1023 Physio Foundations
1/88
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
89 Terms
Unilateral vs bilateral
Unilateral - involving one side of the body
Bilateral - involving both sides of the body
Ipsilateral vs Contralateral
Ipsilateral - on the same side of the body
Contralateral - on different sides of the body
Clinical reasoning cycle
Consider the patient information
Collective cues/information
gather
review
recall
process information
interpret
discriminate
relate
infer
match
predict
identify problems/issues
synthesise
establish goals
describe
take action
select
evaluate outcomes
evaluate
reflect on processes and new learning
contemplate
Clinical reasoning
develops with experience
process of collecting ang and interpreting information
formulate predictions about outcomes
known as:
decision making
problem solving
critical judgements
critical thinking
what is clinical reasoning influenced by
Clinician knowledge base
Scientific & professional
Personal experiences
Beliefs
Values
Skills
Clinical reasoning pathway just the steps
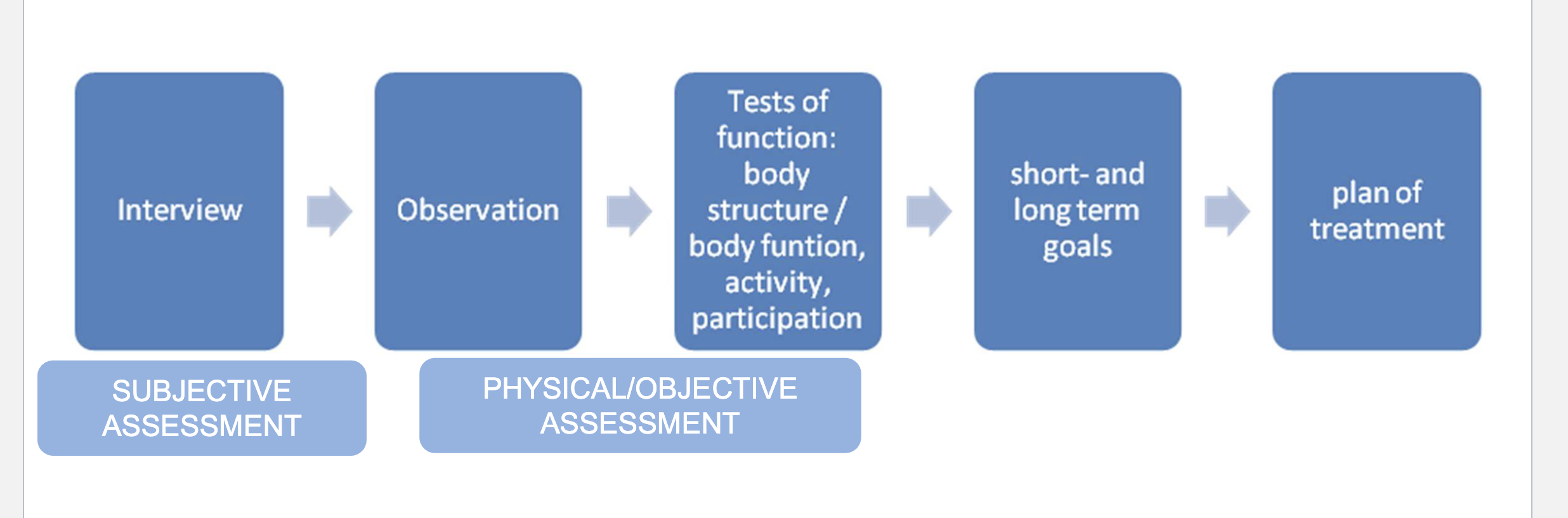
Clinical reasoning pathway 5 step summary
Interview - subjective assessment
Diagnostic hypotheses
Plan Physical/Objective assessment (how to test/measure/identify/characterise results - notice symptoms/dysfunctions)
Develop patient goals and a Treatment plan
observation/tests of body function - PHYSICAL/OBJECTIVEASSESSMENT
Process to establish:
Individual's specific diagnosis and prognosis
can i treat this with physiotherapy
short/long term goals and treatment plan - treatment plan
Judgments about diagnoses and prognoses
Consider an individual's goals and resources
Gathering information clinical reasoning steps
Subjective assessment
interview
objective assessment
observation
tests of body function
eg: Observation, Functional tests, Range of movement, Muscle strength etc
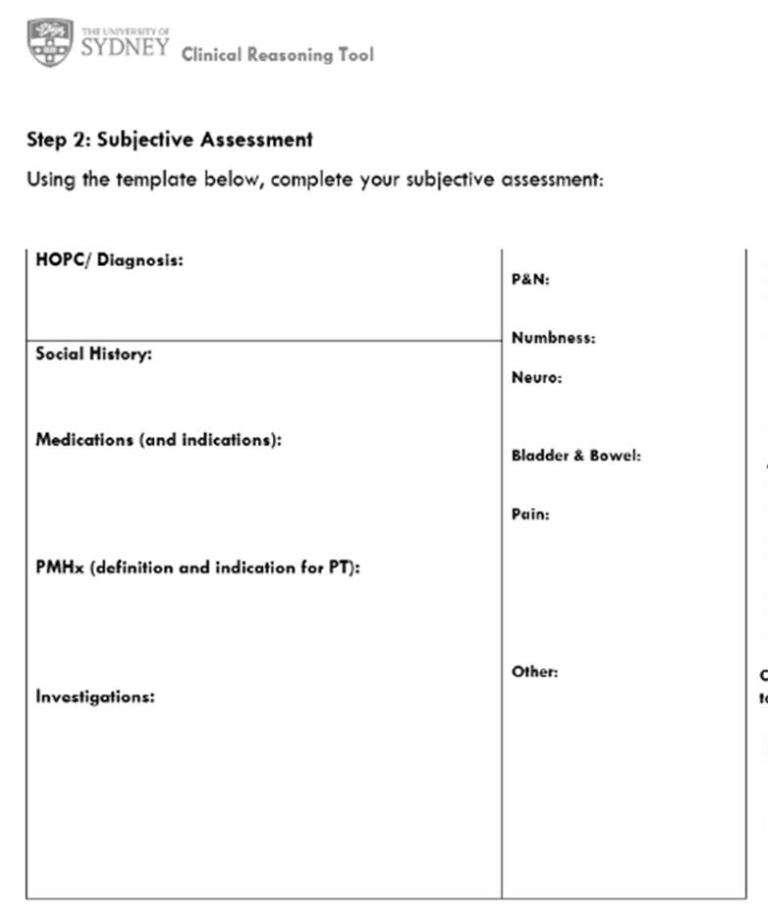
subjective assessment sample form
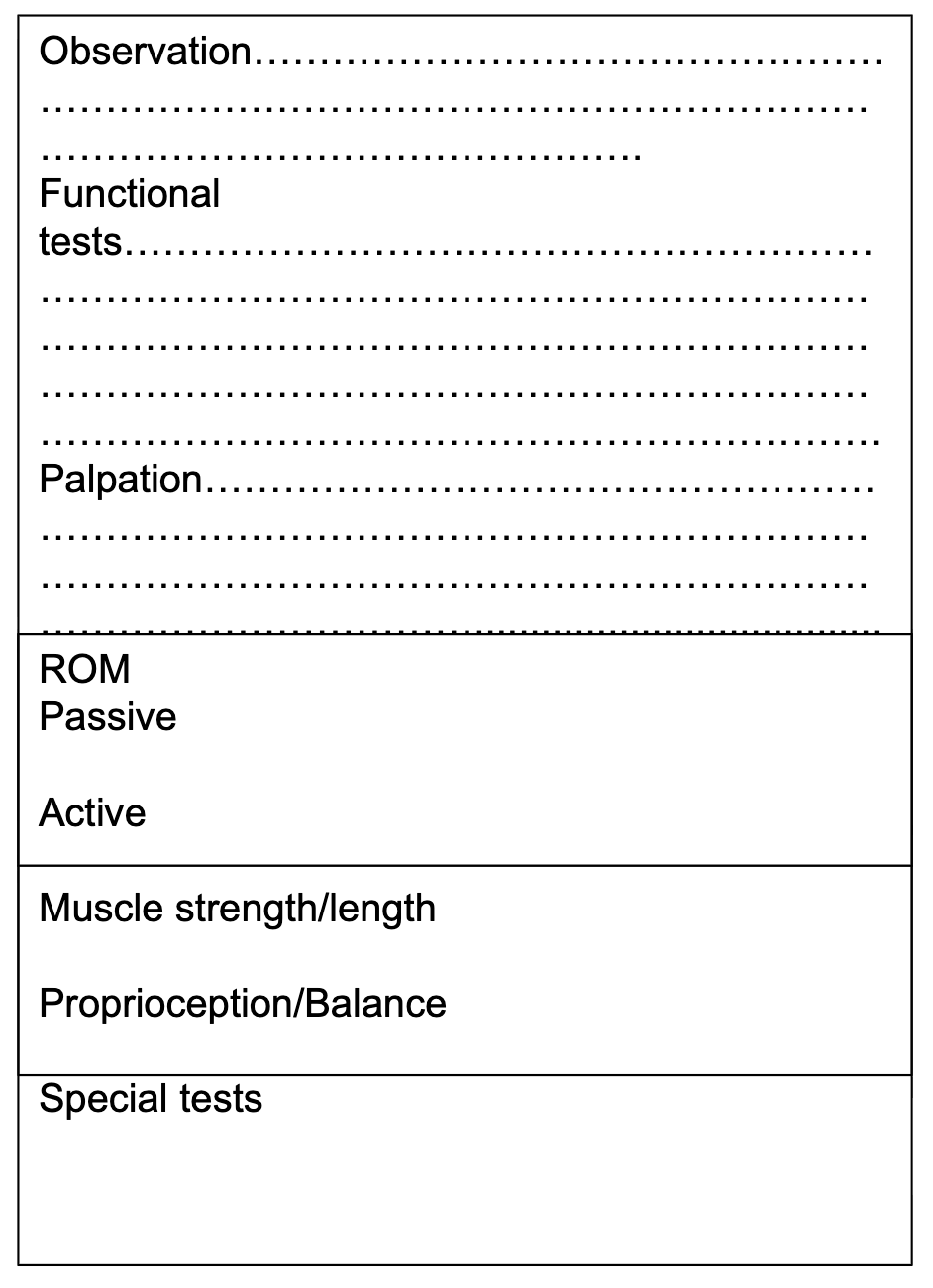
objective assessment sample
what things to consider when developing a hypothesis and processing information
how to target these impairments in physiotherapy? - also guide goals for treatment
