memory and dementia
1/140
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
141 Terms
What is Learning?
The acquisition of new information or knowledge.
What is Memory?
The storage or retention of acquired knowledge.
What is an Engram?
The physical representation or location of memory.
What term refers to the physical representation or location of a memory in the brain?
Engram
What are the three main types of Memory?
Declarative, Emotional, and Procedural memory.
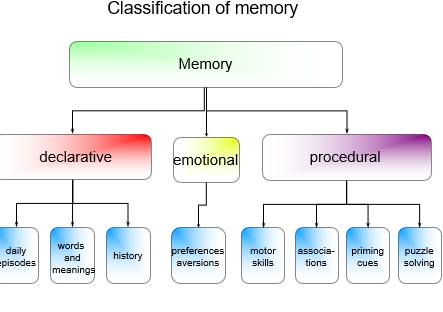
Q: What is Declarative Memory?
Memory for facts and events, such as daily episodes, words, and meanings.
hat is Emotional Memory?
Memory linked to feelings, including preferential or aversive responses.
What type of memory is associated with preferential or aversive reactions to experiences?
Emotional memory.
What is Procedural Memory?
Memory for skills and habits, such as motor skills, associations, puzzle solving, and priming cues.
Which brain areas are mainly involved in Declarative Memory?
The hippocampus and cortical association areas — especially the temporal, parietal, and prefrontal regions.
Which brain regions are most associated with Emotional Memory?
The amygdala and hypothalamus, which connect emotional experiences to autonomic and hormonal responses.
Which brain structures are involved in Procedural Memory?
The cerebellum, striatum, brainstem, and spinal cord, supporting motor skills, habits, and associative learning.
In the context of dementia, which brain region is most vulnerable and critical for memory loss?
The hippocampus, as its degeneration leads to major impairments in declarative memory and new learning.
hich brain regions are less affected in early dementia, preserving procedural memory?
The cerebellum and striatum, allowing motor skills and habits to remain relatively intact in early stages.
What does the term Engram refer to in memory?
: The physical representation or pattern of strengthened synapses that stores a memory in the brain.
What is Hebb’s Law?
“Neurons that fire together, wire together” — synapses are strengthened by intense or repeated activity.
According to Hebb’s Law, how does learning occur at the neuronal level?
Through strengthening of synaptic connections between neurons that are repeatedly activated together.
How does the Engram relate to Hebb’s Law?
The pattern of strengthened synapses (as described by Hebb’s Law) forms the engram, the neural basis of memory.
In relation to dementia, what happens to engrams?
: Synaptic loss and neuronal degeneration disrupt the engrams, leading to memory loss and impaired recall.
How does a synapse become stronger?
Through brief, repetitive synaptic activation, which increases the efficiency of neurotransmission.
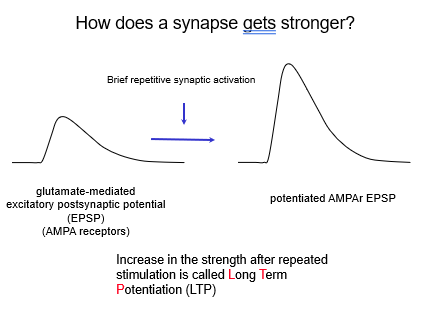
: What neurotransmitter is primarily involved in strengthening synapses?
Glutamate, which produces an excitatory postsynaptic potential (EPSP).
Which receptors mediate glutamate’s excitatory effect at the synapse?
: AMPA receptors (AMPAr).
What happens to AMPA receptor activity during repeated stimulation?
The EPSP mediated by AMPA receptors becomes stronger, leading to enhanced synaptic transmission.
What is the process called when a synapse increases in strength after repeated stimulation?
Long-Term Potentiation (LTP).
How is Long-Term Potentiation (LTP) related to memory?
LTP is considered the cellular basis of learning and memory, as it strengthens the connections between neurons.
In dementia, how might synaptic strengthening be affected?
: LTP mechanisms are impaired, reducing the brain’s ability to form and retain new memories.
What makes a synapse stronger?
: Repeated, brief activation of the same pathway — the more it fires, the stronger the connection becomes.
hich neurotransmitter strengthens synaptic connections?
