses affect the appearance of small letters or thin gratings?
They reduce contrast:
Black–white patterns appear gray
Effects are strongest for very small letters and thin square‑wave gratings
Why aren’t aliased gratings visible above the Nyquist limit in real eyes?
Because optical blur and scatter suppress high spatial frequencies so strongly that fine gratings are not seen at all, even in their aliased form.
How can aliasing beyond the Nyquist limit be observed experimentally?
By bypassing the eye’s optics, such as with adaptive optics or laser interference gratings, which remove blur from the ocular media and allow very high spatial frequencies to reach the retina.
How does optical blur affect visual perception of high spatial frequencies?
Blur suppresses fine spatial detail, effectively “rescuing” the retina from seeing strange aliasing artifacts.
Blur isn’t always bad, it can improve perceptual stability.
What ultimately limits the best possible human resolution acuity under ideal conditions?
The Nyquist limit set by foveal cone anatomy (cone spacing and outer‑segment width).
→ Maximum resolution ≈ 60 cycles/degree, equivalent to 20/10 Snellen.
Why do many people not reach the anatomical maximum acuity of 20/10?
Because of optical aberrations (defocus and higher‑order aberrations), which reduce contrast and fine detail. Practical maximum acuity for many observers is ~20/20.
How does retinal wiring in the scotopic (rod) system affect resolution acuity?
There is extensive spatial summation:
Many rods → one rod bipolar cell
Many rod bipolar cells → one AII amacrine cell
Signals from many rods converge on single ganglion cells
What is the best achievable rod‑mediated resolution acuity, and why is it limited?
Approximately 20/100 to 20/200.
Limited by high convergence and spatial summation in the rod system, which sacrifices spatial resolution to increase sensitivity in low light.
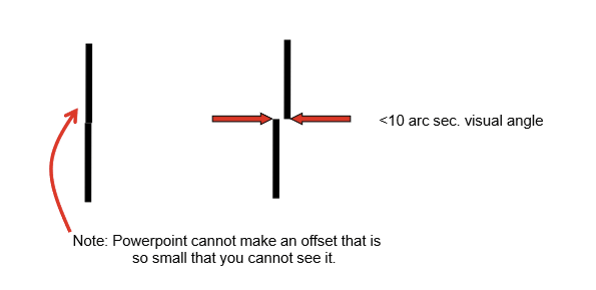
What is Vernier acuity, and why is it considered a hyperacuity?
Vernier acuity is the ability to judge the relative position of two stimuli (e.g., alignment or offset).
It is a hyperacuity because performance is not limited by the photoreceptor mosaic, allowing detection of spatial offsets smaller than cone spacing. This allows us to detect offsets of only a few arc seconds of visual angle, far better than predicted by photoreceptor spacing.
What are some other examples of hyperacuities besides Vernier acuity?
Other hyperacuities include:
Leveling (judging whether an object or picture is truly horizontal)
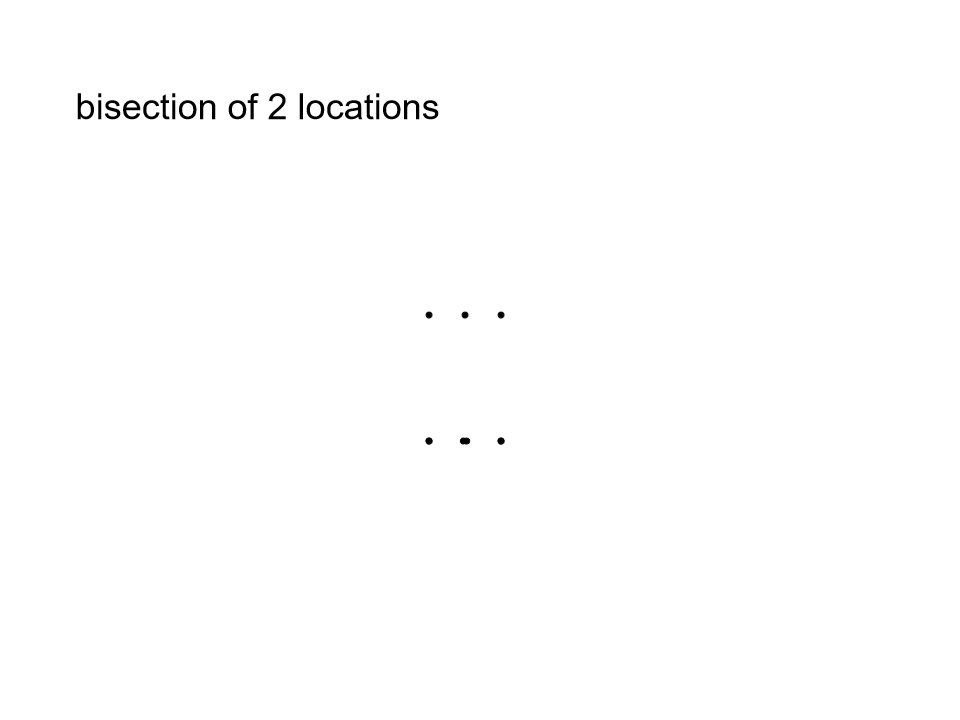
Centering / bisection (judging whether a point divides a line equally; e.g., “spirit level” tasks)
Orientation discrimination (detecting very small differences in line orientation)
All involve precise relative judgments and exceed limits predicted by photoreceptor spacing.
