Equine GI case studies
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
20 Terms
A 12yo WB gelding is QAR and not interested in food. He looks like he’s rolled and has been pawing the ground.
T: 102.1 F
P: 80 bpm
R: 32 bpm
MM are congested w/ a CRT of 3 seconds
Jugular refill time + skin pinch > 2 seconds
All 4 legs feel colder on palpation
No increased digital pulse
Abdominal auscultation= decreased gut sounds in all 4 quadrants
NG tube: abundant reflux ~ 8L of brown reflux
Rectal exam: distended SI
Abd U/S: Distended SI
Abdominocentesis: yellow turbid, TP 2.8, WBC < 5000
PCV, 45%, TP 7.3
Give estimated dehydration % and why
8%; HR > 60 bpm, CRT 3
A 12yo WB gelding is QAR and not interested in food. He looks like he’s rolled and has been pawing the ground.
T: 102.1 F
P: 80 bpm
R: 32 bpm
MM are congested w/ a CRT of 3 seconds
Jugular refill time + skin pinch > 2 seconds
All 4 legs feel colder on palpation
No increased digital pulse
Abdominal auscultation= decreased gut sounds in all 4 quadrants
NG tube: abundant reflux ~ 8L of brown reflux
Rectal exam: distended SI
Abd U/S: Distended SI
Abdominocentesis: yellow turbid, TP 2.8, WBC < 5000
PCV, 45%, TP 7.3
What is your top differential and why?
Duodenal proximal jejunitis; brown reflux and large amount, yellow turbid abd fluid, tachycardia tachypnea, fever, distended SI
A 12yo WB gelding is QAR and not interested in food. He looks like he’s rolled and has been pawing the ground.
T: 102.1 F
P: 80 bpm
R: 32 bpm
MM are congested w/ a CRT of 3 seconds
Jugular refill time + skin pinch > 2 seconds
All 4 legs feel colder on palpation
No increased digital pulse
Abdominal auscultation= decreased gut sounds in all 4 quadrants
NG tube: abundant reflux ~ 8L of brown reflux
Rectal exam: distended SI
Abd U/S: Distended SI
Abdominocentesis: yellow turbid, TP 2.8, WBC < 5000
PCV, 45%, TP 7.3
What is a sequelae of concern? Reasons and treatment against it
Endotoxemia— congested mm; flunixin meglumine + BS abx (gm-)
A 12yo WB gelding is QAR and not interested in food. He looks like he’s rolled and has been pawing the ground.
T: 102.1 F
P: 80 bpm
R: 32 bpm
MM are congested w/ a CRT of 3 seconds
Jugular refill time + skin pinch > 2 seconds
All 4 legs feel colder on palpation
No increased digital pulse
Abdominal auscultation= decreased gut sounds in all 4 quadrants
NG tube: abundant reflux ~ 8L of brown reflux
Rectal exam: distended SI
Abd U/S: Distended SI
Abdominocentesis: yellow turbid, TP 2.8, WBC < 5000
PCV, 45%, TP 7.3
Would you treat this horse in medically or surgically? Would you be able to treat in the field or refer to a hospital?
Medically— refer to hospital bc aggressive fluid therapy needed + medical management + reflux management
What PE parameters would differentiate SI vs LI colic in a horse?
SI: reflux, melena
LI: bloat, hematochezia, small frequent diarrhea
Equine glandular gastric ulcer syndrome vs equine squamous gastric ulcer syndrome treatment and why
EGGUS: Omeprazole + mucosal protectants + prokinetic
EGSUS: Omeprazole + H2 blocker + mucosal protectants+ prokinetic
EGSUS not usually acidic→ needs less acidic environment
Horse presented for colic and painful. Horse got into grain feed 2 days ago.
Tachycardia + tachypnea
Red-purple mucus membranes
Severe lameness and no gut sounds
Tight bands on rectal
Polycythemia + neutropenia w/ L shift and toxic changes
Diagnosis?
Acute grain overload
Horse presented for colic and painful. Horse got into grain feed 2 days ago.
Tachycardia + tachypnea
Red-purple mucus membranes
Severe lameness and no gut sounds
Tight bands on rectal
Polycythemia + neutropenia w/ L shift and toxic changes
Treatment plan for this symptomatic case
IV fluid therapy w/ hypertonic fluids ± plasma
NG tube to relieve gas
If renal function ok→ give polymyxin to bind endotoxins
Tx for endotoxemia: flunixin + BS abx
Horse presented with acute colic and reflux. BW shows hypokalemia, hypochloremia and hemoconcentration
Suddenly horse is no longer painful but is sweating and having muscle fasciculations.
What is your top ddx?
Equine GDV
Horse presented with acute colic and reflux. BW shows hypokalemia, hypochloremia and hemoconcentration
Suddenly horse is no longer painful but is sweating and having muscle fasciculations.
What is the most likely course of treatment?
Euthanasia— poor prognosis
400 kg Foal presented for weight loss and lethargy in September
PE reveals peripheral edema and diarrhea
BW: Hypoproteinemia
U/S: thickened SI walls and excessive abd fluid
What is your etiologic diagnosis?
Lawsonia intracellularis - equine proliferative enteropathy
400 kg Foal presented for weight loss and lethargy in September
PE reveals peripheral edema and diarrhea
BW: Hypoproteinemia
U/S: thickened SI walls and excessive abd fluid
What is the recommended treatment plan?
Macrolides + colloids+ parenteral nutrition + anti-ulcer: H2 blocker, omeprazole
500 kg Foal presented for weight loss and lethargy in September
PE reveals peripheral edema and diarrhea
BW: Hypoproteinemia
U/S: thickened SI walls and excessive abd fluid
What is the recommended treatment plan?
