Midterm- Ocular bacterial infections (I & II)
1/95
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
96 Terms
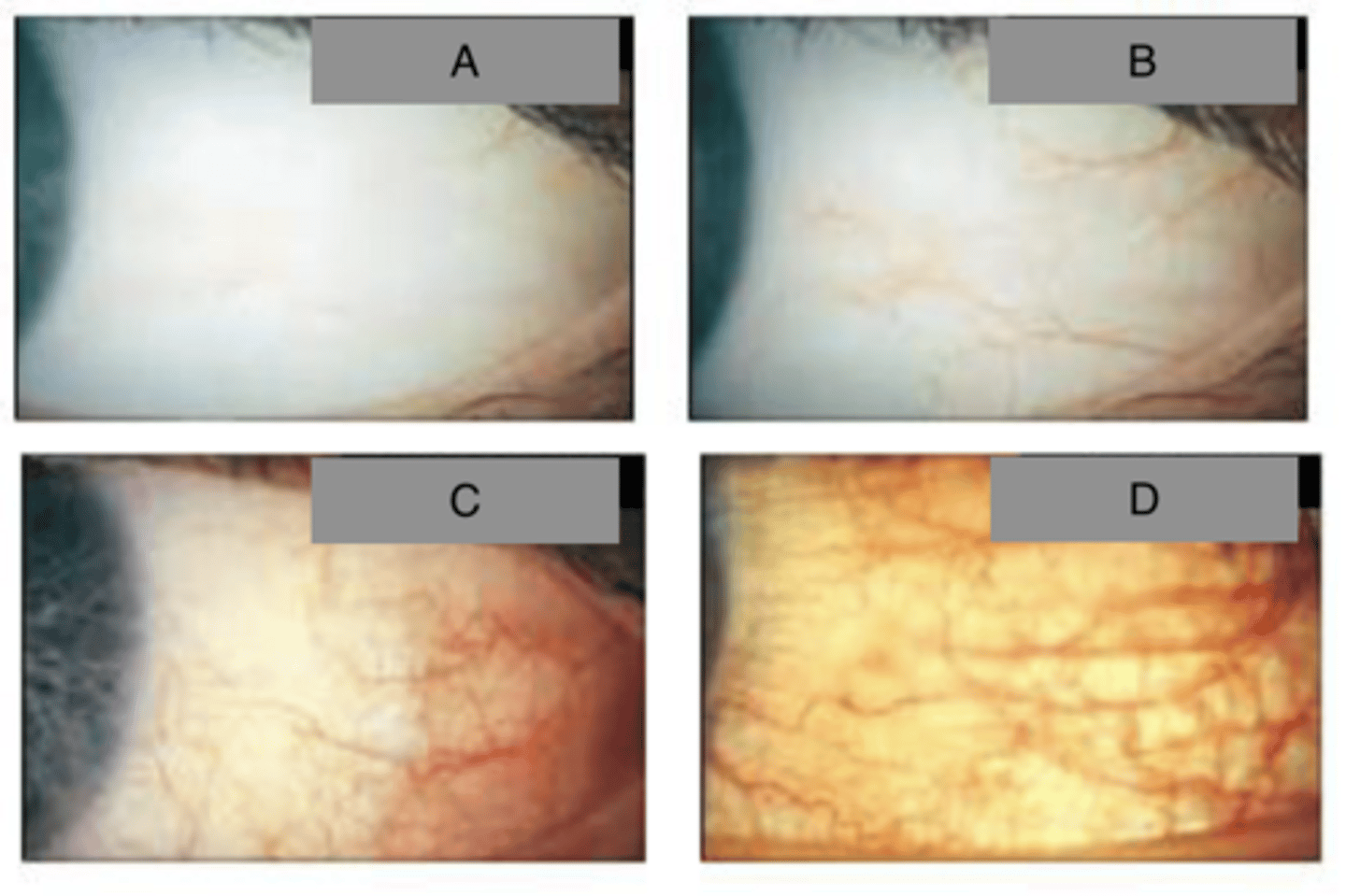
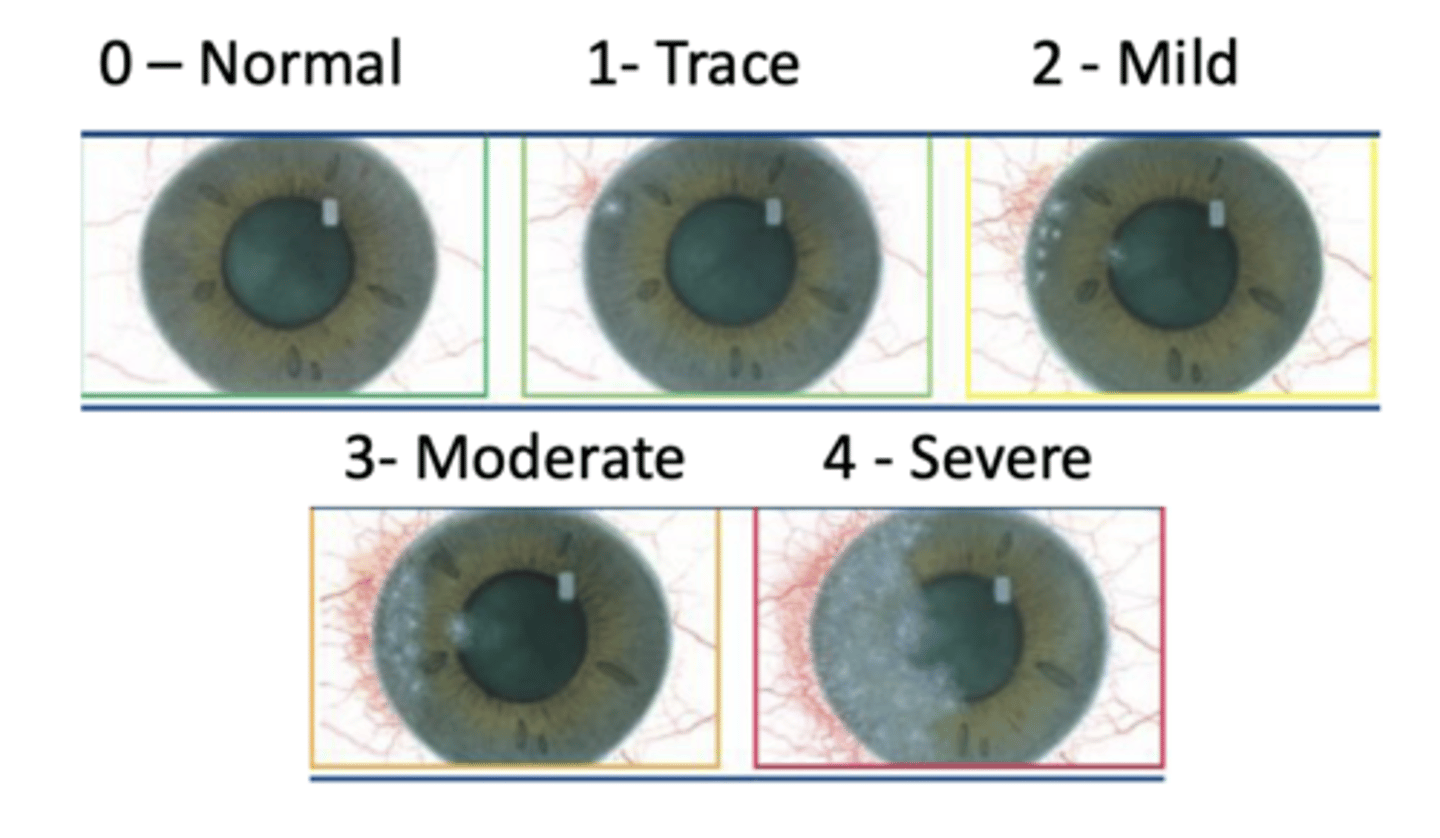
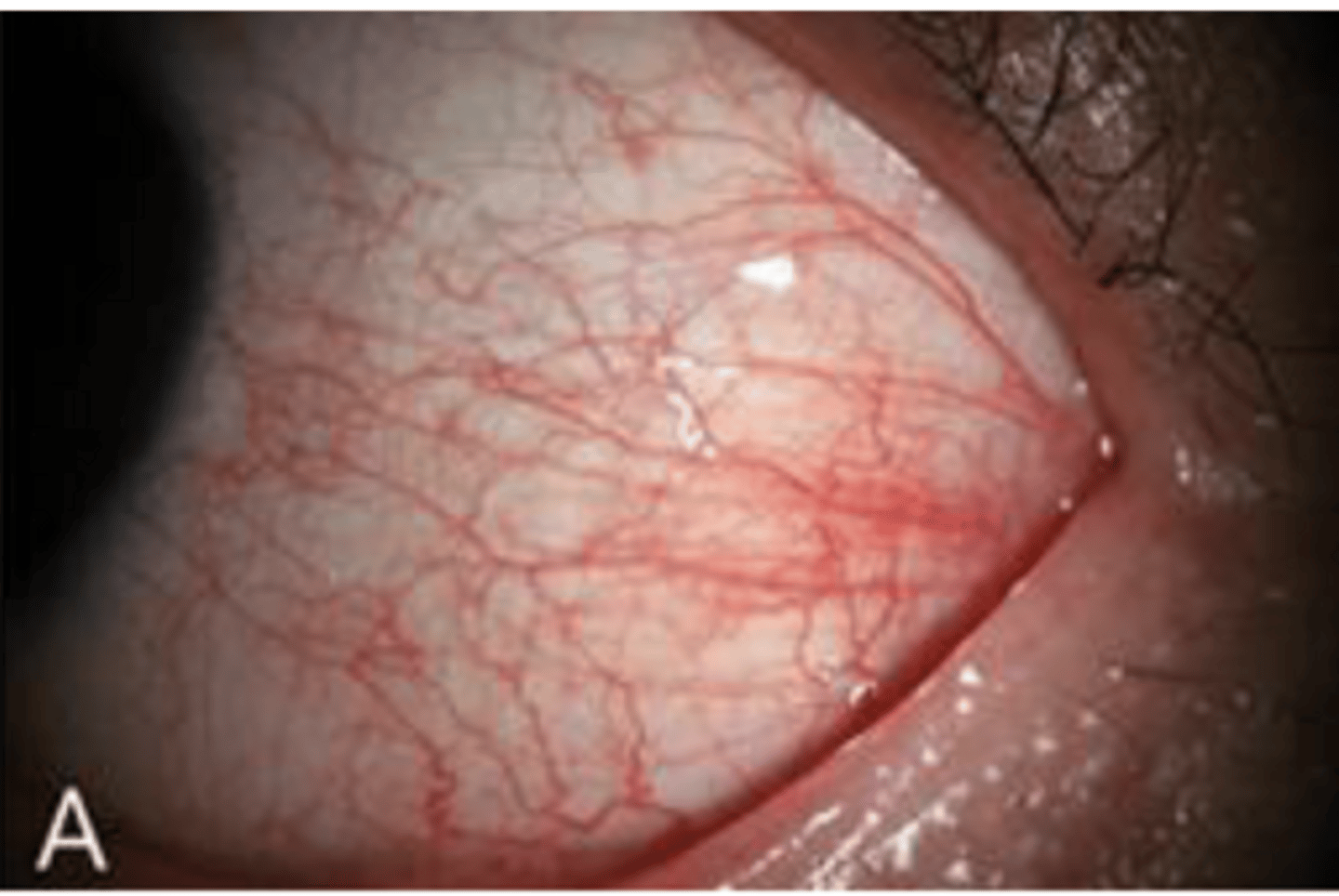
Bulbar conjunctival redness (hyperemia)
What is the name of redness of the non-keratinized tissue that covers the sclera?

Blanching with phenylephrine. This is important because its easy to confuse w sclera redness (which would be a deeper issue)!
How can you test if the redness is coming from the bulbar region of the conj?
A= 1; very slight,
B= 2; slight,
C= 3; moderate,
D= 4; severe
Grade the following bulbar conj redness (hyperemia)
Conjunctival papillae
What is it called when there is hyperplasia (increase in number of cells) of the epithelium?
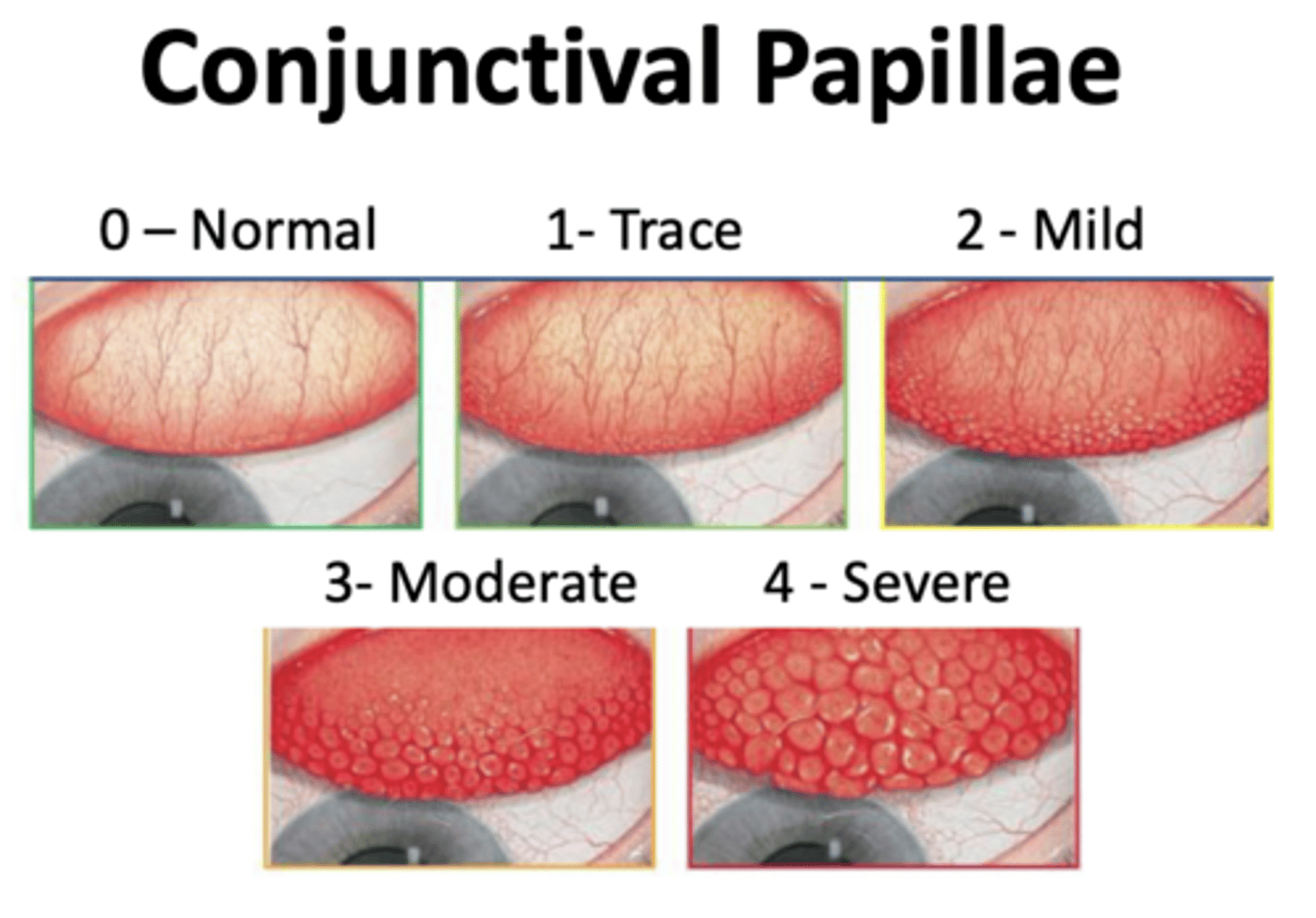
Allergic reactions or reaction to foreign body
What would cause Conjunctival papillae
Conjunctival Follicles