How are hyperacuities (e.g., Vernier acuity) possible despite limits of photoreceptor spacing?
Hyperacuities are possible because neural responses to nearby stimuli overlap.
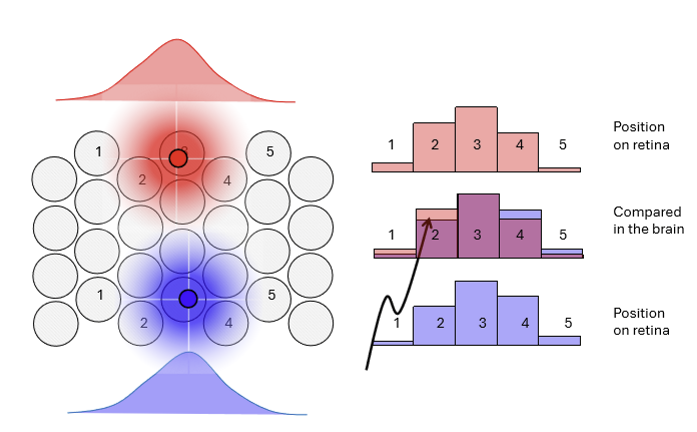
When narrowly tuned detectors (small receptive fields) are activated by multiple stimuli, the visual system can compare relative patterns of activity, allowing extremely precise judgments of position or alignment.
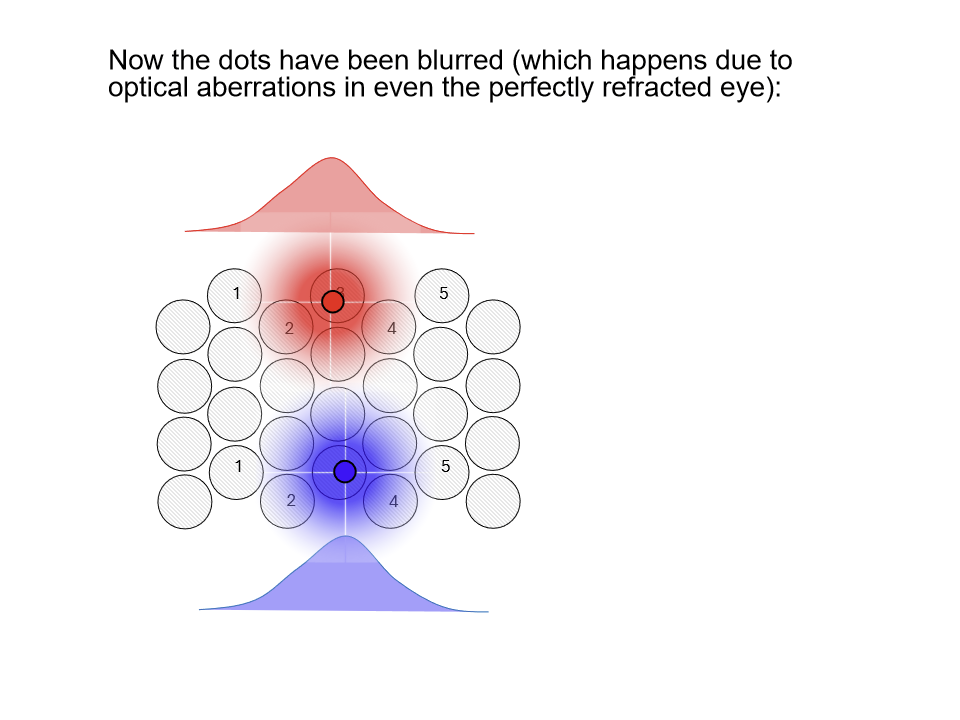
How can the visual system achieve hyperacuities beyond photoreceptor spacing?
When dots are blurred, misalignment can still be detected because adjacent cones capture different amounts of light.
The overlapping photon capture across neighboring cones creates subtle differences in neural responses, enabling precise relative position judgments despite blur.
Why is a small amount of blur in the normal (emmetropic) eye actually beneficial for vision?
A small amount of blur reduces high spatial frequencies, which:
Protects against aliasing artifacts
Enables hyperacuities like Vernier acuity by allowing overlapping neural responses
When does blur become harmful to vision, and how is it managed clinically?
