Exam 2: Muscles of the Shoulder Complex
1/60
Earn XP
Description and Tags
Pt. 2 of Shoulder Complex lecture
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
61 Terms
Axioscapular Muscles: Originate on spine, ribs, cranium = Insert on scapula & clavicle
Posterior muscles
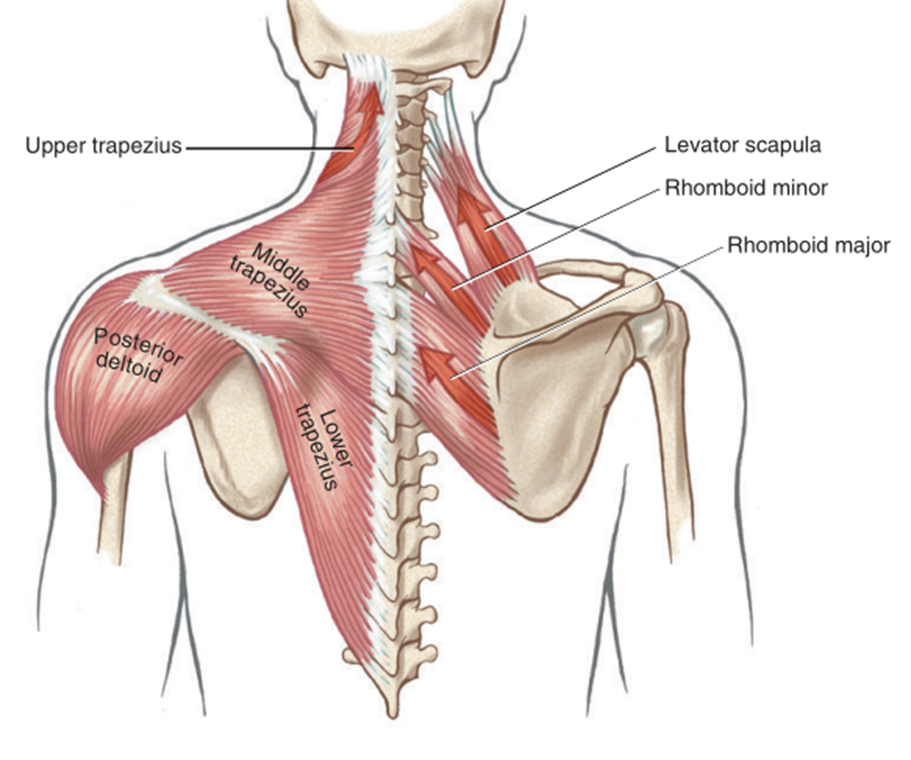
Trapezius (upper, middle, lower)
Levator scapulae
Rhomboids
Anterior muscles
Serratus anterior
Pectoralis minor
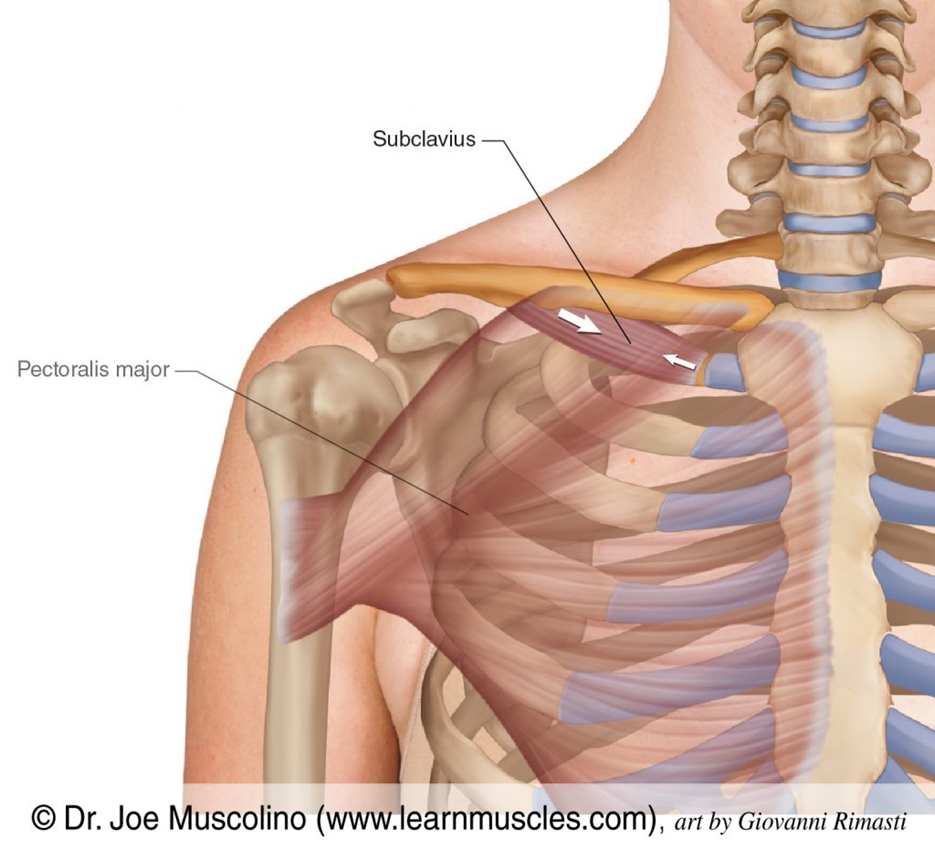
Subclavius
Axiohumeral Muscles: directly link axial skeleton & humerus
Anterior: Pectoralis major
Posterior: Latissimus dorsi *function on the scapula and GH joint vital
Trapezius 🛶
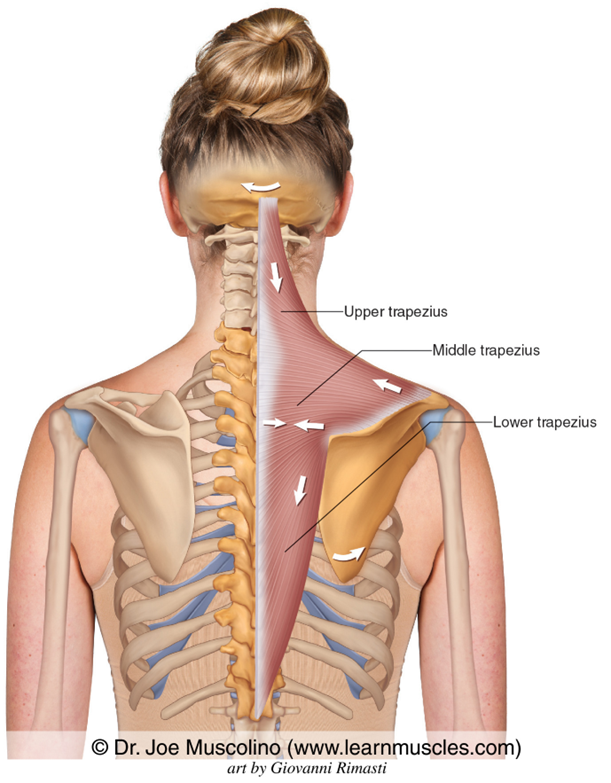
Purposeful activity: reaching for overhead object (upper/lower trapezius), rowing kayak or canoe (middle trapezius)
Upper trap
Middle trap
Lower trap
Innervation from: spinal part of CN XI (accessory) + ventral ramus C2-4
Levator Scapulae 🤷
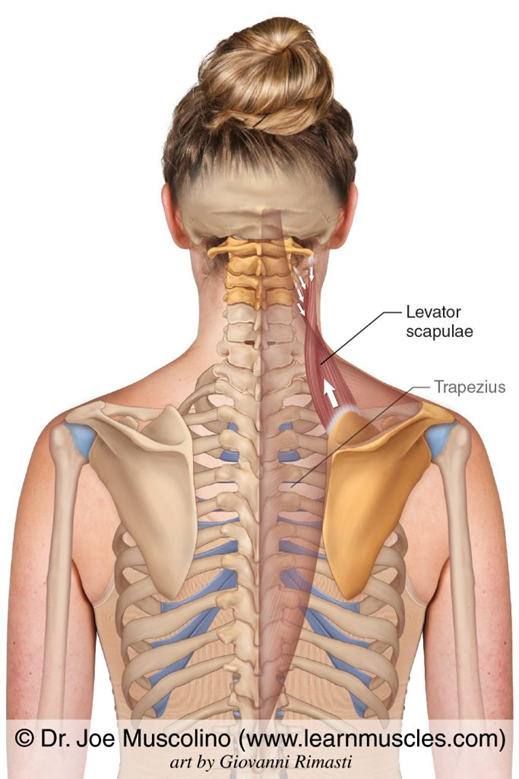
Elevates & downwardly rotates scapula, laterally flexes head & neck, rotate head & neck to same side
Muscle assisting scapula mvmt
Shrug shoulders
Innervation from: C3-4, dorsal scapular C4-5
Rhomboids 👖
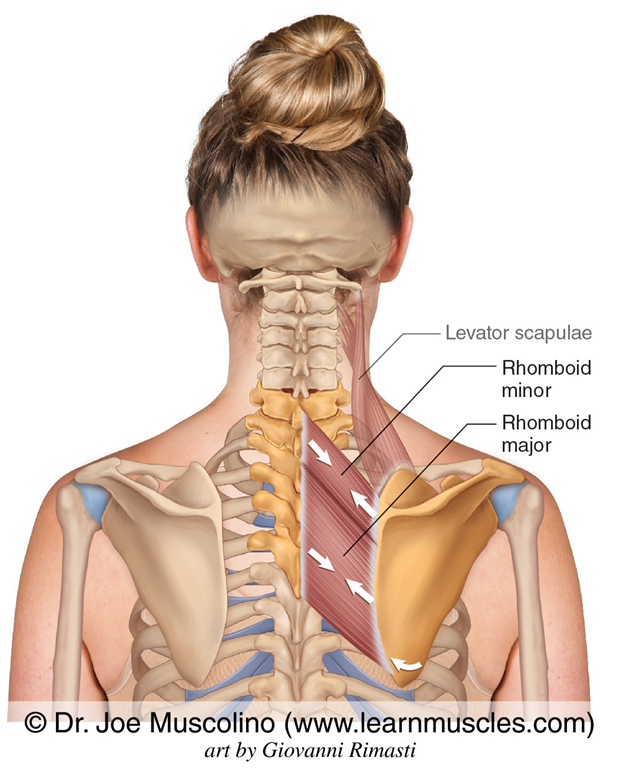
Adduct, elevate, downwardly rotate scapula (ST joint)
Reaching into back pocket 👖
Innervation from: dorsal scapular n. C4-5
Latissimus Dorsi ♿🧍
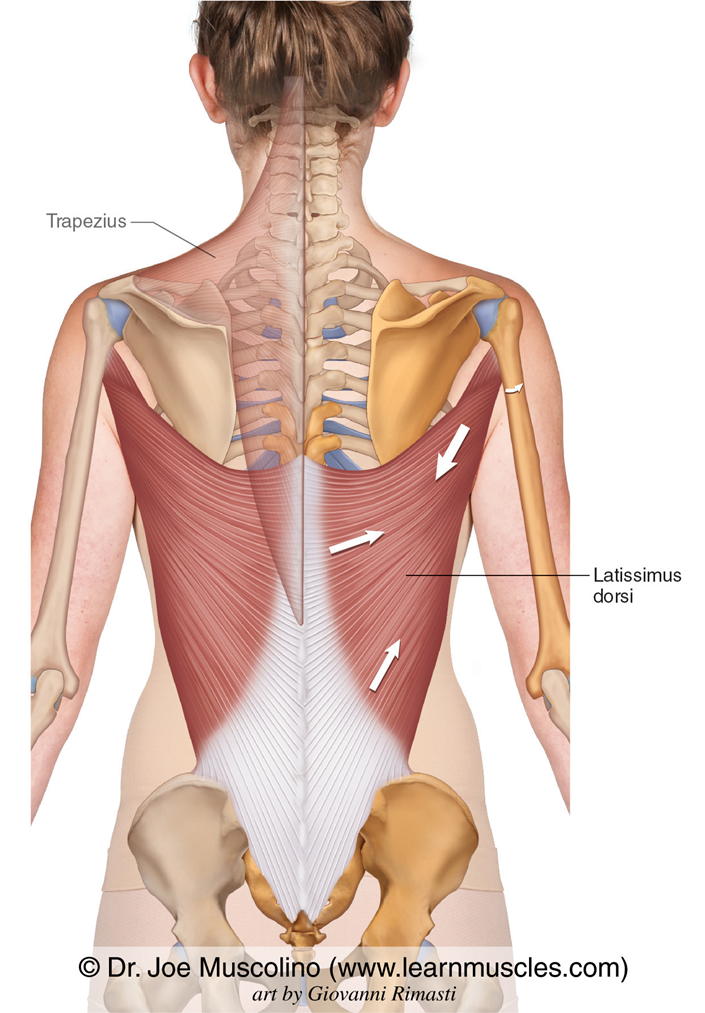
Purposeful activity: W/C mobility (propel forward), standing from sitting (push down on chair arms) ♿🧍
Extend, adduct, internally/medially rotate shoulder (GH)
Innervation from: Thoracodorsal n. C6-C8
Serratus Anterior 🚪
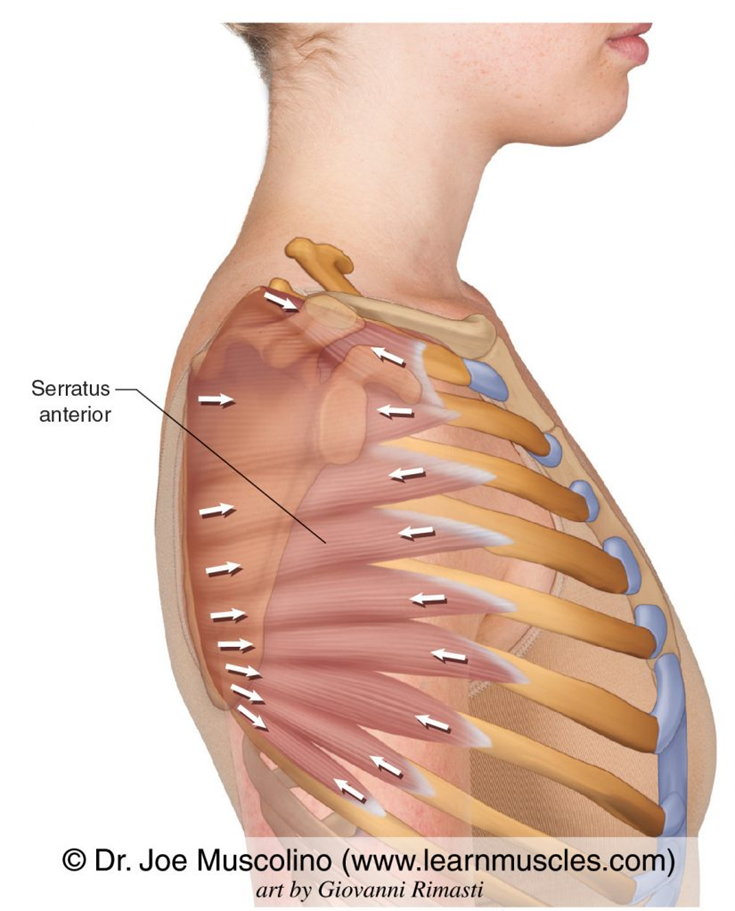
Pushing open heavy door🚪Protractor!
W/ origin fixed: abducts, upwardly rotates, and depresses scapula (ST joint). Hold medial border of scapula against rib cage.
W/ scapula fixed: elevate thorax during forced inhalation
Innervation from: long thoracic n. C5-8
Pectoralis Minor 😤🩼
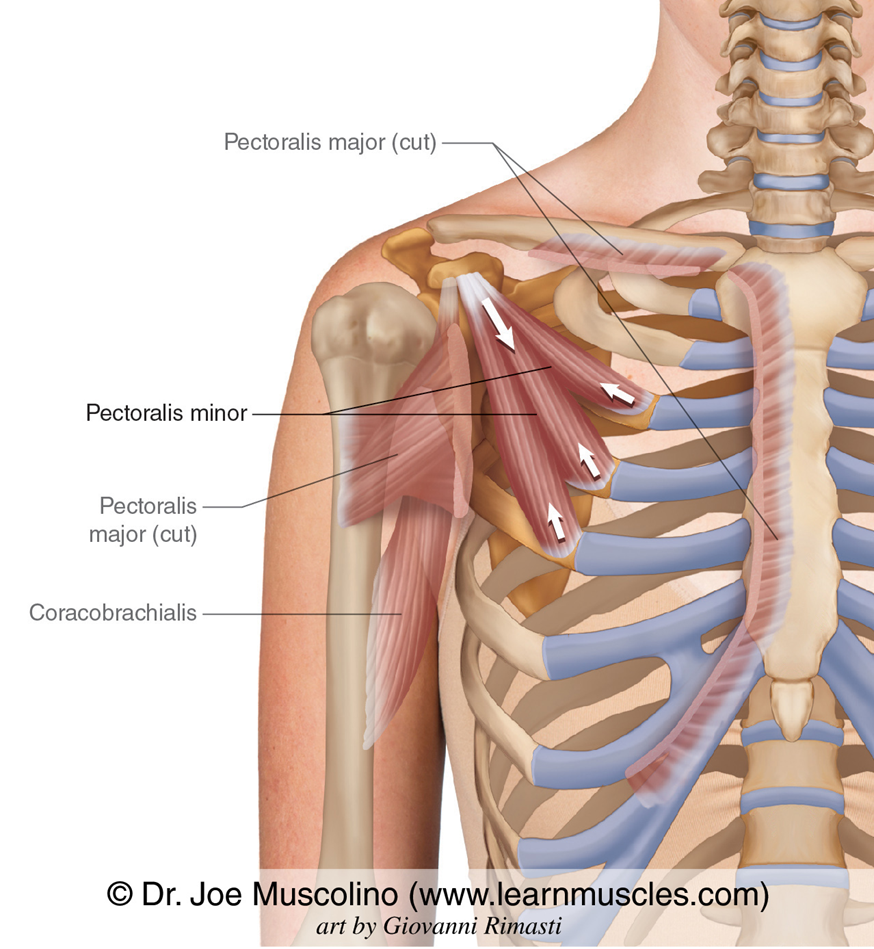
Taking deep breath, walk w/ crutches 😤🩼
Depress, abduct, downwardly rotate scapula (ST joint)
W/ scapula fixed: assist to elevate thorax in forced inhalation
Innervation from: medial pectoral, w/ fibers communicating to branch of lateral pectoral C6-C8, T1
Subclavius: Stabilizer
Action: anchors & depresses clavicle
Origin: junction of 1st rib & its costal cartilage
Insertion: inferior surface of middle third of clavicle
Innervation: subclavian nerve (C5,6) = closer to neck
Scapular muscles by fxn: Elevators 🤷

