Venous Plethysmography
1/90
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
91 Terms
What does Plethysmography mean? (define it)
DEFINED: EVALUATING CHANGES IN VOLUME BY MEANS OF A PLETHYSMOGRAPH •
PLETHYSMOGRAPH: DEVICE THAT MEASURES VOLUME CHANGES
What does Plethysmography record? and name two other TYPES of plethysmography?
Evaluating measurements of what?
RECORDS BLOOD VOLUME CHANGES IN TISSUES OF LIMBS OR DIGITS
AIR
ELECTRICAL IMPEDANCE
EVALUATING MEASUREMENT OF VOLUME CHANGES IN EXTREMITY
Plethysmography, volume changes are related to what?
VOLUME CHANGES ARE RELATED TO THE CHANGES IN THE CARDIAC CYCLE •
SYSTOLE • DIASTOLE
Name the 3 types of different Plethysmography?
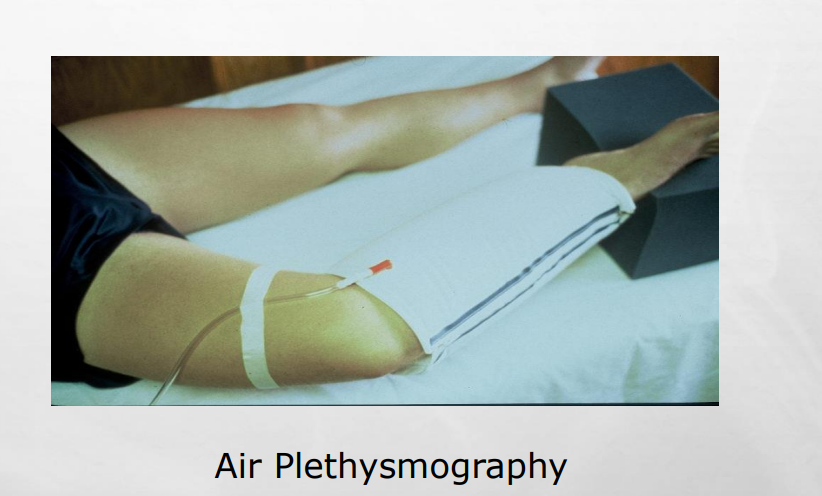
AIR PLETHYSMOGRAPHY
STRAIN GAUGE/IMPEDANCE
PHOTO
Explain how Air Plethysmography is used?
AIR PLETHYSMOGRAPHY: AIR IS USED TO MEASURE VOLUME CHANGES
Explain how Strain Gauge/ Impedance is used?
STRAIN GAUGE/IMPEDANCE: USES ELECTRICAL IMPEDANCE
Explain how Photo Plethysmography is used?
PHOTO: INFRARED LIGHT IS USED TO ASSESS THE QUANTITY OF BLOOD SUBCUTANEOUSLY
When it says blood is measured subcutaneously:
👉 It means the device is detecting blood in the small vessels just beneath the skin (not deep veins)
What does not true Plethysmography mean?
PHOTO!
NOT TRUE PLETHYSMOGRAPHY AS IT IS NOT MEASURING VOLUME CHANGES
What does Photo Plethysmography measure? and what does it reflect ?
MEASURES BLOOD CONTENT OF SKIN WHICH REFLECTS INTRAVENOUS VOLUME
“Photoplethysmography measures blood volume in the skin using infrared light, which indirectly reflects venous blood volume and venous function.”
what does VENOUS VOLUME = ? (mean)
VENOUS VOLUME = VENOUS CAPACITY
AMOUNT OF BLOOD THAT FILLS AN “EMPTY” VENOUS SYSTEM
Explain the NORMAL CONDITION: VENOUS SYSTEM
NORMAL CONDITION: VENOUS SYSTEM CAN BE FILLED WITH A LARGE VOLUME OF BLOOD
Explain the ABNORMAL CONDITION: VENOUS SYSTEM - name some things that can affect this (3)
ABNORMAL CONDITION: VENOUS SYSTEM ALREADY FILLED WILL NOT BE ABLE TO HOLD MUCH MORE (VENOUS HYPERTENSION) •
THROMBOSIS / BLOOD CLOT
“Thrombosis obstructs venous outflow, causing blood to accumulate and distend the veins, which leads to increased venous pressure (venous hypertension) and reduced capacity to hold additional blood.”
TERMINOLOGY
VENOUS OUTFLOW- what does this mean
• VENOUS OUTFLOW: HOW MUCH LEAVES THE VENOUS SYSTEM
TERMINOLOGY
EMPTY- what does this mean?
• EMPTY: SYSTEM DEVOID OF BLOOD
Devoid = completely empty / lacking something
Devoid means completely empty or lacking; in this context, it means the venous system has been emptied of blood.”