What is the hyperplasia of the lymphoid tissue; blood vessels will circle each follicle; looks like a grain of "grain of rice" below the conjunctiva
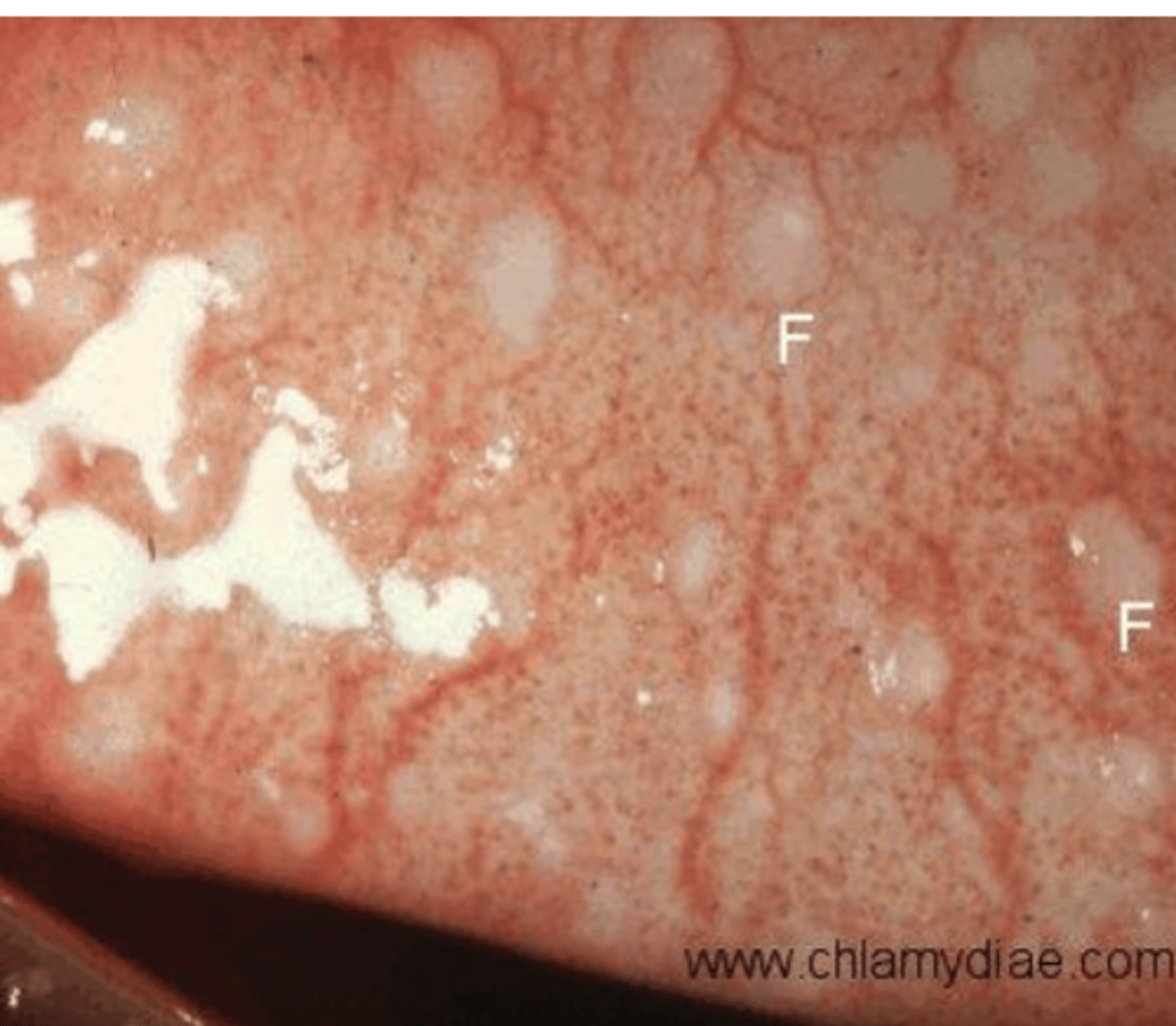
Conj follicles= Pale at center and red around the bumps,
conj. papillae= central red dot in the cells (central vessel) and pale at the base.
What is the difference in appearance of conjunctival follicles and conjunctival papillae
Conj papillae
What is more common conj. papillae or conj follicles?
Viral infections
What would cause conj. follicles?
Pseudomembrane= Mucus/debris that is attached to the surface of lids and looks like a new tissue, will not bleed with removal.
Membrane= A new fibrous tissue that is attached to the surface of lids & will bleed if you remove it
What is a pseudomembranve vs a membrane?
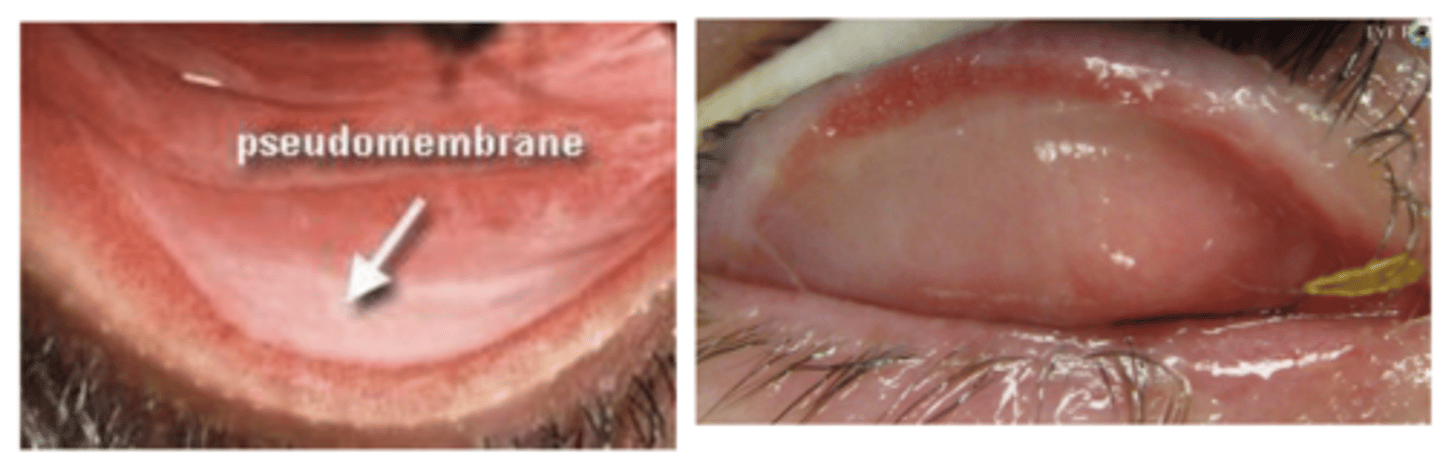
Bacteria (e.g. neisseria gonorrhoeae, streptococcus species, chlamydia trachomatis), and viruses (e.g. herpes simplex virus and adenovirus)
