Nursing Exam 3
1/105
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
106 Terms
Healthcare is a business
A hospital must stay in the black (make a profit) in order to pay its employees, buy new equipment, and keep the doors open
The nursing department often has the largest number of employees
Healthcare organizations
Acute care hospitals
Nurse-managed clinics
Ambulatory care clinics
Family practice
Dermatology clinic
Home healthcare agencies
Hospice care
Long-term care facilities
Occupational health clinics
Rehabilitation centers
Urgent care centers
School health clinics
Skilled nursing facilities
Pediatric hospital
Psychiatric-mental health facility
Substance use disorder center (inpatient and outpatient)
for-profit hospitals
are owned by private stockholders and must pay them back a portion of what they make
hospital must always have funds to pay stockholders/owners:
Methodist Hospital (San Antonio)
CJW Medical Center – Chippenham Campus (Richmond, Va.)
Henrico Doctors’ Hospital (Richmond, Va.)
Medical City Hospital (Dallas)
Sunrise Hospital & Medical Center (Las Vegas)
non profit hospitals
are owned by communities, religious-affiliations, etc.
Make no mistake, a non-profit hospital is still making a profit, they just don’t have to pay it back
most community hospitls are
not for profit
Many hospitals are part of a network Health Care Organization just like MaineHealth
community hospitals
The AHA (2022) defines a community hospital as all non-federal, short-term, general or specialty hospitals – including teaching hospitals.
2022 most hopsitals are community
Other terms to classify hospitals
Bed-size
Less 100
100-150
150-250
250-500
More than 500
Teaching versus non-teaching
Length of stay
Multi-hospital system
Critical Access
What is a Critical Access Hospital?
Small hospitals in rural areas that support emergency care of a public
24-hour ED
Up to 25 inpatient beds
Average length of stay less than 96 hours
More than 35 minutes from another hospital, more than 15 miles over mountainous terrain and secondary roads, or certified by the State to be a necessary provider of healthcare services
In general, critical access care sites are medical facilities that offer healthcare services to rural communities. In some situations, they will stabilize the patient and then transfer them to a higher level of care facility
Critical Access Hospitals (16) examples
Northern Light Blue Hill
Brighton Hospital
Calais Regional
Northern Light C.A. Dean Hospital
Down East Community Hospital
Houlton Regional
Lincoln Health
Northern Light Mayo Hospital
Millinocket Regional Hospital
Mount Desert Island Hospital
Penobscot Valley Hospital
Redington-Fairview Hospital
Rumford Hospital
Northern Light Sebasticook Hospital
Stephen’s Memorial Hospital
Waldo County General Hospital
maines hospitals
According to the Maine Hospital Association (2022), Maine has 36 hospitals:
33 non-profit general hospitals
Two private psychiatric hospitals
One acute rehab hospital
PLUS, the State government run facilities:
Dorothea Dix Psychiatric Hospital in Bangor
Riverview Psychiatric Hospital in Augusta
One Federal facility:
The VA Hospital in Togus
Cary Medical Center in Caribou, Maine is owned by the Caribou Hospital District – owned by the municipality of Caribou.
where do nurses work
While most nurses work in acute care, there are many other settings where nurses can care for patients and many different roles a nurse can fulfill
About 30% work in hospitals
15% outpatient
12% in home health
9% in long term care
7% in physician offices
hospital departments
Administration
Nursing
Medical staff
Admission and Discharge
Social services
Medical records
Information management
Quality improvement
Infection control
Research and Evidence-based practices
Staff development
Environmental services
Dietary
Healthcare providers
Registered Nurse
Licensed Practical Nurse
Patient Care Assistant/Technician
Certified Nursing Assistant
Advanced Practice Registered Nurse
Clinical Nurse Specialist
Clinical Nurse Leader
Certified Nurse Midwife
Certified Registered Nurse Anesthetist
Doctor of Nursing Practice
Physician
Physician Assistant
Pharmacist
Occupational Therapist
Physical Therapist
Registered Dietician
Respiratory Therapist
Social worker
work place culture-consonant
Functional / effective
workplace culture dissonant
Nonfunctional / ineffective
Culture has an impact on nursing staff and the care they provide
$$$ spent – Macro view
National Health Expenditures increased to $4.9 TRILLION in 2023
That’s $14,570 per person!