Glutamate, which excites the next neuron and produces an excitatory postsynaptic potential (EPSP).
What receptors respond to glutamate to create the EPSP?
AMPA receptors, which open to let positive ions in and excite the postsynaptic cell.
What happens to AMPA receptors with repeated stimulation?
They become more responsive or increase in number, making the EPSP stronger each time.
What is it called when repeated stimulation makes a synapse stronger over time?
Long-Term Potentiation (LTP) — a long-lasting increase in synaptic strength.
Why is Long-Term Potentiation (LTP) important?
It’s the cellular basis for learning and memory — how the brain “locks in” new information.
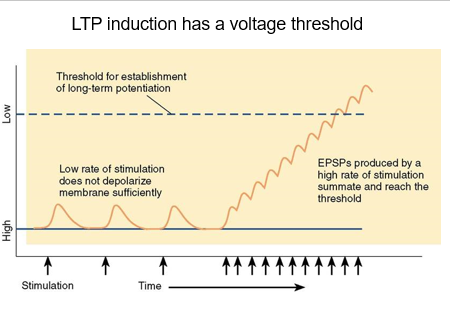
Does LTP happen with any level of stimulation?
No — LTP has a voltage threshold. The membrane must be sufficiently depolarized to trigger it.
What happens if the synapse is stimulated at a low rate?
Low-rate stimulation doesn’t depolarize the membrane enough, so LTP is not established.
How is the threshold for LTP reached?
High-rate stimulation produces EPSPs that summate, depolarizing the membrane enough to cross the LTP threshold.
Why is high-frequency stimulation important for memory formation?
: Because it allows synapses to reach the depolarization threshold, strengthening connections and supporting long-term memory.
In terms of membrane potential, what does “high” and “low” mean?
High = hyperpolarized (more negative, harder to reach threshold)
Low = relatively depolarized (less negative, closer to threshold for LTP)
How does membrane potential affect LTP induction?
LTP is easier to induce when the membrane is relatively depolarized (low) and harder when it’s hyperpolarized (high).
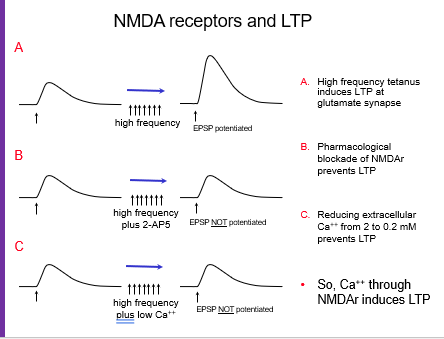
What happens at a glutamate synapse during high-frequency stimulation?
EPSPs are potentiated, and high-frequency tetanus can induce LTP.
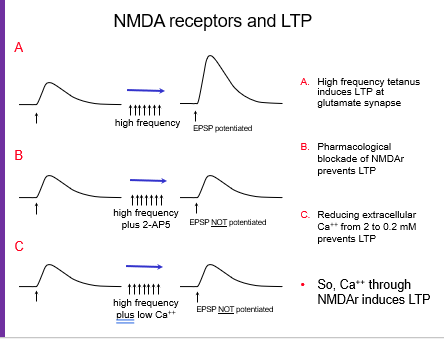
What happens if NMDA receptors are blocked during high-frequency stimulation (e.g., with 2-AP5)?
EPSPs are not potentiated — pharmacological blockade of NMDA receptors prevents LTP.
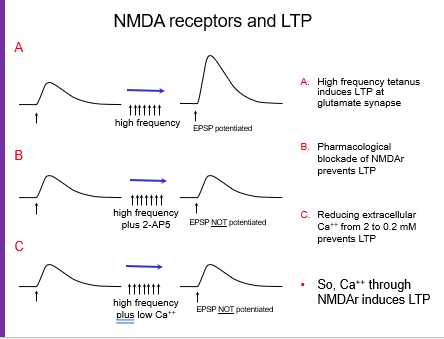
What happens if calcium levels are low during high-frequency stimulation?
EPSPs are not potentiated, showing that calcium entry through NMDA receptors is essential for LTP.
What is the role of NMDA receptors in LTP?
They allow calcium to enter the postsynaptic neuron during strong stimulation, which triggers synaptic strengthening.
How do these NMDA receptor experiments show the mechanism of LTP?
