OB EXAM 3
1/235
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
236 Terms
high risk pregnancy
a condition that threatens the health of the mother, fetus, or pregnncy
trimester zero
a social media trend where pregnancy will only occur and be healthy if the woman performs bizarre trends like no nail polish
increases maternal guilt and shame if pregnancy ends up being unhealthy and they didn't perform all requirements
components of prenatal/conception care
decrease teratogen exposure/risk factors like smoking
education
genetic testing
prenatal vitamins
how to deal with modifiable risk factors?
education/interventions
follow up
close monitoring
how to deal with non-modifiable risk factors
determine the need for additional testing
consider referral to specialty medicine (maternal fetal medicine)
causes of early pregnancy bleeding
miscarriage or abortion
ectopic pregnancy
cervical insufficiency
molar preg
most common complication of early pregnancy
abortions/miscarriages
most abortions/miscarriages occur in
the 1st trimester
causes of abortions/miscarriages in the 1st trimester
genetic abnormalities, not necessarily a syndrome
ex: zygote replication is abnormal
causes of abortions/miscarriages in the 2nd trimester
cervical insufficiency
maternal diseases
acquired infections (viruses from working with children)
abortion/miscarriage assessment findings/manifestations
risk factors
bleeding in the 1st/2nd trimester
pad count, quality (clots), cramping with bleeding
increased HR and decrease BP d/t pain, stress, and blood loss
decreased hcG and H+H
Rh/blood type
abortion/miscarriage management
pain relief
prep for D&C if indicated
expectant meds (help aid with miscarriage)
emotional support
D&C
dilation and curettage, which is a surgery to remove contents of conception
threatened miscarriage
vaginal bleeding with a closed cervical os
FHR remains with a transvag US
can't do anything but wait.... may continue to a healthy baby or evacuate eventually
inevitable miscarriage
vaginal bleeding with a dilated cervical os
products of conception may be seen or felt at or above cervical os
despite possibly having FHR, but since os is open, the miscarriage is inevitable
incomplete miscarriage
vaginal bleeding with a dilate os
some products of conception expelled and some remain
need meds and dc to help remove products
dangers of remaining products of conception
sepsis and infection
Complete miscarriage
vaginal bleeding with a closed cervical os
products of conception completely expelled
Misprostol (Cytotec)
stimulates uterine contractions to terminate a preg and evacuate the uterus AFTER abortion
ensures the passage of ALL products
taken 24-48 hrs after mifepristone
Mifepristone (Korlym)
Acts as progesterone antagonist, allowing prostaglandins to stimulate uterine contractions
causes the endometrium to slough;
may be followed by administration of misoprostol within 48 hours
rhoGAm
given to rh- mothers after abortion, miscarriage, or pregnancy
ectopic pregnancy
ovum implants outside the uterus, typically in the fallopian tube
causes of ectopic pregnancies
conditions that slow down the ovums passage to the uterus:
-fibroids
-endometriosis
-infections like STI and pelvic inflammatory disease d/t scarring of fallopian tubes
ectopic pregnancy s/s
early bleeding (6-8wks)
abdominal pain (ALL OVER)-> then localizes to the location of the preg
shoulder pain (referred)
results of a ruptured ectopic pregnancy
septic shock (decreased BP, increased HR, decreased O2, trouble breathing)
nursing management for ectopic pregnancy
catch before rupture (bc after they lose the fallopian tubes)
determine s/s and Rh status
education ab medications
prepare/educate for surgery
diagnosis of ectopic pregnancy
hCG levels and transvaginal ultrasound
if the ectopic pregnancy is early and unruptured, what is the treatment?
give methotrexate and follow with a transvag US to see if successful
if the ectopic preg is late and ruptured, what is the treatment?
surgery to remove the fallopian tube (salpingectomy)
Gestational Trophoblastic Disease
an abnormal proliferation of cells during pregnancy;
may also be referred to as molar pregnancy
Types of gestational trophoblastic disease
Hydatidiform mole
Choriocarcinoma
molar pregnancy manifestations
elevated hCG levels
vaginal bleeding
pelvic pressure or pain
enlarged uterus
hyperemesis gravidarum
molar pregnancy nursing managment
prepare for d/c
education (avoid preg for a year)
emotional support
strict adherence to follow up (serial hCG measurements to check for recurrence)
gestational trophoblastic disease can occur with
a fetus, but not often viable
can attempt to carry out if fetal activity is found.
gestational trophoblastic disease treatment
obtain hCG levels
transvag US
surgery to evacuate tissue
Fetal viability is defined as how many weeks of gestation?
