SG Quiz 3 FUNDS
1/82
Earn XP
Description and Tags
Janice Mark Spring 2026
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
83 Terms
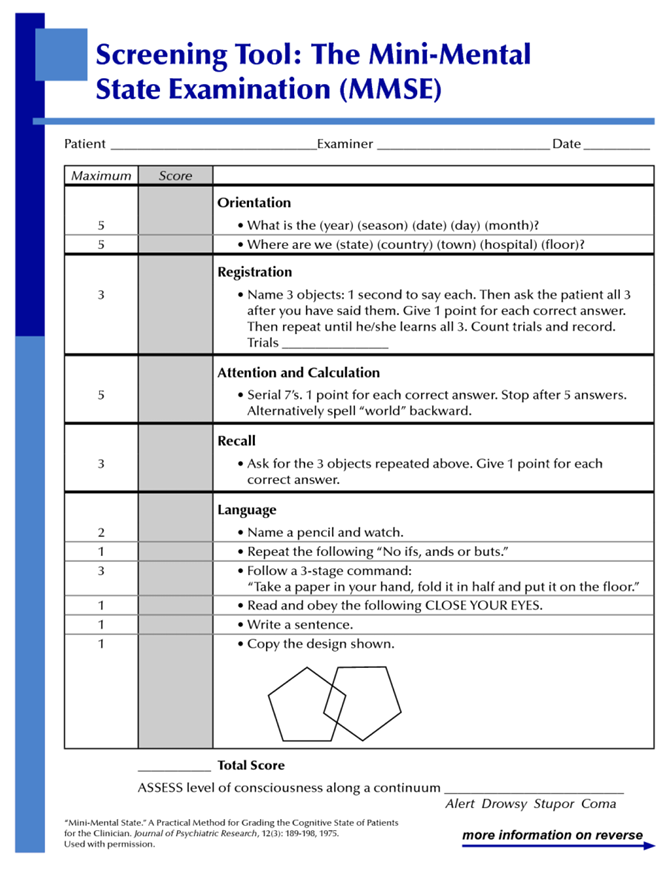
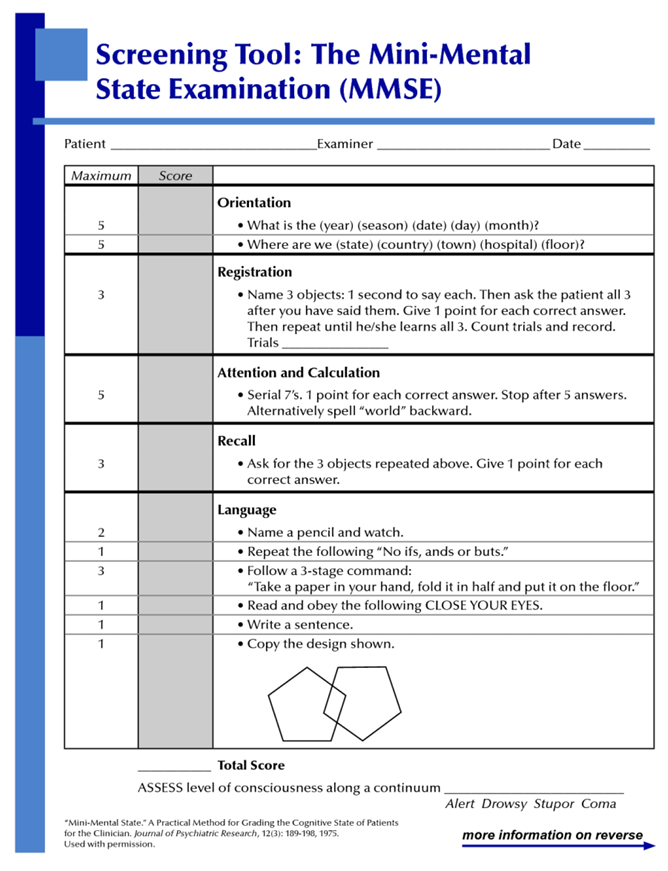
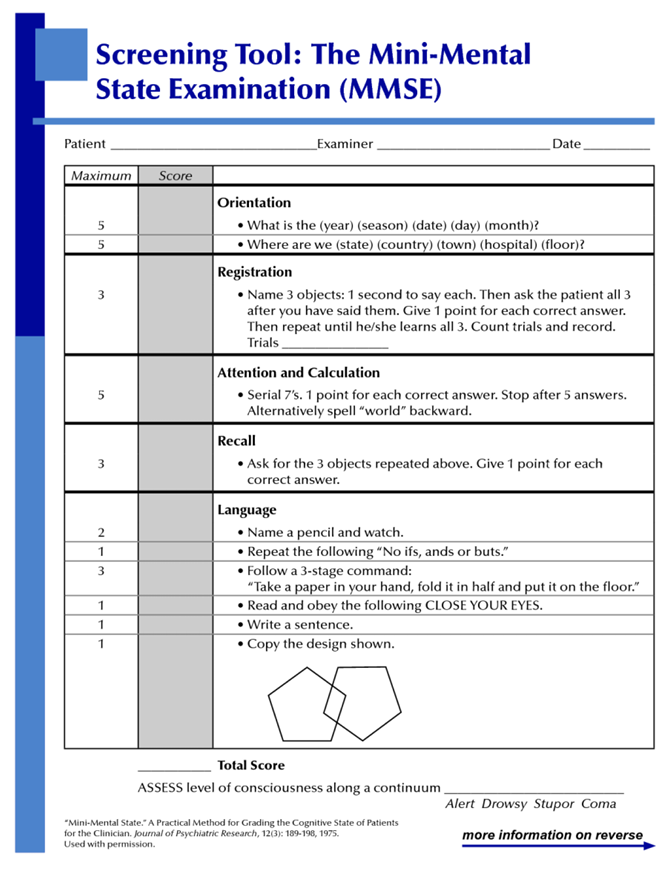
What are the key elements of cognition and how would you assess each one? Give an example. (multiple flashcards)
Orientation: Awareness of person, place, time, and situation
Registration: Ability to repeat named prompts
Attention & Calculation: Ability to remember objects named earlier
Recall: Ability to remember objects named earlier
Language: Ability to follow series of spoken or written instructions
What are the key elements of cognition and how would you assess each one? (ORIENTATION) Give an example. (multiple flashcards)
Orientation Assessment
Person: Please tell me your name?
Place: Please tell me where are you?
Time: What day is it today? What’s the date today
Purpose: Can you tell me why you are here?
Documentation:
▪ If patient oriented to person, time, place, situation→ “Oriented x 4”
▪ If patient not fully oriented → “Oriented x ____” ▪ More accurate -→ “oriented to _______ and ______ only”
What are the key elements of cognition and how would you assess each one? (REGISTRATION) Give an example. (multiple flashcards)
Registration: Ability to repeat named prompts
EX MMSE Question:
“I’m going to say 3 words and try to remember them. Ball, Cat, Boat. Can you repeat them back to me?”