What causes conjunctival membranes/ pseudomembranes?
Swelling of preauricular node (lymph node in front of ear) due to increased number of immune cells
What is preauricular node (PAN)?
An accumulation of inflammatory cells in the corneal sub-epithelial stroma (looks like a round grey spot; e.g. ulcer)
What are corneal infiltrates?
Immune response to injury
What causes corneal infiltrates?
sterile and infection infiltrates
What are the 2 types of infiltrates?
Sterile= Small lesion (<1 mm), more peripheral, minimal epithelial damage, no mucous discharge, less pain and photophobia, no lid involvement, little anterior chamber reaction.
Infectious= Larger lesion (>1 mm), more central, significant epithelial defect (large stain), discharge, pain and photophobia, lid edema, anterior chamber reaction.
Describe sterile vs infectious infiltrates
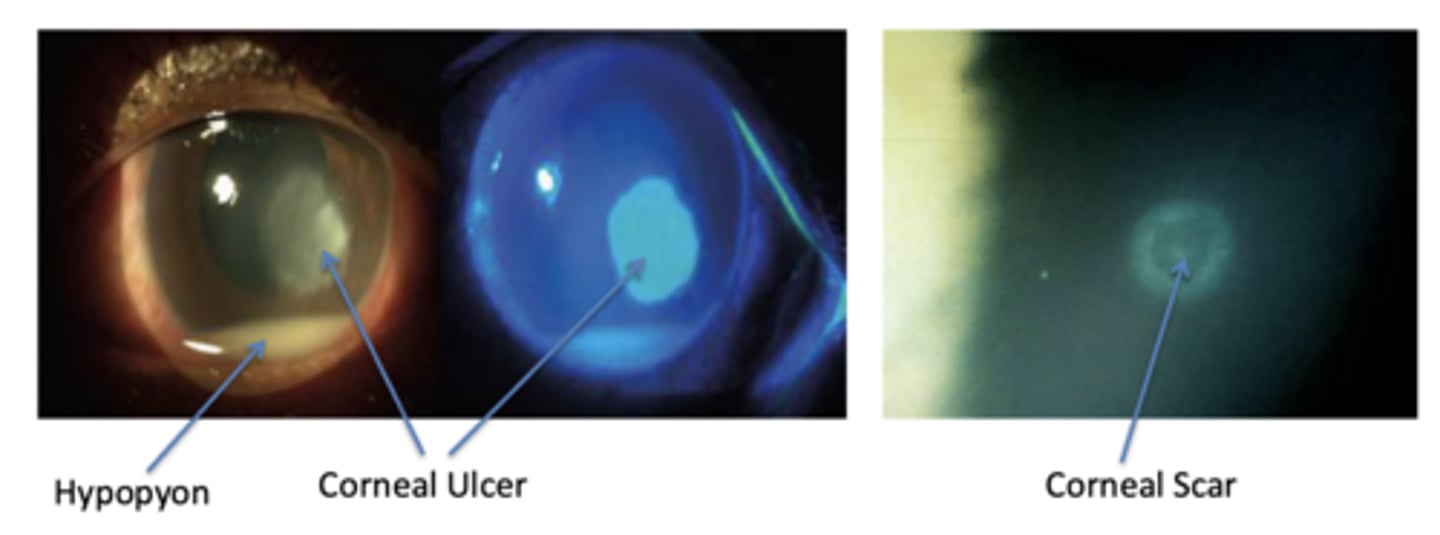
Corneal scars
What is a common misdiagnosis for corneal infiltrates?