They show that high-frequency stimulation alone isn’t enough; NMDA receptor activation and calcium influx are required for LTP to occur.
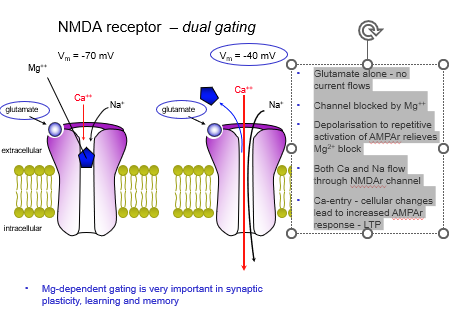
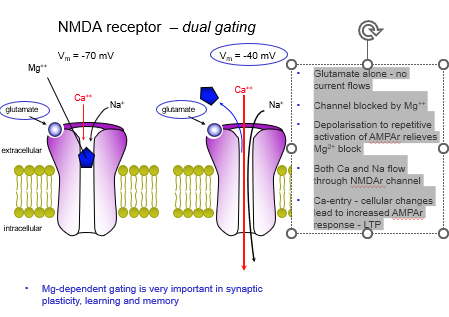
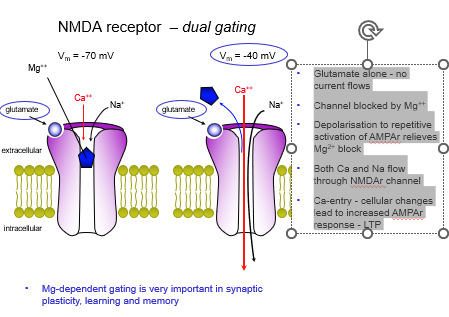
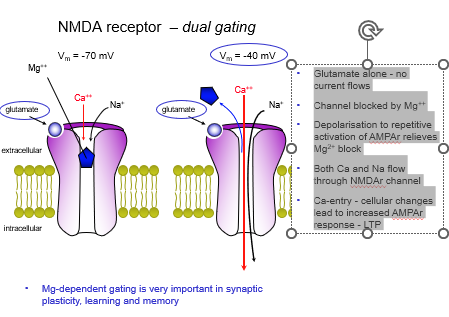
What is dual gating of NMDA receptors?
NMDA receptors require both glutamate binding and postsynaptic depolarization to open.
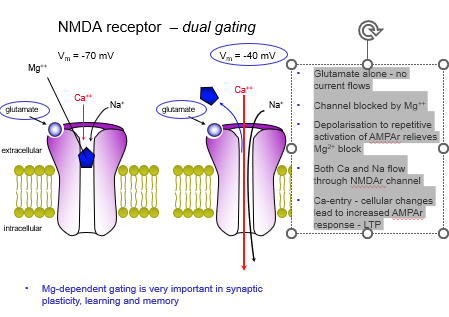
What happens to NMDA receptors at resting potential (-70 mV) when glutamate binds?
The channel is blocked by Mg²⁺, so no current flows.
How is the Mg²⁺ block relieved?
glutamate released causes repetitive AMPA receptor activation on postsynaptic, postsynaptic membrane depolarises, this causes mg2+ block on NMDA to be removed.
What ions flow through the NMDA receptor once the Mg²⁺ block is removed?
Calcium (Ca²⁺) and sodium (Na⁺) enter the postsynaptic cell.
Why is calcium entry through NMDA receptors important?
Ca²⁺ triggers cellular changes that increase AMPA receptor responses, leading to LTP.
Why is Mg²⁺-dependent gating critical for learning and memory?
It ensures synaptic plasticity only occurs with strong, coincident activity, which is essential for memory formation.
What does “dual gating” mean for NMDA receptors?
hey only open when glutamate binds and the postsynaptic cell is depolarized.
At resting potential (-70 mV), what happens if glutamate binds NMDA receptors?
The channel is blocked by Mg²⁺, so no ions can flow in.
How is the Mg²⁺ block removed?
Repetitive activation of AMPA receptors depolarizes the membrane, kicking out the Mg²⁺.
Which ions enter the cell through NMDA receptors once the Mg²⁺ block is gone?
: Calcium (Ca²⁺) and sodium (Na⁺) flow in.
