AP Psych Unit 5- Mental and Physical Health, Different Therapies/ Treatments
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
55 Terms
Schizophrenia:
-Psychotic Disorder: Distorts reality
-Strikes during adolescence or early adulthood.
-Spectrum disorder (Variety of levels)
-Triggered by stress
-Diathesis Stress Model: More stress and bad lifestyle triggers schizophrenia.
Positive Symptoms:
Positive Symptoms: Presence of unwanted behaviors. It is adding behaviors, not positive itself.
Hallucinations: Unreal sensory perceptions (Seeing, hearing, or feeling things
Delusions: Beliefs not based in reality. Example: The tv is talking to me.
Delusions of Persecution or Grandeur: A delusion of persecution is the belief that someone is out to get you, and you start to distrust people. A delusion of grandeur is the belief that you are very powerful and have superpowers.
Disorganized thinking
Disorganized motor behavior
Negative Symptoms:
-Absence of desired behaviors. They lose things that were normally there.
-Flat Affect- An inability to show emotion
-Inappropriate Affect- Wrong emotional response. Someone cries when someone tells a joke.
-Catatonia- inability to move
Causes of Schizophrenia:
-Dopamine Hypothesis: Schizophrenia is associated with high levels of dopamine (Too much). This is why antipsychotics are used. Very high dopamine causes no movement. Low dopamine causes a lot of movement.
-Genetics
-Enlarged Brain Ventricles
-Exposure to Influenza in utero (Women who have the flu when pregnant have a higher chance of getting a kid with schizophrenia.
-Double Binds (Psychoanalytic View): Environments where conflicting messages are given. No consistency can cause a break of reality.
Schizophrenia Treatment:
-Antipsychotics reduce hallucinations resulting from schizophrenia.
-Side Effect: Tardive Dyskinesia (involuntary facial movements)
-Cognitive-Behavioral Therapy: This therapy checks reality and monitors stress
Personality Disorders:
-Extreme and inflexible personality traits that cause problems for the individual and those around them.
-It is very difficult to treat because they make up the patient's personality.
Antisocial Personality Disorder:
-Deceitfulness, impulsivity, a disregard for the safety of others, and little to no remorse for actions.
-Cognitive Behavioral Therapy (CBT): This helps the patient learn how they are responsible for their actions and behaviors.
MacDonald Triad: Animal cruelty, Fire starting, and bed wetting.
Medication: Lithium helps reduce aggression.
Borderline Personality Disorder (BPD)
-Extreme fluctuations in mood or behavior and makes relationships difficult to maintain.
-Promiscuity, black and white thinking (One extreme or the other), and self-harm.
-Cognitive Behavioral Treatment (CBT) Treatment: This teaches patients to take control of their lives, emotions, and themselves.
Histrionic Personality Disorder (HPD):
-An extreme need for attention, highly dramatic, emotionally needy, and insecure.
-It is difficult to treat but therapists are recommended to approach patients skeptically due to the use of exaggeration.

Narcissistic Personality Disorder
-Inflated sense of self and importance.
-Requires constant attention, easily jealous, and often lacks empathy.
-Therapists are advised to avoid therapy that heightens grandiose feelings or devalues the patient.
Dependent Personality:
The identifying feature of the dependent personality disorder is the heavy reliance on others. This takes many forms. The dependent person relies on others to accept responsibility for his or her life. This means that major decisions are deferred to another person. Dependent people tend to lack self-confidence, seeing themselves as helpless, inadequate, or dumb. As soon as they find a person willing to be supportive and engage in making those types of decisions, they will tolerate being dominated, even mentally or physically abused, in order to maintain a relationship.
Paranoid Personality:
Paranoid Personalities believe others to be hostile toward them and want to take advantage of them. They are wary, suspicious, hypersensitive, distrustful, and they tend to ascribe evil motives to others. Such persons are envious of the better treatment they often believe others are receiving. Given these attitudes, those with paranoid personalities have difficulty maintaining relationships. They may become increasingly isolated and closed off to others.