Medicare spending increased to $1,029.8 BILLION in 2023
Medicaid spending increased to $871.7 BILLION in 2023
Private insurance spending increased to $1464.6 BILLION in 2023
Out-of-pocket spending increased to $505.7 BILLION in 2023
Prescription drug spending increased to $449.7 BILLION
$$$ spent – Micro view
Considers financial needs of individual hospitals and health care organizations
THE BUDGET – made to manage financial issues for a specified period (usually a year)
Salaries and benefits
Equipment, supplies, utilities
Pharmaceutical needs
Facility maintenance
Dietary needs
And more!
Nursing management must have an active role in planning the budget
It takes about $40,000 to on-board a new nurse!
Reimbursement
Payment of the patient’s bill for healthcare services provided, which in turn, covers the cost of care (salaries, benefits, drugs, supplies, equipment, etc.)
One move changed everything
In 1965, Title XVIII amendment to the Social Security Act created Medicare – the federal health insurance program for people over 65 years old, people with disabilities, and people with end-stage renal disease
Also in 1965, Title XIX amendment to the Social Security Act created Medicaid – the federally funded STATE insurance program for people who met certain income restrictions, children, disabled, the blind and others depending on your state of legal residence
Remember, there is also third-party insurance (employer)
Insurance
If your employer does not offer insurance, you must either purchase your own private insurance, apply for Medicare or Medicaid, or go without insurance (complicated with the ACA)
Patient receives healthcare services through a fee-for-service reimbursement model, then pays:
deductible and copayment
deductible
the part of the bill that the patient must pay before the insurer pays the rest of the bill (annual limit)
copayment
the fixed amount that the patient may be required to pay per service
Changes in healthcare delivery
Must focus on meeting the needs of the public
Develop new processes with better financial models
Improve efficiency and flexibility
Clear communication
Have a voice in decisions that affect nursing
IOM 5 Core Competencies For Health Care Professionals
Provide Patient-Centered Care
Work in Interprofessional Teams
Employ Evidence-based Practice
Apply Quality Improvement
Utilize informatics
patinet centered care
Identify, respect and care about patient differences and expressed needs
Relieve pain and suffering
Coordinate continuous care
Listen to the patient!
Clearly inform, communicate with, and educate patients
Patient Centered Care:
Three levels
Individual … frame the plan of care to meet the specific needs of the patient
Organizational … environmental and broader impacts on care that impact patient-centeredness
MACRO – the Health Care System…regulations, expectations, and support factors
Patient Centered Care Theories
dorothea orem
jean watson
madeleine leininger
hildegard peplau
dorothea orem
Self-Care Theory
Help the patient learn how to help themselves and how to manage their life and challenges
Empower!
jean watson
Transformational Caring
The reciprocal relationship we have with patients impacts both patient and nurse
Madeleine Leininger
Transcultural Caring Theory
Focuses on cultural competence, seeking understanding, and providing individualized culturally appropriate care
Hildegard Peplau
Interpersonal Relations Theory
Focuses on the unique nature of nurse-patient therapeutic, professional relationships
Patient Centered Care:
What is the nurse’s role?
Advocate for the patient
Help the patient to care for self
Address health literacy and provide education
Involve appropriate participants
Seek feedback
Increase sense of self-efficacy
Increase resilience and confidence
Create a therapeutic nurse-patient relationship
PCC: Coordinate Care
Create the Plan of Care (POC) through clinical reasoning, critical thinking, and clinical judgment
Collaboration and interdisciplinary communication (team management, teamwork, communication!)
Post-Discharge follow up plans (easy contact info, easy instructions, medications, etc.)
Effective delegation (assigning responsibility of a task to someone else)
PCC: Must Consider disparities, patient priorities, diversity
Inclusion of patient’s cultural and spiritual values
Consideration of health disparities
Respect patient needs and preferences as they are
Sensitivity to spiritual dimensions of care… they matter!