Corneal scars have well defined margins vs. infiltrates w/ blurred margins
What is the difference between a corneal infiltrate and a corneal scar
How long has the spot been present? Previous infections?
What are some important questions to ask a patient to gauge the difference between corneal scars and infiltrates?
Full thickness epithelial loss with stromal necrosis and inflammation
What does a corneal ulcer look like?
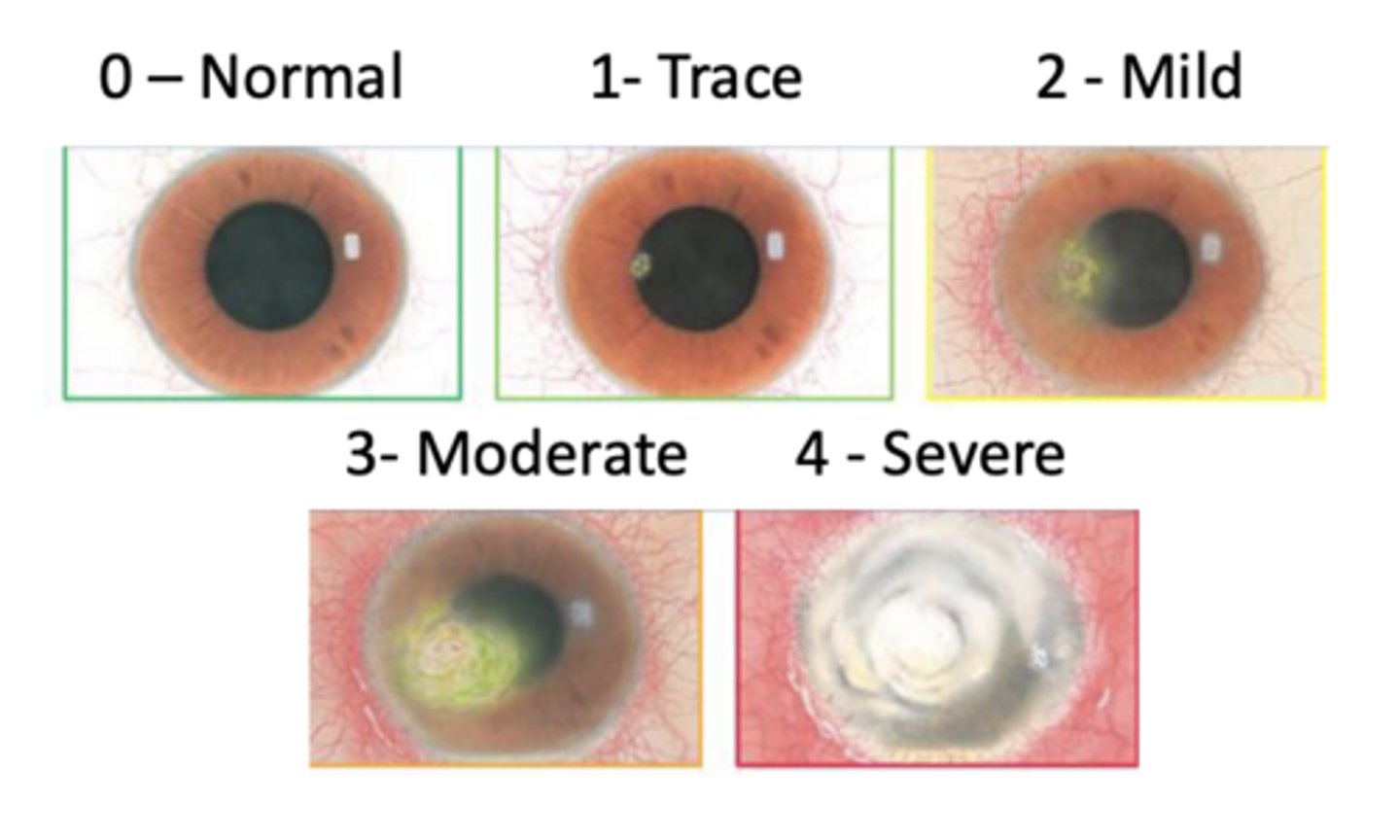
Central and paracentral
Where is a corneal ulcer typically located (and familiarize yourself with scaling pictured)
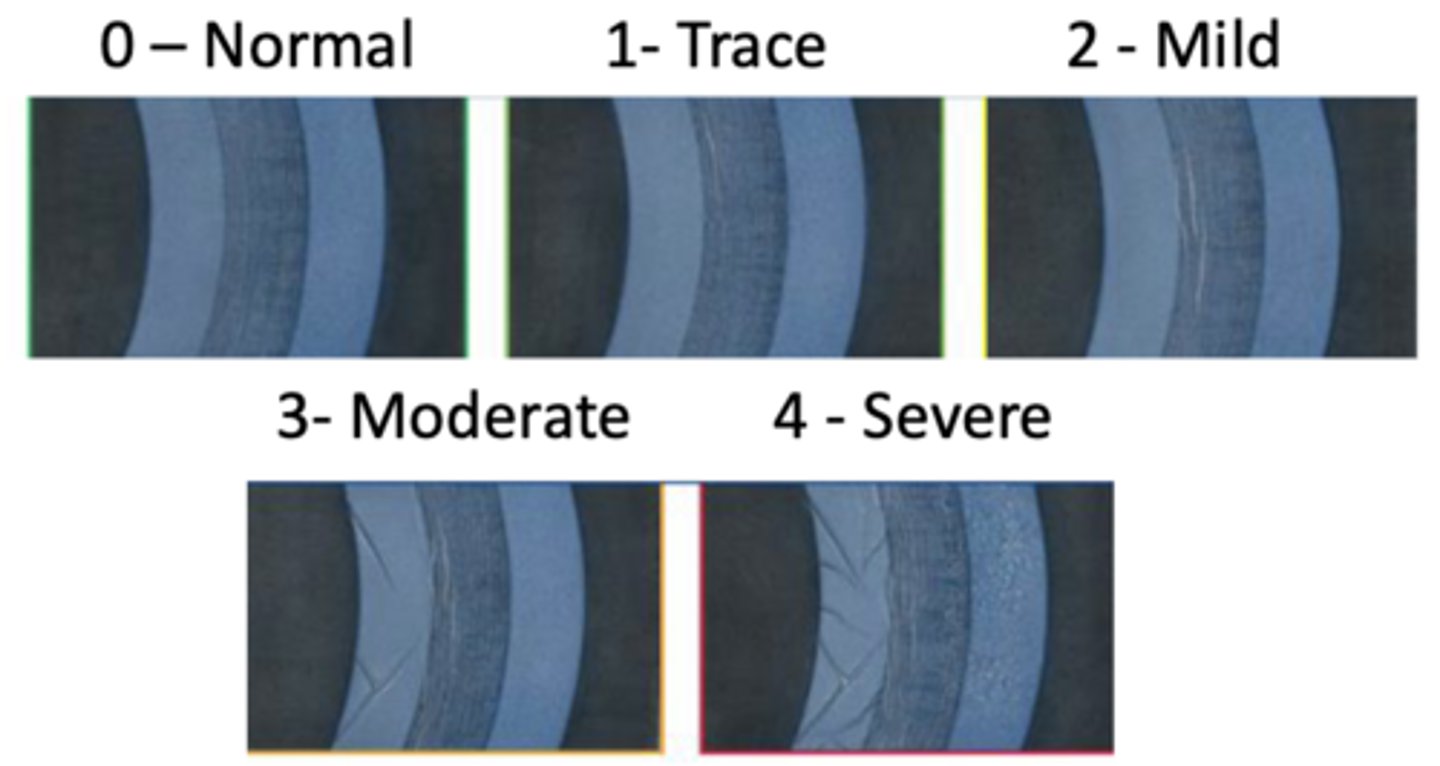
Corneal edema; infection, inflammation, endothelial cell death, ect.