Schizoid Personality:
Like paranoid personalities, schizoid personalities alienate themselves from other people. Unlike paranoid individuals, however, schizoid behaviors are based not on active wariness but on a shy seclusiveness. Individuals with this personality disorder tend to be introverted, seclusive, and reserved. Instead of seeking out companionship, they find little need for other people and are emotionally independent. Their daydreams and fantasies may be intense and emotional and are oversensitive to others’ attitudes and actions. Thus the lack of emotional reactions is actually a defense against pains of rejection, depreciation, or punishment.
Schizotypal Personality:
Schizotypal personality is marked by discomfort with close relationships as well as by cognitive or perceptual distortions of behavior. They maintain odd beliefs and/or the notion that thoughts can produce actions. Those with schizotypal personalities harbor suspiciousness or paranoid ideation and display inappropriate or constricted emotions. Their behavior or appearance that is at times odd, eccentric, or peculiar socially, they lack close friends or confidants other than first degree relatives. Excessive social anxiety does not diminish with familiarity and tends to be associated with paranoid fears rather than negative judgments about themselves.
Different between Schizoid and Schizotypal:
People with Schizoid are isolated.
People with SchizotyPAL have friends/pals.
Avoidant Personality:
This disorder involves a pervasive pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation, beginning by early adulthood and may be present in a variety of contexts. Interpersonal interactions are usually avoided because of a fear of criticism, disapproval, or rejection. They are unwilling to get involved with people unless they are certain of being liked. In intimate relationships, they show restraint in order to avoid being shamed or ridiculed and are preoccupied with being criticized or rejected in social situations. They are unusually reluctant to take personal risks or to engage in any new activities because they may prove embarrassing.
Obsessive-Compulsive Personality:
This is different than OCD because it is a personality.