Give 1 point for each correct answer, repeat until he/she learns all 3. Count and record number of trials it takes to learn all 3.
“Ball, Cat, Boat” (1 trial)
“Okay try to keep those in mind we’re going to come back to them.”
What are the key elements of cognition and how would you assess each one? (ATTENTION & CALCULATION) Give an example. (multiple flashcards)
Attention & Calculation: Ability to remember objects named earlier
EX MMSE Question:
Serial 7’s. 1 point for each correct answer. Stop after 5 answers.
Alternatively spell “world” backwards
“How is your math normally?” “Good” “Okay we’re going to do serial 7’s so start counting off from 100 in 7s backwards start when you’re ready.”
“93, 86, 79, 72, 65..” “Okay that’s good thank you”
What are the key elements of cognition and how would you assess each one? (RECALL) Give an example. (multiple flashcards)
Recall: Ability to remember objects named earlier
“I asked you to remember 3 words a moment ago, what were they?”
Ask for the 3 objects repeated from Registration. Give 1 point for each correct answer
“Cat, Basketball, and I don’t know the last one”
“That’s fine thank you (1/3 points)”
What are the key elements of cognition and how would you assess each one? (LANGUAGE) Give an example. (multiple flashcards)
Language: Ability to follow series of spoken or written instructions
Language
Name a pencil and watch.
Repeat the following "No ifs, ands or buts."
Follow a 3-stage command:
"Take a paper in your hand, fold it in half and put it on the floor."
Read and obey the following CLOSE YOUR EYES.
Write a sentence.
Copy the design shown.
What is consciousness and how do you differentiate each level (LOC)?
Being aware of one’s own existence, feelings, thoughts and of the environment
What is consciousness and how do you differentiate each level (LOC)?
Alert, Lethargic, Obtunded, Stupor, Coma
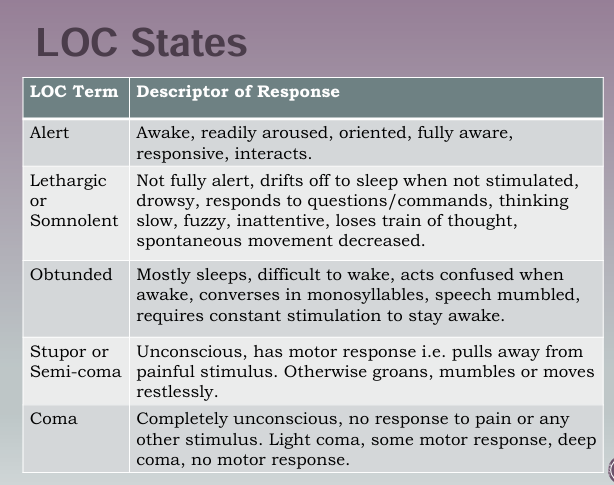
What is consciousness and how do you differentiate each level (LOC)? (ALERT)
Awake and oriented
Patient open eyes at your approach or spontaneously
Oriented to person, place, time, and situation
Can follow verbal commands appropriately
What is consciousness and how do you differentiate each level (LOC)? (LETHARGIC)
Not fully awake and oriented
Not fully alert throughout interaction
Drowsy, responds to questions slow, inattentive, loses train of thought
Drift to sleep when not stimulated. MORE than just sleepy
What is consciousness and how do you differentiate each level (LOC)? (OBTUNDED)
Mostly sleeps and difficult to wake
Responds to light shaking but slow to respond and may confused
Falls asleep multiple times throughout interaction
Speech mumbled, converses in monosyllables, acts confused when awake
What is consciousness and how do you differentiate each level (LOC)? (STUPOR)
Unconscious
Vigorous stimulus or pain for a response
Pain stimulation to wake up (trap pinch, sternum pressure, supraorbital pressure)
Has motor response
Pulls away from painful stimulation, groans mumbles, or moves restlessly
What is consciousness and how do you differentiate each level (LOC)? (COMA)
Unresponsive, completely unconscious
No response to pain or any stimulus
Light coma: Some motor response
Deep Coma: No motor response
Is there a particular order to arousing a patient?
Call name in normal tone
Call name in loud voice
Light touch on arm w/ loud voice
Vigorous shoulder shake w/ loud voice
Apply pain
(trap pinch, sternum pressure, supraorbital pressure, nail bed pressure)
Define Orientation
Ability to comprehend and adjust to person, place, time and situation
How would you assess for orientation?
Ask questions about person, place, time, and situation
Person: Please tell me your name?
Place: Please tell me where are you?
Time: What day is it today? What’s the date today
Purpose: Can you tell me why you are here?
Documentation:
▪ If patient oriented to person, time, place, situation→ “Oriented x 4”
▪ If patient not fully oriented → “Oriented x ____” ▪ More accurate -→ “oriented to _______ and ______ only”
What are the common tests used to assess cognition? What are the normal responses and scores? When would you use each one?