Assess access to care past and future
Assess patient resources- financial and human
Roles of the nurse – We have many
Provider of care
Educator
Counselor
Manager
Researcher
Collaborator
Change agent
Entrepreneur
Patient advocate
Leader
nursing process
Method for how we provide patient care
nursing process acronym
assement, diagnosis, planning, implementation, emulation
assessment
subjective: current complaiment, history, medications
objective: vital signs, intake and output of fluids, height and weight
diagnosis
rns clinicals judgment about acual or potential health problems to help prioritize and plan care
planning
goals and outcomes formulated personalized to indvisuals unqiue needs
implementation
carrying out interventions outlined like a cardiac monitor or o2, medication and standard protocols
evaluation
evulated implenation to ensure desired outcome has been met, continuous reassesment may be needed
Strategies to encourage patient participation
Talk to patients in their room, not from the doorway
Pay attention to your body language
Use open-ended questions “Tell me about…”
Therapeutic touch
Collaborative thinking language “Let’s think this through”
Don’t sound like the pt’s case is very unusual
Address patients respectfully “Mr.” “Mrs.”
Be direct and honest
Don’t look at your watch
consumerism
Patients expect to be active in their own care at all levels
Micro consumers = patients
Macro consumers = government and insurers who are the major purchasers of care
Macro consumers have influence over the care provided since they pay the majority
Patient rights
Can’t be denied health care coverage, even if they have a pre-existing condition
Right to choose their own doctor
Right to fair treatment and emergency care
Insurance policies cannot be cancelled unfairly
Ended annual and lifetime limits for coverage/benefits
Enhanced access to preventative services
Right to appeal health plan/insurer decisions
Ensure health coverage for young adults (up to age 26)
Privacy
Informed consent
Patient Self-Determination Act of 1990
Patient satisfaction (HCAHPS)
Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHP) – national survey to assess patient satisfaction
Sent out to randomly selected patients that were discharged from the hospital each month
Patients are asked about:
Facilities – cleanliness of the room, food, room temperature, noise levels
Nurses and physicians – communication, interactions, attentiveness, pain management, care provided, discharge instructions, instructions about medications, and coordination of care
HCAHPS
29 item questionnaire to measure patient’s perceptions of their hospital experience
Allows valid comparisons to be made across hospitals (locally, regionally, nationally)
National Database of Nursing Quality Indicators (NDNQI)
Another external organization that tracks patient harm:
Falls
Pressure ulcers
Catheter-associated urinary tract infections (CAUTI)
Central line-associated blood stream infections (CLABSI)
Ventilator associated pneumonia (VAP)
The care quality information is available to the public
NDNQI also provides an employee survey that many hospitals administer yearly to track employee satisfaction – this information stays within the organization
Leapfrog
Data is available to health care consumers (patients) regarding patient satisfaction scores and quality of care provided at hospitals across the USA through a public website called Leapfrog.
Patient Advocacy and the role of the nurse
Help the patient understand
Help the patient find their voice
Work with the patient to assure the best possible outcome based on what they want, even if what they want is to do nothing – even if you disagree
Capacity for self-management and the role of the nurse (education)
Health literacy – 90 million Americans do not understand
Results in patient harm, readmissions, and overuse of EDs
Language barriers have to be addressed – medical interpreters, more diverse staff
Where do the problems arise?
Inadequate assessment, diagnoses, planning
Bad planning– lack of money, not realistic they can follow it or will, lack of resources, lack of awareness
Timing stressors – interruptions, understaffed, not evaluating patient understanding
Care coordination through
Nurse-patient communication/
interaction
Make care transitions seamless
Improve quality of life for patients with chronic illness
Work with others to improve quality of care and reduce health disparities
Therapeutic use of self = maintaining an effective, professional relationship
Therapeutic communication techniques
Use silence effectively
Accept others for who they are
Use broad openings; offer general leads
Make observations
Encourage perceptions
Restate
Seek clarification
Present reality
Voice doubt with a positive tone
Assess/evaluate with the patient
Cultural competence
When a healthcare provider develops the ability to function within the context of the cultural beliefs, behaviors, and needs of patients and communities
Justice
Equity
Diversity
Inclusion
culture
Shared values, ideas, attitudes, beliefs, norms, understandings, symbols, and practices of a group of people
Inclusion of patient’s culture/diversity
Respect for patient needs and preferences
Sensitivity to spiritual dimensions of care
Assess how they define health and wellness
Assess access to care
Assess patient resources – financial and human
Awareness and recognition of health care disparities
Racial & Ethnic
racial adn ethnic minorities
minorities experience more disease, disability, and premature death compared to non-minorities. Infant mortality, CV disease, DM, HIV/AIDs, immunizations, cancer and cancer screening rates are examples where disparities exist in USA.