Tetracycline, chloramphenicol
Which colic diseases always need surgery?
Strangulating lipoma
Small intestinal volvulus
Epiploic foramen entrapment
Gastrosplenic ligament entrapment
Diaphragmatic hernia entrapment
Intussusception
Mesenteric rents
Adult inguinal/ scrotal herniation
What equine Gi diseases do you consider medical vs surgical management?
Ascarid obstruction
Ileal impaction
Duodenitis proximal jejunitis
Foal inguinal herniation
Intestinal hypertrophy
A 5-month-old male Quarter horse kept on pasture is brought to the clinic due to an acute colic episode. The colt had been noticed straining to defecate with increased frequency over the past 6 weeks. As recommended, the owner had been soaking the colt's hay after a veterinarian administered mineral oil by nasogastric tube 1 week prior. The owner had also administered commercial enemas per rectum that had not been recommended by the veterinarian.
General: Quiet, lying down
Pulmonary: Increased respiratory rate
Gastrointestinal: Straining to defecate dry, disc-shaped fecal balls
Neurologic: Quiet and responsive
Medical history: Healthy until recent tenesmus and colicSurgical history: None
Medications: Recent mineral oil via nasogastric tube and enemas. Dewormed twice, 60 days apart, with an oral ivermectin product. Vaccinated 1 month ago for influenza, EHV-1, EHV-4, tetanus, rabies, and strangles (intranasal).
Allergies: No known allergies
Social history: Lives on pasture with several other horses
General appearance: Quiet and alertVital signs:
Temperature: 38.8°C (101.8°F)
Pulse: 48 beats/min
Respirations: 54/minute
Weight: 242 kg (535 lb)
Skin: Long, dull haircoat
HEENT: Mucous membranes tacky
Pulmonary: No abnormalities
Cardiovascular: Capillary refill time >2 s; no arrhythmias or pulse deficits
Gastrointestinal: Decreased borborygmi on left, normal on right with gas sounds. A dorsal perirectal mass is noted on digital palpation. Fecal balls are disc-shaped.
Genitourinary: Urination not observed
What tests do you need to establish a diagnosis?
Rectal exam, NG tube, abdominocentesis
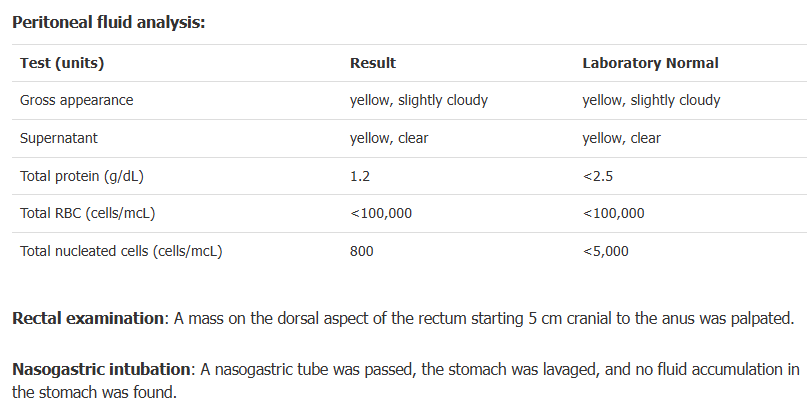
Based on the lab findings and the PE of this colt, name 2 differentials
Perirectal abscessation
Primary anorectal lymphadenopathy
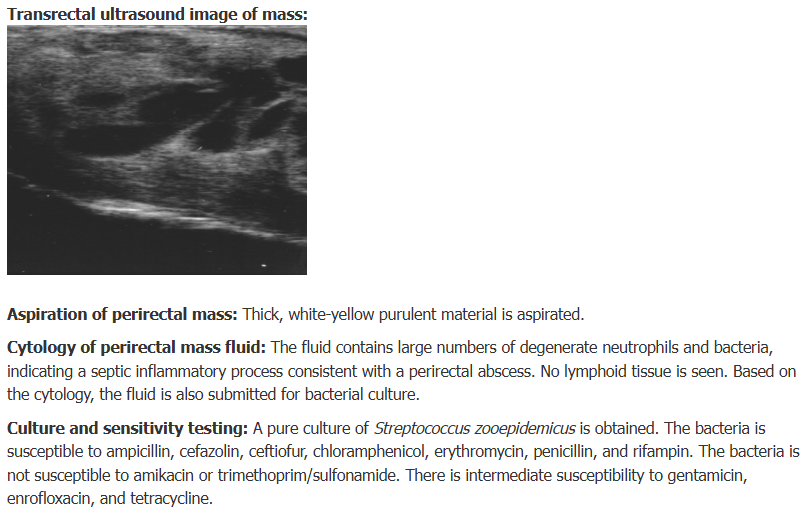
What would be your next steps on this colt?
Perform transrectal U/S of mass
Aspirate perirectal mass for cytologic evaluation
Administer miner oil via NG tube for dry misshapen stool
Here are the additional test results for the colt. Based on your diagnosis, what is your treatment plan?
Hospitalize for parenteral abx + abscess monitoring
- IV fluid therapy not needed bc colt not dehydrated and drinking
Provide stool-softening diet
- NG tube mineral oil
- Multiple small bran meals + warm water
- Fresh grass for grazing
- Soak dry hay in water for small meals
Tx w/ NSAIDs for inflammation + abscess
Tx with anti-ulcer meds: omeprazole, H2 blockers