Excess blur from correctable refractive errors (sphere and cylinder) impairs:
Grating acuity
Optotype (letter) acuity
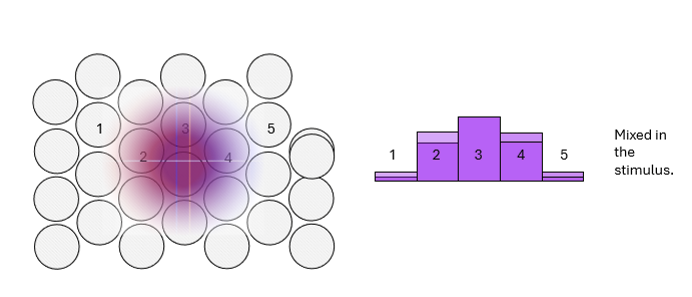
What happens if two blurred dots are perfectly aligned on top of each other?
They cannot be distinguished as separate stimuli because the same cones respond to both dots.
The overlapping blur circles activate identical receptors, so the stimulus is perceived as slightly wider, not misaligned or double.
Which disorders significantly affect Vernier acuity, and how does this relate to resolution acuity?
Refractive amblyopia: Vernier acuity loss is closely related to resolution acuity loss
Strabismic amblyopia: Vernier acuity loss is much greater than resolution acuity loss, reflecting a disproportionate deficit in positional processing
Which common disorder has relatively little effect on Vernier acuity, and why?
Cataract has relatively little effect on Vernier acuity because it primarily causes optical blur.
It reduces resolution and optotype acuity, but hyperacuity tasks like Vernier judgments are largely preserved.
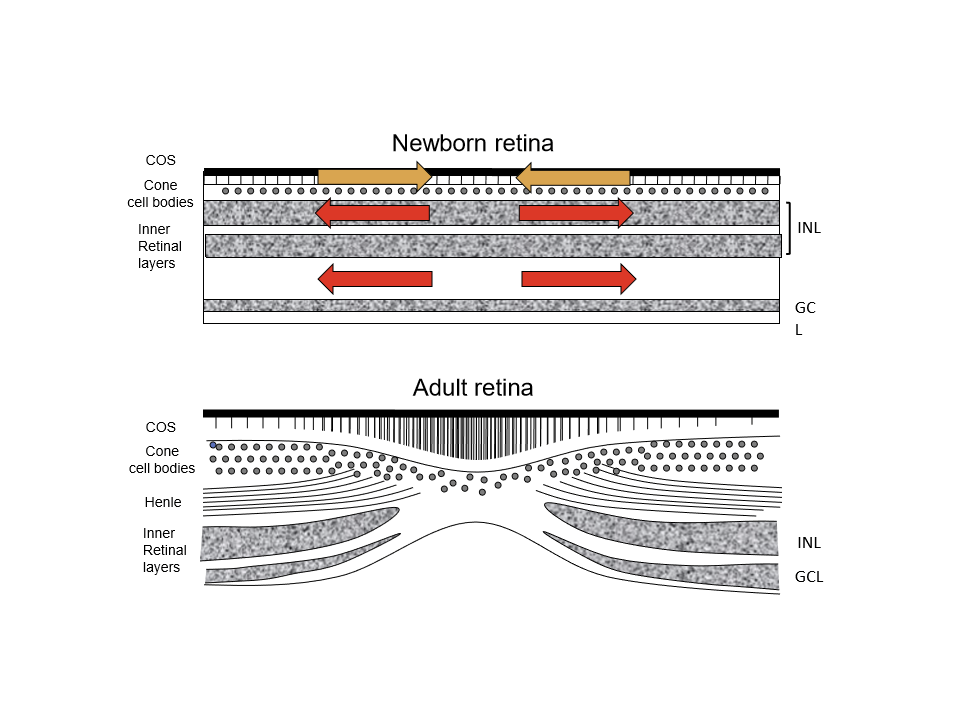
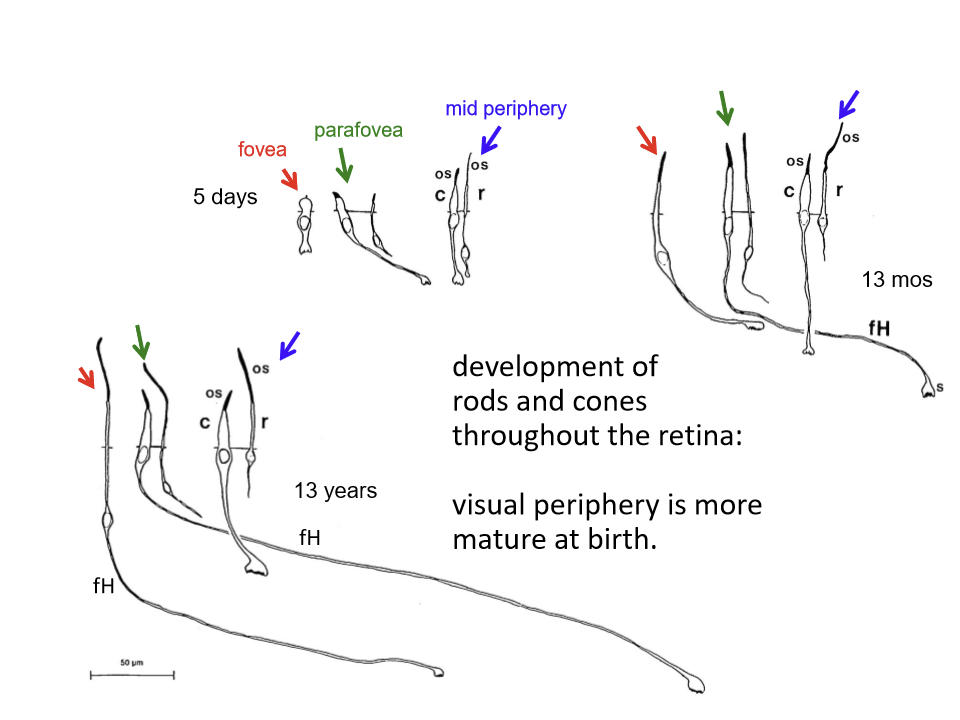
What are the key morphological features of the newborn infant fovea?