23 wks (maybe...22)
cervical insufficiency
premature dilation of the cervix
cervical insufficiency is commonly a cause of
late miscarriage (after 12wks/2nd trimester)
pregnancy loss
preterm labor
cervical insufficiency risk factors
pre-existing collagen disorders
previous cervical trauma leads to scarring (cervical cancer/surgery)
uterine anomalies
cervical insufficiency s/s
painless dilation
pink spotting
pelvic pressure/fullness
cervical insufficiency nursing management
assess FHR/activity
education on sx of preterm labor
prepare for cervical exam and cerclage
cerclage
suturing of the cervix to prevent it from dilating prematurely or further during pregnancy
can lead to a healthy term pregnancy, but HEAVY follow ups
once ready to deliver, the stitch is removed.
for the next pregnancy, a cerclage is usually planned.
causes of bleeding late in pregnancy
placenta previa and placental abruption
placenta previa
placenta implants in the lower part of the uterus (near or over the cervical os)
placenta previa risk factors
scarring in the uterus (placenta lowers to find healthier tissue)
advanced maternal age
multiparity
smoking and substance abus
IVF and reproductive tech
placenta previa s/s
Painless bright red bleeding
may be intermittent
FHR usually normal
placenta previa management depends on
depends on gest and sx severity
placenta previa management
identified at the 20wk US
modify activity and pelvic rest
NOTHING IN THE VAGINA so no sex, no cervical or vag exams
ALWAYS C-section (scheduled prior to labor time)
placental abruption
Placenta detaches from uterine wall before delivery, leading to maternal blood loss and decreased BF to the baby
detachment can be partial or complete
placental abruption risk factors
substance abuse
previous abruption