Primary movers: Upper trapezius & levator scapulae
Assist: Rhomboids
Scapular muscles by fxn: Protractors ✋🚪(anterior muscles)
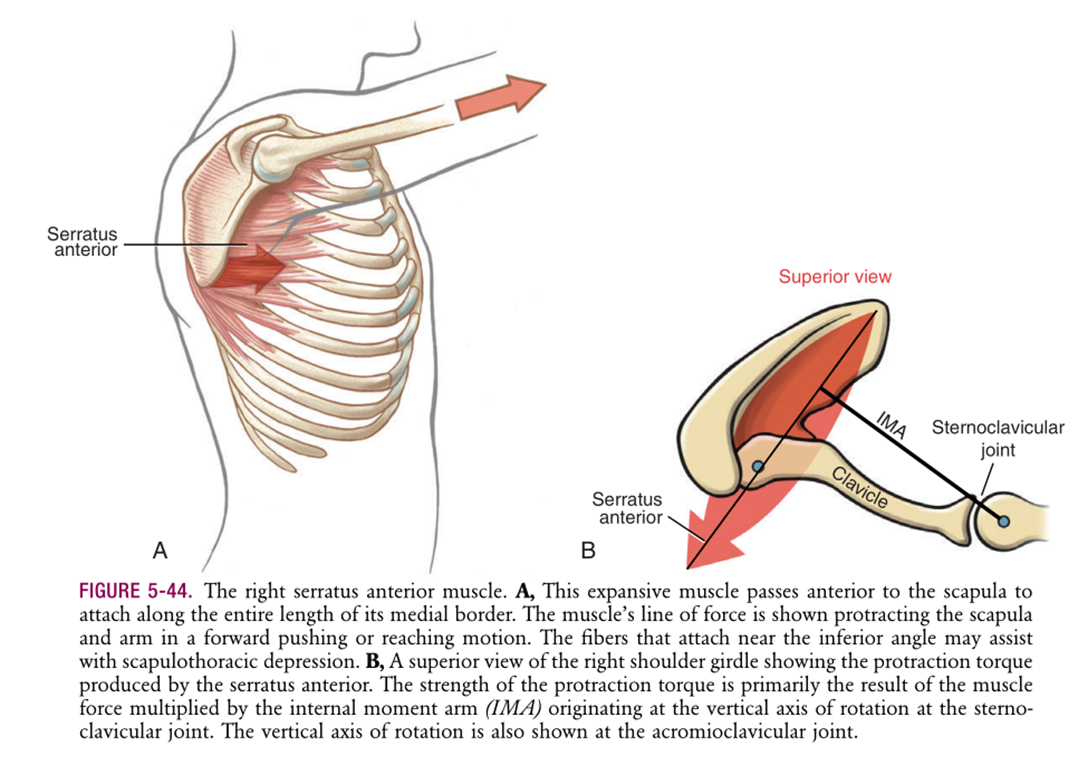
Serratus anterior: punching out muscle🥊(pulls scapula in protracted way against ribs)
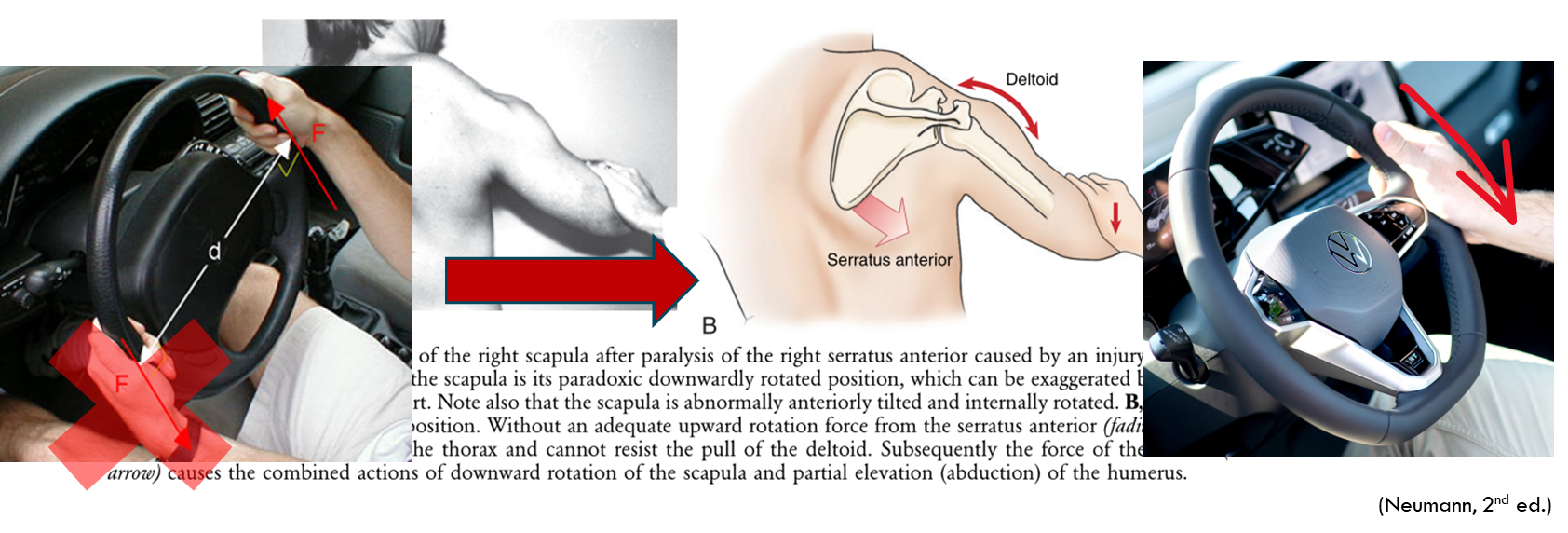
Scapular muscles by fxn: Upward rotators