TERMINOLOGY
REFILL TIME: what does this mean?
• REFILL TIME: LENGTH OF TIME IT TAKES TO FILL WITH BLOOD
TERMINOLOGY
INDEX - what does this mean?
INDEX: RATIO
“An index is a ratio used to compare two values, allowing for standardized and meaningful assessment of venous function regardless of patient size.”
“Index = relationship, not just a number”
TERMINOLOGY
EJECTION- what does this mean?
• EJECTION: EXPELLING OF BLOOD FROM CALF
VENOUS HTN:
In the presence of what the vein becomes distended?
• IN THE PRESENCE OF THROMBUS, VEINS BECOME DISTENDED
VENOUS HTN
Distension leads to what?
DISTENSION LEADS TO ↑ HYDROSTATIC PRESSURE (HP)
What does a increase of HP lead to?
↑ HP LEADS TO A GREATER PRESSURE GRADIENT IN VEINS
Break it down: 🔵 HP = Hydrostatic Pressure
👉 Pressure from blood weight + gravity + fluid buildup
🟢 Pressure gradient
👉 The difference in pressure between two points
➡ Blood flows from:
👉 high pressure → low pressure
🔬 What this means: Step-by-step: 1⃣ Vein becomes distended (ex: DVT)
Blood backs up
Pressure in the vein increases
➡ Hydrostatic pressure ↑
2⃣ Now you have:
High pressure in the leg
Lower pressure toward the heart
➡ Bigger difference between the two
👉 That difference = greater pressure gradient
💡 Why this matters:
👉 A higher pressure gradient:
Forces fluid out of vessels
➡ Leads to:Edema
Swelling
Ulcers
🔥 BUT important nuance:
👉 Even though gradient increases:
If there’s a clot, flow is still impaired ❌
🧠 Easy way to remember:
👉 “More pressure buildup = bigger push difference”
🎯 Exam answer:
“An increase in hydrostatic pressure raises venous pressure, creating a larger difference between peripheral and central pressures, which increases the pressure gradient.”
🔥 One-line summary:
👉 “More pressure in veins = bigger pressure difference driving flow”
Please discuss two things VENOUS HTN affects on the veins and what it can lead too?
REDUCTION OF BLOOD FLOW INTO VEINS •
EVENTUALLY, FLUID LEAKS INTO THE TISSUES AND ULCERS FORM
🧠 Why would LESS blood enter veins?
👉 Because the veins are already:
➡ full and under high pressure (venous hypertension)
🔬 Step-by-step: 🟥 1⃣ There is a problem (ex: clot / DVT)
Blood can’t leave the vein ❌
➡ Blood backs up
🟠 2⃣ Veins become distended (overfilled)
Pressure inside the veins increases
➡ Hydrostatic pressure ↑
🟡 3⃣ Now think about flow into veins:
👉 Blood normally goes:
arteries → capillaries → veins
BUT…
➡ If venous pressure is HIGH:
👉 It becomes harder for blood to move from capillaries → veins
⚠ Why?
👉 Flow depends on pressure gradient:
Normally:
Capillaries (higher pressure) → veins (lower pressure) ✅
In this case:
Veins already have high pressure ❌
➡ Gradient decreases
➡ Less blood enters veins
💡 So:
👉 High venous pressure = resistance to incoming blood
🔥 Result:
Reduced flow into veins
Fluid leaks into tissues
➡ Edema + ulcers
🧠 Easy way to remember:
👉 “If veins are full → nothing else can enter”
🎯 Exam answer:
“Blood flow into the veins is reduced because elevated venous pressure decreases the pressure gradient between capillaries and veins, limiting forward flow into the venous system.”
🔥 One-line summary:
👉 “High venous pressure blocks incoming blood”
Normal state for veins, please discuss the function?
How it leaves and what type of system is this explain why that is?^^^
what is it Known as?
what does it determine?
VENOUS BLOOD EASILY LEAVES THE CALF
• VENOUS BLOOD SLOWLY FILLS AN “EMPTY” SYSTEM •
KNOWN AS VENOUS REFILL TIME •
DETERMINE VENOUS VOLUME
WHY DOES IT SLOWLY FILL AN EMPTY SYSTEM?
Blood slowly fills an empty venous system because it must pass through the entire circulatory pathway, including slow capillary flow, before returning to the veins.
The venous system slowly fills because blood must travel through the entire circulatory system, including the capillary bed, resulting in gradual venous filling under normal conditions.”
VENOUS CAPACITY TECHNIQUE, explain the 3 steps
DRAIN THE DEEP VENOUS SYSTEM OF BLOOD
OBSTRUCT VENOUS RETURN WITH A LARGE BLOOD PRESSURE CUFF, PLACED AT THE THIGH
MEASURE VOLUME FILLING
A normal venous capacity system shows what?