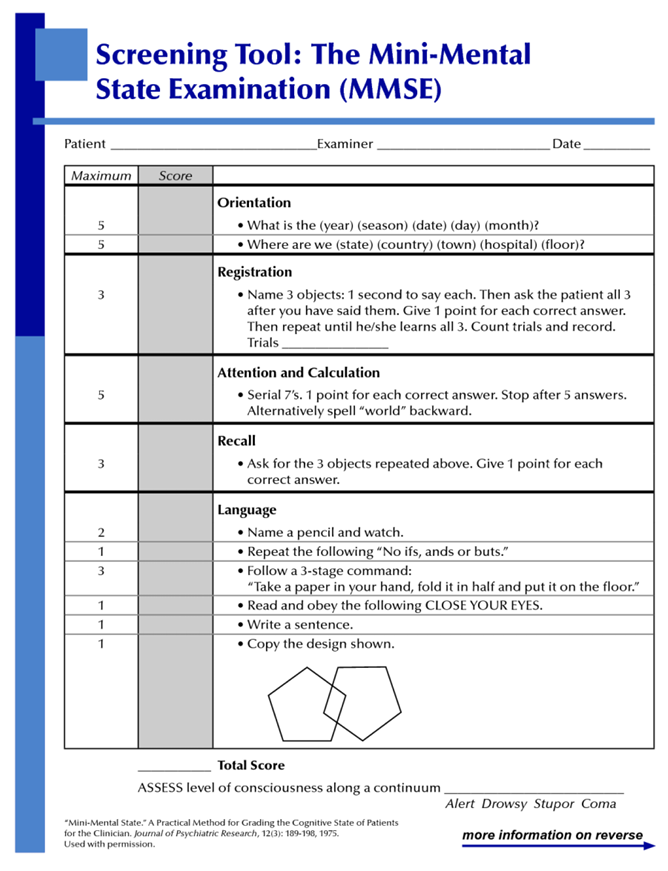
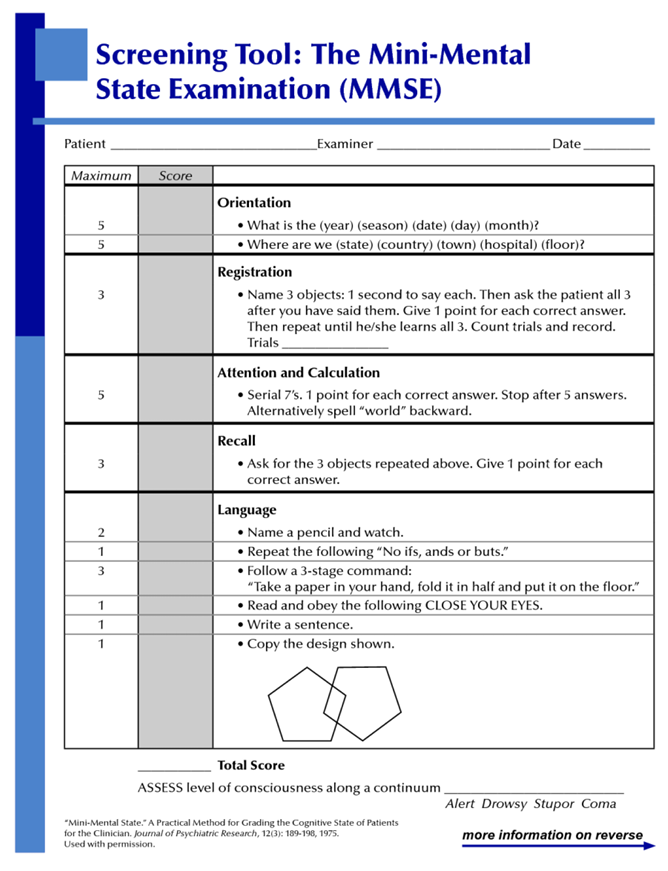
Mini-Mental State Examination (MMSE)
Mini-Cog
What are the common tests used to assess cognition? What are the normal responses and scores? When would you use each one? (MMSE)
MMSE used as an initial assessment and as a serial measure (repeated over time to track changes in cognitive impairment)
30 Questions: Assesses Orientation, Registration, Attention & Calculation, Recall, Language
Maximum score 30
23-30 → Normal
19-23 → Borderline
<19 → Impaired
What are the common tests used to assess cognition? What are the normal responses and scores? When would you use each one? (Mini-Cog)
Used when you need to screen for cognitive impairment in otherwise healthy older adults
Consists of 3-item recall test
Clock Drawing test
Total Score 0-5
Score 3, 4, or 5 → Lower likelihood of Dementia
Score < 3 → Validated for dementia screening and further assessment

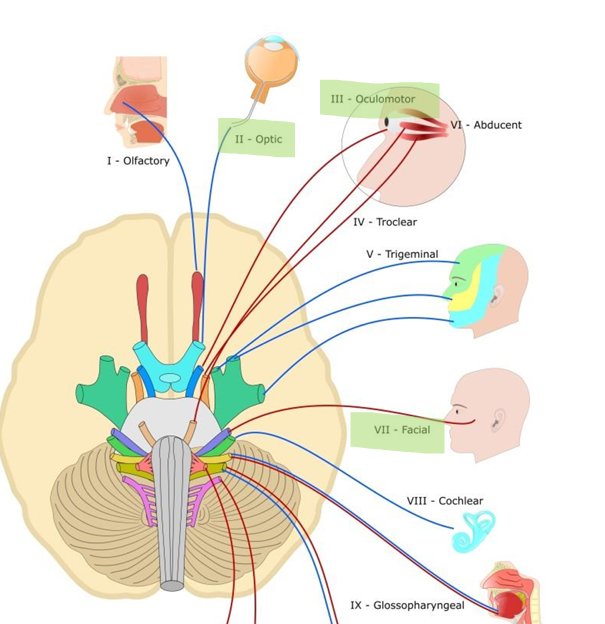
What does the Pupillary Light Reflex assess?
CN II (optic) and CN III (oculomotor) and brainstem activity
What are the steps to perform Pupillary Light Reflex assessment and what are the assessment elements? What are normal & abnormal responses? How would you document your findings? What is accommodation and how do we assess for it?
Prepare environment (dim/darken room)
Inspect pupils before testing (size, shape and symmetry)
Test direct light reflex (shine penlight from side and watch for constriction)
Test consensual light reflex (observe opposite pupil, both should constrict same time without shining light on it)
Assessment Elements:
PERRL(A)
Pupils, Equal, Round, React to Light, Accommodation
What are the steps to perform Pupillary Light Reflex assessment and what are the assessment elements? What are normal & abnormal responses? How would you document your findings? What is accommodation and how do we assess for it?
Normal Responses
Pupil constricts (direct light reflex)
Normal findings document PERRLA: P 3-5 mm, E symmetry, equal, R round shape, RL response to light, brisk bilateral
Opposite pupil constricts same time without shining light on it (consensual light reflex)
Abnormal Response
Pupils don’t react to light / remain dilated (Optic nerve injury (CN II) )
Opposite pupil doesn’t constrict (Oculomotor injury (CN III) )
What are the steps to perform Pupillary Light Reflex assessment and what are the assessment elements? What are normal & abnormal responses? How would you document your findings? What is accommodation and how do we assess for it?
Accommodation is adaptation of the eye for near vision
With focus on distant object → pupils dilate
With focus on a near object → pupils constrict
Normal findings
Pupil constriction and convergence
Interpretation: Patient has good CN2, CN3 and brain stem function, neurologically intact
What is the purpose of a motor assessment? What does ______ movement require?
To check voluntary movement by giving the person specific commands
Voluntary movement requires transmission of a message from cerebral cortex to the appropriate muscle on opposite side of body
Normal finding of pupillary light reflex and how do we document?
Document: PERRLA - Pupils Equal Round React to Light Accommodation
3-5mm (Pupil)
Symmetry, equal (Equal)
Round shape (Round)
Response to light, brisk bilateral (React to Light)
Accommodation (A)
What is Anisocoria?
When the pupils are different sizes (not symmetrical)
How do you assess motor function in a neurological exam as discussed in class? What are the assessment elements? What are the normal and abnormal responses?
Check for strength & symmetry of CN VII (Facial), upper extremity, lower extremity
CN VII: lift eyebrows, frown, bare teeth
Upper extremity: hand grasps
Lower extremity: push one foot at a time against you psalms one at a time
How do you assess motor function in a neurological exam as discussed in class? What are the assessment elements? What are the normal and abnormal responses?