Force-couple: 2 equal forces acting in opp. directions to rotate a part about its own axis of mvmt
Serratus anterior
Upper & lower trapezius
EX: turning steering wheel (1 hand pulls this way, other assists to create upward rotation)

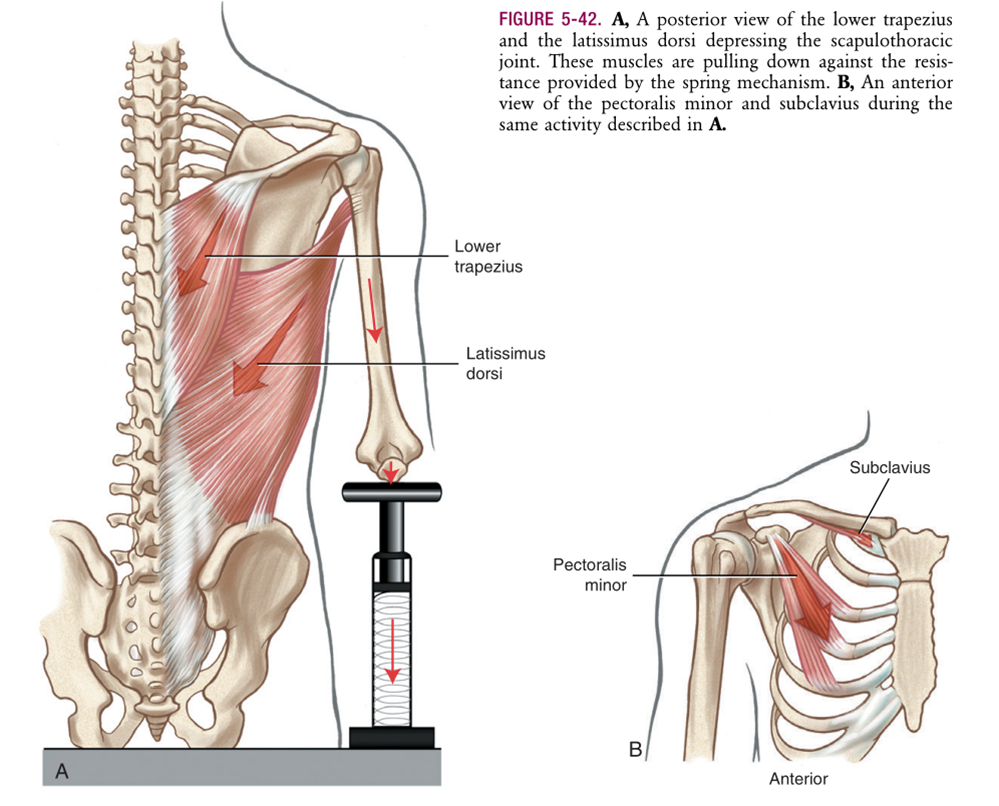
Scapular muscles by fxn: Depressors 🔽 Eccentric mvmt