• NORMAL SYSTEM SHOWS MARKED INCREASE IN VOLUME
A abnormal venous capacity system shows what?
ABNORMAL SYSTEM DOES NOT SHOW AN INCREASE VOLUME BECAUSE VEIN IS ALREADY DISTENDED
VENOUS OUTFLOW TECHNIQUE, explain what this mean
OPPOSITE OF VENOUS CAPACITANCE •
HOW EASILY BLOOD LEAVES VENOUS SYSTEM
VENOUS OUTFLOW TECHNIQUE
what is allowed to flow into the Limb?
what is prevented from flowing out?
What is used to occlude flow?
ARTERIAL BLOOD IS ALLOWED TO FLOW INTO THE LIMB •
VENOUS BLOOD IS PREVENTED FROM FLOWING OUT •
PRESSURE CUFF USED TO OCCLUDE FLOW
BLOOD PRESSURE CUFF IS DEFLATED, what will a normal system show?
NORMAL SYSTEM- BLOOD WILL EMPTY QUICKLY
BLOOD PRESSURE CUFF IS DEFLATED, what will an abnormal system show?
ABNORMAL SYSTEM- CLOT OBSTRUCTS FLOW, BLOOD MUST FIND AN ALTERNATE ROUTE, EMPTING TIME WILL BE DELAYED
REFLUX PLETHYSMOGRAPHY, which ones would you use?
PHOTOPLETHYSMOGRAPHY •
AIR PLETHYSMOGRAPHY
PHOTOPLETHYSMOGRAPHY, what are you evaluting for? and using what blood volume?
EVALUATE FOR PRESENCE / SEVERITY OF VALVULAR INCOMPETENCE •
USING THE CAPILLARY BLOOD VOLUME
What are the limitations for PHOTOPLETHYSMOGRAPHY (name 4)
LIMITATIONS:
KNOWN DVT
•IMPROPER PPG SENSOR PLACEMENT •
PRESENCE OF COLLATERALS •
VENOUS ULCERS – OCCUR IN AREA WHERE SENSOR IS PLACED
Please explain the PPG TECHNIQUE
how is the patient postion?
where are the PPG sensor placed, where would you never place them?
what should the patient do explain, what does this do?
what should you establish?
1. PATIENT SITTING; LEGS DANGLING
2. PPG SENSOR PLACED 5-10 CM ABOVE MEDIAL MALLEOLUS •
DON’T PLACE ON VARICOSE VEINS
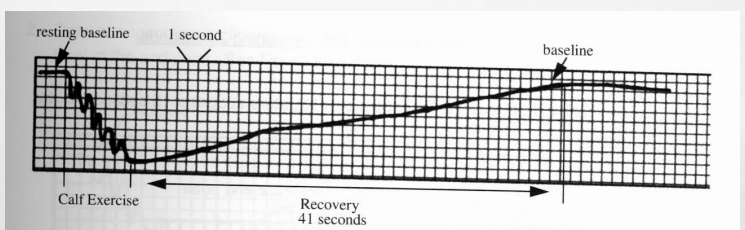
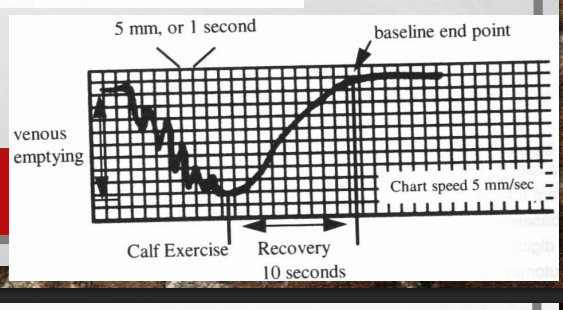
3. PATIENT DORSIFLEXES FOOT 5X’S; BLOOD EMPTIES FROM CALF •
BASELINE IS ESTABLISHED
PPG TRACING IS MONITORED FOR what? (hint volume)
• PPG TRACING IS MONITORED FOR VENOUS REFILL TIME (VRT)
Explain the normal and abnormal numbers for VRT
VRT>20-25 SECONDS; EXAM IS NORMAL AND COMPLETED •
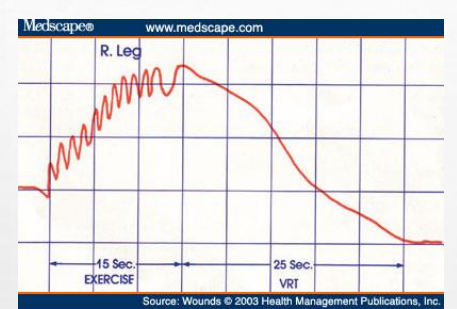
VRT<20-25 SECONDS; EXAM IS ABNORMAL
VRT<20-25 SECONDS; EXAM IS ABNORMAL,
what does it indicate?
what test would you perform and what do you want to determine?