The common characteristics of obsessive-compulsive personality disorder are a preoccupation with orderliness, perfectionism, and mental and interpersonal control, at the expense of flexibility, openness, and efficiency. They are preoccupied with details, rules, lists, order, organization, or schedules to the extent that the major point of the activity is lost. Individuals with this personality disorder show perfectionism that interferes with task completion. For example, they are unable to complete a project because his or her own overly strict standards are not met. They are often excessively devoted to work and productivity to the exclusion of leisure activities and friendships. Those with this disorder can be overconscientious, scrupulous, and inflexible about matters of morality, ethics, or values and are unable to discard worn out or worthless objects even when they have no sentimental value. They are reluctant to delegate tasks and display rigidity and stubbornness.
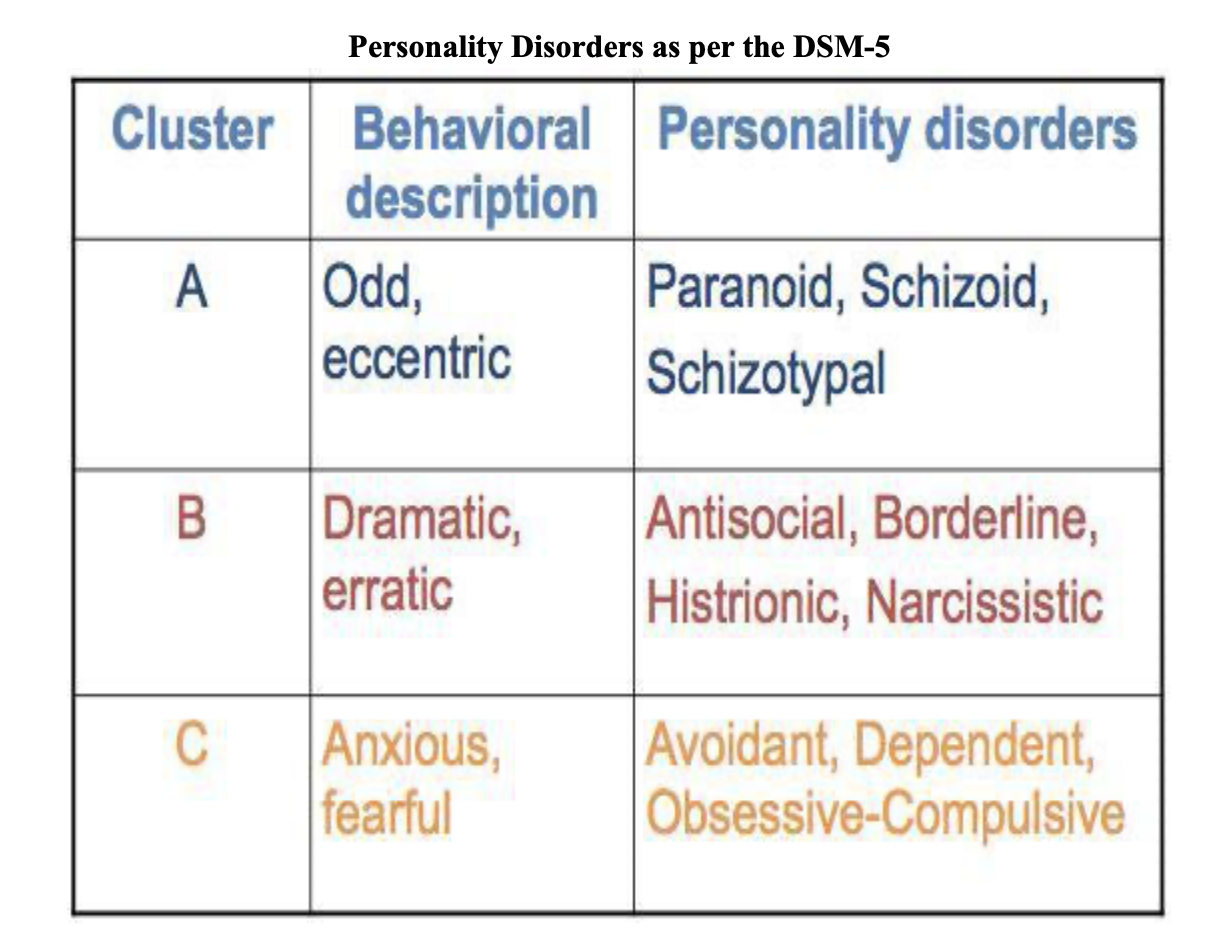
Personality Disorders as per the DSM-5:
Major Depressive Disorder:
Two or more weeks of depressed moods, feelings of worthlessness, and diminished interest or pleasure in activities. The difference between this and persistent depressive disorder is the time.
Persistent Depressive Disorder:
2 or more years of MDD.
Bipolar 1 Disorder vs. Bipolar II Disorder:
Bipolar 1 Disorder: Severe manic episodes, and depression is less severe. Someone experiences highs and lows, never in the middle. Number 1= The MANic.
Bipolar 2 Disorder: Alternates between severe depression and hypomania (lesser manic episodes).
Causes of Depressive and Bipolar Disorders:
-Genetics (35-40 %)
-Less brain activity during depressed states, more during mania
-Left Frontal Lobe: Positive feelings center is inactive. The right side is responsible for negative emotions.
-Depression: Low levels of norepinephrine (Arousal, motivation) and Serotonin
-Negative Thinking (COGNITIVE ASPECT)
-Learned helplessness (Seligman)
Anxiety Disorders:
Generalized Anxiety Disorder, Social Anxiety Disorder, Panic Dosorder, Tajijin Kyofusho, Ataque de Nervios
Generalized Anxiety Disorder:
Continual state of anxiety in general situations.
Social Anxiety Disorder:
Fear of social situations/activities.
Panic Disorder:
Sudden and unpredictable panic attacks.
Taijin kyofusho Japanese Variation:
Fear of body judgement
Ataque de Nervios:
Latino/Hispanic cultural variation
Obsessive Compulsive Disorder (OCD):
Obsessive thoughts that are coupled with compulsive actions to avoid anxious feelings.