Lower trapezius
Latissimus dorsi
Pectoralis minor
Subclavius
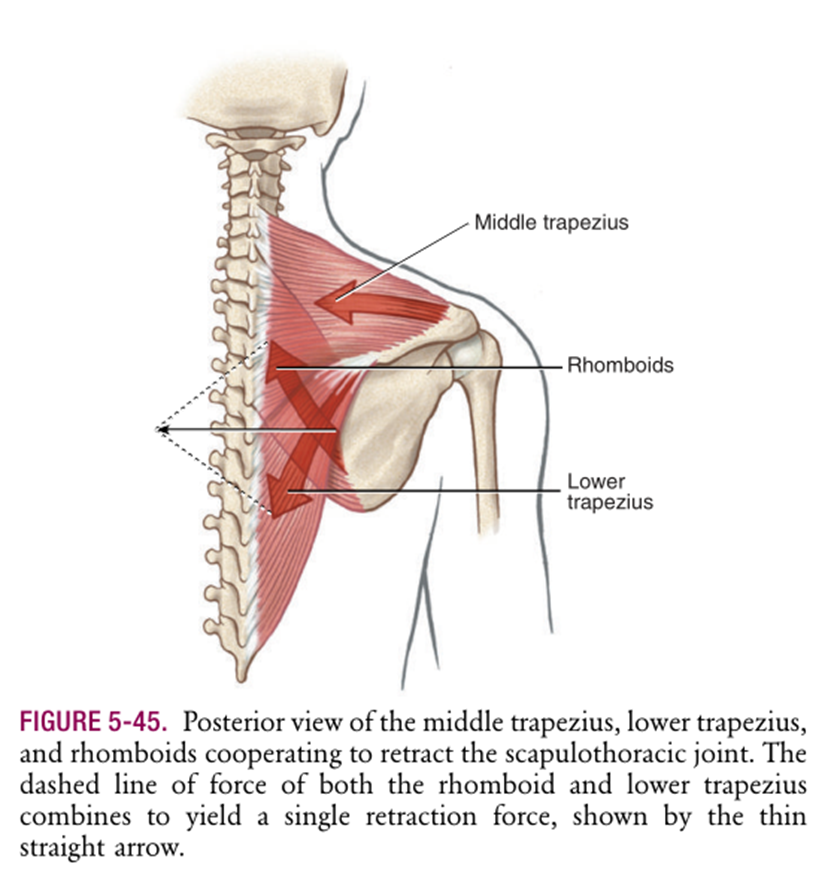
Scapular muscles by fxn: Retractors (posterior muscles)