What is the name for corneal swelling? What can cause this?
View in slit lamp to see that the width of the slit beam changes as you pass over the swelling
What does corneal edema look like (how can it be diagnosed)?
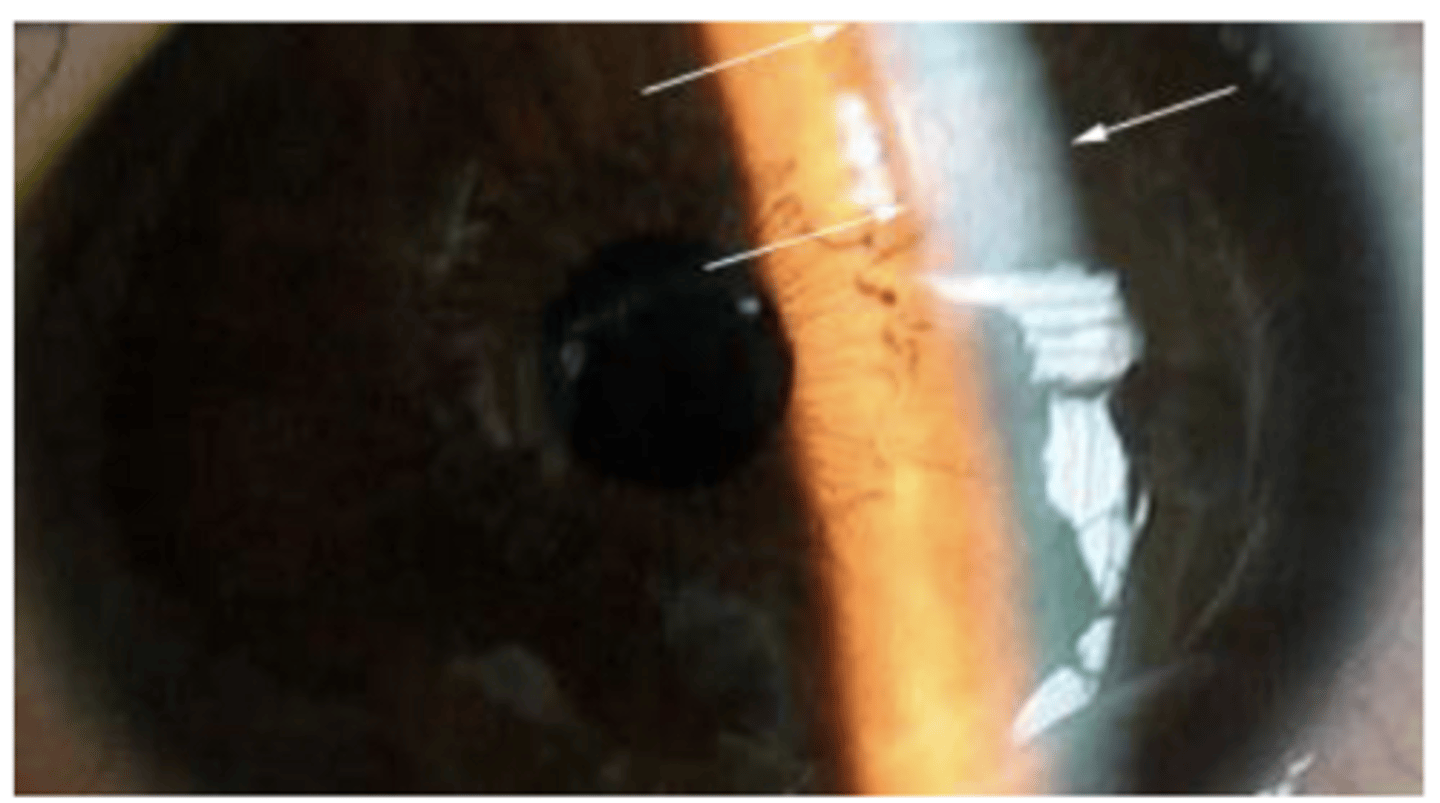
Folds= Long, straight, dark lines in the endothelium,
Striae= Fine vertical lines which tend not to branch in the posterior stroma
What are some characteristics of corneal edema?
1. Serous= Watery (clear) discharge,
2. Mucoid= Stringy/ropy white discharge,
3. Mucopurulent= Mucous + pus that is yellow, white, or green fluid (morning crust),
4. Purulent= Pus that is typically produced in large amounts.
What are 4 types of discharge?
Serous= viral, mucoid= allergy, mucopurulent= bacteria, purulent= neisseria gonorrhoeae infection
What is the cause of the different discharges?
serous & mucoid
An allergic reaction would cause what kind of discharge?
mucopurulent & purulent
Bacterial infections would cause what kind of discharge?
mucoid & mucopurulent
Chlamydia would cause what kind of discharge?
serous
Viruses would cause what kind of discharge?
conjunctivitis
What is the name for inflammation of the conjunctiva?
keratitis
What is the name for inflammation of the cornea?
True
T/F- Infections are associated with inflammation, though
inflammation is not always associated with infections
Coagulase-negative staphylococcus, staph aureus, propionibacterium sp, diphtheroid (corynebacterium), streptococcus sp (more in children)
What is part of normal ocular flora?
An acute staphylococcal abscess of a lash follicle and its associated gland of zeis
What is an external hordeolum (type of infection, location)
Tender swelling of the anterior eyelid margin, usually with an eyelash at the apex
What does an external hordeolum present as?
Chalazion is non-infectious, a build up of cells, hard to the touch, and bulges both under and on top of the lid
What is the difference between a hordeolum and a chalazion?
staphylococcus aureus
What bacteria is typically associated with an external hordeolum (stye)?
Gram positive
Is staphylococcus aureus gram negative or positive?
gram positive bacteria (they have cell walls )
What kind of bacteria is more susceptible to antibiotics?
topical antibiotics, hot compress, epilation of the affected gland (lash removal), and in severe cases oral antbiotics
How can you treat an external hordeolum?
DO NOT POP! This can cause preseptal cellulitis (bacterial infection of the entire eyelid)
Other than medication, what should you instruct a patient to do when they have a stye?
Mucopurulent or purulent discharge, crusty eyelids, redness, foreign body sensation, begins unilateral and becomes bilateral, papillary reaction, conjunctival injection (redness), - PAN
How does simple bacterial conjunctivitis present?
1. Haemophilus influenza- Gram negative,
2. Streptococcus pneumoniae- Gram positive
What are 2 common simple bacterial conjunctivitis conditions in kids?
1. Streptococcus pneumoniae- Gram positive,
2. Staphylococcus aureus- Gram positive,
3. Pseudomonas aeruginosa- Gram negative
What are 3 common simple bacterial conjunctivitis conditions in adults?
Pseudomonas aeruginosa
What bacterial infection is common in CL wearers?
Kids
Are bacterial conjunctivitises more common in kids or adults?
Both eyes should be treated even if it starts unilaterally, eyelids should be cleansed, topical antibiotic will help resolve faster
How should you treat simple bacterial conjunctivitis?
10-14 days on its own, 5-7 days with topical antibiotic
How long does it take simple bacterial conjunctivitis to resolve?
Gonococcal keratoconjunctivitis
What is a severe bacterial conjunctivitis?
Diffuse, thick purulent discharge, redness, irritation, edematous eyelids, conjunctival hyperemia, pseudomembrane, +PAN, keratitis, corneal ulcers
How does gonococcal keratoconjunctivitis present?
neisseria gonorrhea
What causes gonococcal keratoconjunctivitis?
gram-negative bacteria, can penetrate an intact cornea
Describe neisseria gonorrhea
Refer pt for a chlamydial infection! Pt will be hospitalized and an eye will be cultured is there is corneal involvement.
Before sending them to hospital, do a saline wash & topical antibiotics
How should you treat gonococcal keratoconjunctivitis?
Obtained either during birth (passage through mothers vagina) or a cross infection in the neonatal period.
Presentation occurs 3-5 days after birth; eyelid edema, mucopurulent discharge, about 1/2 have corneal involvement that can lead to ulcers and perforations
How can you obtain neonatal gonococcal keratoconjunctivitis? How does it present?