INDICATES RAPID RETURN OF BLOOD TO CALF VIA INCOMPETENT VENOUS CHANNELS
PERFORM TOURNIQUET TEST: DETERMINES DEEP VS. SUPERFICIAL REFLUX
“A VRT < 20–25 seconds indicates rapid refilling due to venous reflux, where incompetent valves allow blood to flow backward from proximal veins into the calf instead of slowly filling via capillary flow.”
“Rapid return of blood is abnormal because incompetent venous valves allow reflux, causing blood to flow backward into the calf instead of slowly filling via the normal circulatory pathway.”
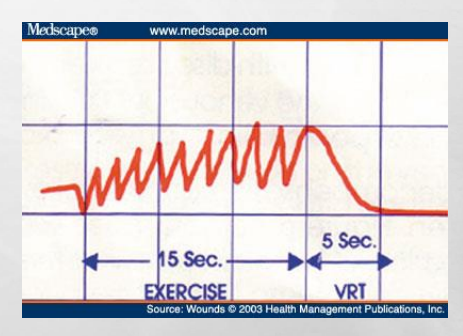
is the normal or abnormal
This is abnormal
Is this normal or abnormal
This is normal
PPG TOURNIQUET TEST
Establishe location of what? what system? what is placed at determined location? - what is the location
ESTABLISHES LOCATION OF REFLUX •
DEEP SYSTEM •
SUPERFICIAL SYSTEM •
TOURNIQUET OR PRESSURE CUFF PLACED AT DETERMINED LOCATION •
LOWER THIGH •
PROXIMAL CALF
PPG TOURNIQUET TEST • PRESSURE CUFF / TOURNIQUET PLACED ON LOWER THIGH; INFLATE TO what MMGH, what is goal to do?
You want to perform what, and monitor what?
PRESSURE CUFF / TOURNIQUET PLACED ON LOWER THIGH; INFLATE TO 50 MMHG •
OCCLUDE GSV •
DEEP VEINS OPEN
PERFORM DORSIFLEXION'S AND MONITOR VRT
PPG TOURNIQUET TEST
>? secounds tells you what
<? secounds tells you what?
>20 SECONDS; GSV INSUFFICIENCY AND EXAM COMPLETED •
<20 SECONDS; MOVE CUFF TO UPPER CALF AND OCCLUDE SSV
What does VRT stand for ?
VRT: Venous Refill Time
PPG TOURNIQUET TEST • TOURNIQUET PLACED ON UPPER CALF: inflate cuff to what? and you want to repeat what and monitor what?
TOURNIQUET PLACED ON UPPER CALF •
INFLATE CUFF TO 50 MMHG •
REPEAT DORSIFLEXIONS; MONITOR VRT
PPG TOURNIQUET TEST, • TOURNIQUET PLACED ON UPPER CALF
>? SECONDS; =
• <? SECONDS=
>20 SECONDS; SSV INSUFFICIENCY •
<20 SECONDS; DEEP VEIN INSUFFICIENCY
what does this tracing above represents?
Represents normal PPG exam
what does this tracing above represents?
Abnormal
AIR PLETHYSMOGRAPHY (APG), AKA know as what?
its a what cuff that is wrapped around where and connected to what that detects what?
AKA: PNEUMOPLETHYSMOGRAPHY •
A PNEUMATIC CUFF THAT IS WRAPPED AROUND THE LIMB IS CONNECTED TO A PRESSURE TRANSDUCER THAT DETECTS VOLUME CHANGES
AIR PLETHYSMOGRAPHY (APG)
VOLUME CHANGES ARE SECONDARY TO what?
• VOLUME CHANGES ARE SECONDARY TO POSITION CHANGES AND EXERCISE
APG - CAPABILITIES 👉 APG = Air Plethysmography
what does it determine?
and what does it measures? name 5
DETERMINES THE PRESENCE OR ABSENCE OF VENOUS INSUFFICIENCY •
MEASURES: •
CALF VENOUS VOLUME •
RATE AT WHICH CALF VENOUS VOLUME IS RESTORED •
NORMAL VS REFLUX •
EFFECTIVENESS OF CALF MUSCLE PUMP •
AMBULATORY VENOUS PRESSURE (INDIRECTLY)
“Ambulatory venous pressure refers to the pressure in leg veins during walking, which is estimated indirectly using plethysmography measurements rather than measured directly.”
What are the APG -LIMITATIONS name 3
PATIENT UNABLE TO MAINTAIN POSITIONS OR PERFORM EXERCISE •
CASTS, TRACTION, OR BANDAGES •
NOT ABLE TO DIAGNOSE INCOMPETENT PERFORATORS OR ISOLATED INCOMPETENT DISTAL VEINS
APG – POSITIONING
how is the patient postion?