Why is calcium entry so important for LTP?
Calcium triggers changes that boost AMPA receptor responses, strengthening the synapse — this is LTP.
Why is Mg²⁺-dependent gating essential for learning and memory?
It makes sure synapses only strengthen with strong, repeated activity, which is key for forming memories.
: How is LTP expressed postsynaptically?
By adding more AMPA receptors, making AMPA receptors more sensitive, and sometimes forming new synapses.
How is LTP expressed presynaptically?
: By releasing more glutamate, forming more release sites, and having more vesicles ready for release.
What is the overall effect of these pre- and postsynaptic changes?
Synapses become stronger and more efficient, enhancing neuronal communication and supporting learning and memory.
: Why do both pre- and postsynaptic changes matter for memory?
Because LTP requires more neurotransmitter release and stronger postsynaptic responses to consolidate memory effectively.
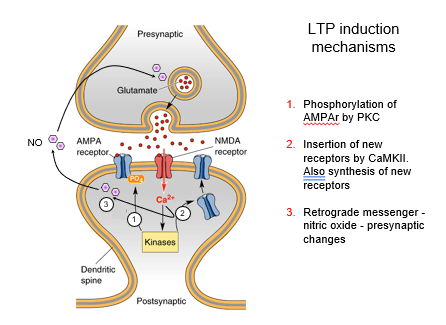
How does phosphorylation affect AMPA receptors during LTP?
Kinases like PKC, PKA, and CaMKII phosphorylate AMPA receptors, making them more sensitive to glutamate.
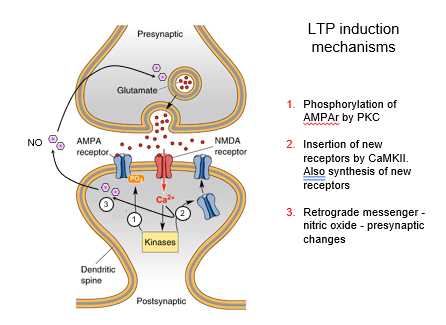
How are new AMPA receptors added to the postsynaptic membrane?
CaMKII helps insert new AMPA receptors, increasing postsynaptic responsiveness.
What is the role of AMPA receptor synthesis and subunit exchange?
To maintain and strengthen synaptic responses over time during LTP.
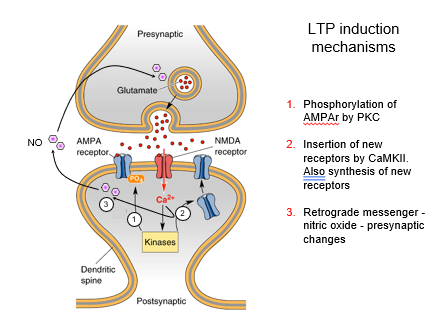
How do retrograde messengers contribute to LTP?
Substances like nitric oxide (NO) signal back to the presynaptic terminal to increase glutamate release and enhance presynaptic function.
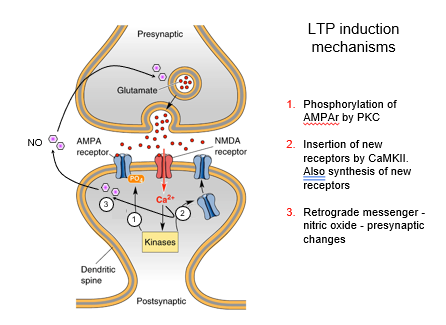
Which kinases are involved in LTP induction?
PKC, PKA, and CaMKII — all contribute to phosphorylation and receptor insertion.
How do these postsynaptic and presynaptic changes work together?
Stronger postsynaptic AMPA responses plus increased presynaptic glutamate release produce robust, long-lasting LTP, the basis of memory formation.
Which receptor triggers LTP induction?
NMDA receptor — activated by glutamate and depolarization.
How is LTP expressed at the synapse?
Through AMPA receptor activity — either more receptors or increased sensitivity.
How is LTP maintained postsynaptically?
By long-lasting changes in AMPA receptor number/sensitivity and structural changes like new dendritic spines.
How is LTP maintained presynaptically?
hrough increased glutamate release, more vesicles, and additional release sites.
Which systems modulate LTP and memory formation?