Cones are thick (“fat”), not slender
Outer segments are very short
No fibers of Henle
Inner nuclear layer (INL) extends through the central retina
Ganglion cell bodies form a single layer throughout
The foveal pit is shallow and poorly defined
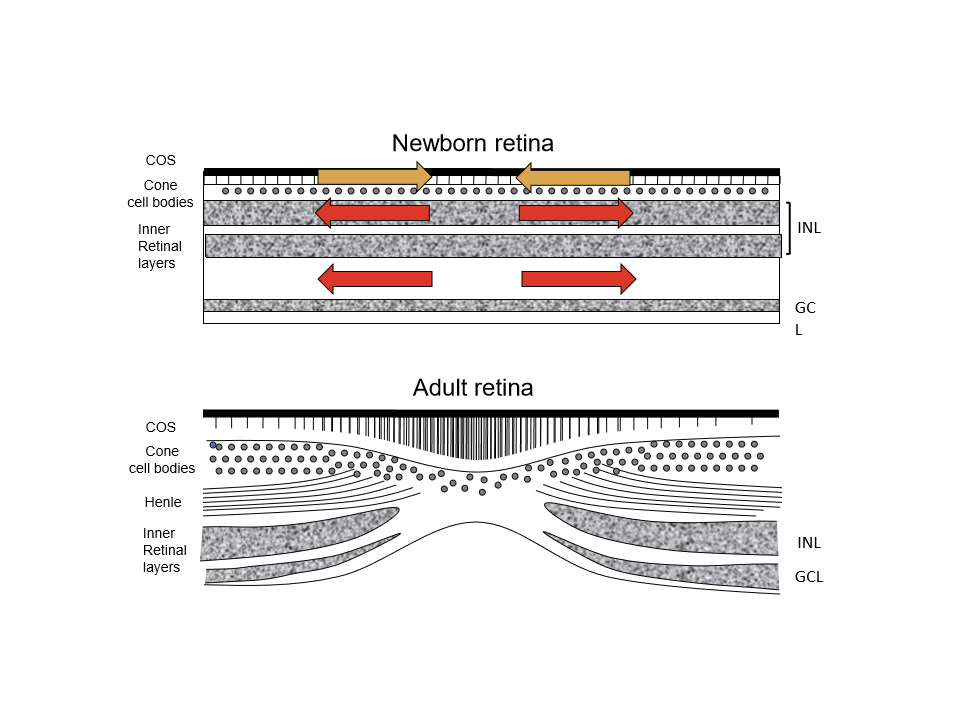
What major structural changes occur in the fovea as infants mature?