Symmetrical, equal
strong
coordinated
CN VII: Patient raise eyebrows symmetrically. Frown smile symmetrical on both sides of the face
Upper Extremity: Symmetrical motor function. Strong and equal strength on both sides of hands
Lower Extremity: Patient has strong and equal strength on both sides. Symmetrical motor function.
Interpretation: Patient neurologically intact. No Neurological deficits
What is the purpose of a musculoskeletal assessment? What are the key elements?
Assess function, mobility, detect abnormalities
Inspection and Palpation for abnormalities or deformities
Range of motion of joints (ROM)
Muscle strength and tone
Soft Tissue Integrity
Mobility: Gait and Balance
What assessment techniques are used? What characteristics are used to assess musculoskeletal system? What are the normal and abnormal responses?
Inspection
Palpation
Range of motion
Strength Testing
Tone assessment
Functional mobility test
What assessment techniques are used? What characteristics are used to assess musculoskeletal system? What are the normal and abnormal responses?
Symmetry
Size and shape
Tenderness, swelling, warmth, erythema, deformities
Crepitus
Postural abnormalities
Pain
What assessment techniques are used? What characteristics are used to assess musculoskeletal system? What are the normal and abnormal responses?
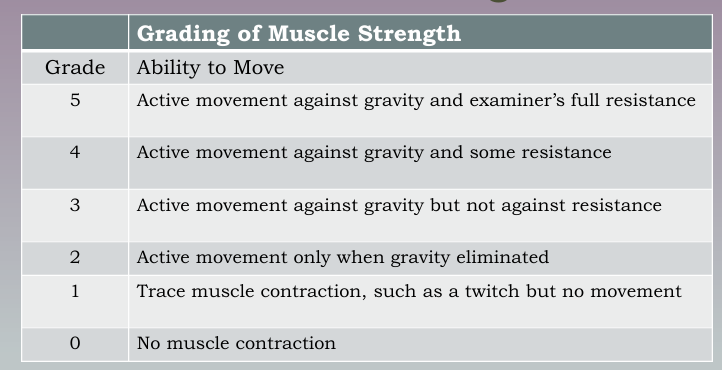
Normal: Equal bilaterally and able to fully resist opposing force
Abnormal: No muscle contraction, no movement, can’t resist against force
Abduction
Movement away from the body
Adduction
Movement toward the body
Internal rotation
Turning limb toward midline
External rotation
Turning limb away from midline
Muscle strength
Ability to contract and create force against resistance
Muscle tone
Tension in a muscle at rest
How is muscular tone assessed? What is normal and abnormal muscle tone?
Felt through movement of muscle in a relaxed state
Normal: Mild, even resistance through entire range
Abnormal: Hypertonic (rigid), Hypotonic (flaccid)
What is ROM? Define some of the terms to describe ROM as discussed in class? What are the assessment elements for assessing ROM?
Range of Motion
Terms: Abduction, Adduction, Internal rotation, External rotation
What is ROM? Define some of the terms to describe ROM as discussed in class? What are the assessment elements for assessing ROM?
Assessment elements through exercises that moves a joint through the extent of its limitations
Active ROM (Pt moves their own joint)
Passive ROM (external force moves their joint via PT or equipment)
Compare for Symmetry
Ease of movement
Pain or Tenderness
Full ROM or Limited ROM
Crepitus
What joints did we assess ROM? What questions do we ask?
Shoulder, Elbow, Wrist, Hip, Knee, Ankle
Questions:
Full ROM or limited?
Symmetrical? (on both sides)
Any pain, tenderness, or crepitation?
How do you assess muscular strength? What are the normal and abnormal responses?
Grades 0-5 Table of muscle strength
Normal Findings:
Equal bilaterally and ability to fully resist opposing force
5/5
Abnormal
Unequal bilaterally (unequal strength on both sides)
Less than 5 grade
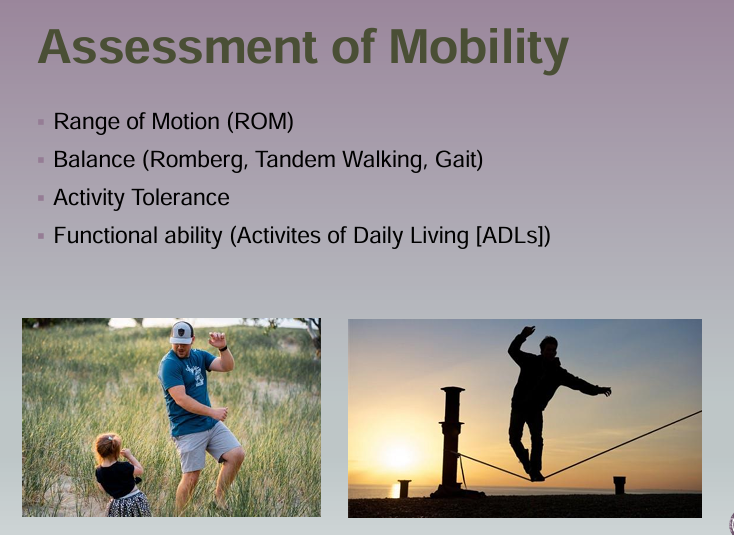
What are the elements of a mobility assessment?
Range of motion (ROM)
Balance (Romberg, Tandem Walking, Gait)
Activity tolerance
Functional ability (Activities of Daily Living (ADLs) )
What are the elements for assessing patient safety for mobility and when are you able to move through the different levels of mobility?
Elements of assessing patient safety begin in position of most support and move to higher levels according to his or her tolerance
Lying down
Sitting up
Standing
Transfer to chair
Walking
What are the tests/tools used to assess balance? How do you perform each test and what are the normal responses?
Romberg
Tandem Walking
Gait
What are the tests/tools used to assess balance? How do you perform each test and what are the normal responses? (Romberg Test)
Ask person to close eyes and hold position of standing with feet together and arms at side. Stand close in case he/she falls
Normal response (negative): patient can hold posture and balance, maybe some swaying
Interpretation normal: Patient had good balance; patient has good cerebellar brain function
Abnormal response (positive): increase sway/inability to keep balance
What are the tests/tools used to assess balance? How do you perform each test and what are the normal responses? (Tandem Walking)
Walk in a straight line heel to toe
Normal: walk straight and stay balances
Interpretation normal: Patient has good balance
Abnormal: inability to walk straight/can't keep balanced
What are the tests/tools used to assess balance? How do you perform each test and what are the normal responses? (Gait)
Person walk 10-20 feet away from you, turn, and return to starting point
Normal: ability to move with a sense of freedom, smooth, rhythmic, effortless, opposing arm swing coordinate, steady
Interpretation normal: has no gait deficits and is able to keep balance
Abnormal: deviation from normal pattern of walking, change in posture, stride, foot placement, rhythm
What are the elements for assessing activity tolerance?