Middle & lower trapezius
Rhomboids
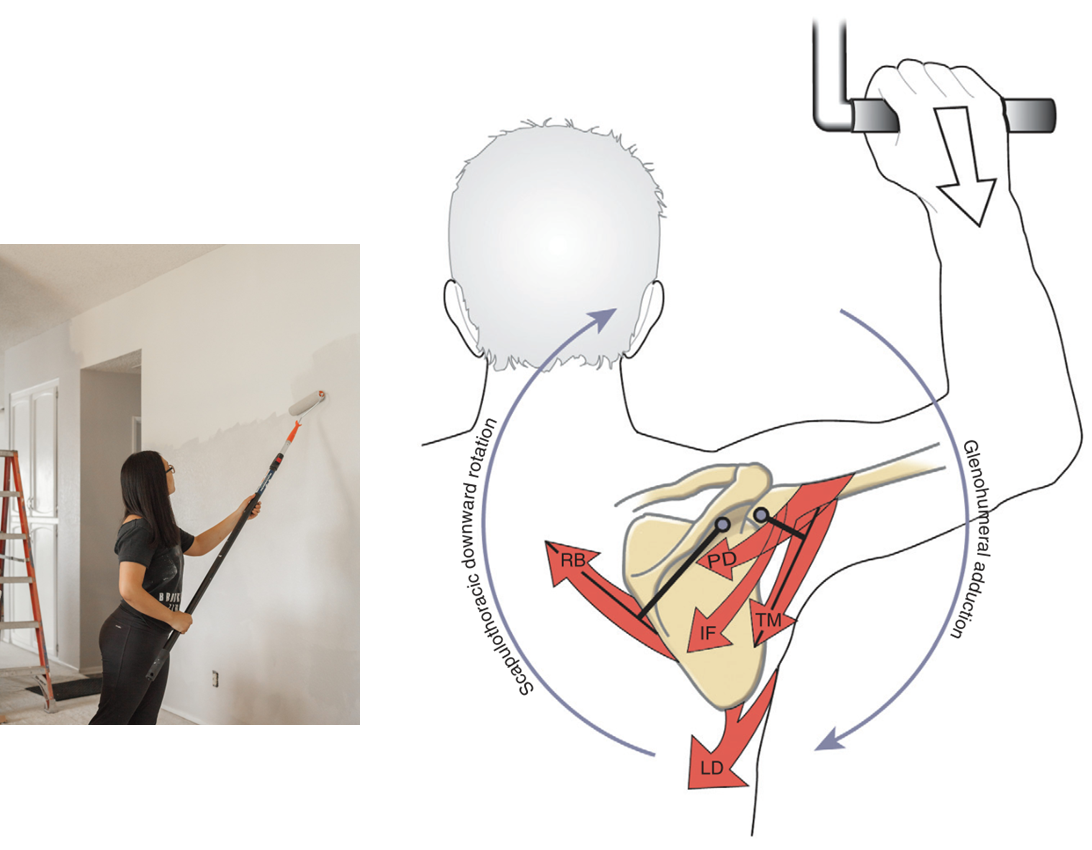
Scapular muscles by fxn: Downward rotators (bring arm back)/pull forcefully down)
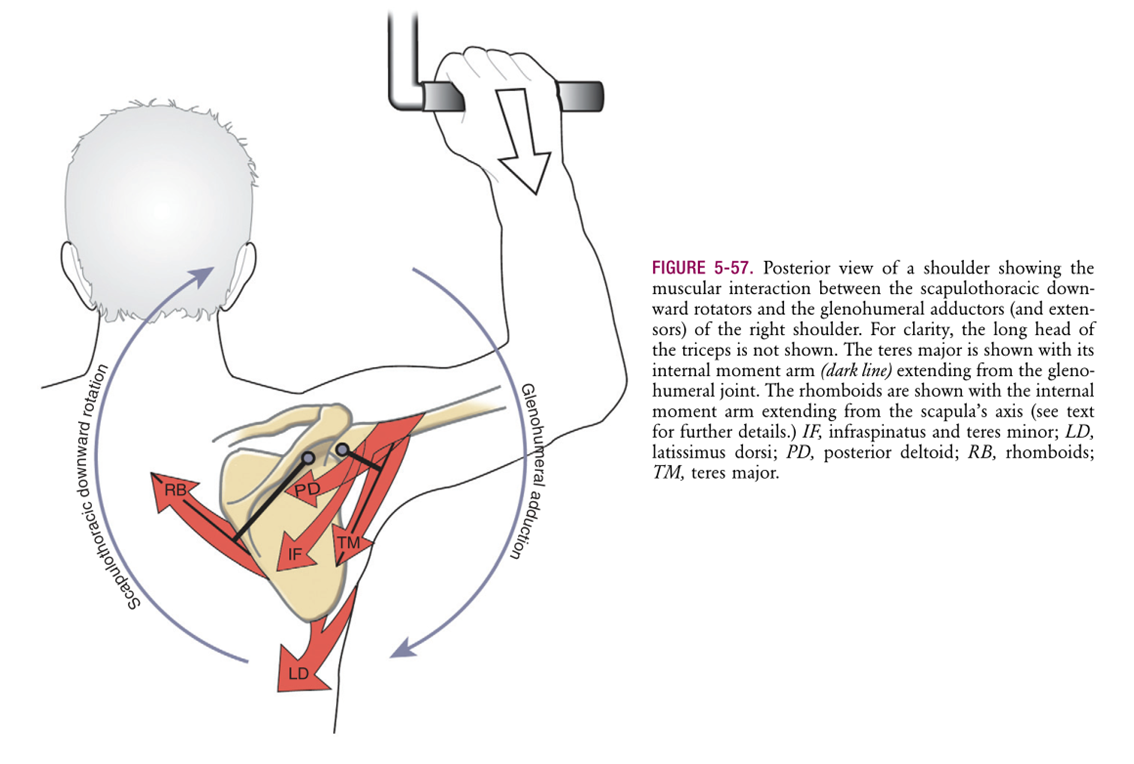
Primary Movers:
Rhomboids
Levator scapulae
Pectoralis minor
Assist muscle: Latissimus dorsi
Long Thoracic Nerve Palsy, C5-7
Lack of serratus anterior ➡
Unopposed deltoid action (tries to bring arm up by bringing humerus closer to scapula) ➡
Scapula paradoxical downward rotation (more deltoid contracts, more scapula goes other way)
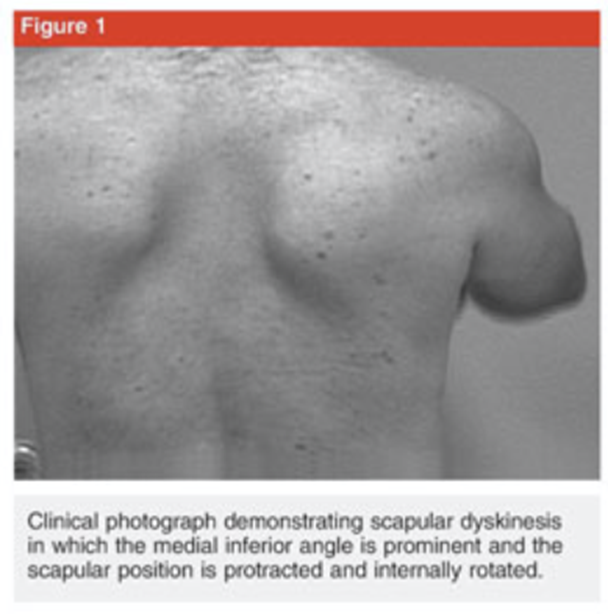
Clinical Presentation: Scapular dyskinesis
Loss of control of normal scapular physiology, mechanics, motion
Not an injury in and of itself; not always directly related to a specific injury!
Reduces efficiency of shoulder function!
Presentation:
Prominence of medial or inferomedial border
Early scapular elevation/shrugging on arm elevation 🤷
Rapid downward rotation on lowering of arm
Scapula winging (type of scapular dyskinesis, medial border prominence) 🪽
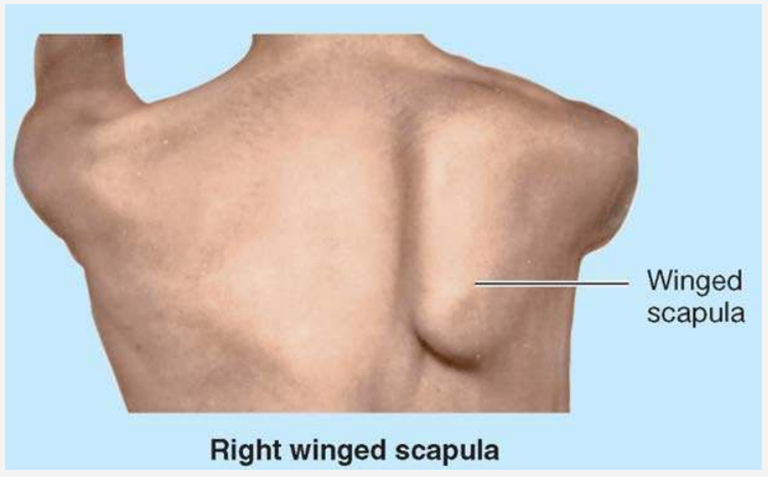
Most common cause: paralysis of serratus anterior due to injury of long thoracic n. (C5-C7)
Scapulohumeral muscles: connect scapula & proximal humerus
Deltoid, teres major, coracobrachialis (in front)
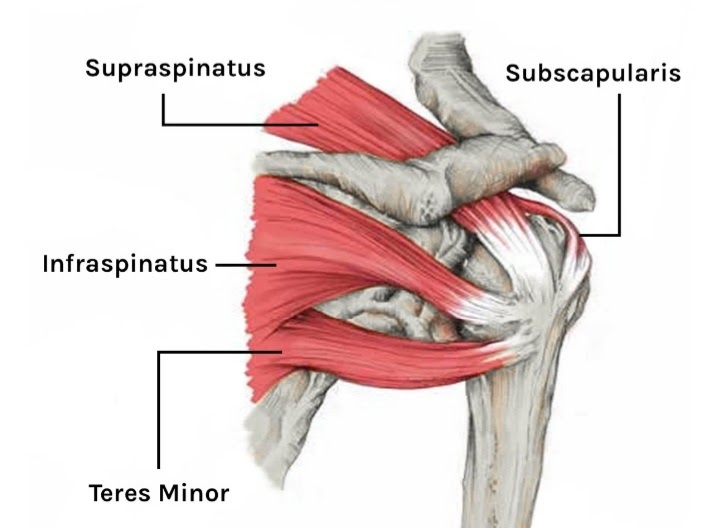
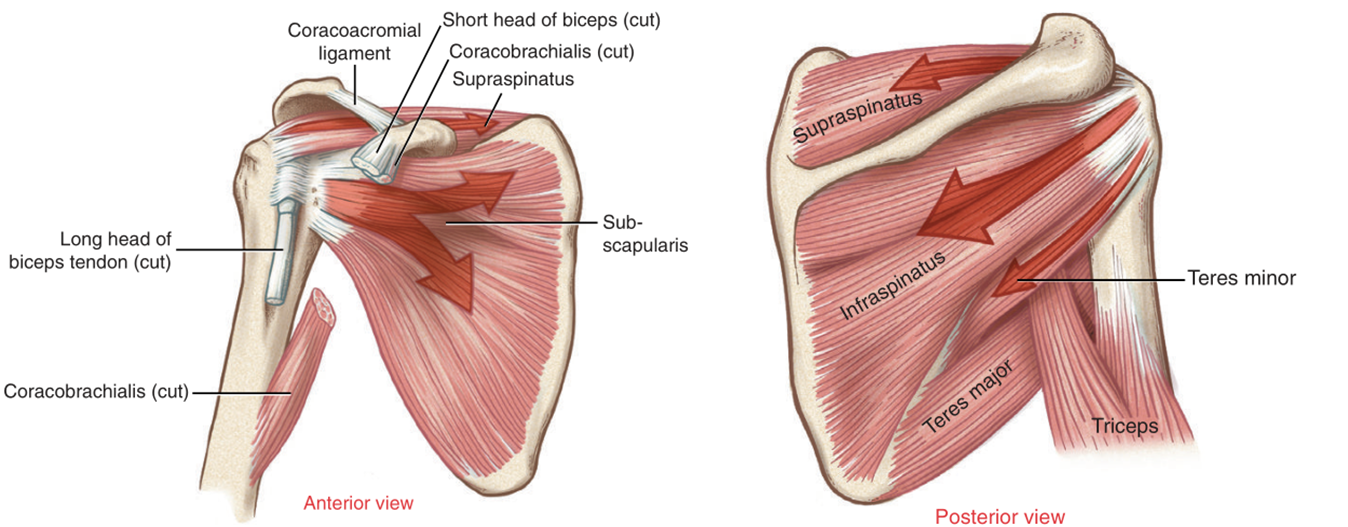
Rotator cuff muscles (SITS)
Supraspinatus
Infraspinatus
Teres minor
Subscapularis
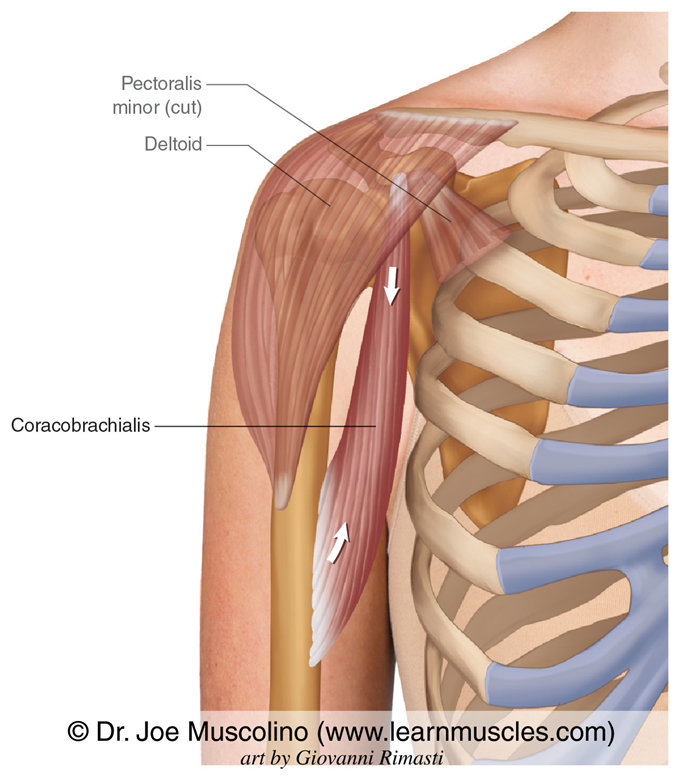
Coracobrachialis 👕🧺 (down low in front)
Placing groceries in fridge, carry laundry basket
Flex & adduct shoulder (GH)
Innervates from: musculocutaneous n. C6-7
O: Coracoid process of scapula
I: Medial surface of midhumeral shaft
Teres major: bottom inferior tip of scapula, wraps around to anterior side to medial side of lesser tubercule of humerus
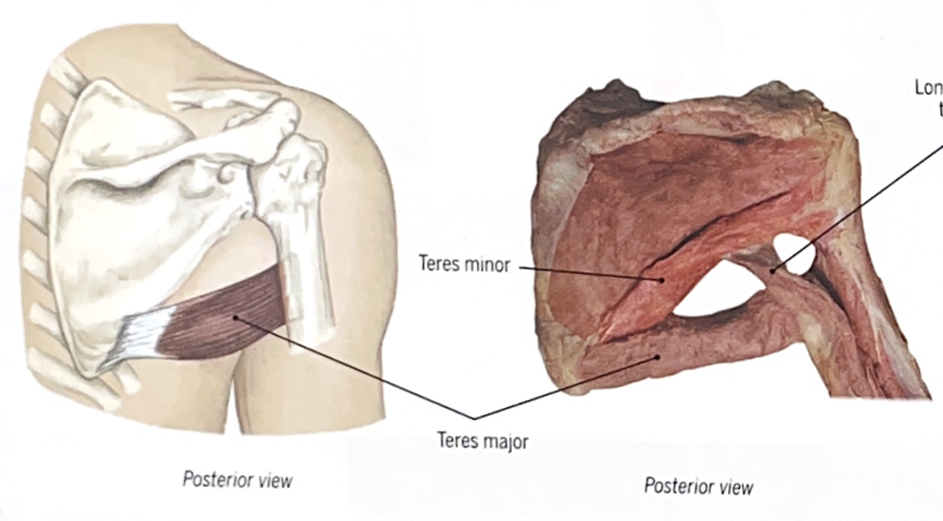
Toileting, perineal care 🚽