Cones become thinner and more tightly packed
Outer segments lengthen
Fibers of Henle appear and elongate
INL cell bodies migrate away from the fovea
Ganglion cells are displaced away from the foveal center
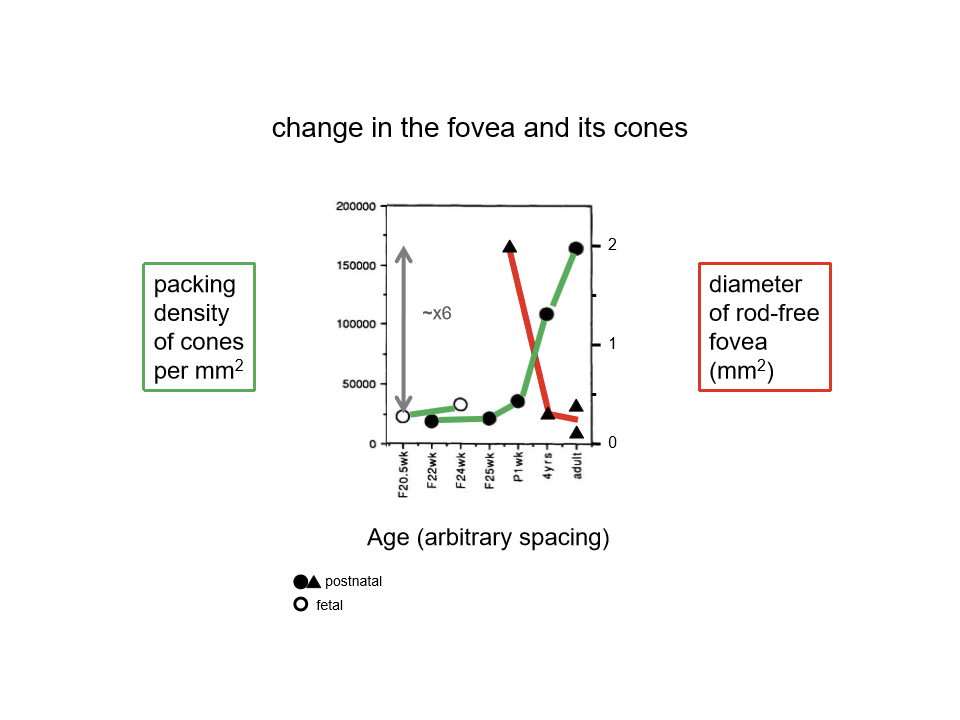
How does foveal cone density change during development?
As the fovea matures, it becomes smaller in area but much more densely packed with cones, increasing potential spatial resolution.
Compared to the fovea, how developmed of rods and cones in the periphery?
Visual periphery is more mature at birth.
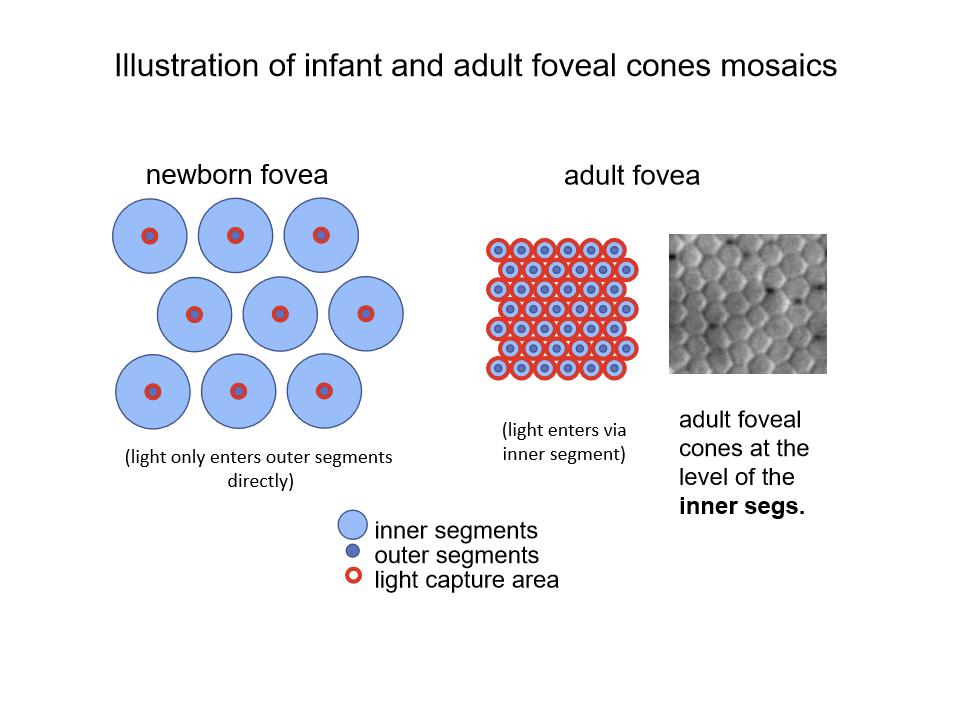
What are the visual consequences of foveal immaturity in newborns compared to adults?