Disparities exist because of:
Legal/regulatory issues which make it difficult for people to receive equal care
Socioeconomic issues
Lack of facilities to provide care
Discrimination at the patient-provider level related to race/ethnicity
Bias – predisposed to a point of view
Ethnocentrism – belief that one’s group is superior to others
Prejudice – assumptions / negative attitudes of others
Stereotyping – unfairly labeling groups
None of this is new… it is just being brought to attention more
US is a diverse pop…
(race, ethnicity, gender identities, age, abilities, cultural background, religious and spiritual beliefs)
Some say … until “we” look more like the overall population of the United States, it will be difficult to serve the public and provide patient centered care
Core competency # 2:
Work in interprofessional teams
Caregivers should “cooperate, collaborate, communicate, and integrate care in teams to ensure that care is continuous and reliable”
The Core Competency: Work in Interprofessional Teams. In order to ensure that care is continuous and reliable:
Communicate
Coordinate
Collaborate
Delegate effectively and appropriately
Manage change
Apply principles of conflict resolution
WE HAVE TO WORK TOGETHER
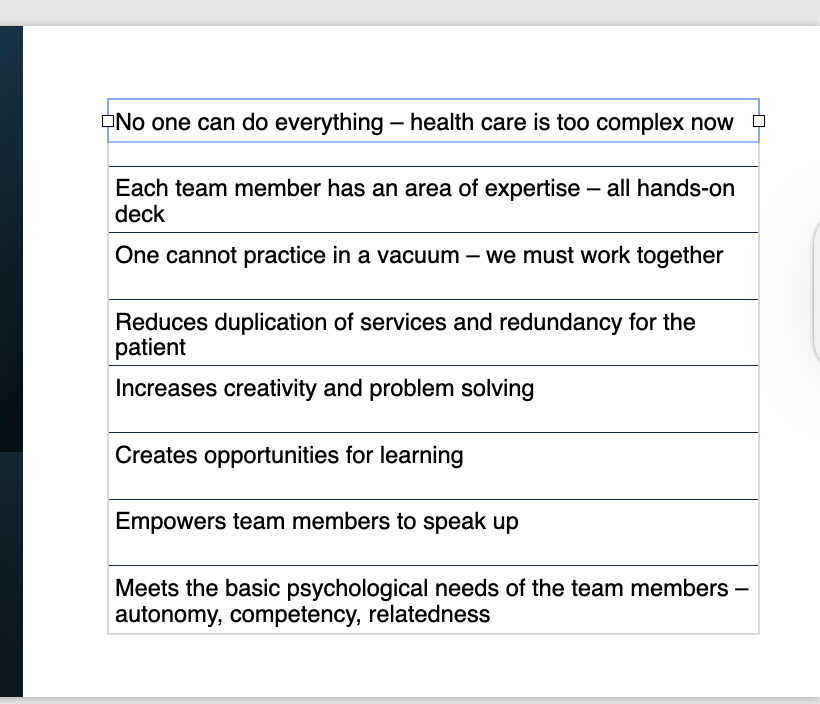
What do we know about teamwork and the work environment?
We know health care is growing more and more complex
Patients are sicker and care requires input from all disciplines
Not all teams are created equal – we must be able to work together
Job satisfaction is about more than just money – you need to feel appreciated, supported, and valued – feel like you make a difference
Organizational structure
Can be horizontal – flat – decentralized – considers input from staff
Can be hierarchal or bureaucratic – more likely to have top-down decision-making
Newer: Matrix organizational structure – focuses of departments and providing services within that department like cardiovascular service line that includes ICU, the Catheterization Lab, Respiratory Therapy, the Electrophysiology Lab, and Outpatient CV Rehabilitation services.
Nursing Organizational structure
Upper level = CNO or CNE or VP of Nursing Services
Middle level = Directors who supervise multiple units with a common function – Director of Critical Care Services
First level = Unit manager or supervisors
teamwork
why is teamwork hard?
We have PT, OT, SW, RN, NA, MD… all expected to work together when one discipline may not even fully understand the functions of the other
The more we understand each other’s role and what they bring to the table, the more teamwork shines and works in our favor
COMMUNICATION…
How many times do we ask the patient the same question?
How much work are we duplicating unnecessarily?
