PHARM EXAM #1 DRUGS + INFO
1/29
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
30 Terms
PSYCHIATRIC MEDS
Lithium
Chlorpromazine
Diazepam
Fluoxetine
MAOI (class of antidepressants)
NON-OPIOIDS (Analgesics)
Acetaminophen
NSAIDS —> Aspirin, Ibuprofen
OPIOIDS (analgesic)
Morphine
Tramadol
OPIOID ANTIDOTE
Naloxone
GI MED; LAXATIVE
Docusate (soften stool)
ANITBIOITCS
Rifampin
Gentamicin
Rifampin
ANTIMYCOBACTERIALS (TB)
ANTI-INFECTION; TB, RED-ORANGE, HEPA, contraceptives
TB/LEPROSY (bacteria on hands)
Pharm: suppresses protein synthesis
Adverse:
Body Fluids —> RED ORANGE
Avoid wearing contact lenses; harmful
HEPATOTOXIC —> monitor ALT, AST
Jaundice, anorexia, fatigue
GI SYMPTOMS
AVOID ALC, HISTORY W/ ALC
Avoid using w/ other hepatotoxic drugs
can be used as combo med w/ other TB drugs
Take contraceptives
PREGNANCY CATEGORY RISK C
Gentamicin
Aminoglycoside
Pharm: inhibits protein synthesis (30s)
Adverse Rec:
OTOTOXICITY (tinnitius, vertigo, ataxia, headache)
NEPHROTOXICITY
Creatinine: 0.6-1.3
BUN: >20 —> BAD
GFR: <90 mL/min —> BAD
I&O: <30mL/hr —> kidney distress'
Peak: 30min (IV);;; 1hr(IM) after admin
Trough: right before next dose
Muscle weakness
Respiratory failure
Contra: allergies, elderly, renal dysfunction
PREGNANCY CATEGORY D
DIAZEPAM
BENZODIAZEPINE; sedative/hypnotic, ADDICTIVE
Anxiety disorders, seizures, alcohol withdrawal symptoms, sedates
Pharm: enhances action of GABA in CNS
Admin: Take at BEDTIME/EVENING (grandma)
Effective WITHIN MINUTES
DONT SKIP DOSES
Adverse (ABUSED) → ***HIGHLY ADDICTIVE***
A-altered mental status
B- bradycardia (Low HR)
U - unable to walk/coordination (ATAXIA)
S- speech slur
E-experience hallucination/memory loss
D- decreased resp (low RR)
Contra: BENZO
B - BEERS —> avoid old people (toxic,
E - ETOH —> AVOID ALCOHOL, OPIOIDS, CNS DEPRESSION —> OVERDOSE, DEATH ***BLACKBOX****
N - No longterm use —> withdrawal, addiction
***TAPER OFF***
Z - zzz —> sedative, hypnotic, sedative (grandma) == NO FOCUS ACTIVITY (driving
O- overdose reversal (ANTIDOTE) —> FLUMAZENIL
Pregnancy Category Risk D
FLUOXETINE/PROZAC (happy pill)
Antidepressant; SSRI; 2-4 WEEK EFFECTIVE
Depression, OCD, BPD, Builimia, panic disorder
Pharm: selectively blocks reuptake of serotonin
Adverse (SSS)
SUICIDAL IDEATION (children, young adults) → eval for suicide/depression ***BLACKBOX***
Sexual Dysfunction (decreased libido) → decrease dosage
Serotonin Syndrome (SRI)→ start serotnin-receptor blockade treatment
S - sweaty, hot, fever
R - rigid muscle, restless, agitation (tremor)
I - increase HR (tachycardia),
Hyponatremia (>older pt taking diuretics) → get serum sodium lvl & monitor
LOW sodium concentration
WITHDRAWAL SYMPTOMS = headache, hallucinations, tremors, anxiety
GRADUALLY TAPER DOSE
Early→weightloss // Long-term → weightgain
Bruxism(grinding) → mouthgaurd
Rash → antihistamine
GI bleeding
Interactions:
CANNOT MIX W/ MAOI OR TCA
T2 WEEK FLUSH-OUT PERIOD
NSAIDS —> increase GI bleed
ST JOHNS WART —> increase seratonin syndrome (SRI)