In newborns, vision is limited because:
There is little or no waveguiding
Much of the incident light does not reach cone outer segments
Short cone outer segments absorb less light
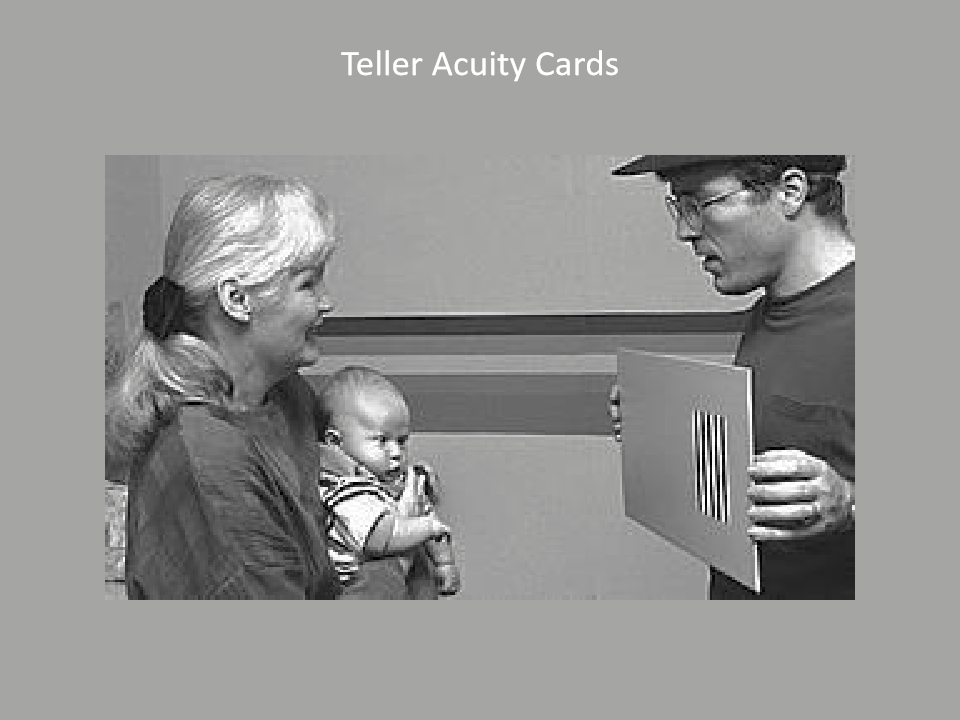
How is VA of infants measured?
Teller Acuity Cards. Adults guess which side based on looking.
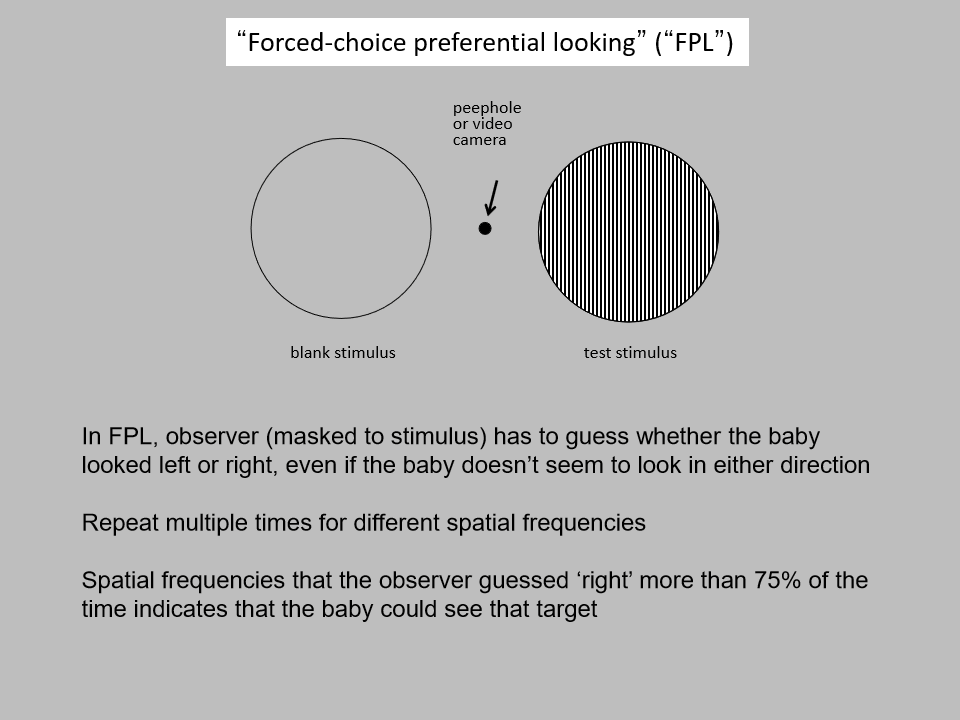
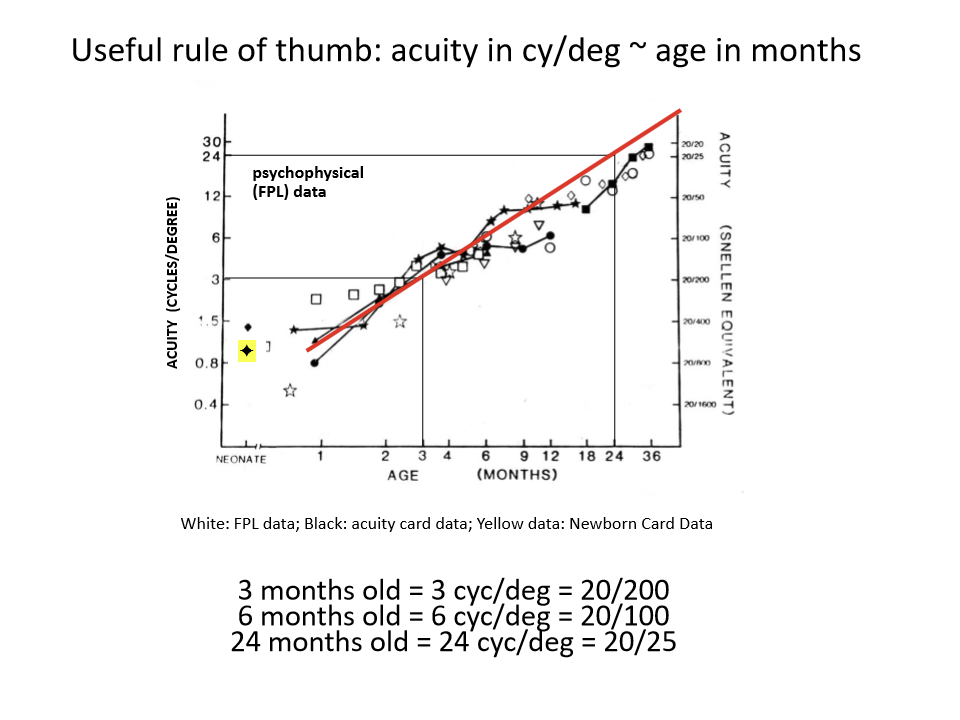
What is Forced‑Choice Preferential Looking (FPL) and why is it used in infants?