How is the limb?
what is recorded? during when?
what is established?
venous is what?
series of maneuvers with the patient postion how?
cuff inflated to what MMHG?
PATIENT STARTS SUPINE, HEEL SLIGHTLY ELEVATED
• LIMB EXTERNALLY ROTATED
• VOLUME CHANGES ARE RECORDED DURING •
LIMB ELEVATION (EMPTIES THE VEINS) • BASELINE IS ESTABLISHED • VENOUS REFILLING
• SERIES OF MANEUVERS WITH THE PATIENT UPRIGHT
• CUFF INFLATED TO 6 MMHG
What APG positioning/technique is REALLY doing
👉 The whole goal is:
Empty the veins → then watch how they refill → then test function
🔄 Step-by-step (clean version) 🟢 STEP 1: Start supine (lying down)
Heel slightly elevated
Limb externally rotated
👉 Why?
Gravity helps drain blood out of the leg
Veins become as empty as possible
🟢 STEP 2: Establish baseline
Once veins are empty → machine sets baseline (zero point)
👉 This is your starting reference
🟢 STEP 3: Stand the patient up
Patient moves upright
👉 Now:
Gravity causes blood to flow back into the leg
This is venous refilling
🟢 STEP 4: Record volume changes
The cuff (inflated ~6 mmHg) detects changes in leg volume
👉 This is how APG measures:
Venous volume (VV)
Venous filling time (VFT)
Venous filling index (VFI)
🟢 STEP 5: Perform maneuvers
Tip-toe exercises
Weight shifting
👉 To evaluate:
Calf muscle pump
Residual blood
🔑 Why the cuff is only 6 mmHg:
👉 It’s NOT occluding anything
👉 It’s just:
sensing volume changes (like a detector)
🧠 Fix the confusing bullet:
The slide says:
“Volume changes are recorded during limb elevation…”
🚨 That’s misleading
👉 The real idea:
Elevation = empties veins
Recording happens mainly during refilling + maneuvers
🔥 Easy way to remember:
Empty → baseline → fill → test
🩺 Exam one-liner:
APG begins with venous emptying in the supine position, followed by upright positioning to measure venous refilling and assess venous function
APG - TECHNIQUE • MANUAL CALIBRATION •
MAXIMUM VENOUS EMPTYING OCCURS WHEN?
MAXIMUM VENOUS EMPTYING OCCURS WHEN BASELINE STABILIZES • ZERO BASELINE
APG - TECHNIQUE • MANUAL CALIBRATION
CALF VEIN FILLING IS ESTABLISHED WHEN?
CALF VEIN FILLING IS ESTABLISHED WHEN STEADY BASELINE OCCURS
APG - TECHNIQUE, MANUAL CALIBRATION
BASELINE OCCURS WHEN?
• BASELINE: OCCURS WHEN THERE IS NO VARIATION IN FLOW
APG – TECHNIQUE (INSUFFICIENCY), what does the pateint do?
PATIENT STANDS UP QUICKLY BEARING WEIGHT ON NON-TEST LEG
“The patient stands on the non-test leg to prevent activation of the calf muscle pump in the test leg, allowing accurate measurement of passive venous filling due to gravity.”
Weight is placed on the non-test leg to prevent calf muscle contraction in the test leg, allowing accurate assessment of venous filling
APG – TECHNIQUE (INSUFFICIENCY), filling of leg is recorded until what?
FILLING OF LEG IS RECORDED UNTIL BASELINE IS OBTAINED – FUNCTIONAL VENOUS VOLUME
APG – TECHNIQUE (INSUFFICIENCY)
COMPARISON IS MADE BETWEEN what?, this determines what
COMPARISON IS MADE BETWEEN THE VENOUS VOLUME AND VENOUS FILLING TIME •
DETERMINES IF INSUFFICIENCY IS PRESENT
APG – TECHNIQUE (INSUFFICIENCY)
What do you do TO LOCALIZE INSUFFICIENCY,?
TO LOCALIZE INSUFFICIENCY, A BELOW THE KNEE TOURNIQUET IS PLACED TO OCCLUDE SMALL AND GREAT SAPHENOUS VEINS
APG – INTERPRETATION
(VV) - what does this mean?
What is CONTINUALLY DOCUMENTED? (when patient does what)
FUNCTIONAL VENOUS VOLUME IS REACHED WHEN?
COMPETENT VENOUS VALVES- you know this when the leg volume of whst?
what is the leg volume for venous insufficiency?