Contra: allergy, children <7
PREGNANCY CATEGORY C
LITHIUM
PSYCHOTHERAPETUIC, NEPHROTOXIC
Acute Mania, controls manic episodes of BPD
Thep Range: 0.6-1.2 mEq
***DO NOT LIMIT SODIUM / WATER INTAKE***
Pharm: produces neurochemical changes in brain; protects against neuronal atrophy
Adverse (LITHIUM):
L- leukocytosis
I-increase in urine/thirst → drink 2k/3kmL
T-tremors (fine)
H-hypothyroid/heart arrhythmias
I-increase weight
U-upset stomach (N/V/D)
M-muscle weakness
NEPHROTIXIC: check BUN, CREATININE
HYPONATREMIA: low serum sodium → lithium toxicity
Lithium toxicity (WITHOLD MED)
Early: below 1.5 mEq/L → toxic
N/V/D, fine tremors, polyuria, thirst, slurred speech
Advanced: 1.5 - 2.0 mEq/L → serious toxicity
GI (N/V/D), confusion, coarse tremors, hypotension, ataxia
Severe: 2.0 - 2.5 mEq/L, OR greater than 2.5 → DEATH
Interactions: (AVOID)
Duiretics → lowers lvl of sodium (lithium toxic)
NSAIDS → increases renal absorption of lithium (toxic!!)
Anticholinergics → abdominal discomfort
PREGNANCY CATEGORY RISK D
CHLORPROMAZINE
PSYCHOTHERAPEUTIC, typical(1stgen), HEPATOTOXIC
Schizophrenia, BPD, N/V, tractable hiccups
DO NOT STOP ABRUPTLY —> withdrawal
Pharm: blocks dopamine receptors
Adverse:
Photosensitivity → sunscreen
Otherostaic hypotension → monitor BP
drowsiness, sexual dysfunction
Agranulocytosis → do WBC baseline
Neuroleptic Malignant Syndrome → HIGH FEVER/ HIGH EVERYTHING → STOP MED!!
Acute Dystonia → spams in tongue,neck,face → monitor for 5h-5days after admin
Tardive dyskinesia - involuntary face tics/lip smacking/grimacing
Parkinsonism (1st month) → monitor
Rigidity, shuffling gait, drooling, tremors, bradykinesia(slow movement
Akathisia → unable to stand still
Contra:
Anticholinergic agent
CNS dep
Levodopa
PREGNANCY RISK UNKNOWN
MAOI
ANTIDEPRESSANT CLASS; PSYCHOTHERAPEUTIC, HTN, HEPATOTOXIC, TYRAMINE, OTC (CAAN), 2 WEEK WASH
Pharm Act: increases norepinephrine, serotonine, dopamine
MAOI: (AVOID!!)
M - Massive Hypertension (HTN) crisis Risk → headache, agitation
A - AVOID TYRAMINE!! → INCREASES BP!!
NO ALC, CHEESE, MEETS, CHOCOLATE, avocado, banana
NO FERMENTED/PROCESSED THINGS
Start diet 2 weeks before med admin and continue for 2 weeks after med stop
O - OTC DRUGS = HTN CRISIS (2-week wash)
C - calcium
A - antacids
A - acetaminophen
N - NSAIDS (naproxin, ibuprofen)
O- Other Antidepressants (AVOID!!) → SSRI, SNRI, TCA → serotonin syndrome
2-WEEK WASH OUT;;; MAOI= CANT MIX!! (slowly taper off)
I - Increased suicide
PREGNANCY CATEGORY C
ACETAMINOPHEN (TYLENOL)
NON-OPIOID, NON-INFLAMMATORY, PAIN MED, **HEPATOTOXIC, ANTIPYRETIC, ANALGESIC
Pharm: slows down production of prostaglandins in CNS (AAAA)
A - acetaminophen (tylenol)
A - absence of bleeding (instead of NSAIDS)
use acetaminophen instead of NSAID bc NSAID = antiplatelet
A - AVOID ALC!!/ALC HISTORY → toxic liver
A - ANTIDOTE = acetylcysteine (aspirin)
Adverse:
LIVER DAMAGE → monitor ALT & AST
Overdose: A/N/V/D/S (48-72h)
ANTIDOTE: ACETYLCYSTEIN (oral/IV) → blocks acetaminophen; counters OD, reduce liver inj.