FPL is a behavioral method to assess infant vision where a masked observer guesses whether the baby looked left or right toward a patterned stimulus.
It is used because infants cannot give verbal responses or follow instructions.
How does FPL determine whether an infant can see a given spatial frequency?
The test is repeated across multiple spatial frequencies.
If the observer correctly guesses the stimulus side >75% of the time, it indicates the infant can see that spatial frequency.
What is the acuity of an infant as they develop?
3 months old = 3 cyc/deg =20/200
6 months old = 6 cyc/deg = 20/100
24 months old = 24 cyc/deg =20/25
Can infants make discriminations based on luminance?
Yes, they can. They get better with age.
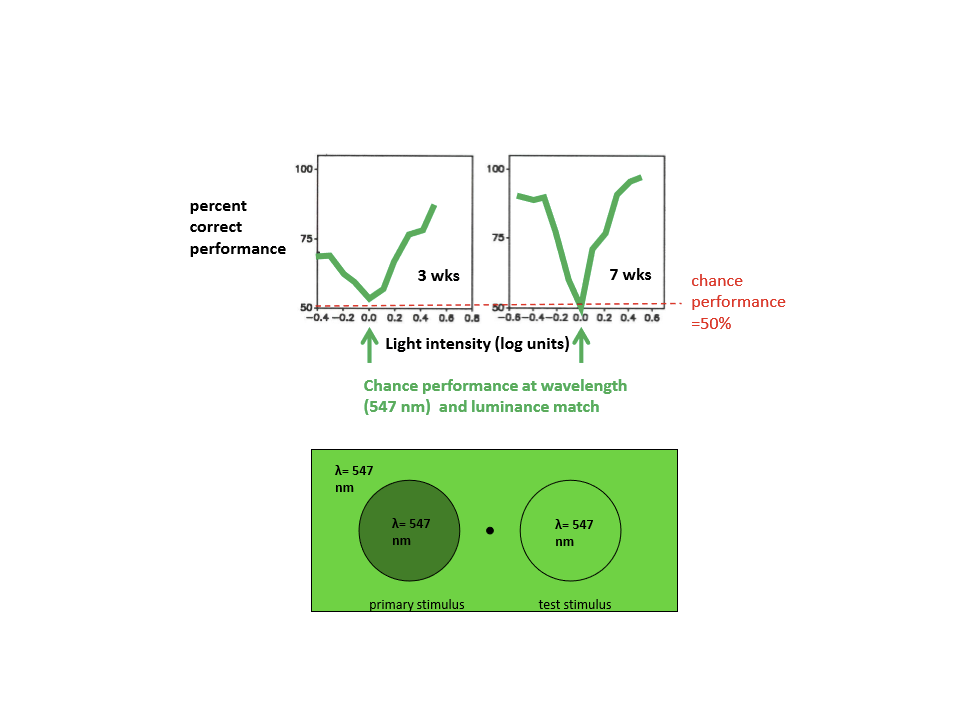
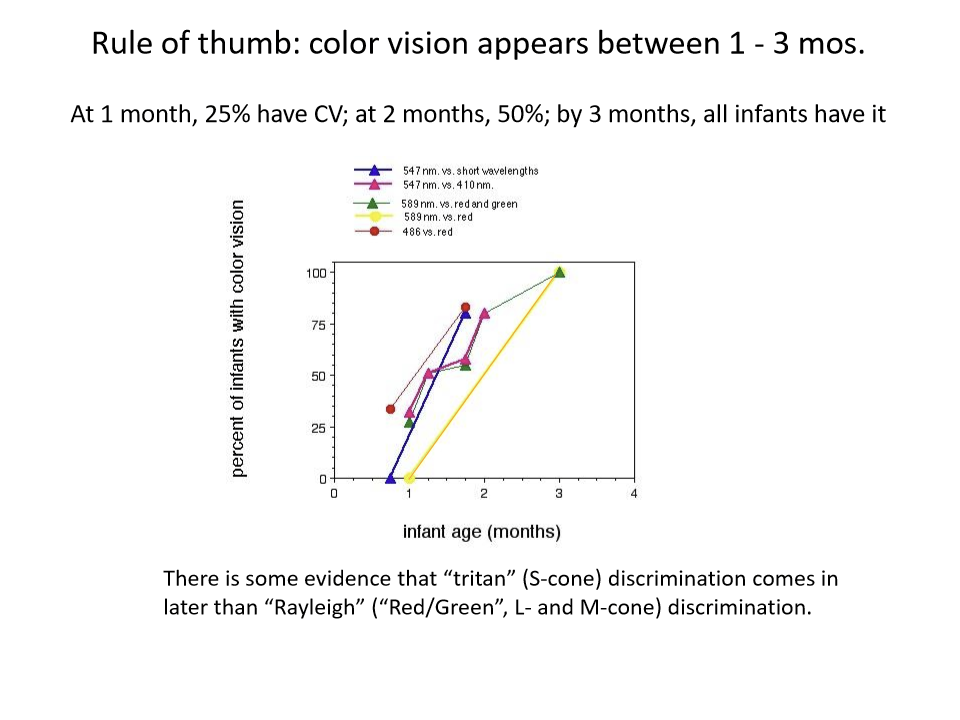
Do very young infants show color vision?
For 7-week-olds, they do show that they have color vision. For 3-week-old infants, they do not show evidence of color vision.
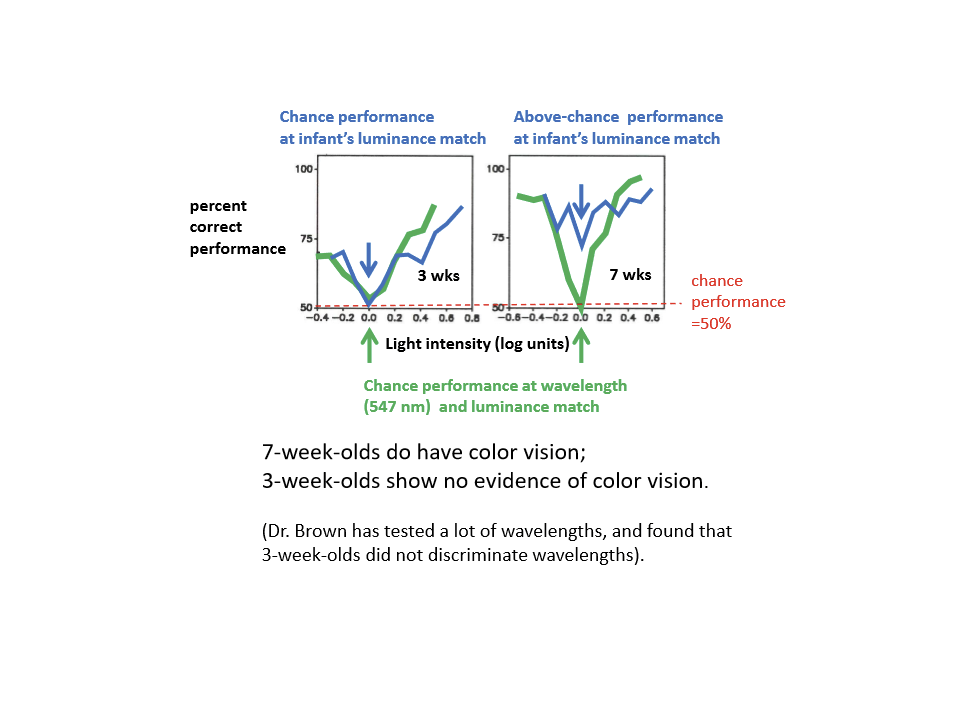
When does color vision appear in infants?
Between 1-3 months. at 1 month, 25% VC; at 2 months, 50%; by 3 months, all infants have it