VENOUS VOLUME (VV)
• FILLING OF CALF VEINS WHEN PATIENT STANDS IS CONTINUALLY DOCUMENTED
• FUNCTIONAL VENOUS VOLUME IS REACHED WHEN A STEADY BASELINE IS OBTAINED
• COMPETENT VENOUS VALVES – INCREASE IN LEG VOLUME OF 100 – 150 ML •
VENOUS INSUFFICIENCY – 100 – 350 ML
APG - INTERPRETATION • (VFI) =
documents what?
based on what?
calculated by using what?
normal valve function is what
minor/mod reflux is what?
Severe reflux is what?
VENOUS FILLING INDEX (VFI)
DOCUMENTS RATE OF VENOUS REFILL •
BASED ON REFILLING AFTER PATIENT QUICKLY STANDS •
CALCULATED BY USING VV AND VFT •
NORMAL VALVE FUNCTION – VFI < 2.0 ML/SEC •
MINOR/MODERATE REFLUX – VFI > 2.0 – 10.0 ML/SEC •
SEVERE REFLUX – VFI >10 ML/SEC
VV: venous volume VFT: venous filling time
APG – TECHNIQUE (CALF PUMP)
GRAVITATIONAL PRESSURE CAUSES what? what is documented on strip chart recorder?
GRAVITATIONAL PRESSURE CAUSES INCREASED VENOUS VOLUME •
INCREASING VOLUME IS DOCUMENTED ON STRIP CHART RECORDER
APG – TECHNIQUE (CALF PUMP), PATIENT THEN does what? and what maneuver is performed? what does that test result in and explain what its due too?
PATIENT THEN STANDS WITH WEIGHT ON BOTH LEGS EQUALLY
• 1 TIP-TOE MANEUVER IS PERFORMED •
RESULTS IN REDUCTION OF VENOUS VOLUME DUE TO ENGAGED CALF MUSCLE PUMP
APG - TECHNIQUE
what MANEUVERS ARE THEN COMPLETED? what does this do and what is it used for (calculate whar?) ? and then what does the patient resume to do?
10 TIP-TOE MANEUVERS ARE THEN COMPLETED •
DECREASE IN VENOUS VOLUME IS USED TO CALCULATE EJECTION VOLUME (EV) AND VENOUS FILLING TIME (VFT) •
THE PATIENT RESUMES THE SUPINE POSITION WITH LEG ELEVATED AGAIN TO EMPTY THE VENOUS SYSTEM
APG – INTERPRETATION • EJECTION FRACTION (EF)
measures what function?
based on results of what maneuver?
what does it quantifies?
calculated using what?
whats the normal EF?
MEASURES CALF MUSCLE FUNCTION •
BASED ON RESULTS OF 1 TIP-TOE EXERCISE •
QUANTIFIES HOW MUCH BLOOD IS LEFT IN LEG AFTER ONE CONTRACTION OF CALF MUSCLE PUMP •
CALCULATED USING EJECTION VOLUME (EV) AND VV •
NORMAL – EF > 60%
APG – INTERPRETATION • (RVF) =
calculated as what of what after what movements?
equivalent to what
what is the normal RVF?
RESIDUAL VENOUS VOLUME FRACTION (RVF)
CALCULATED AS % OF VENOUS VOLUME REMAINING AFTER 10 TIP-TOE MOVEMENTS •
EQUIVALENT TO AMBULATORY VENOUS PRESSURE IN MMHG •
NORMAL – RVF LESS THAN 35%
THROMBUS DETECTION • DVT TESTS, what are they name 2
APG •
CW DOPPLER
APG • DETECTION OF THROMBUS IN what veins?, what does it use? ( hint the vocab words)
• DETECTION OF THROMBUS IN THE ILIAC, FEMORAL AND POPLITEAL VEINS
USES MAXIMUM VENOUS CAPACITANCE (MVC) AND MAXIMUM VENOUS OUTFLOW (MVO)
What are the APG -LIMITATIONS name 3 (and maybe a couple others?)
CAN’T DETECT CALF VEIN THROMBUS •
SMALL THROMBUS WILL NOT BE DETECTED •
FALSE POSITIVE WITH:
APG - POSITIONING
how is the PT postion, where is the head and lower legs? and how are the knees postion?
SUPINE •
HEAD FLAT AND LOWER LEGS ABOVE THE HEART •
KNEES SLIGHTLY BENT AND EXTERNALLY ROTATED
APG - TECHNIQUE
Name 3 things you use on the PT like instruments
“MONITORING TRANSDUCERS
OCCLUDING CUFF:
CUFF DEFLATION
APG - TECHNIQUE
“MONITORING TRANSDUCERS”: where is it placed to detect what, with what?
“MONITORING TRANSDUCERS”: PLACED ON CALF TO DETECT VOLUME CHANGES WITH CUFF INFLATION / DEFLATION
APG - TECHNIQUE
OCCLUDING CUFF, placed where, inflated where, and what about the baseline?