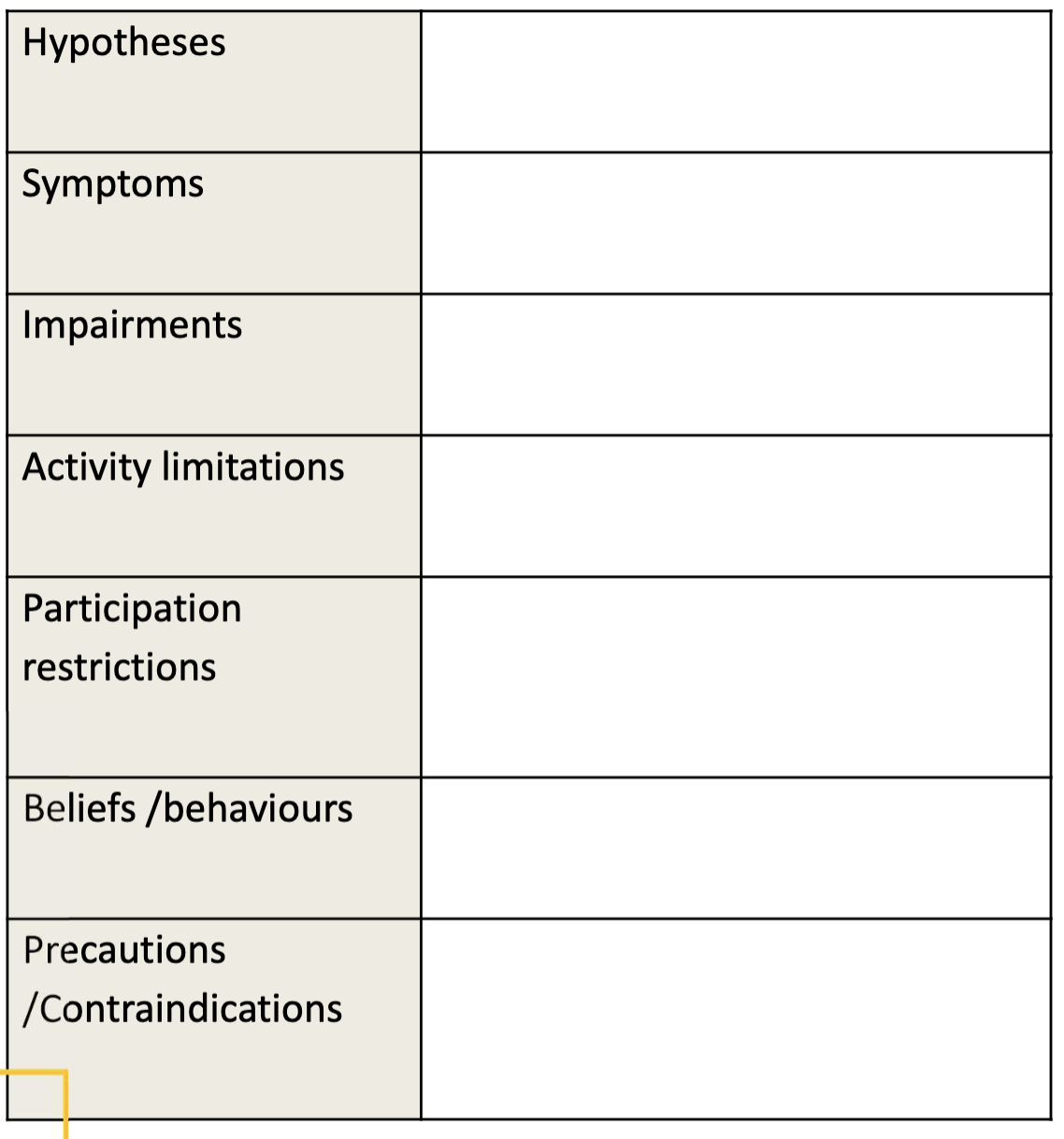
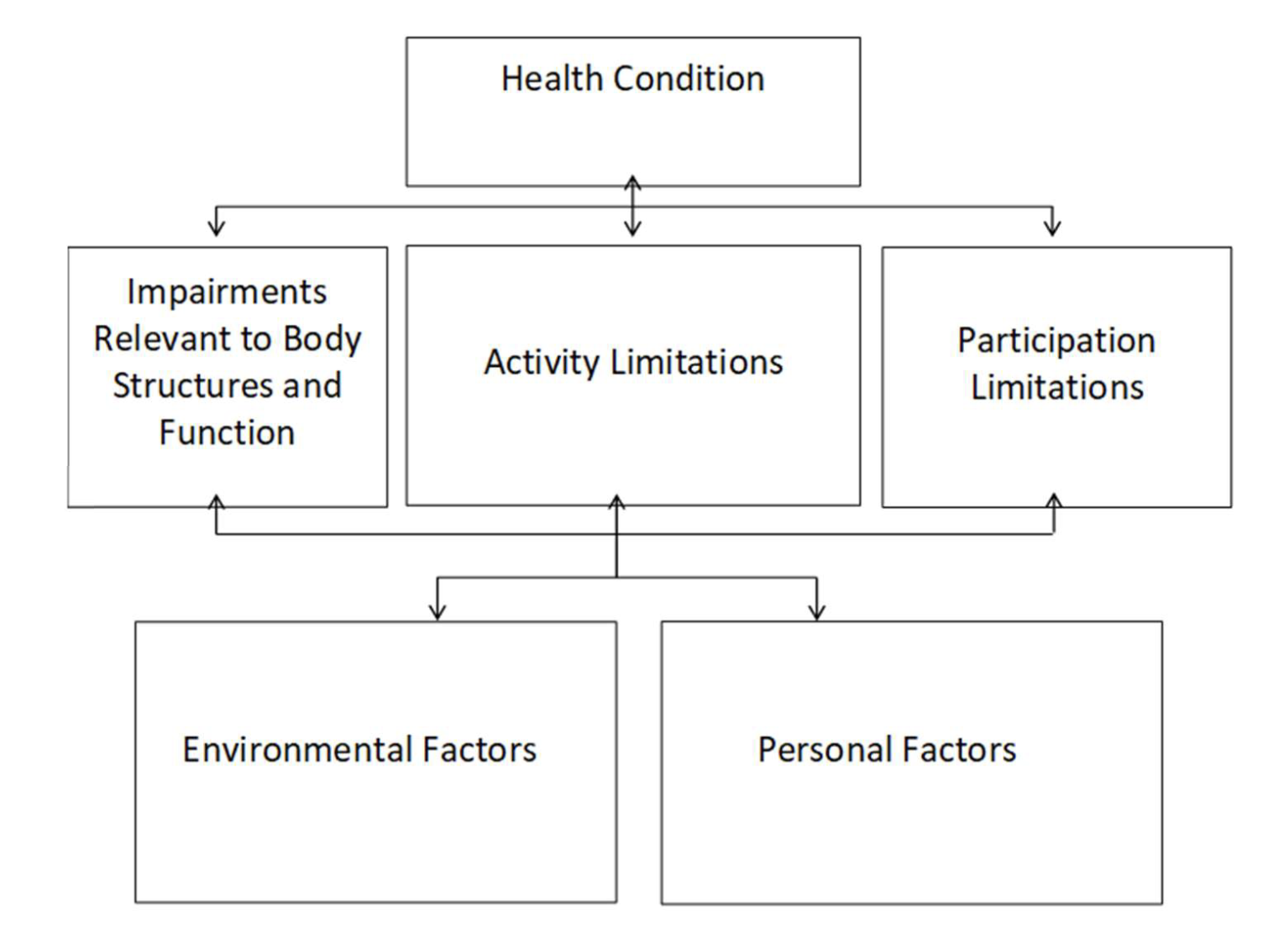
Synthesise - ICF framework
clinical reasoning cycle
gather
interpret
sythesise
describe
select
evaluate (may go back between select and evaluate if chosen treatment is not
contemplate
GISDSEC
GuIdeS and SEleCts
diagnosis vs prognosis
diagnosis:
reason for symptoms etc - causes of issue
Prognosis:
suggested response - decision on how to address issue
what are heuristics?
Generalisations/ rules of thumb/ educated guess
Efficient and automatic so decrease cognitive load
types of heuristics
availability heuristic
Pattern heuristic
Recognition heuristic:
explain availability heuristics
Tendency to rely on information that is easy to recall when making decisions.
Conversely, something that is hard to remember doesn’t get fed into the decision-making process as much.
eg: “I recently saw two disc herniations → this is probably another.”
explain pattern heuristics
It involves making judgments by comparing things to concepts/patterns we already have in mind.
Healthcare professionals may make diagnostic and treatment decisions based on how well a patient and their symptoms match an existing pattern/protoype.
Focuses on clinical features
matching up symptoms to a patter - thus subconsciously/consciously ask questions which suit that pattern
eg: “Young athlete and ankle swelling = lateral sprain”
explain recognition heuristics
mental shortcut in which a person judges that an option or explanation is more likely to be correct simply because it is familiar or recognised.
judgement is driven by recognition, not yet by formal testing.
eg: “I’ve seen this shoulder presentation many times before it looks like frozen shoulder.”
what is Hypothetico-deductive reasoning
Use heuristics and inductive/deductive/abductive/ rule based/ reasoning to make hypothesis
Iterative
Hypothesis modification
what is dual process thinking
Type 1 thinking
‘intuitive’
Fast
Automatic
Effortless
Experience based
Pattern recognition
Type 2 thinking
Analytic
Slow
Systematic
Logical
Effortful
what is effective clinical reasoning?