MVA or trauma like a severe fall, IPV, kicked in the stomach
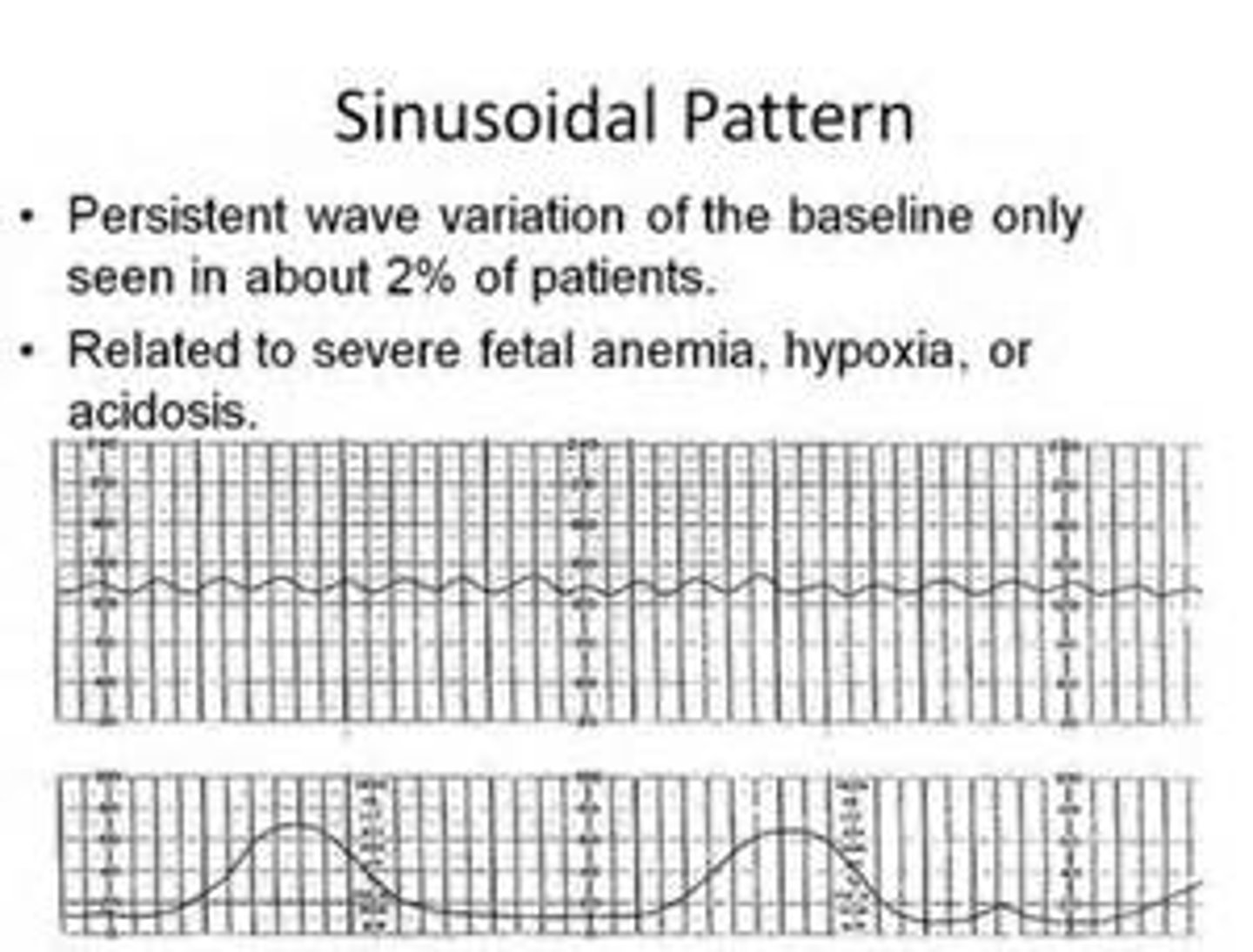
placental abruption s/s
dark red or port-wine bleeding
KNIFE-like pain
board like or rigid abdomen
fetal distress or absent FHT (SINUSOIDAL rhythm)
placenta abruption management
MEDICAL EMERGENCY
intrauterine resuscitation to increase perfusion
monitor fetus and mom with abruption labs (H+H, clotting factors like PT, INR)
watch for DIC and shock
prep for C-section
#1 priority with known or suspected placental abruption
FHR!!
hyperemesis gravidarum occurs usually in the
1st and 2nd trimester
when does hyperemesis gravidarum peak and resolve?
8-12 wks of preg and resolves by 20th week
hyperemesis gravidarum can result in
need for hospitalization
anxiety and depression
work performance impairment
consideration of termination of preg d/t poor health
hyperemesis gravidarum s/s
persistent and uncontrolled n/v
weight loss
ketosis
e- imbalances
nutritional deficiencies
HG management (if hospitalized)
assess VS
monitor labs (urinalysis, e-)
IVF
antiemetics (diclegis, phenergan, zofran)
NPO!! if really severe, parenteral nutrition
best way to assess hydration status is?
urine output
chronic HTN
HTN prior to pregnancy
>140/90
dont necessarily have preeclampsia always
gestational HTN
onset of HTN after 20 weeks
>140/90 but NO proteinuria or organ involvement
after 12wks PP, goes back to normal
preeclampsia
new onset HTN with signs of organ involvement and/or proteinuria
therapeutic management depends on the severity
preeclampsia patho
vasospasm happens thoughout the body in response to hypoperfusion, which increases BP
this leads to leaky capillaries d/t endothelial cell dysfunction
abnormal arteries develop (spiral arteries) leading to hypoperfusion, whcih affects the kidneys, livers, and CNS.