HTN → daily use, women→ monitor BP
Interactions:
AVOID ALC
WARFARIN (coumadin) → risk of bleeding
PREGNANCY CATEGORY B
IBUPROFEN/ASPIRIN
NSAIDS, NONOPIOD, ANALGEISC, REYES SYNDROME (ASPIRIN), NEPHROTOXIC, GI, SALICTYE (ASPIRIN), HTN, ASTHMA ;;; antipyretic, analgesia, dysmenorrhea (painful menstrual periods)
Pharm: COX-1 & COX-2 inhibitors
Adverse:
REYE’S SYNDROME - dont give aspirin to kids w viral illness (chicken pox, influenza) → liver dysfunction
Aspirin = Avoid kids
Alternative: ibuprofen, tylenol
GI: abd pain, heartburn nausea
Avoid peptic ulcer pt
black/dark colored stool
BLEED RISK (aspirin = anti-platelet)
stops thromboxane production
dont take w other anticoagulant
SALICYLISM → TINNITUS**, sweating, dizzy → check 8th cranial nerve
Give 1 week before surgery
Admin: discontinue 1 week b4 surgery TAKE W FOOD
Contra:
ASTHMA WORSENING
peptic ulcer disease
DONT GIVE TO CHILDREN PT (<19) THAT HAVE INFLUENZA/CHICKENPOX
PREGNANCY RISK CATEGORY D
MORPHINE
OPIOIDS (SEDATING) → vitals (loow&sloow)
ANALGESIA (MOD-SEVERE PAIN), COUGH SUPPRESSION, REDUCTION OF BOWEL MOTILITY
***EFFECTIVE IMMEDIATELY***
Pharm: mimics actions of natural opioids, endorphins, enkephalins;;; binds w mu receptors at opioid receptor sites
Address:
Respiratory depression: <12 RR → STOP MED!!
ANTIDOTE: NALAXONE!!
Constipation → increase fluid/fiber intake; prn stool softener
Orthostatic HYPOtension → sit/lie down,slowly change position, use call button for assist
Urinary retention → urinate every 4h
N/V/D → tolerance to med will build
ADMIN:
IV: ***SLOWLY*** ADMIN 4-5 MINS
FAST = DEATH
Burning (normal) → slower, dilute
Itchy (normal)→ antihistamine (benadryl)
REASSESS AFTER 15-30 MINS!!