Diffuse amine systems (dopamine, noradrenaline) and cholinergic systems, which enhance or weaken synaptic plasticity.
How do all these mechanisms link together in memory?
: NMDA receptor activation → AMPA receptor expression → structural and presynaptic changes → neuromodulatory influence = LTP, the cellular basis of memory.
Do cognition enhancers improve memory in healthy people?
No — there is no evidence they benefit individuals without cognitive impairment.
Which cholinergic drugs are used to enhance cognition in dementia?
Anticholinesterases (donepezil, galantamine) and agonists (nicotine, arecoline).
How do stimulants like amphetamine, methylphenidate, modafinil, and caffeine affect cognition?
Likely via dopamine, may enhance alertness or productivity, but limited evidence for true cognitive improvement in healthy people.
Which serotonin drugs may enhance cognition?
5HT6 antagonists.
How do GABAergic drugs potentially enhance cognition?
GABAA receptor blockers/inverse agonists (e.g., suritozole) increase excitability and may improve cognitive function.
Which glutamate-based drugs are cognition enhancers?
AMPAkines (piracetam, IDRA-21) and mGluR5 positive allosteric modulators. They enhance AMPA/mGluR receptor activity and support memory.
Overall, which neurotransmitter systems are targeted by cognition enhancers?
cholinergic, dopaminergic, serotonergic, GABAergic, and glutamatergic systems
What are the main causes of amnesia?
Drug-induced (e.g., alcohol) or head trauma.
What are the two types of amnesia?
Retrograde (loss of past memories) and anterograde (inability to form new memories).
Q: How is dementia defined?
A syndrome of cognitive decline sufficient to impair social and occupational function.
Which memory problems occur in dementia?
Loss of multiple memory types, especially inability to form new memories (learning)
What is often the first presenting symptom of dementia?
Memory impairment
How does dementia differ from amnesia?
Dementia involves progressive general cognitive decline affecting multiple domains, whereas amnesia is usually isolated memory loss from trauma or drugs.
What is the most common dementia in people over 65?
Alzheimer’s disease.
What is the female:male ratio in Alzheimer’s?
2:1 (more common in females).
What is usually the first presenting symptom of Alzheimer’s?
A: Memory deficits.
What are initiation deficits in Alzheimer’s?
Difficulty starting tasks or activities.
What visuo-spatial problems occur in Alzheimer’s?
roblems with navigation, depth perception, and spatial tasks.
What language deficits occur in Alzheimer’s?
Word-finding difficulties, comprehension problems, paraphasia.
What executive function deficits occur in Alzheimer’s?
impaired judgment, planning, and risk assessment
: Can Alzheimer’s patients experience psychotic episodes?
Yes, some patients may develop psychotic symptoms.
Which brain areas show early shrinkage in Alzheimer’s?
Temporal poles and frontal cortex.
Which area is damaged earliest in Alzheimer’s and contributes to memory and speech deficits?
Entorhinal cortex.
How does Alzheimer’s pathology progress?
Spreads to the whole cortex and subcortical structures.
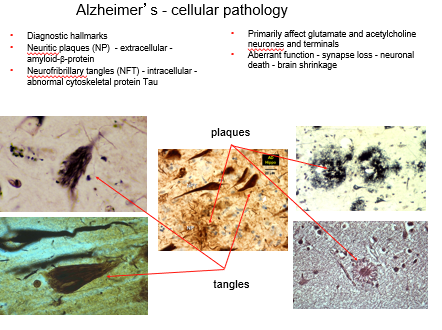
What are the diagnostic hallmarks of Alzheimer’s?
Neuritic plaques (amyloid-β, extracellular) and neurofibrillary tangles (tau, intracellular).
Which neurons are primarily affected in Alzheimer’s?
Glutamatergic and cholinergic neurons and their terminals.
What are the main consequences of Alzheimer’s pathology?
Aberrant function → synapse loss → neuronal death → brain shrinkage with intracellular tangles and extracellular plaques.
How do plaques and tangles relate to symptoms?
They cause loss of synapses and neurons, leading to memory, language, and executive deficits.
Which brain areas show early shrinkage in Alzheimer’s, and why is this important?
: Temporal poles and frontal cortex. Early shrinkage in these regions affects memory, executive function, and planning.