Good clinical skills
Use and interpret clinical tests
Understand cognitive biases and human factors
Meta-cognition (thinking about thinking)
Patient centred evidence-based therapy
Shared decision making
what is a cognitive bias
Thinking error
a predictable tendency in thinking to favour one perspective over others.
Not related to intelligence
Subconscious deviations in judgement which lead to :
Perceptual distortions
Inaccurate judgement
Illogical interpretation
Types of cognitive biasse
Blind spot bias - able to see others biases but neglecting our own
Anchoring/Primacy - rely more heavily to an initial piece of information, failing to adjust with new info
Premature closure - prematurely decide on hypothesis before propper/full exploration
Diagnostic momentum - attached to one diagnostic label which gathers momentum with each revision - blinding to new possibilities
Confirmation bias - give more attention/focus on information that fits with our existing beliefs - less critical reflection
Ascertainment bias - thinking is shaped by previous expectations - what we expect
Halo effect/horns effect - A positive/negative impression of a person in one area affects how we think of them in others - eg: attractive = nicer/successful/intellegent obese=lazy look healthy=think they are
Visceral bias - influence of negative or positive feeling towards a patient
biases to watch for in the dual process theory
type 1
Blind spot bias
Anchoring
Ascertainment
belief bias
Visceral bias
Diagnostic momentum
Halo/horns effect
Type 2:
Premature closure
Confirmation bias
internal vs external factors which influence clinical reasoning
Internal
Knowledge
Training
Confidence
Emotions
Fatigue
Stress
Illness
External
Workload
Interruptions
Patient factors
Team factors
Insufficient data
also may be influenced by the time of day
what is metacognition
Ability to pull back and think about the thinking underlying our clinical reasoning
Can use it to reduce the impact of biases
Not easy and needs multiple strategies and ongoing maintenance
Easier with outside input
Experts in clinical reasoning
Use heuristics frequently
Errors occur when heuristics dominate without analytical checking (deductive/rule-based reasoning)
So Good/Expert clinicians:
Use heuristics to generate hypotheses
then use deductive + rule-based reasoning to test and safeguard decisions.
Methods to counteract cognitive biases
learn cognitive biases to recognise and counteract them
Question question decision making process where biases may have influenced decisions
collaborate a diverse group of contributors from varying experitise areas may be able to spot areas overlooked - identify biases
remain blind to avoid being influenced by gender, race, or other easily stereotyped considerations
Use checklists, algorithms or other objective measures to focus on relevent factors and no overlook processes
GALS screen view purpose
designed fro the routine assessment of a patient
starts with 3 questions which should be included in routine systemic inquirey
identify common problems in the usculo skeletal system
identify significant abnormalities in the upper and lower limb function
3 starting gal question
do you have any pain or stiffness in your muscles, joints or back
can you dress yourself completely without any difficulty
can you walk up and down stairs without any difficulty
order of things assess in GALS
GAIT
smoothness symmetry and ability to turn quickly
“can you take a few steps for me please?”
EXAMINE MUSCLE BULK
shoulder muscle bulk + symetry
spinal alignment
gluteal muscle bulk
politeal swelling or abnormalities
hindfoot abnormality or swelling
EXAMINE SPINE
from side:
normal cervical lordosis
normal thoracic kyphosis
normal lumber lordosis
“can you bend forwards and try touch your toes and come back up”
as they rise your fingers on lower back should mover back together
indicates movement isn’t purely from the hips
EXAMINE ARMS
stand in anatomical position
shows normal elbow extension
ask for cervicle spine lateral flexion
ask to open jaw wide - move it side to side
assess for temporal mandibular joint pain
hands behind head
creates humeral movement allows for elbow flexion to be examined and assesses arm function
pronation and flex elbows so hands face down
assess composite range of movement of elbow range of rotaion and wrist movement
can inspect patient hand for any swelling or deformity in the fingers
look and palms of the hands
examine muscle bulk, look for tendon thickening or abnormality
make a fist
test function
touch fingers together
test function smoothness and concentration
grip strength test
gently squeezing across the metacarpal phalangeal joints
screens for inflammatory joint disease
EXAMINE LEGS
assess knee flexion
hip flexion
internal rotation of the hip
patella tap
checks for fluid or knee effusion
cross fluctuation or bulge test
check feet for callus formation on soles
squeeze gently across the metatarsal phalangeal joints while watching patients face for signs of discomfort
If no abnormalities are found this should be recorded as GALS NAD
WHEN is the History taken by the Physiotherapist?
Initial consultation
During treatments (reassessment with reference to the initial history).
Signs and symptoms can vary rapidly
Following each treatment
objective and subjective reassessment
Reassessment at the start of each subsequent session
things to remember as a physio when taking history/notes
Allocate enough time
Be attentive and a good listener
Be aware of your body language & tone of voice
Be prepared eg: How are you taking notes?
empathy
insight
active listening
understanding
Where do phyios take a history
inpatient
general ward
high dependency
icu
transitional care
rehab/outpatients
Structure of taking a history - 7 Categories, each relating to one part of the problem
Area and type of the symptoms (Body Chart)
Current history (CHx)
Past history (PHx)
Behaviour of symptoms (24/24 hrs, Aggs/eases)
Irritability of symptoms (how easily aggravated)
Contraindications and precautions (‘special questions’)
Social history (SHx) and Goals
what information to gather on current presentation of symptoms
Spatial distribution
Exact area (site of pathology?)
referral patterns (somatic/visceral)
# of areas, check unaffected areas (✓)
Type of symptoms
pain, paraesthesia, anaesthesia, stiffness, weakness
Quality
dull ache, burning, sharp, stabbing, maybe noises.