Hoarding Disorder: Difficulty parting with possessions.
Post Traumatic Stress Disorder (PTSD):
Re-experiencing traumatic events in thoughts and dreams; avoiding stimuli associated with the event
Causes of Anxiety Disorders:
-Fears are learned via observational learning.
-Natural Selection: Fears tend to reflect ancestral concerns: Dangerous animals, heights, confinement, etc.
The amygdala (Emotion center) is overactive
Cause of OCD: Anterior Cingulate Cortex: Monitors actions and checks for error-hyperactive.
Cognitive Behavioral Therapy (CBT) Treatment for Anxiety:
This gets the patient to change irrational thoughts and behaviors.
Anti-Anxiety Drugs (Benzodiazepines):
Minor tranquilizers (Valium, Ativan)- increase GABA- Side Effects- addiction
Anti-Depressants:
Selective Serotonin Reuptake Inhibitors (SSRIs)- SSRI's ncrease Serotonin and keeps it there for a longer time. (& some Norepinephrine)- Zoloft, Paxil, Prozac, Lexapro, and Cymbalta.
SIde Effects of Anti-Depressants:
SIde Effects of Anti-Depressants: Weight gain, suicidal thoughts (if Norepinephrine increased)
Monoamine Oxidase Inhibitors (MAO Inhibitors):
This reduces the Breakdown of Seratonin and Norepinephrine.
Bipolar Disorder Treatment:
Lithium: Alters body salt levels- has stabilizing effect- Side Effects of Lithium: drowsiness, loss of appetite
Electroconvulsive Therapy (ECT):
This Induces seizures and alters brain functioning- used for major depression
TMS (Transcranial Magnetic Stimulation) Treatment:
Magnetic brain stimulation
ADHD (Neurodevelopmental Disorder) Treatment:
Ritalin (stimulant): This increases dopamine and norepinephrine.
Side Effects: Sleep problems
Dissociative disorders:
Dissociative disorders involve a prolonged loss of memory. They often create new identities, don’t remember who they are, wander off and disappear (Dissociative fugue), and they have more than 2 personalities.
Dissociative Amnesia:
The loss of information about one's self or life and forget their past
Dissociative Fugue:
A sudden and extreme memory disturbance in which individuals wander off, form new identities, without memory of prior life. When someone has a compulsive urge to travel and disappear. People forget who they are.
Dissociative Identity Disorder (Multiple Personality Disorder):
A person possesses two or more identities and they take control of the person's behavior periodically. Usually, one of the personalities is the "tough guy."
Somatic Symptom Disorders:
Disorders which involve physical pain and symptoms of disease or injury, but lack a physical origin. It originates as an untreated psychological condition. The pain is real and not faked (It is not physical, it is psychological.
Treatment for Somatic Symptom Disorders= CBT teaches patients to cope with stress.
Conversion Disorders:
Somatoform disorders that result in severe conditions like paralysis, blindness, etc.