Extend, adduct, internally rotate shoulder (GH)
Innervates from: lower subscapular n. C5-7
Deltoid
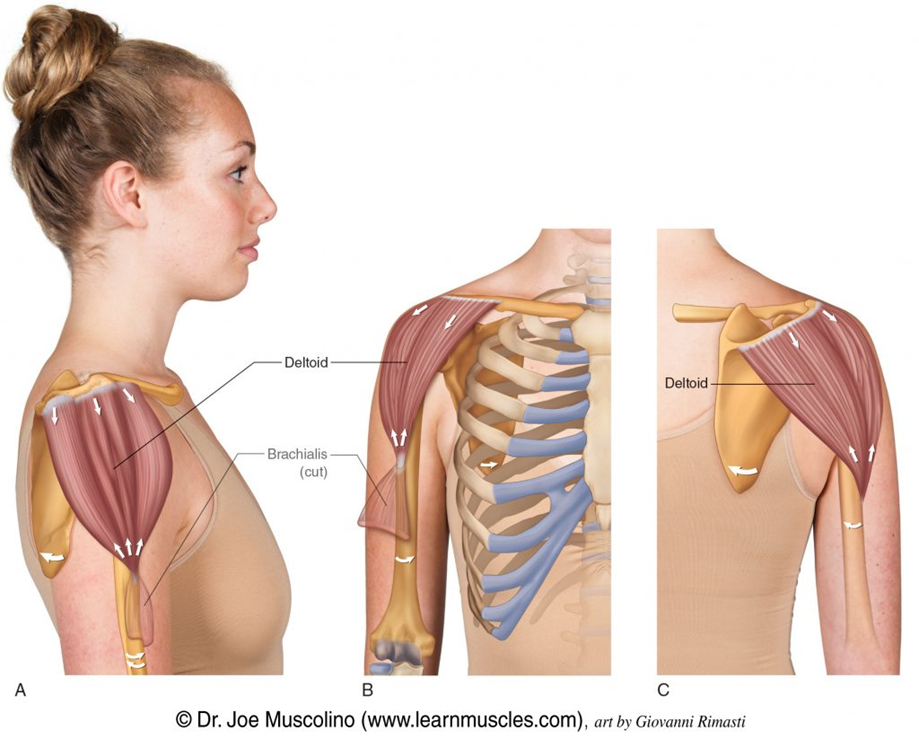
Yoga poses w/ arms overhead (all fibers), reaching for (anterior fibers) & putting on (posterior) seat belt
Innervates from: Axillary n. C5-6
Rotator Cuff Muscles
Group of 4 muscles forming protective, dynamic, muscular “cuff” around GH joint
Key dynamic stabilizers of GH joint
Rotator Cuff: Supraspinatus
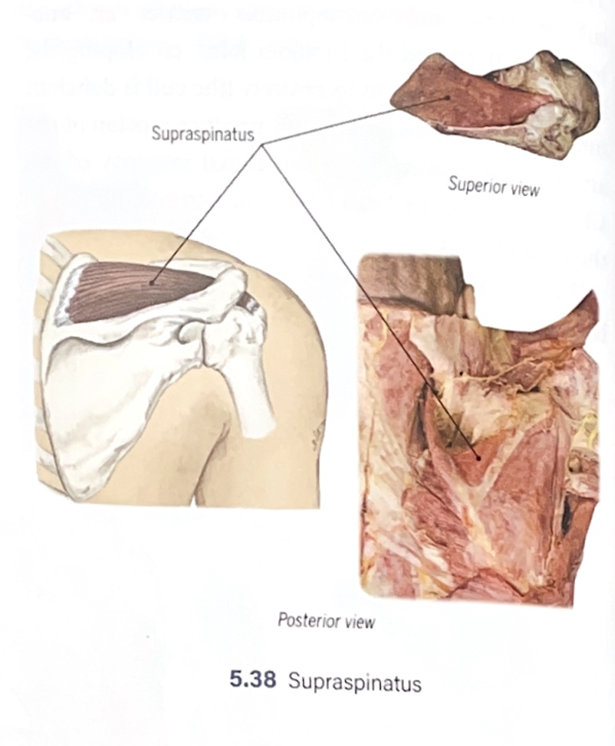
Painting overhead, washing hair 💇♀🧼🫧
Abduct shoulder (GH), stabilize head of humerus in glenoid cavity
Innervates from: suprascapular n. C4-6
Rotator Cuff: Infraspinatus
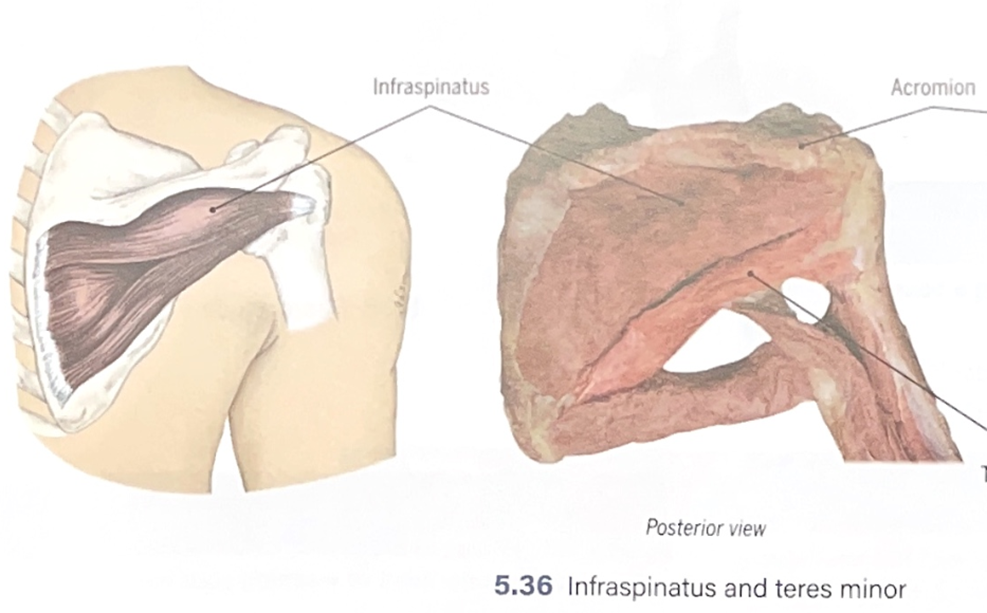
Playing racket sports, table tennis 🎾
Externally rotate, adduct shoulder (GH) + stabilize head of humerus in glenoid cavity
Innervates from: suprascapular C4-6
Rotator Cuff: Teres Minor
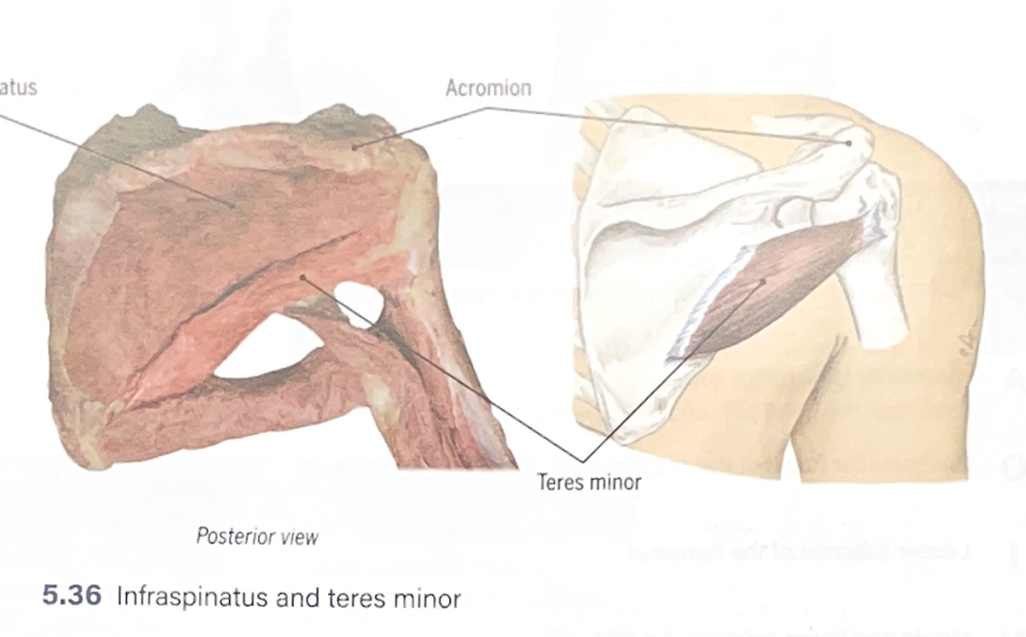
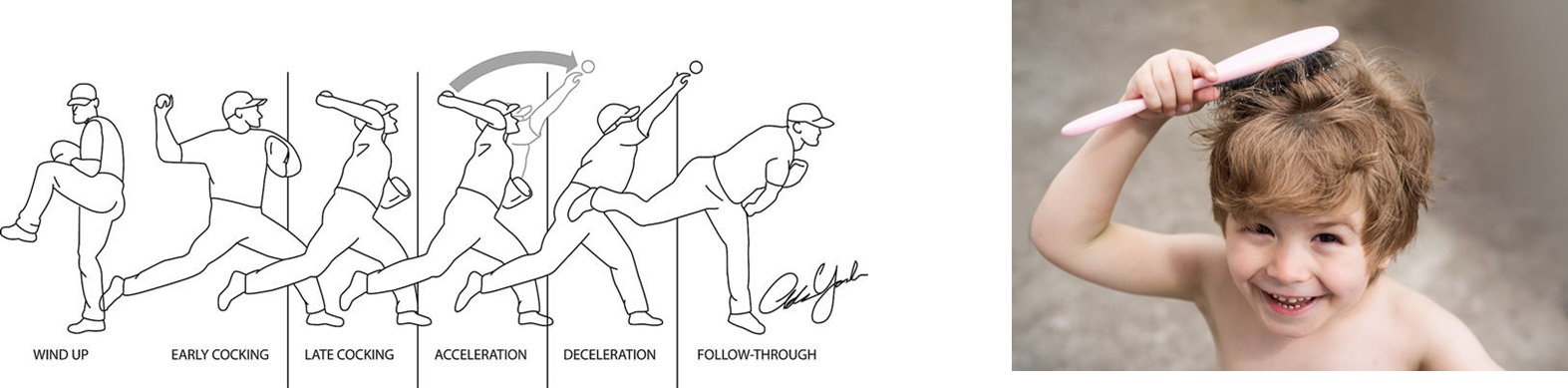
Wash back of head & neck
Externally rotate, adduct shoulder (GH) + stabilize head of humerus in glenoid cavity
Innervates from: Axillary C5-6
Rotator Cuff: Subscapularis
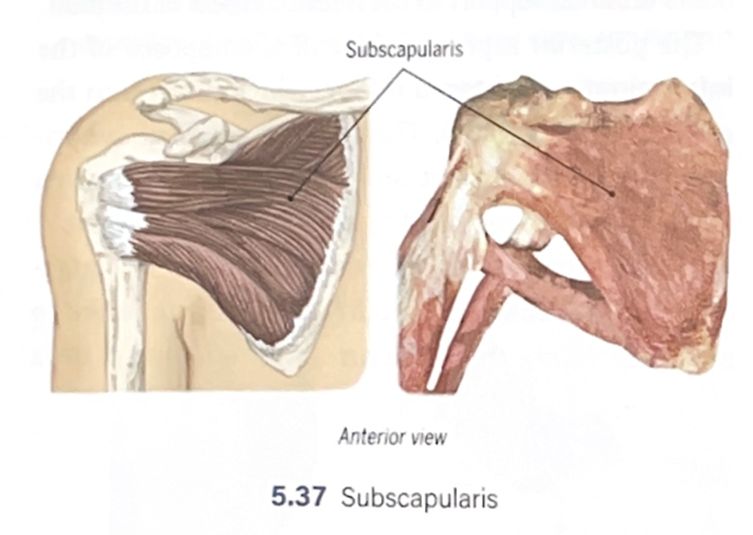
Toileting, donning bra, throwing baseball 🚽👙⚾
Internally rotate shoulder (GH), stabilize head of humerus in glenoid cavity
Innervates from: upper & lower subscapular C5-7
Rotator Cuff in Glenohumeral (GH) Abduction
Supraspinatus: Compressive force on humeral head against the glenoid fossa
Infraspinatus, Teres minor ⬅➡Subscapularis: Depressive force on humeral head
Rotator cuff: Force couple
2 or more muscles on opposing side of joints cooperate in harmony, stabilizing joint or facilitating movement
Deltoid rotator cuff force couple: largest amt force in shoulder (raise arm, up/out force on humerus)
Anterior posterior RC FC
Upper + Lower Trapezius & Serratus Anterior RC FC
Clinical corner: Glenohumeral subluxation