Poor Communications is 3rd root cause for sentinel event
sentiel event
unexpected harmful event in healthcare setting that results in psychological or physical harm (or death), not related to the natural course of the patient’s illness.
Examples of sentinel events…
Wrong-site surgery
Foreign body retention
Falls
Administering wrong medication due to ordering error
How could communication effect these events?
Occupational Therapist
This team member provides important services for patients who have impaired function and difficulty performing activities of daily living after a stroke, traumatic brain injury, or other serious injury. This team member helps the patient work within their disability to gain back function and independence.
Physical Therapist
This team member provides important services for patients who have impaired mobility and strength after a stroke or serious injury, as well as after many types of orthopedic surgery. This team member may teach a patient how to ambulate safely with a walker or cane or how to transfer safely from bed to chair.
Respiratory Therapist
This team member provides important services for patients who have trouble with breathing and airway clearance. This team member is trained to provide oxygen therapy, inhalation therapy (inhalers or nebulizers), ventilatory support, and even mechanical ventilation.
Physician’s Assistant
This team member can perform physical examinations, order diagnostic tests, diagnose and treat diseases, assist with procedures, and write for some prescriptions - but must always perform these care activities under the supervision of a physician.
Communication = sharing a message
Sender - Message – Receiver- Feedback
Mindful communication
Process by which actively aware individuals engage in meaningful communication (text vs email vs phone vs in-person)
One thing worse than poor communication, NO communication!
We must LISTEN more than we talk
Improving Team Communication
Effective communication takes practice and awareness
Structured communication methods
Improves team communication
Reduces communication barriers
Reduces communication errors
Organizational culture will have an impact
Respect is critical
Dissonant culture

Consonant culture
Functional
Effective – care, communication
Accept new staff/students/visitors, friendly, welcoming
Positive
Tools to help with communication, collaboration, and coordination
Evidence-based clinical pathways/Care bundles
Checklists
TeamSTEPPS
SBAR and CUS communication strategies
TeamSTEPPS
Communication: structured, clear and accurate exchange of info
Mutual Support: anticipate and support team members’ needs through accurate knowledge about their responsibilities/workloads
Leadership: maximize team actions by ensuring members are understood, information is shared, and resources are available.
Situation Monitoring: Process of actively scanning and assessing situational elements to gain information or understanding, or to maintain awareness to support the team
SBAR
Situation – what is going on with the patient?
Background – what is the clinical context?
Assessment – what do I think the problem is?
Recommendation – what would I do to correct it?
sbar not effective
use CUS
concerned
uncomfortable
safety issue
Improving Team Communication
Formal meetings
Should be held in a private place conducive to communication
Steps for conducting meetings
Attendance
Minutes
Pre-posted agenda
Goals of the meeting
Votes or consensus making
Start and end on time
Assigned tasks with due dates and people responsible
Opportunities to speak
Debriefing: Open discussion about nursing care.
Setting the stage
Description
Analysis
Take aways
Improving Team Communication