Able to perform activity without undue exertion/possible injury
Assess for dyspnea, fatigue, chest pain when activity begins
Assess for change in vital signs if such s/s develop
What are the different complications as a result of immobility? What are preventative measures for each one?
Contractures
Muscle weakness
Loss of muscle mass and strength
Orthostatic hypotension
Thrombus formation (blood clots)
Respiratory Complications
Pressure injuries (Integumentary complications)
What are the different complications as a result of immobility? What are preventative measures for each one? (Muscle Weakness)
Prevention of Muscle Weakness
Encouraging daily out of bed activity or mobilization
Walking
Sitting in chair/wheelchair
Physical Therapy
What are the different complications as a result of immobility? What are preventative measures for each one? (Thrombus formation)
Definition: Blood clot formed withing the vascular system caused by stagnant blood
Preventative:
Leg, foot, and ankle exercises
Provide fluids if permitted
Frequent position changes
Educate patient about risk
SCD device (compression device)
Compression socks
Medication prophylaxis (e.g. heparin, lovenox)
What are the different complications as a result of immobility? What are preventative measures for each one? (Respiratory Complication)
Mobilization/High Fowlers
Cough and Deep Breathing
Fluid increase
incentive spirometer
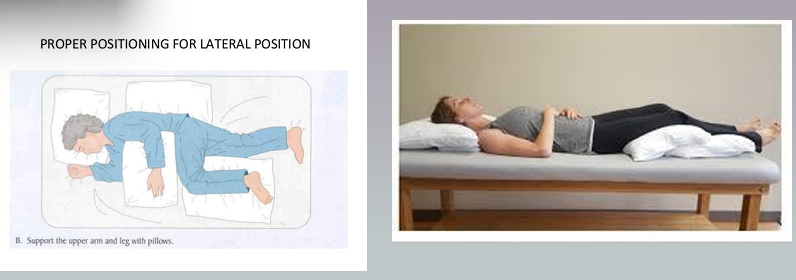
What are the different complications as a result of immobility? What are preventative measures for each one? (Skin Complications)
Pressure Injuries
Prevention
Reposition body every 1-2 hours in bed and every hour when sitting up in a chair
Teach patient who are able, to shift weight every 15 minutes
Skin care
Apply pressure relieving devices including specially designed beds
Nurses IRL uses a lot of pillows
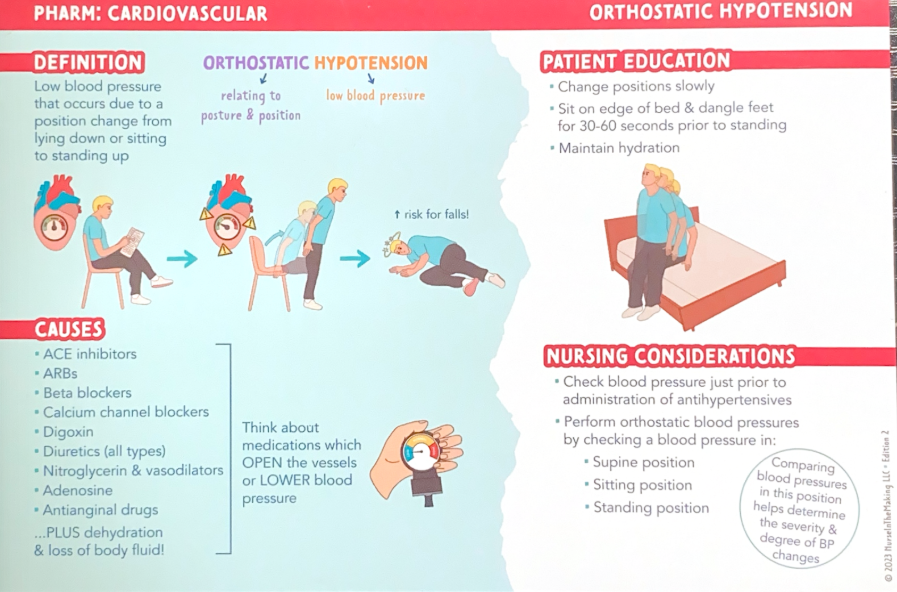
What is orthostatic hypotension and when do you assess for it? When is a patient positive for orthostatic hypotension?
Orthostatic (relates to posture & position)
Hypotension (low blood pressure)
Definition: Low blood pressure that occurs due to a position change from lying down or sitting to standing up
Assess for it for patients at risk:
Elderly (greatest risk)
Prolonged bedrest
Hypovolemic
Some medications
What is orthostatic hypotension and when do you assess for it? When is a patient positive for orthostatic hypotension?
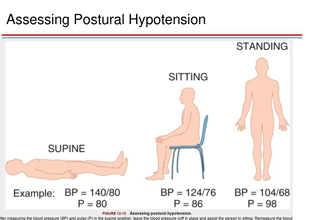
Positive for patients with drop of blood pressure or following symptoms
Greater or equal than 20 mmHg systolic pressure (↓ >20 mmHg)
Lying BP 140/70 → Standing BP 115/68 BP
OR
Greater or equal than 10 mmHg diastolic pressure (↓ >10 mmHg)
Lying BP 140/70 → Standing BP 138/58
Symptoms
Dizziness
Lightheadness
Nausea
Tachycardia
Pallor or fainting when patient changes from supine → standing
Orthostatic hypotension prevention
Mobilize patient as soon as physical condition allows to minimize risk
Expected findings in Healthy Adult (normal) orthostatic blood pressure
Systolic pressure of 10 mmHg or less with position change (↓ >10 mmHg)
EX: Lying BP 140/70 → Standing BP 131/68
How to assess orthostatic hypotension
Have patient rest supine for 2-3 minutes
▪ Take baseline BP and P (supine)
▪ Take BP and pulse with patient sitting on side of bed
▪ Take BP and pulse with patient standing
Take within 1-2 minutes of each position change
What if the patient is too weak of dizzy to stand?
Assess Supine and then sitting on side of bed with legs dangling
Don’t sit this patient up at the side of the bed without help
You must help them
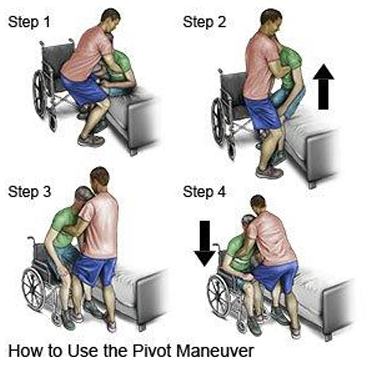
What are principles of body mechanics?
Plan ahead
Broad base of support
Lower the center of gravity
Face direction of movement, don’t twist
Keep close to the patient
What is the purpose of a lung assessment?