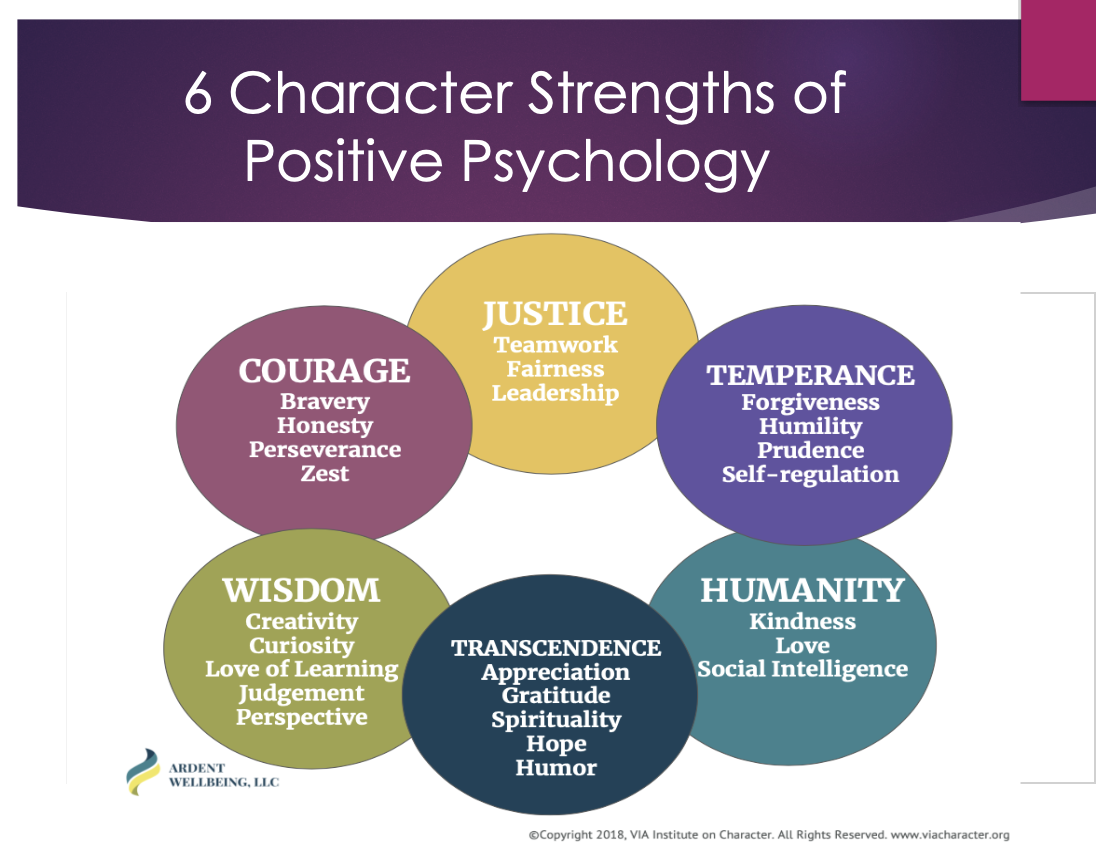
6 Character Strengths of Positive Psychology:
Courage, Justice, Temperance, Humanity, Transcendence, Wisdom, and Courage.
Psychodynamic Therapy/ Insight Therapy: Freudian Model
-Goal: Unconscious conflicts must be brought to the surface.
-Once root of disorder is found, the disorder will fade.
-Patients gained insight into themselves.
-Dream analysis.
Free Association Therapy:
A method of exploring the unconscious. A person relaxes and says whatever comes to mind no matter how unimportant or embarrassing.
Humanistic Therapy/ People Centered Therapy:
-Carl Rogers.
-Dream analysis.
-Goal: Clients become their "true" selves,
-Client Centered Therapy: An environment where the therapist offers only empathy and acceptance. Humanistic therapists do not call people their "patients," and they call them "clients." They don't even diagnose their clients.
-Eliminate conditions of worth-not being yourself to be accepted.
-Unconditional Positive Regard: The therapist will not challenge you.
Encounter groups.
Cognitive Behavioral Therapy:
It changes self defeating thinking and aims to change behavior.
Rational Emotive Behavioral Therapy/ Cognitive Behavioral Therapy:
-Albert Ellis: Rational Emotive Behavioral Therapy (REBT).
A (Adversity), B (Beliefs), C (Consequences). Adversity will happen like failing a test. Someone believes they are dumb and then will not try as hard and feel bad.
Cognitive Behavioral Therapy (CBT):
-Aaron Beck (CBT).
-Goal of CBT: Eliminate irrational beliefs.
-Irrational Beliefs: Anxiety about not meeting them. Failing to meet them. Depression is about more irrational beliefs.
-Becomes a self defeating cycle.
-The therapist must identify irrational beliefs and challenge them.
Eclectic Perspective:
-Most modern psychologists use more than one perspective when treating patients.