Presentation: Paralysis of deltoid & rotator cuff muscles = inability of humeral head to align w/ glenoid fossa against gravity
Key muscles involved:
Deltoid
Rotator cuff muscles: esp. the supraspinatus muscle
Causes:
Stroke or brain injury
Brachial plexus injury
Managing shoulder subluxation: Why is it NOT a good idea to position the shoulder in internal rotation for someone w/ shoulder subluxation for long?

External rotators would become weaker with internal rotation contracture if patient is left in an internal rotation position.
We have 4 ½ internal rotators = develop more tightness
2 external rotators = become weaker/lax over time
Clinical corner: Rotator cuff tear
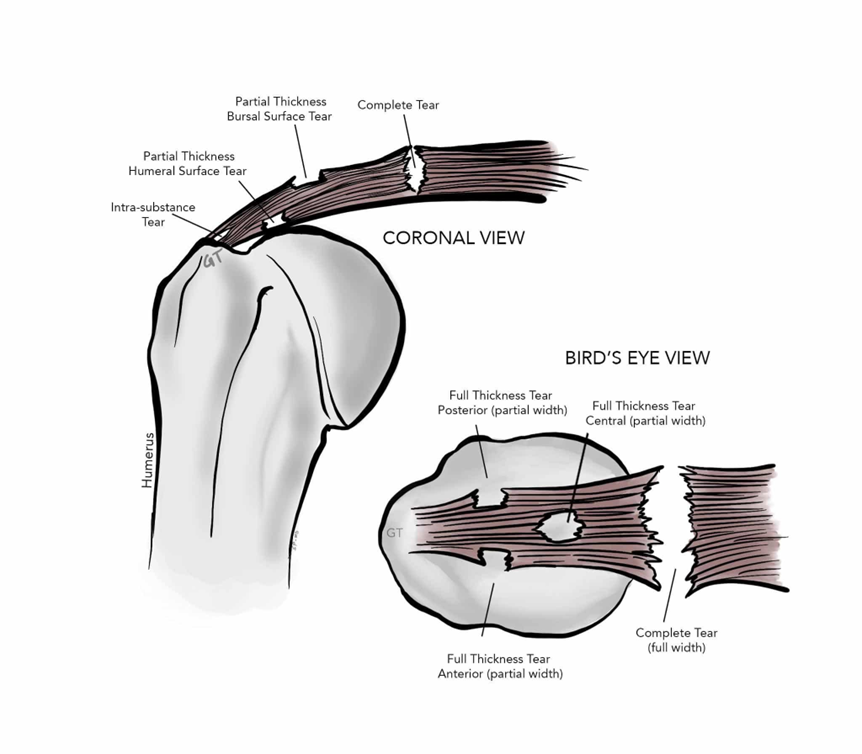
Prevalence: 25% in people 50+
Symptoms
Pain: majority of tears don’t cause pain, only a 1/3
Weakness: depends on size of tear
Muscles involved:
Commonly, supraspinatus
Massive tear = 2 or more muscles involved
Rotator cuff tear: A patient is asked to bring the hands to the mouth. He can do it, but only with the elbow in a high position (right arm). The unaffected side can reach the mouth without bringing the elbow high. Why does this occur?
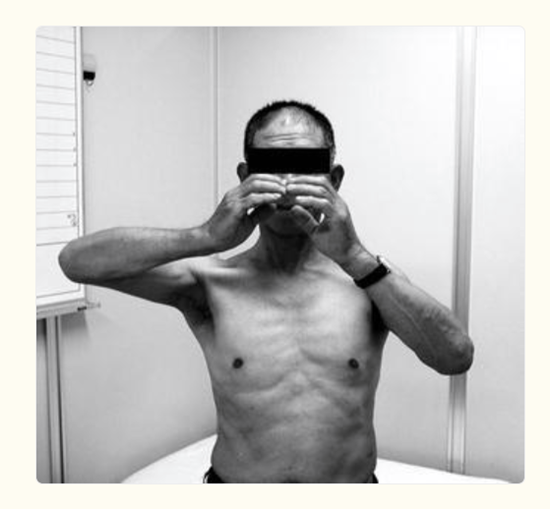
Pt exhibits weakness of supraspinatus muscle = difficulty initiating shoulder abduction
Weakness in external rotation is the cause, as this position eliminates the need to externally rotate the shoulder to bring cup to mouth
Rotator cuff tear: A patient isn’t able to lift the hand away from his back. Which rotator cuff muscle is torn?
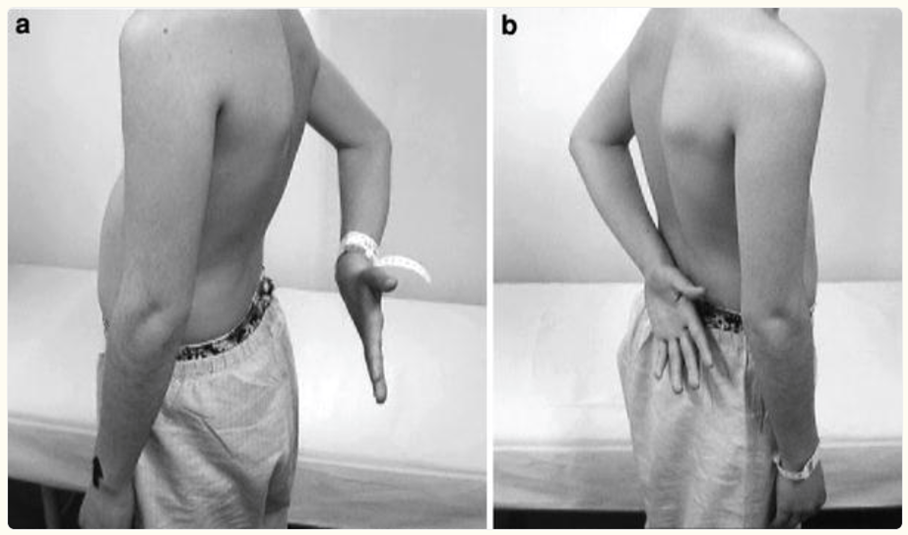
Subscapularis tear, can’t do internal rotation in this posture
Putting it together: GH + Scapula muscles
Fxnal shoulder motion = primary motion from muscles @ GH joint + assist/stabilization from scapula muscles acting @ ST joint
Scapulothoracic muscles DON’T move the humerus directly, but are vital for efficient GH motion by positioning & stabilizing scapula
Shoulder abductors: Primary movers 🩰