Contra:
DEATH RISK: OD/RESP DEPRESSION
Advanced age: >70 y
Post-surgery
COPD, asthma
infants - resp depression
PREGNANCY RISK CATEGORY C
TRAMADOL
OPIOIDS; LOW & SLOW
Pharm: opioid receptor bind → blocks reuptake of norepinephrine & serotonin in CNS
Thep: moderate/severe pain
***EFFECTIVE IN 1HR***
Adverse:
Sedation, dizziness
H/N/V/C → give med w food
Urinary retention
Resp depression (rare) → if <12 RR, stimulate breathing
OR naloxone to restore RR
Seizures (rare)
Route: ORAL (absorbs within 1-2hr)
Interactions
AVOID MAOI, SSRI, SNRI, ANTIDEPRESSANTS → HTN CRISIS & SEROTONIN SYNDROME
St John’s Wort → increases sedative effects
PREGNANCY CATEGORY C
NALOXONE (NARCAN)
OPIOID ANTAGONIST/ANTIDOTE ;;
***REVERSES OPIOID EFFECTS***
**1-2 MINS EFFECTIVE
Pharm: blocks opioid receptors
Adverse:
Ventricular tachycardia, tachpnea
Increased RR, HR., BP
Abstinence syndrome → hypotension, vomiting, cramping in opioid-dependent pt
Adminster: (AIMS); REASSES EVERY 60MIN BC 1/2hr HALF LIFE
A - ABC (RR<12)
I - intervention oxygen (02<90%)
M- make HCP aware
S - second dose
FALLING ASLEEP WHILE TALKING TO U, UNAROUSABLE
PREGNANCY RISK CATEGORY D
DOCUSATE
LAXATIVE; STOOL SOFTENER → ****RELIEVES CONSTIPATION***; OTC;
may be nephrotoxic (caution)
Pharm: draws water in stool to make softer
Adverse: bitter taste, throat irritation, nausea, bad cramps
GI irritation → dont crush/chew enteric-coated tablets
Rectal burning
TOXIC MAGNESIUM LVL; electrolyte imbalance
Dehydration → monitor I&O, poor skin turgor,
8-10 glasses of water/day
Sodium absorption
Admin: don’t use for more than 1 week
Contra:
Acute surgical abdomen
Appendicitis
Intestinal obstruction
Fecal impaction
Nociceptive pain
type of pain caused by damage body tissue; sharp, aching, throbbing
body’s ability to detect detect changes in env w/ stimuli that could damage skin
pain is subjective
RIGHTS OF MEDICATION ADMINISTRATION
PPDT RRAD EF
PATIENT
DRUG
DOSE
TIME
ROUTE
REASON
ASSESSMENT
DOCUMENTATION
EVALUATION
REFUSE