Assess ventilation, respiratory function and detect possible respiratory problems
What are the common elements of a subjective lung assessment? How do we further assess each one? What are the normal and abnormal findings?
Asking questions
"Do you any problems with breathing?”
“Do you have it at rest or with activity?”
“Do you have a cough?”
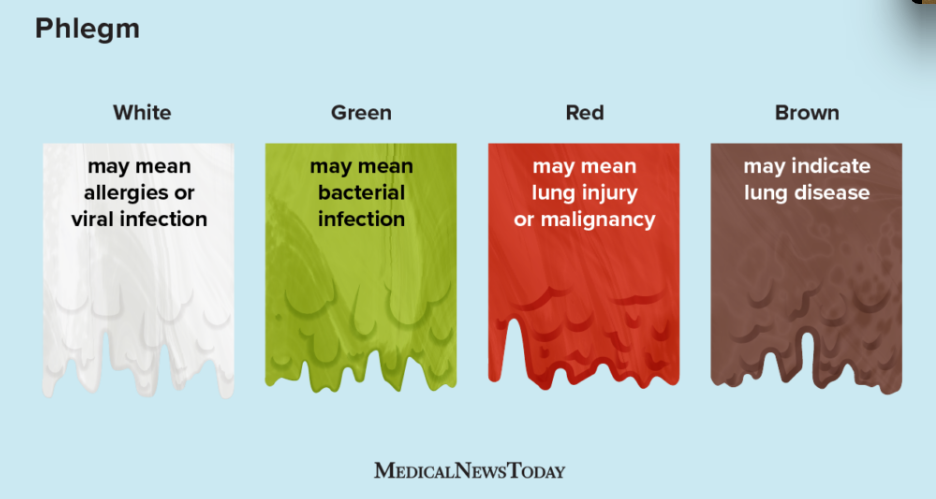
“Do you cough up any phlegm or sputum?”
- “How much?”
- “What color is it?”
- “What is the consistency?”
- “Are you coughing up any blood?”
What are the common elements of a subjective lung assessment? How do we further assess each one? What are the normal and abnormal findings?
Further assessed through
Inspection
Palpation
Percussion
Auscultation
Normal findings: Clear and symmetrical on both sides for anterior and posterior lung sounds
What is the purpose of auscultation? What sounds to note for?
To listen to lung sounds using a stethoscope. Assess ventilation and note if the lung sounds are either clear, diminished, and adventitious.
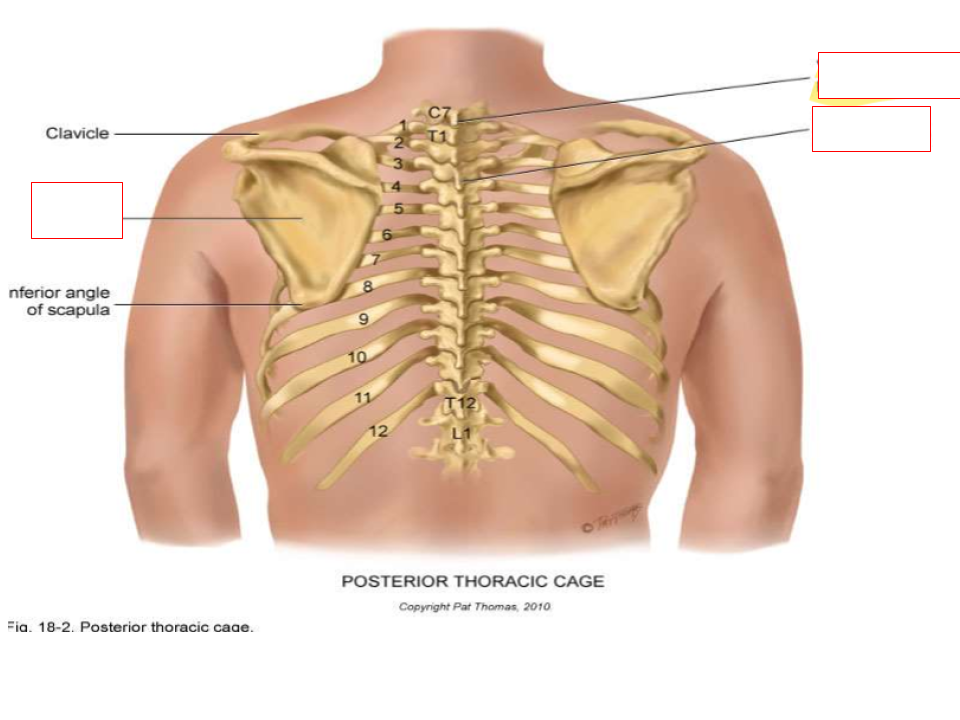
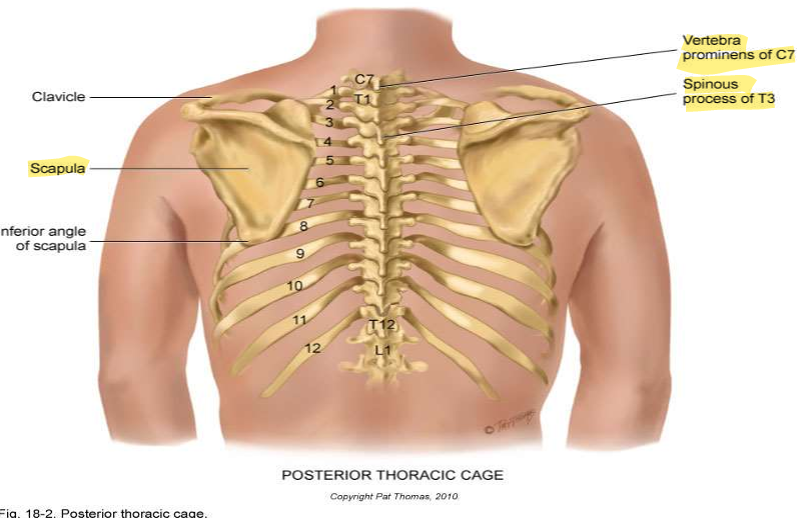
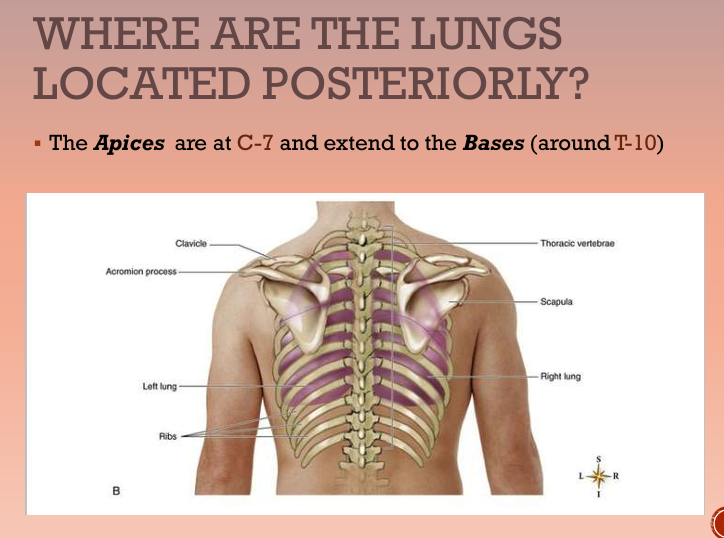
What are the posterior landmarks for lung assessment?