Intensity: (use scale /10)
Depth
Constant or intermittent
Establish relationship of symptoms
what to ask initially to a patient?
what brings you in today?
tell me where your experiencing pain or discomfort?
pain threshold?
constant or intimitent
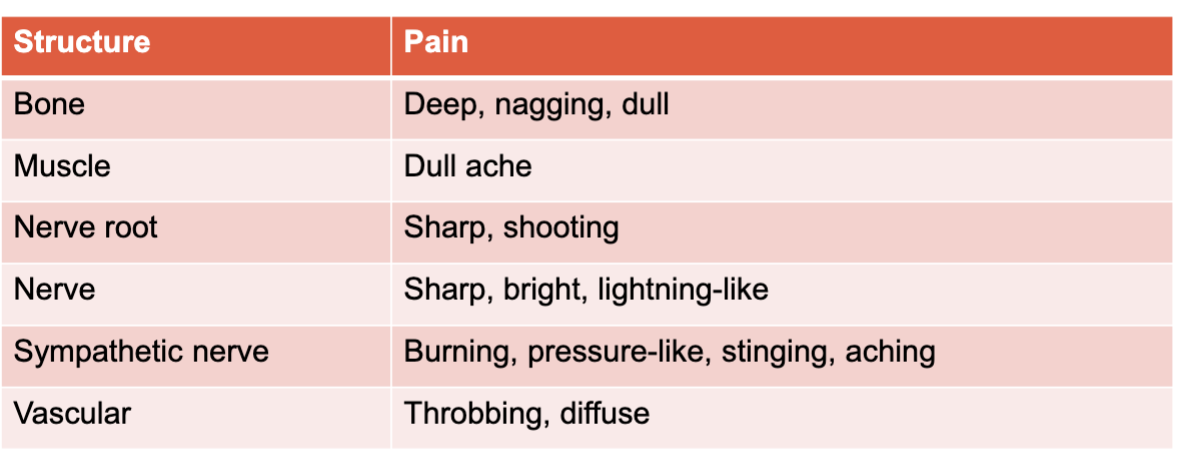
Suspected structure and pain quality
how to take a current history? and potential questions?
aka: History of Present Condition
Determine details of the incident/onset
potential qs:
when did symptoms begin
which symptoms - chronological onset
mechanism of injury - how did they start (trauma, gradual onset?) - (any lifestyle changes?)
progress of symptoms? worse/ better/ same since onset of episode?
treatment since this episode began? effect?
Past history potential questions
First episode?
when did it occur?
how did it occur?
previous treatment and effect?
Subsequent episodes?
are they changing in frequency, intensity and duration?
behaviour of symtoms can be used for?
used to?
hypothesise structure affected
Indicate functional impairment
Gain information re:
Severity
Irritability
Nature of condition
Examples of Aggravating factors
Aggravating factors
Knee - squat / stairs
Hip - squat
Ankle - stairs / tipee-toes
Foot – walking on uneven ground / barefoot
Shoulder - overhead/ HBB
Lx Sp - sitting/ standing
Tx Sp - deep inspiration/ cough
Cx Sp - sustained flexion
examples of easing factors
Positions
eg. avoid putting much weight through leg, sitting rather than standing, walking not running, changing how put a bra on)
Heat / cold / massage
Exercises
patient assessment and outcome measures
history
physical assessment
goals
plant treatment
what is a subjective assessment/history
In a subjective assessment/history, we are gathering data through patient interview to:
Generate diagnostic hypotheses
Plan the physical assessment including selecting specific tests and measures to identify and characterize signs, symptoms, and risk of movement dysfunctions
Determining irritability
what is an objective/ physical examination entail
Objective Assessment; an evaluation process to establish:
Individual's specific diagnosis
Individual's specific prognosis
Whether the potential or existing disorders can be managed within the scope of physiotherapy practice.
what does assessing goals entail?
Plan of care based on patients goals
Consider short term and long-term goals
SMART goals
Goal setting keeps the focus of rehabilitation patient-centred.
Goal setting helps health professionals plan their interventions for what is best or most meaningful for the patient.
What does establishing a treatment plan entail?
The treatment plan is based on:
Your subsequent judgments about diagnoses and prognoses and patient goals
Physiotherapists manage an individual by:
Making referrals
Providing interventions
Conducting re-assessments
Modifying interventions to achieve the individual's goals and outcomes
Determine a conclusion to the plan of care
the purpose and three aspects to determine in an irritability of symptoms assessment
Purpose:
Plan an appropriate amount of examination & treatment
Avoid making symptoms worse from too much examination or treatment
Three aspects:
Ease of onset
What activity (and/or how much) aggravates symptoms?