leaky capillaries leads to
severe leg, facial, and periorbital edema
presentations of kidney injury d/t preeclampsia
proteinuria
abnormal kidney labs
presentations of liver injury d/t preeclampsia
RUQ pain and abnormal LFTs
presentations of neuro injury d/t preeclampsia
HA
blurred vision
decreased LOC (if severe)
preeclampsia without severe features
140/90 or higher after 20 wks gestation
no seizures, coma, hyperreflexia, or other s/s
home treatment for preeclampsia without severe features
no renal or liver impairment or coagulopathies
bedrest, kick counts, BP monitoring, limit Na+ in diet
more frequent visits
hospitalization for preeclampsia without severe features
keep pregnant as long as possible for fetus
monitoring for hyperreflexia, HA, BP, and labs
preeclampsia with severe features
160/100 or higher on two occasions at least 6 hours apart while on bed rest
no seizures or coma
presence of hyperreflexia
s/s of organ involvement like pulmonary edema, HELLP, RUQ pain, etc.
hospital management for preeclampsia with severe features
may develop quickly
treated aggressively to stabilize for birth
may deliver if preterm even
goal is to control HTN, prevent seizures, and prevent morbidity/mortality
Antihypertensive Medications for preeclampsia
hydralazine, nifedipine, labetalol
magnesium sulfate
CNS depressant administered as an IV piggyback to prevent and treat seizure activity
magnesium sulfate side effects
vasodilation leads to warmth, flushing, and diaphoresis
makes pt feel TERRIBLE, so OOB x 1
magnesium sulfate toxicity management
VS
SERUM LEVELS
strict I+Os to monitor for fluid overload/pulmonary congestion
lung assessments (resp depression, pulm congestion)
CNS assessments (hyporeflexia)
decreased urine output (<30ml/hr) is a red flag for decreased kidney function
Magnesium sulfate antidote
calcium gluconate
eclampsia
>160/110 with seizures, coma, hyperreflexia, and organ involvement
premonitory signs of eclampsia
HA
blurred vision, floaters, trouble w eye tracking
altered MS
abdominal pain
eclampsia features
tonic contractions
respirations stop
hypotension
vomiting or incontinence
immediate care for eclampsia
-ABCs, suction, O2
-side rails up, dim the lights, decrease visitation and noise
-mag sulfate, IVF
-prepare for delivery of baby
assessments that measures seizure risk the best?
REFLEXES!!
clonus, hypo/hyperreflexia
HELLP syndrome
occurs in up to 20% of people with severe features of preeclampsia
characterized by abnormal vascular tone, vasospasm, and coagulation defects
HELLP syndrome s/s
hemolysis, elevated liver enzymes, low platelets
n/v, RUQ pain, HTN, proteinuria
*do NOT always have HTN!!
individuals with HELLP syndrome are at an increased risk for
cerebral hemorrhage
retinal detachment
hematoma/liver rupture
DIC
placental abruption
death
multifetal pregnancies can lead to....
preterm labor
polyhydraminos
hyperemesis grav
congenital abnormalities
twin to twin tranfusion syndrome
intrauterine growth restriction
conjoined twins
prenatal care for multifetal pregnancies
serial US
BBP and NST
multifetal pregnancies will most likely require...
a c-section
multifetal pregnancy nursing assessments
fetal movement
fundal height measurements
nausea
fatigue
weight gain
there is a higher risk for twin to twin transfusion with...
a shared amniotic sac or placenta.
PROM vs PPROM
PROM: 37 wks gestation
PPROM: <37 wks gestation
PROM therapeutic management
dep on gest age
NOTHING in vagina
expectant management if fetal lungs are immature (corticosteroids)
corticosteroids
betamethasone helps speed up fetal lung maturity by increasing surfactant production
#1 concern with PROM
cord compression (monitor FHR!!)
PROM nursing assessment
Risk factors, s/s of labor, FHR monitoring, amniotic fluid characteristics and POC testing
PROM nursing management
Infection prevention
Identification of uterine contractions
NST and frequent monitoring!!
Discharge home (PPROM) if not labor within 48 hrs. with STRICT instructions
72-84 hrs max, then induce labor
an increased use of glucose in the 1st trimester leads to
increased insulin resistance and a compensatory increase of insulin secretion in the 2nd trimester
pre-gestational diabetes
having diabetes type 1 (autoimmune) or 2 (loss of insulin secretion) before pregnancy
risks/complications unique to pre-gestational diabetes
perinatal mortality
congenital malformations
A1C levels are...
teratogenic to babies, leading to congenital malformations and perinatal mortality