Scapula
C7 Vertebra prominens
T3 spinous process
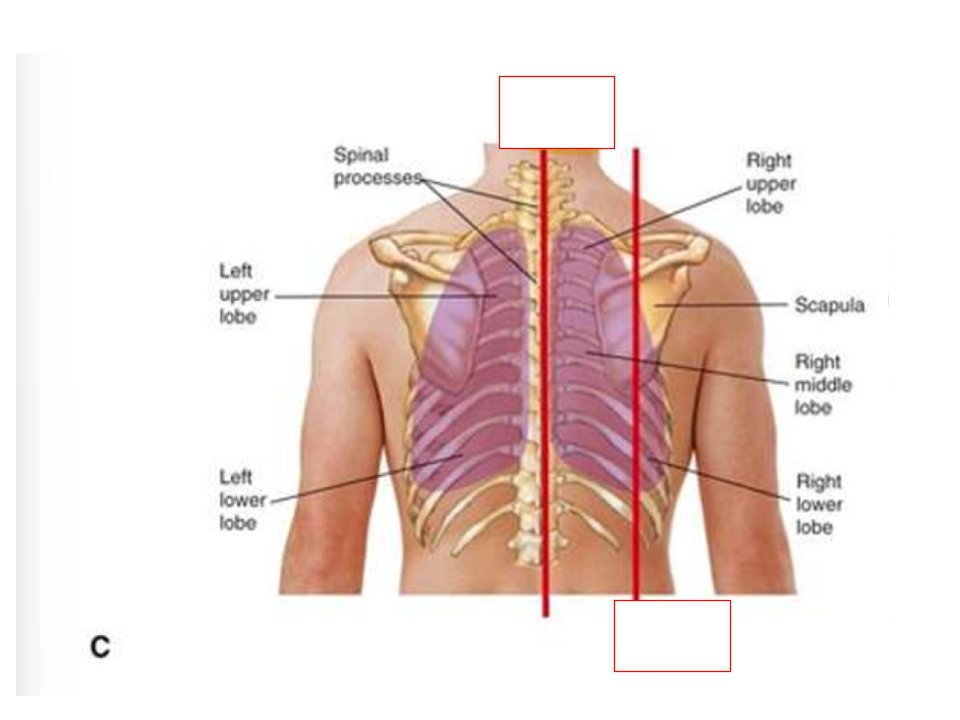
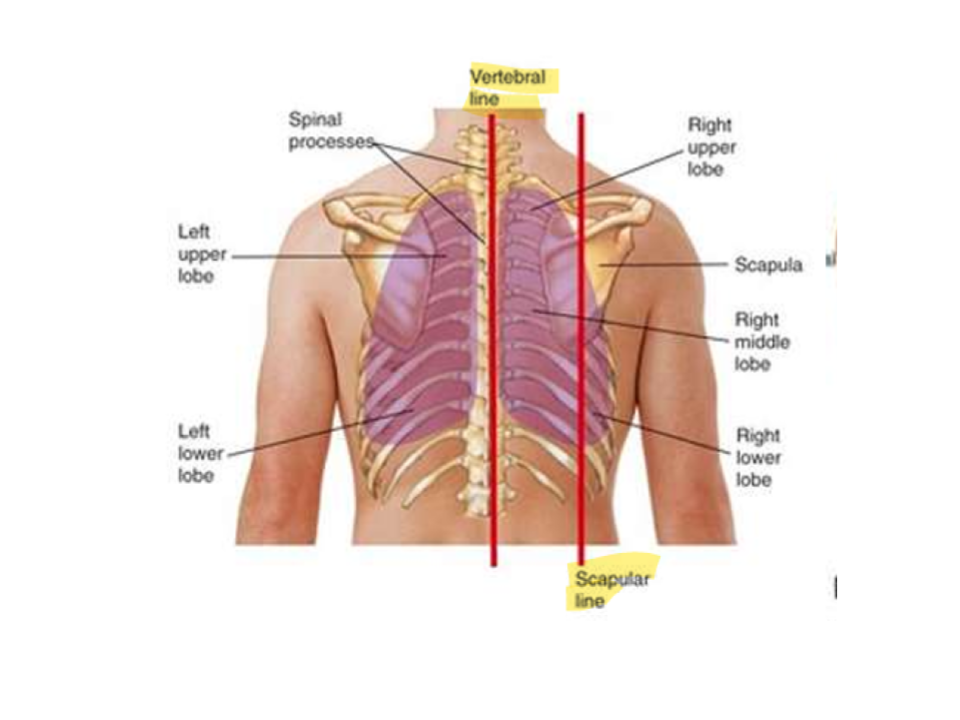
What are the posterior reference lines for lung assessment?
Vertebral line
Scapular line
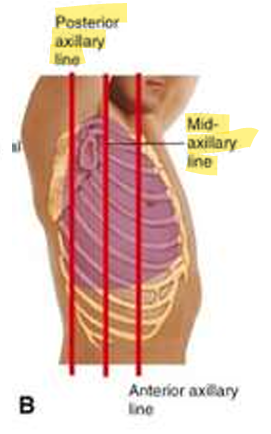
What are the posterior reference lines for lung assessment?