Topical or systemic antibiotic, refer for chlamydial infection screening
How can you treat neonatal gonococcal keratoconjunctivitis?
neonatal conjunctivitis, postoperative eye infections, severe long-standing conjunctivitis, suspected fungal eye infection, corneal ulcers that aren't obviously herpetic, hyperacute conjunctivitis, membraneous conjunctivitis,
What are some instances where micro lab studies are mandatory?
How long has this beem going on? Any history of infection/ if so what was used to treat in the past? Does it feel like theres a foreign body/ bump on the inside of the lid? Is it hard to the touch or painful? Is there an eyelash protruding from the bump?
A 30-year-old non-contact wearer presents with a red, irritated eye (pictured). What questions would you ask your patient to help
you with your diagnosis?

Grade 3
What grade would you assign to this conjunctival hyperemia?
External hordeolum (stye), and treat with topical antibiotics, warm, compresses, instruct not to pop, remove eyelash, and if severe consider oral antibiotics
For this case (red bump + conj hyperemia), what would be the top diagnosis and treatment?
mucopurulent, bacterial conjunctivitis, haemophilus influenza or Streptococcus pneumoniae, topical antibiotics, 5-7 days
The pictured 4-year-old, non-contact lens-wearing male presents with complaints of eye irritation and the following ocular presentation. What type of ocular discharge is this? What's your differential diagnosis? What is the most likely offending microorganism? What is the best treatment plan for this patient? How long will it likely take for this patient's condition to resolve if treatment is initiated?

Chlamydial conjunctivitis
What is the most commonly transmitted sexual disease in the US?
Typically no symptoms for months-years, follicular conjunctivitis (inferior palpebral or bulbar conjunctival), peripheral corneal infiltrates, corneal vascularization, +PAN, stringy mucus discharge, UTI
How does chlamydia normally present?
Chlamydia trachomatis
What bacteria causes chlamydia?
gram negative, egg/ovoid shape, obligate intracellular parasite
What are some characteristics of chlamydia trachomatis?
Serotypes D through K
What strains of chlamydia cause adult chlamydial conjunctivitis?
a distinct variation within a species of a bacteria or a virus
What is a serotype?
Oral antibiotics, treat partner, warn pt chronic untreated chlamydia can result in infertility/sterility & blindness due to corneal ulcers
How should you treat chlamydial conjunctivis?
Trachoma
What is the leading cause of preventable infectious blindness in the world
Found in third world countries with poor sanitation/ crowded conditions; chlamydia trachomatis bacteria
What typically causes trachoma?
Gram negative with egg/ovoid shape
What are characteristics of chlamydia trachomatis?
Serotypes A, B, Ba, & C
What strains of chlamydia trachomatis cause trachoma?
1. Superior palpebral follicles, SPK (corneal staining), purulent discharge, + PAN.
2. Additional superior palpebral follicles or papillary hypertrophy, superior corneal infiltrates, pannus, and limbal follicles.
3. Follicles and scaring of superior palpebral conjunctiva.
4. No follicles with extensive conjunctival scaring.
**Late complications: severe dry eye, trichiasis, entropion, keratitis, Herbert pits, corneal scaring, corneal ulcers
What are the stages of trachoma?
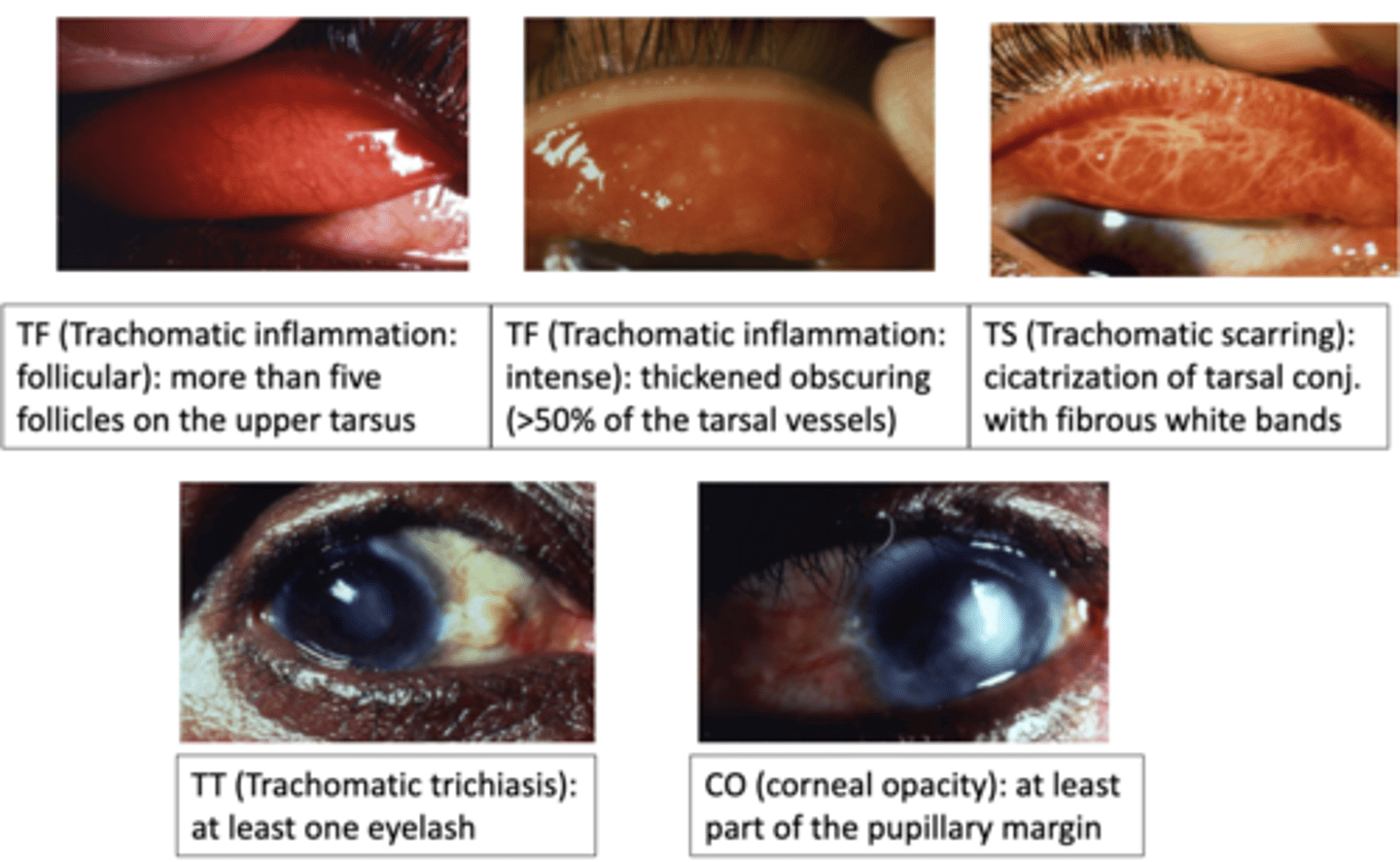
Oral antibiotics & SAFE (Surgery for Trichiasis, Antibiotics to clear infection, Facial cleanliness, and Environmental improvement to limit transmission)
How can we treat trachoma?