OCCLUDING CUFF: PLACED ABOVE THE KNEE; INFLATED ABOVE VENOUS PRESSURE BUT BELOW ARTERIAL PRESSURE (≈45MMHG) •
OCCLUDING CUFF: BASELINE TRACING RISES AND REACHES MVC
APG - TECHNIQUE
CUFF DEFLATION what is measured and what is obtained?
• CUFF DEFLATION: 3 SECOND OUTFLOW IS MEASURED AND MVO IS OBTAINED
APG - INTERPRETATION whats normal?
NORMAL: TRACING FALLS TO BASELINE WITHIN 3 SECONDS OF CUFF DEFLATION
APG - INTERPRETATION what is abnormal?
ABNORMAL: >3 SECONDS TO FALL TO BASELINE
APG - INTERPRETATION
how many times must the test be done to rule out false positives?
TEST MUST BE REPEATED 3-5 TIMES TO RULE OUT FALSE POSITIVES
CW DOPPLER, what are the CAPABILITIES name two?
OBSTRUCTION •
VENOUS INCOMPETENCE
CW DOPPLER, POSITIONING
how is the PT laying? les? HIP and KNEE? what is the position called?
PATIENT SUPINE •
LEG EXTERNALLY ROTATED, HIP AND KNEE FLEXED
• REVERSED TRENDELENBURG’S POSITION
CW DOPPLER • LIMITATIONS name 8
DIFFICULT TO DIFFERENTIATE THE CAUSE OF ABNORMAL FLOW PATTERN •
DVT VS. EXTRINSIC COMPRESSION •
FLOW PATTERNS MAY BE NORMAL IN PARTIAL THROMBOSIS
• FLOW PATTERNS MAY BE NORMAL IN CASES OF COLLATERALIZATION
FALSE NEGATIVE IN DUPLICATED SYSTEMS •
ISOLATED CALF VEIN THROMBOSIS DIFFICULT •
REQUIRES EXPERIENCED SONOGRAPHER •
INFORMATION IS MORE SUBJECTIVE AND OPEN TO INTERPRETATION
CW DOPPLER • TECHNIQUE
what probe is used?
what angle to skin surface?
correct vessel ID depends on what?
EXAM IS BASED ON EVALUATION OF?
5 MHZ PROBE •
45-60° TO SKIN SURFACE •
CORRECT VESSEL ID DEPENDS ON HEARING THE CORRESPONDING ARTERIAL SIGNAL •
EXAM IS BASED ON EVALUATION OF AUDITORY VENOUS SIGNAL IN THE RESTING LIMB AND WITH PROXIMAL AND DISTAL COMPRESSION
You are listening to the vein signal (sound) at rest and when you compress the limb
🔊 “Auditory venous signal”
👉 With continuous wave (CW) Doppler, you’re not looking at an image
👉 You are LISTENING to blood flow
🧠 The 3 parts of the exam: 1. 🟢 Resting limb
Just listen to the vein normally
Should hear:
Spontaneous flow
Phasic flow (changes with breathing)
2. ✋ Distal compression (below probe)
👉 You squeeze the leg below where you’re listening
Normal:
💥 BIG increase in sound (augmentation)
Abnormal (DVT):
❌ Little or no increase
→ suggests obstruction
3. ✋ Proximal compression (above probe)
👉 You squeeze above the probe
Normal:
❌ Flow should STOP
Abnormal (reflux):
🚨 You hear flow DURING compression
→ blood is going backward (reflux)
🔑 Easy way to remember:
Distal squeeze = push blood TO probe (should increase)
Proximal squeeze = push blood AWAY (should stop)
🩺 What you’re testing:
Obstruction (DVT) → poor augmentation
Venous insufficiency → flow during proximal compression
🔥 Exam one-liner:
CW Doppler evaluates venous flow by listening at rest and assessing changes with distal (augmentation) and proximal (reflux) compression
CW DOPPLER • TECHNIQUE
begin on what side at what ligament?
ID what?
what are the 4 venous signal?
BEGIN ON ASYMPTOMATIC SIDE AT INGUINAL LIGAMENT
•ID CFA, MOVE MEDIAL ID CFV •
VENOUS SIGNAL •
SPONTANEOUS •
PHASIC •
AUGMENTS WITH DISTAL COMPRESSION/PROX RELEASE •
NORMAL VALSALVA RESPONSE
CW DOPPLER • TECHNIQUE
evaluate what vein on what side for what>
also evaluation of what veins ?
EVALUATE CFV ON CONTRALATERAL SIDE FOR SAME FLOW PATTERN AND RESPONSE AS ASYMPTOMATIC
• EVALUATION OF FV, POP, AND PTV IS CONDUCTED AS PREVIOUSLY DESCRIBED
CW DOPPLER • INTERPRETATION • SPONTANEITY?