Assertiveness
Standing up for what you believe in
Not pushing / controlling
Confused with aggression
Use “I” statements
Nonverbal messages matter too
Listening
To patients, families, team members
Barriers to effective listening
Anxiety, stress
Distractions and interruptions
Workload
Fatigue and hunger
Lack of confidence
Burnout/Frustration/Upset
Healthcare Team Members:
Knowledge and Competencies
Key competencies:
Work with individuals of other professions
Use knowledge of one’s own role and roles of other professions to appropriately assess patient care needs
Communicate with patients, families, and communities
Apply relationship-building values and principles to perform effectively
Teamwork : Leadership
Effective leader:
Recognizes that work of team is critical
Should not focus on personal success or on success of any member
Emphasizes entire team effectiveness
Designated team leaders
Nursing team = leader is a RN
There does have to be a leader
A good leader:
Keeps the team on point – ID timeline/time constraints
Clarifies the purpose and the rules/guidelines of the team
Selects and/or orients and trains team members
Keeps the team focused on the task at hand
Reports up or down and updates the team as needed
Recognizes individuals and the team’s work
Is open to and supports other’s ideas
Resolves conflicts when they arise
Evaluates the outcomes of the team’s work
Accepts and provides constructive feedback
Facilitate group collaboration, communication, and delegation
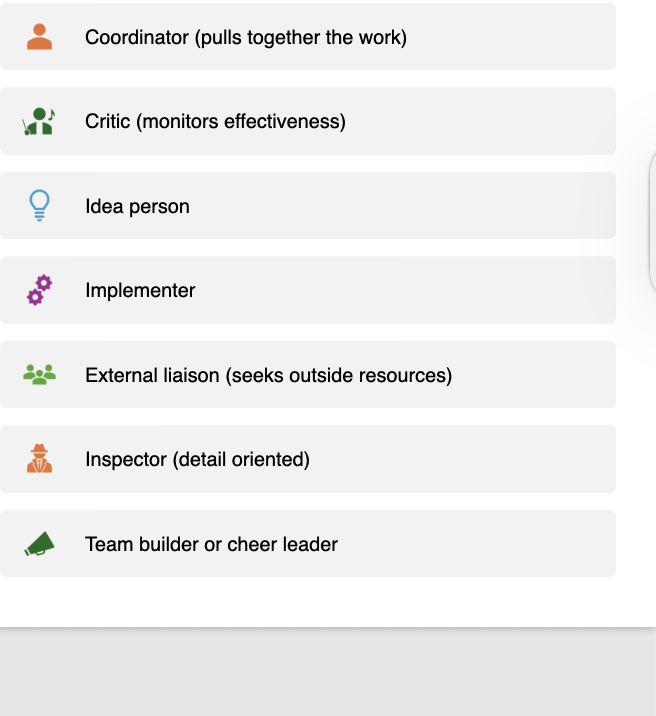
Formal and informal roles
within a team
Evaluating the effectiveness
of a team
Team size and composition
Team processes – clear goals and expectations, communication, conflict resolution strategies, leadership
Team tasks assigned appropriately
Ability to obtain resources and recognize the strengths of the team
Teams and Decision-Making
What is the issue?
What type of data are needed?
How complicated and substantial is the issue?
What are the solutions, and how many are there?
Can the outcome be acceptable with all standards?
Must consider pros/cons, ethical implications, and legal implications
Is the plan feasible?
collaboration
everyone has input, and decisions are made together
Requires compromise
Everyone has a say in the outcome
Requires mutual respect and good working relationships
Need quiet, private, neutral meeting place
Goal: Arrive at the best possible decision
Integral part of patient-centered-care
Tools to Improve Coordination
Use of Evidence-Based Practice guidelines for clinical protocols/pathways
INTERPROFESSIONAL ROUNDING with inclusion of the patient
An understanding of roles within the team
Support good documentation that is easy for others to locate
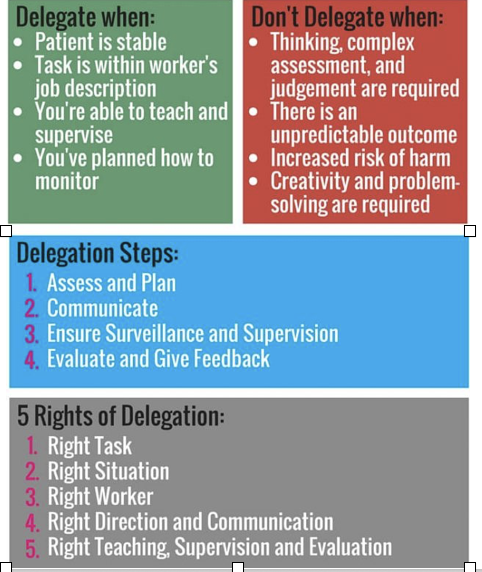
Delegation
Part of nurses’ daily work
Sharing responsibility by assigning tasks to others
Key terms
Supervision
Assignment
Transferring
Delegation how to
The delegated activity must be within the other persons scope of practice
The other person must be competent/able to perform the delegated task
Who can the RN delegate to?
Another RN
LPN/LVN
Unlicensed Assistive Personnel (UAP = CNA, PCA, PCT)
delegation for nurses
What is power?
When one healthcare provider has an advantage over another person
What is empowerment?
A feeling of increased personal achievement and autonomy
power type- Legitimate
(formal position like team leader or nurse manager)
Referent -type of power
(informal, from others’ recognizing leadership qualities)
informational type of power
(from having info others need)
Expert type of power
(expertise that is useful to guide others)
reward type of power
able to reward others if they do something)