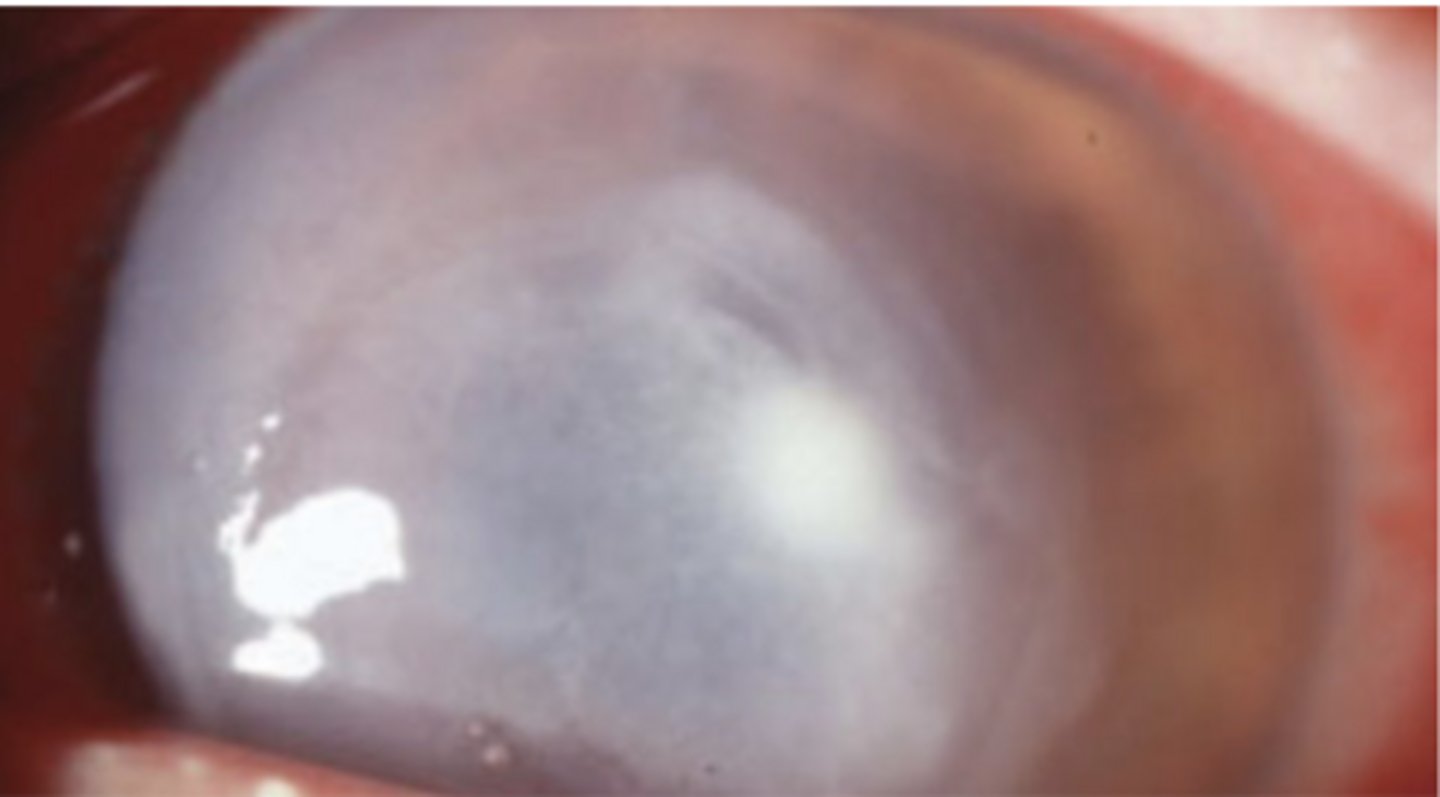
Infectious corneal ulcer
What is an infection of the cornea that may result in a large geographical area of epithelial loss?
Ulceration of the cornea that occurs without microbial influence (typically due to bacterial toxin & needs testing to confirm)
What would a sterile corneal ulcer describe in comparison to the infectious corneal ulcer?
Consider it bacterial until proven otherwise!
How should you treat an infective keratitis?
Fluorescent stain!
How can you view a corneal keratitis?
Red eye, pain, photophobia, acute CL intolerance (overnight CL use), Mucopurulent discharge, corneal edema, anterior chamber reaction, an infiltrate or a corneal ulcer
How does bacterial keratitis present?
1. Commensalism= One organism benefits from the other
without affecting it,
2. Parasitism= One organism benefits while the other is harmed,
3. Mutualism= both organism benefit
What are the 3 types of bacterial relationships?
A dense, round-to-oval, focal white infiltrate with clear margins
What is the classic presentation of staphylococcus/ streptococcus?
Corneal ulcer with a gray, necrotic appearance that extends beyond the site of excavation
What is the classic presentation of pseudomonas?
Discontinue CL use, discard old CL's, topical antibiotics, pain meds, topical steroids after condition is under control, daily monitoring (until epithelial defect is closed), large (>1 mm) and central ulcers should be referred and cultured, if no improvement a corneal biopsy might be necessary
How should you treat bacterial keratitis?
1. Neisseria gonorrhoeae (gram neg),
2. Nesseria meningitidis (gram neg),
3. Corynebacterium diphtheria (gram pos),
4. Haemophilus influenzae (gram neg),
5. Listeria monocytogenes (gram pos)
What are some corneal bacteria that can penetrate the epithelia?
caused by a Staphylococcal antigen hypersensitivity (reaction against staph exotoxins and cell wall proteins with deposition of antigen-antibody complexes in peripheral cornea)
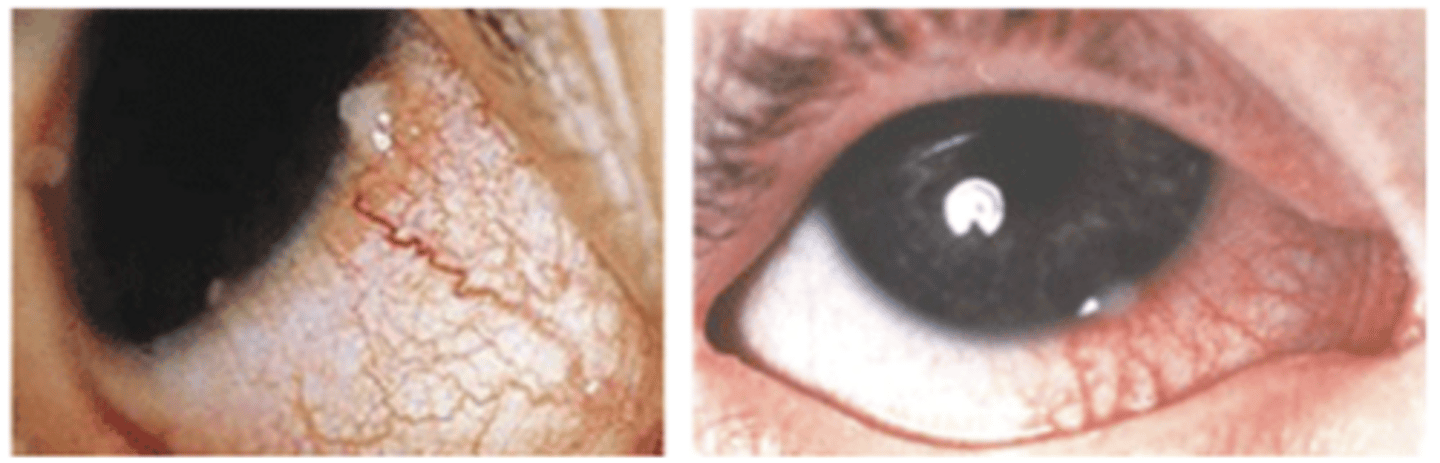
What is marginal keratitis?
middle aged pt, non-CL wearer, chronic eyelid disease (bleph), ocular discomfort, lacrimation, red eye, photophobia, infiltrates parallel to limbus, oval shape, 1-2 mm clear zone between infiltrates & limbus, blood vessels may dilate & extend towards the infiltrates in a bridging manner
How does marginal keratitis typically present?
Staphylococcus aureus on eyelid margin (negative culture/sterile bacteria from lesion)
What is a bacteria associated with marginal keratitis?
Treat with topical antibiotics/ steroid combo, eyelid hygiene, can self resolve in 3-4 weeks. LIKELY REOCCUR, may prohibit CL use
How should you treat marginal keratitis?
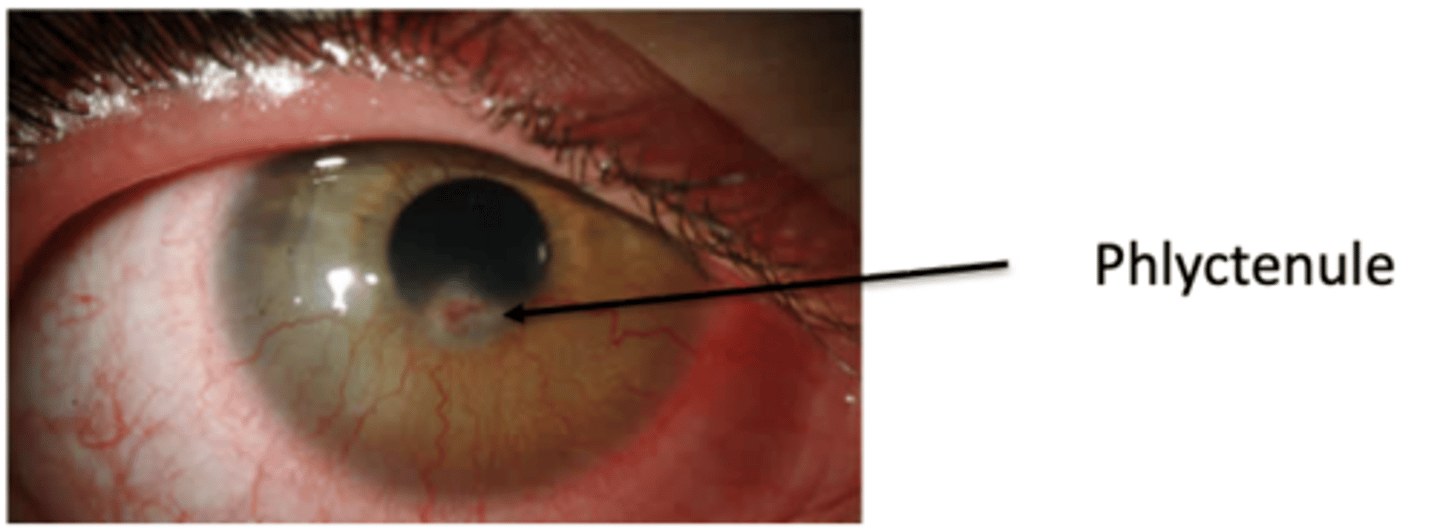
Phlyctenulosis; hypersensitivity to staph cell wall antigen (sterile)
What is an example of a marginal keratitis?