FOOD AND DRUG ADMINISTRATION PREGNANCY CATEGORIES (FDA; ABCDX)
CATEGORY A - proven no risk to humans
studies in pregnant people have not demonstrated risk in fetus during first trimester of pregnancy; no risk in later trimesters
***CATEGORY B*** - no evidence of risk to humans
animal studies does not demonstrate risk to fetus, but there is no adequate/well-controlled studies in pregnant women
CATEGORY C - risks cannot be ruled out in humans
animal studies shown adverse effects fetus; no studies in humans; benefits from use of drug in pregnant people may be acceptable despite risk
CATEGORY D - clear evidence of risk in humans
evidence of human risk; drug benefits from drug may be acceptable despite risk
CATEGORY X - contraindicated in human pregnancy (DO NOT USE)
evidence in humans and animals of fetal abnormalities/adverse reactions; evidence of fetal risk. The risk of use in pregnant woman OUTWEIGHS any benefit (DO NOT USE!!)
IF MED CAN SAVE MOM, USE THE DRUG!!
Medication order
MAKE SURE ALL ROUTE, TIME, DOSE, AND FREQ IS IN THE ORDER:
1200: propranolol 40mg po BID
MAKE SURE MED IS FOR RIGHT PATIENT
ODT
orally disintegrated on tongue
CRIES
FOR NEONATAL (birth-1year) POST-OP PAIN (6 points)
Crying (1)
Requires Oxygen Saturation
Increased vitals (2)
Facial expression (1)
Sleeplessness (2)
6 POINTS → neonate is in pain, GIVE ANALGESICS

FLACC
behavioral pain assessment scale (2months - 7yrs) for post-op pain (0-10)
face
legs
activity
cry
Consolability
0-relaxed/comfy
1-3 = mild
4-6 = moderate pain
7-10 = severe discomfort/pain
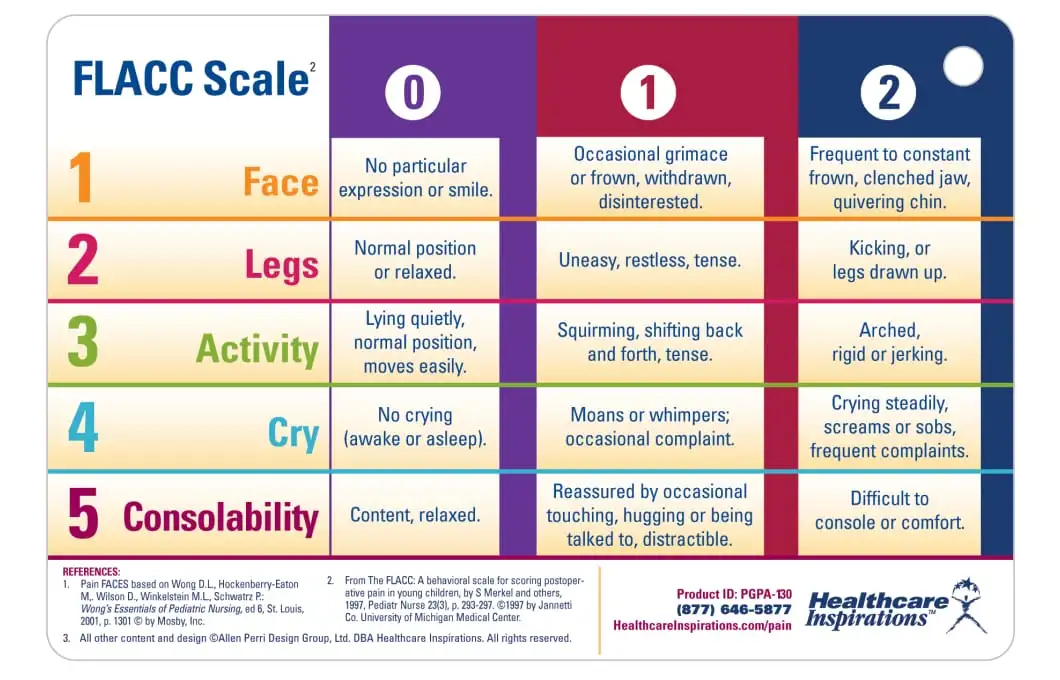
0-10
PAIN SCALE
Can be used up to kids who are 6 (usually 8 & older)
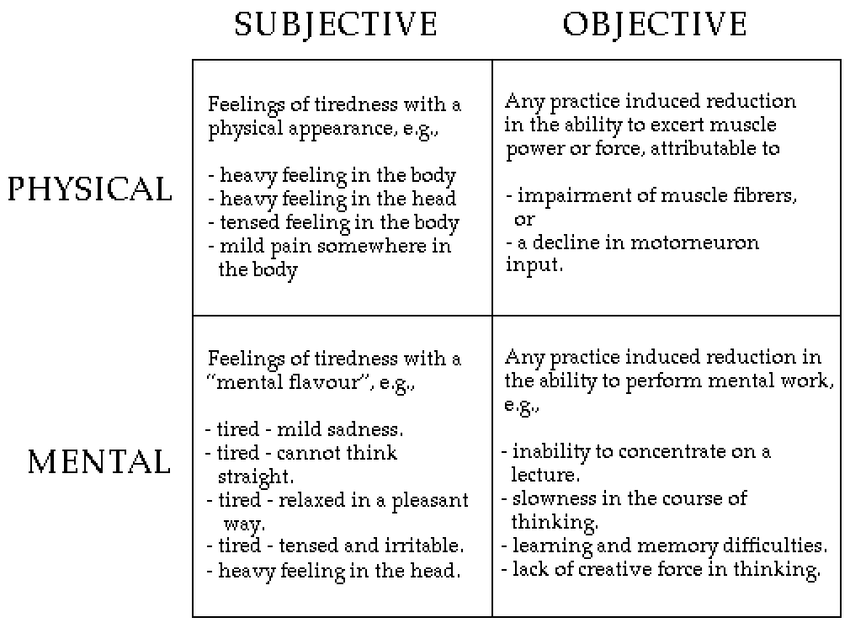
Objective vs Subjective Pain
obj: observations, vital signs, facial exp
sub: what patient tells u
Pt questions med that’s given to the (what’s that blue pill?)
Get more info from the pt first
What meds do u usually take?
Then explain the blue pill
(educate if dont wanna take)