DOPPLER SIGNAL MUST BE CLEARLY HEARD AT ALL SITES (EXCEPT PTV)
CW DOPPLER INTERPRETATION, • RESPIRATORY PATTERNS
SIGNAL INCREASES WITH EXPIRATION, DECREASES WITH INSPIRATION
CW DOPPLER •INTERPRETATION • AUGMENTATION
DISTAL COMPRESSION SHOULD INCREASE SIGNAL
CW DOPPLER INTERPRETATION • AUGMENTATION, DVT/OBSTRUCTION
• SIGNAL PRESENT ONLY AFTER AUGMENTATION •
ABSENCE OF AUGMENTATION WITH DISTAL COMPRESSION
“Signal present ONLY after augmentation”
🧠 What it means:
At rest → you hear nothing (or very weak flow) ❌
When you squeeze distal → suddenly you hear flow ✅
🚨 Why?
👉 There’s an obstruction (DVT) blocking normal flow
Blood can’t flow on its own
Only moves when you force it with compression
🔑 Translation:
Flow is not spontaneous → needs help → abnormal → obstruction
🩺 2.
“Absence of augmentation with distal compression”
🧠 What it means:
You squeeze distal
❌ NO increase in signal
🚨 Why?
👉 There is a complete or significant blockage
Blood cannot pass through at all
So squeezing does nothing
🔑 Translation:
You push… but nothing moves → severe obstruction
🔥 Put them together:
Finding | What it means |
|---|---|
Only heard after augmentation | Partial obstruction (flow needs help) |
No augmentation at all | Severe/complete obstruction |
🧠 Easy way to remember:
No spontaneous flow = problem
No response to squeeze = BIG problem
🩺 Exam one-liner:
DVT is suggested by absent spontaneous flow and abnormal response to distal compression (either only present with augmentation or absent augmentation
CW DOPPLER •INTERPRETATION, VENOUS INSUFFICIENCY
AUGMENTATION DURING PROXIMAL COMPRESSION
Proximal compression (above probe)
👉 You are pushing blood away from the probe
✅ NORMAL:
🚫 Flow STOPS
You should hear silence
🚨 Now — venous insufficiency ❌ ABNORMAL:
👉 When you compress proximally…
💥 You hear augmentation (increase in signal)
Blood is moving TOWARD the probe instead of away
🧠 Why?
👉 Valves are incompetent
So when you push:
Blood leaks backward (reflux)
Travels downward toward the probe
🔥 So what are you supposed to see/hear? 🎧 Answer:
A burst/increase in Doppler signal DURING proximal compression
CW DOPPLER • INTERPRETATION • VALSALVA
NORMAL VS VENOUS INSUFFICIENCY
NORMAL = VENOUS AUGMENTATION FOLLOWING RELEASE OF MANEUVER •
VENOUS INSUFFICIENCY= AUGMENTATION DURING MANEUVER
🫁 What is the Valsalva maneuver?
👉 Patient bears down / holds breath (like straining)
👉 This increases pressure in the chest/abdomen
🩺 What should happen? ✅ NORMAL:
During Valsalva → 🚫 flow STOPS
After release → 💥 brief augmentation
👉 Why?
Pressure temporarily blocks venous return
When released → blood rushes forward → augmentation AFTER
🚨 VENOUS INSUFFICIENCY:
During Valsalva → 💥 augmentation happens DURING
👉 That is WRONG direction
🧠 Why does that happen?
👉 Valves are incompetent
So when pressure increases:
Blood is pushed backward (reflux)
You hear flow while they are straining
🔥 Key difference:
Phase | Normal | Venous Insufficiency |
|---|---|---|
During Valsalva | ❌ No flow | 💥 Flow (reflux) |
After release | 💥 Augmentation | May already have occurred |
🔑 Easy way to remember:
Normal = quiet during, loud after
Insufficiency = loud during
🩺 Exam one-liner:
Augmentation during Valsalva indicates venous insufficiency due to valvular incompetence
:
CW DOPPLER • INTERPRETATION • VALSALVA
what can alter normal flow?
what is VERY PULSATILE FLOW EVIDENT of what?
• EXTRINSIC COMPRESSION- CAN ALTER NORMAL FLOW
• FLUID OVERLOAD- VERY PULSATILE FLOW EVIDENT (CHF/ OVER HYDRATION)
MISCELLANEOUS EXAMS name two
IMPEDANCE PLETHYSMOGRAPHY (IPG) •
STRAIN GAUGE PLETHYSMOGRAPHY (SPG)
MISCELLANEOUS EXAMS
these methods measure what, by what?
these exams have been what by other methods?
THESE METHODS MEASURE THE CHANGE IN RESISTANCE; EITHER BY CALF VOLUME (IPG) OR CALF CIRCUMFERENCE (SPG) •
THESE EXAMS HAVE BEEN REPLACED BY OTHER METHODS