Watery eye, photophobia, small nodule (phlyctenule) with intense local hyperemia, if no phlyctenule there may be a triangular limbal based scar associated with superficial superficial vascularization and corneal thinning, bilateral
How would phlyctenulosis present?
An active infection should not use steroids so it doesn't suppress immune system! Once under control you can use steroids (why can you use combo on marginal keratitis?= because this is a hypersensitivity not an infection)
When should you use steroids/ stay away from them?
Endopthalmitis
What is the name of a condition that occurs from internal microbial ocular infection?
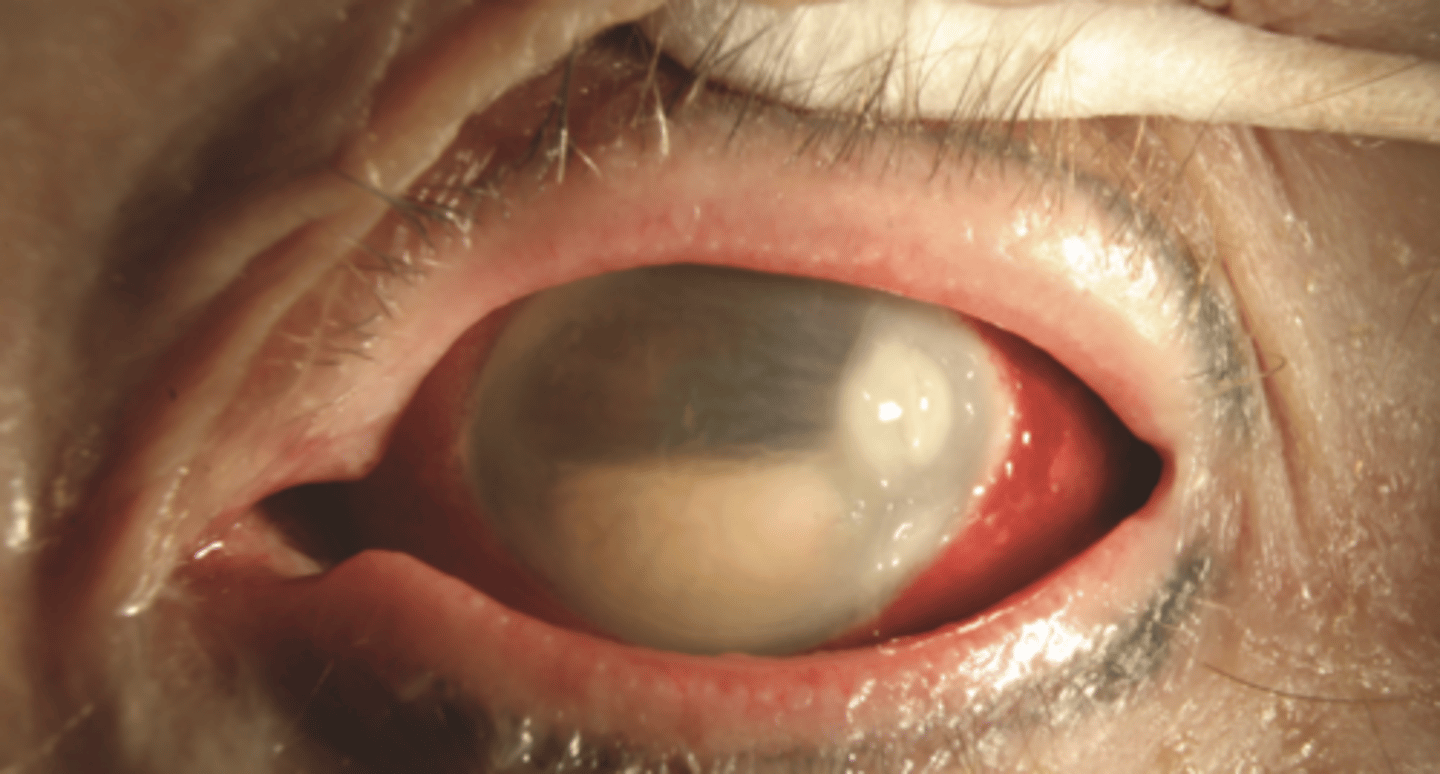
post-sx, traumatic injury, secondary to perforating microbial infection
What causes endopthalmitis?
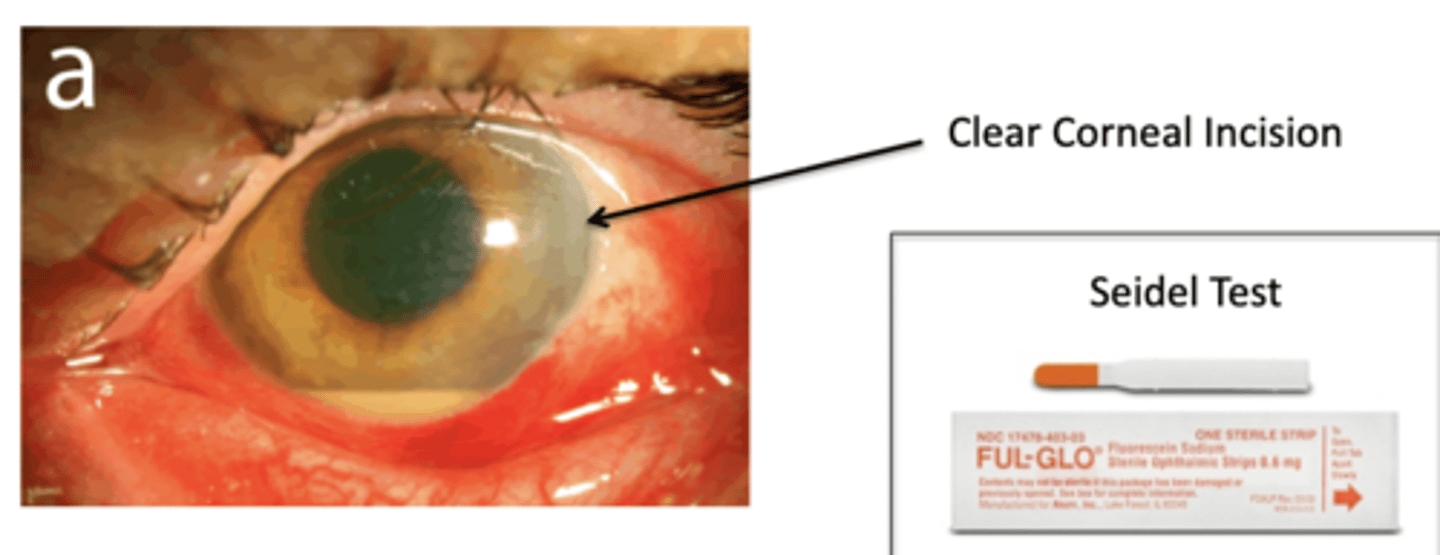
poor vision, conjunctival injection, pain, photophobia, + Seidel test, eyelid
edema, mucopurulent discharge, and hypopyon
How does endopthalmitis present?
You add in a numbing drop then dry off eye and add fluorescence to the limbal region. If you see aqueous starting to flow out of perforation and mix with fluorescence you likely have a endophthalmitis.
What is the seidel test?
aggressive topical antibiotic and systeminc antibiotics, topical steroids, and wound closure (CL, suture, glue)
How do you treat endophthalmitis