Intensity of symptoms
How severe are the symptoms?
Duration of symptoms
Continuation of symptoms after cessation of activity?
assessing symptoms behaviour across 24 hours?
night?
Symptoms prevents from getting to sleep?
Wakens?
Best / worst positions?
Morning?
pain
stiffness
when you first wake up in the morning what is the bodies position like?
During the day and at the end of day?
Purpose?
Determine whether symptoms are caused by a mechanical disorder or a specific disease process.
Systemic Inflammation
Mechanical
use as an indication of progress
how to distinguish between a mechanical or inflammatory problem?
A spectrum: not always this black and white
Mechanical:
Better in the morning
Worse at the end of day
Worse with activity
Obvious aggravating activity causes symptoms
Inflammatory?
Worse in the morning
Improvement with movement
Stiffness >30 minutes in the morning
Night pain
Better with activity
No obvious aggravating activity
what are Contraindications and precautions (‘red flags’)
Certain pathologies may contraindicate all or selected treatment strategies and
may require further medical investigation
Usually identified by asking “Special questions”
purpose:
To alert of possible serious pathology
To alert of possible precautions or contraindications to examination or
treatment
does my patient belong here?
Types of questions (A.K.A. “Special questions”) - which could reveal or answers that indicated red flags
General health
Recent unexplained weight loss
Presence or history of:
Inflammatory disorders
Cancer
Osteoporosis
X-rays and other investigations
Medications
Steroid use
All spinal conditions
Cord signs
Bilateral, non-dermatomal symptoms and ataxia
Lumbar spine disorders
Cauda equina
Disturbed bladder or bowel function, saddle anaesthesia
Cervical spine disorders
Dizziness
Vertebrobasilar insufficiency
what are some yellow flags?
psychosocial and other risk factors that are likely to delay recovery
include:
Unhelpful attitudes and beliefs about pain, resulting in fear/avoidance behaviour
Unhelpful behaviours. eg. use of extended rest and disproportionate downtime
Compensation issues (off work due to injury/pain > 12 weeks)
Inappropriate diagnosis and treatment
Catastrophising and fear (eg. of ending up in a wheelchair and never being able to walk again)
Unhelpful emotions eg. feeling under stress and unable to maintain sense of self control
Inappropriate family response. eg,. Overprotective or socially punitive responses from spouse
Work issues eg. belief that work is harmful or poor job satisfaction
purpose of assessing yellow flags
Decide if more detailed assessment required or if a referral is needed
Identify if more important factors should be addressed & intervened
AIM:
change management to prevent development of chronicity
Some questionnaires to identify unhelpful attitudes & beliefs:
Tampa scale for kinesiophobia
Fear-avoidance beliefs questionnaire (FABQ)
things to assess when observing social history?
age and gender
employments
status and type
domestic role
self care
dependants
leisure activities / plater profile (sports, level, comp, training, equipment, surfaces)
goals of treatment
what are outcome measures?
Outcome measures? - Tools used to evaluate the effectiveness and
impact of healthcare interventions, treatments, or services. - are important to provide credible and reliable
justification for treatment and measure how people look feel and function
The baseline function of a patient at the beginning of treatment
The changes over time
The progress and treatment efficacy, once treatment has commenced
what are outcome measures aiming to measure?
Patient (or self) reported measures (PROMS) - for outcome measures
a measurement based on a report that comes directly from an
individual regarding the status of a particular aspect of their
health.
examples
KOOS
Orebro Musculoskeletal Pain Questionnaire
Fear Avoidance Beliefs Questionnaire (FABQ)
Assessment of Quality of Life (AQoL)
Nordic Musculoskeletal Questionnaire
what are some performance related outcome measures
a measure based on an individual’s performance of a defined task that is quantified in a specified way and does not rely on judgement to determine the measure or score.
what are Clinician reported outcome measures
measure based on clinical judgement or interpretation of observations made by trained healthcare professionals
what re Observer-reported outcome measure
a measurement based on observations made by someone other than a healthcare professional such as a family member or carer, when the patient is unable to self-report.
are reported by a parent, caregiver, or someone who observes the patient in daily life e.g., decline in cognition
Does not include medical judgement or interpretation.
what are some examples of questions to ask before choosing an outcome measure
Is the Outcome Measure Reliable?
is the Outcome Measure Valid?
Is the Outcome Measure Responsive to Change?
Are there any financial considerations?
Are there any limitations in outcome measure implementation for the therapist?
Are there any limitations in outcome measure implementation for the client?
What are resource considerations?
some things in the physical assessment kit bag
observation
palpation
active movement
passive movements
passive accessory
muscle strength
muscle length
neurological
neurodynamic
endurance
functional
reliability vs validity in physio
reliability
When using an outcome measure, the results should be the same (or similar)
regardless of who administers the test or when it is administered
validity
Validity is defined as the degree to which an instrument measures what it
intends to measure. hat we need.
what is layman language
simple, easy-to-understand language that avoids technical jargon, specialized jargon, or complex terminology
Explain kinematics in physio
Motion:
Translation (linear), eg knee movement forward
Rotation (angular), eg ankle dorsiflexion
explain torque in movement
force (ma) x distance from axis of rotation
causes a rotaion
action on joints in the body
to reduce torque
reduce moment arm (distance from axis of rotation)
or reduce mass of load
internal vs external forces on the body?