Deltoid
Supraspinatus (initiates first ~15*)
Shoulder abductors: Assist
ST joint upward rotators
Serratus anterior
Upper & lower trapezius
Shoulder abductors: Stabilizers
Rotator cuff muscles
Shoulder flexors: Primary movers

Anterior deltoid
Clavicular fibers of pectoralis major
Shoulder flexors: Assist
Coracobrachialis
Long of head of biceps brachii (initial ~30*)
Scapulothoracic (ST) joint upward rotators:
Serratus anterior
Upper & lower trapezius
Shoulder flexors: Stabilizers
Rotator cuff muscles
Shoulder extensors: Primary movers

Posterior deltoid
Latissimus dorsi
Teres major
Shoulder extensors: Assist
Long head of triceps brachii
Sternocostal head of pectoralis major
Infraspinatus
Teres minor
Shoulder extensors: Stabilizers
Rotator cuff muscles
Shoulder extensor & adductor muscle group has capacity to generate greatest torque compared to other shoulder muscle groups
ST downward rotators (rhomboids, pectoralis minor, levator scapulae) are both assist & stabilizers for shoulder extension & adduction
Shoulder adductors: Primary movers

Pectoralis major
Latissimus dorsi
Teres major
Shoulder adductors: Assist
Coracobrachialis
Long head of triceps brachii
Infraspinatus
Teres minor
Shoulder adductors: Stabilizers
Rotator cuff muscles
Shoulder External Rotators: Lowest torque muscle group, small part of the total muscle mass @ shoulder
Important muscle group in shoulder stabilization to balance strong internal rotators
Infraspinatus: peaks at 0* abduction
Teres minor: peaks at 90* abduction
Posterior deltoid
EX: cocking phase of pitching baseball ⚾
Shoulder Internal rotators: able to gen. much greater torque compared to external rotators

Subscapularis
Anterior deltoid
Pectoralis major
Latissimus dorsi (in btwn 2 majors)
Teres major
Clinical corner: Upper crossed syndrome (Not on test)
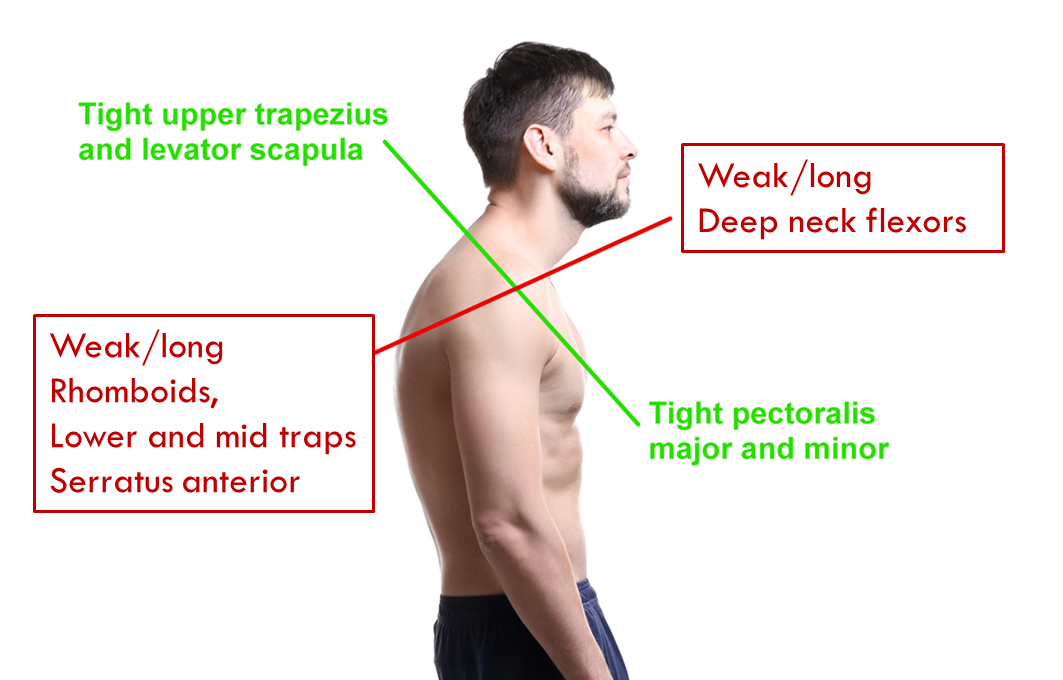
Consistently slouched posture
Large internal rotators adapt to become tight & short
Leads to smaller external rotators becoming weak
Common shoulder nerve palsies
Suprascapular nerve palsy
Axillary n. palsy
Long thoracic n. palsy
Spinal accessory n. palsy
Suprascapular nerve palsy: what muscles are affected?

Supraspinatus & infraspinatus muscles of the rotator cuff
What muscles are affected in axillary nerve palsy?

Deltoid & teres minor muscles
Spinal accessory nerve palsy

Trapezius muscle affected = affects upward rotation
Muscle is diminished compared to other side of shoulder
Can’t shrug shoulders 🤷❌
Which nerve root(s) is/are likely to be involved in GH subluxation? (p. 78)
C5, 6, 7
What kind of brachial plexus injury would likely result in GH subluxation: upper OR lower trunk? (p. 78)
Upper trunk
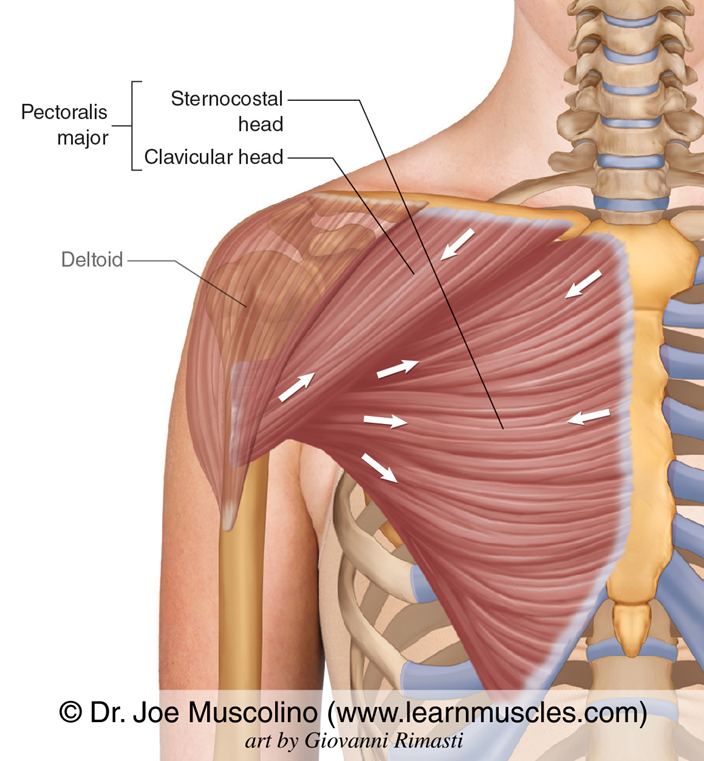
Pectoralis Major
Reaching across body into overhead cabinet, put on seatbelt: shoulder horizontal adduction, internal adduction, flexion of extended arm 🚗
Clavicular head, sternocostal head, abdominal part
Innervation from: Lateral pectoral n. C5-7, lateral & medial pectoral n. C6-8, T1
Accessory muscle to expand ribcage 🫁
Strengthen: push-ups, chest press, dips
Suprascapular nerve palsy: Which shoulder motion would be affected?

Shoulder abduction (supraspinatus): Watch for “shrugging” as a compensatory action when a patient tries initiating
Weakened but NOT completely absent due to deltoid, the main power abductor of shoulder
External rotation (Infraspinatus)
In axillary nerve palsy, which shoulder motions are affected?
Shoulder abduction due to loss of power abduction (deltoid)
External rotation weakness, but action is partly preserved by infraspinatus
Spinal accessory nerve palsy symptoms:

Much weaker scapula elevation (shrugging)
Disruption of scapula upward rotation = scapular dyskinesis (scapular winging)
All shoulder elevation motions (flexion, scaption, abduction) are limited due to lack of ST upward rotation