External forces:
Ground reaction force: reactive force from ground or object against body
external loads
active bodies
passive resistance (wind)
Internal Forces:
Muscle Activity
ligaments
friction in muscles/joints
examples of points of observation of normal movements? (4)
bed mobility
sit to stand
standing
walking
Different ways of Bed mobility?
Supine to sitting up over the side of bed
flexion and rotation of trunk and head
Flexion of hips and knees to swing legs and clear bed
Push up with hand closest to the side of the bed you are movingtowards
Moving across the bed (bridging)
Flexion of hip and knee
Push through feet to lift hip from the bed
Move hips to the side
Move feet and head to straighten body alignment
Supine to side lying (rolling)
Rotation and flexion of the neck
Flexion and protraction of shoulder
Rotation within the trunk
Hip and knee flexion
Side lying to sitting over the edge of bed
Lateral flexion of neck
Lateral flexion of trunk and abduction of lower arm
Legs lifted and lowered over side of bed
important components of sitting up from a chair
Initial alignment (reduce thigh support)
Feet placement (feet apart & pointing forward, knees directly
over feet, ankles dorsiflexion (~75%))
Pre-extension phase:
feet placed back so that ankles behind knees
inclination of trunk forward by flexion at the hips with an
extended trunk
Transition between 2 phases = “thighs off” (occurs at 30% of movement duration - 150% of body weight on occurs during this time)
Extension Phase:
dorsiflexion of ankle to bring the knees forward
sequence of lower limb extensions at knees, hips and ankles
what are the important components of standing posture (4)
Alignment of body segments
Head balanced on level shoulders
Hips in front of ankles
Feet approx. hip width apart
Weight evenly distributed
Posture and movement are interrelated
Normal stance posture is somewhat variable among individuals
influenced by size, age, sex and body type - though share some characteristics - guidlines in performing an individual postural assessment
Antigravity Muscles that maintain upward posture
neck and trunk extensors
neck extensors
trunk extensors
hip extensors
knee extensors
Forces required to maintain Upright Stance
Line of gravity passes either anterior or posterior to the joint axis and as a result gravity creates a moment arm that applies a rotational force to the joint
what does centre of mass COM mean?
a point that corresponds to the centre of the total body mass. The point at which the body is in perfect equilibrium
what does centre of gravity COG mean?
the vertical projection of the COM to the ground.
what does centre of pressure COP mean?
the point on the ground that represents the average position of the forces that a person exerts on the ground
what does base of support mean BOS?
defined as the perimeter of the
contact area between the body and it’s support
surface.
what do limits of stability LOS to mean?
refers to the
sway boundaries in which an
individual can maintain
equilibrium without changing
his/her BOS
what are stability considerations?
Base of support
stability increases as area of BOS increases
Height of centre of mass
Lower centre of mass = COM more stable
Motion of projection of CoM with respect to BoS
stability increases as projection of COM moves closer to perimeter of base of support.
as COM closer towards limits of stability less stable
what is balance? - definition
Defined as the ability to control the body mass relative to the base of support
Static:
COM is maintained within the BOS
Dynamic:
COM is maintained while in motion or switching between positions
explain balance as a complex motor control task
Involves the detection and integration of sensory information to assess the position and motion of the body in space.
Involves the execution of appropriate musculoskeletal responses to control body position within the context of the environment and task.
Involves:
musculoskeletal system
nervous system
contextual effects
Explain the role of the sensory system in balance control
Visual:
information on position which allows for appropriate postural adjustments
most important in a static environment
can be easily altered or eliminated in a clinical setting
Vestibular (labyrinth):
information regarding the position of head
detect positional changes of head
allows for postural correction
Proprioceptive (muscle/joint/skin):
information on bodies position relative to other body parts
enables one to make postural adaptions eg: change base of support or surface stability
postural adjustments?
postural adjustments:
are the muscle activity and segmental movements concerned with the preservation of balance
are:
anticipatory
ongoing
specific
movements not just muscle activity
postural sway:
horizontal movement of the COG
ankle strategy to maintain balance
Shifts CoG by maintaining placement of the feet by rotating body as a rigid mass about the ankle joints
Muscles are activated on the side contralateral to direction that COG is shifted or perturbed
when effective:
Slow CoG movements when BOS is firm and CoG is well
within LOS perimeter
When maintaining a static posture with the COG offset
from the center.
Appears only if somatosensory reception intact
how does the hip strategy maintain balance
Helps control motion of the CoG through initiation of large and rapid motions at the hip with anti-phase rotation of ankles
Muscles are activated on the side toward which COG is shifted or perturbed
Effective when:
COG is near LOS perimeter
LOS boundaries are contracted by narrower base of
support
explain stepping strategy
Utilised when COG is displaced beyond LOS
Step or stumble is the only strategy to prevent a fall