Posterior axillary line
Mid-axillary line
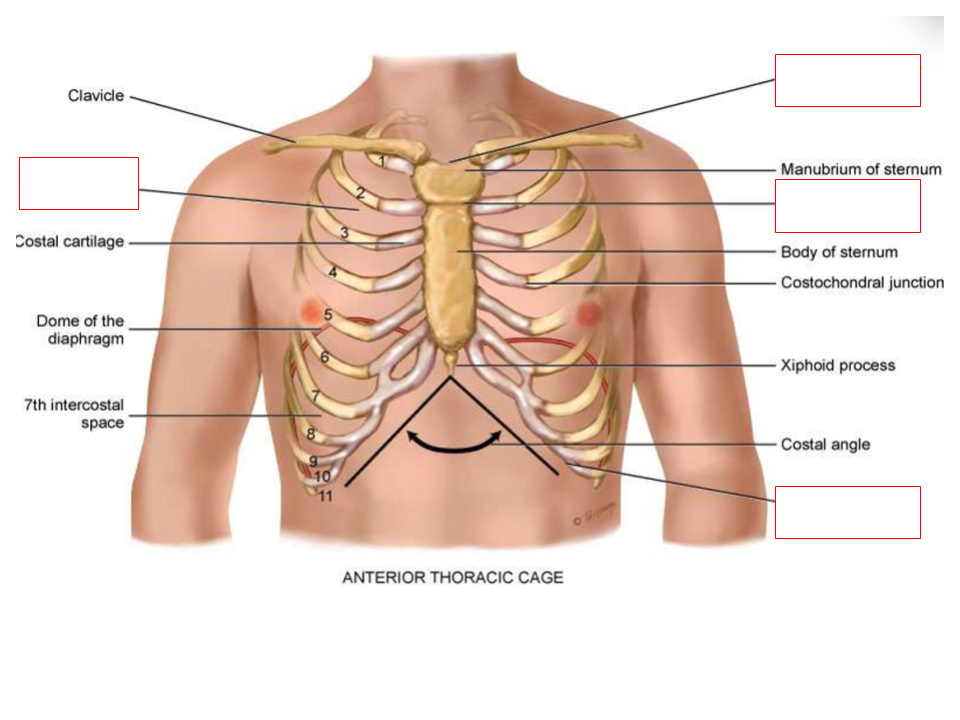
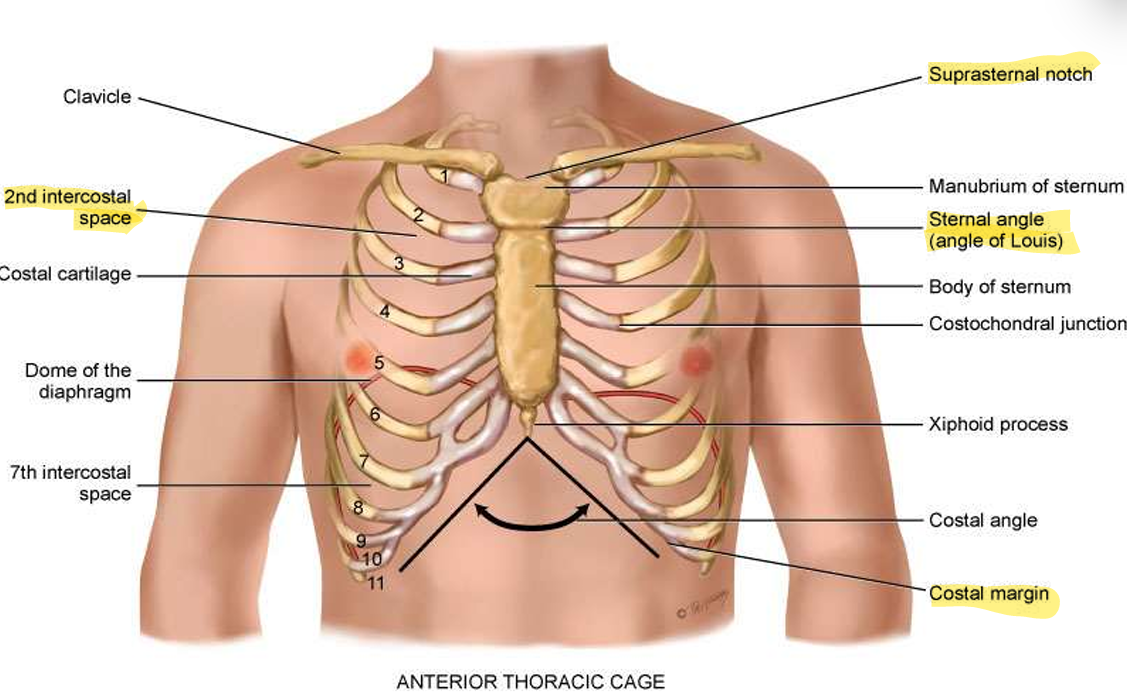
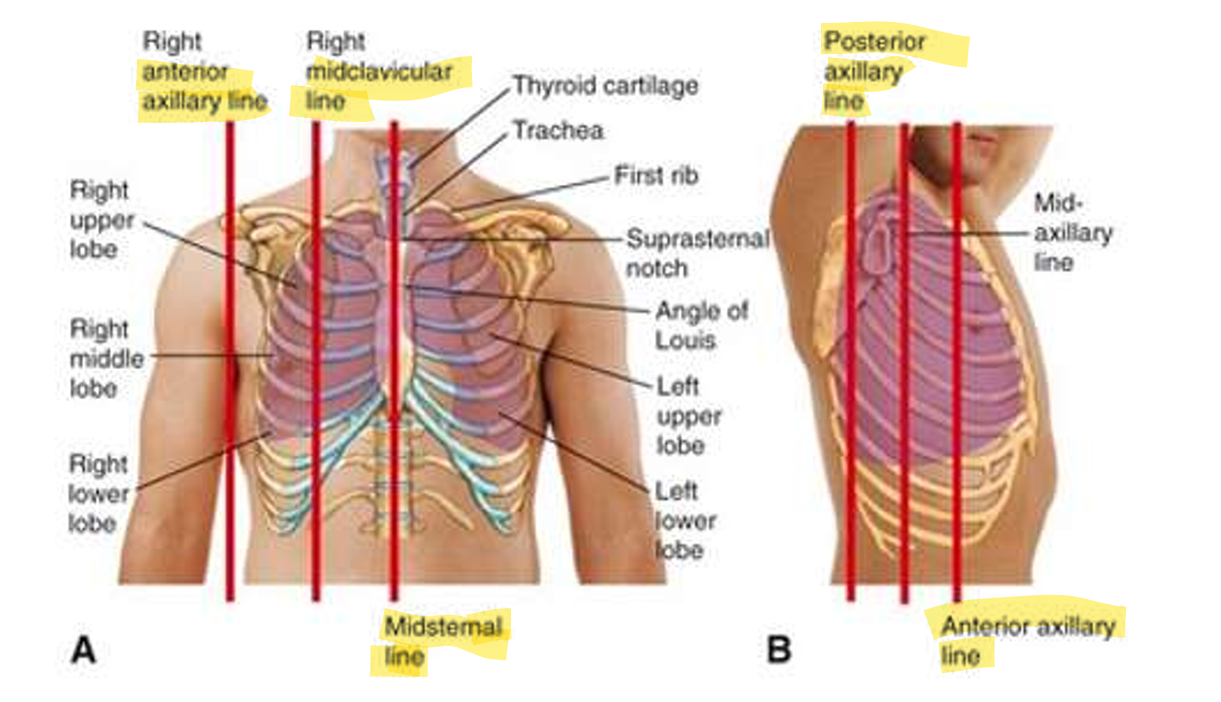
What are the anterior landmarks for lung assesssment?
Suprasternal notch
Sternal angle (angle of Louis)
Costal margin
2nd Intercostal space
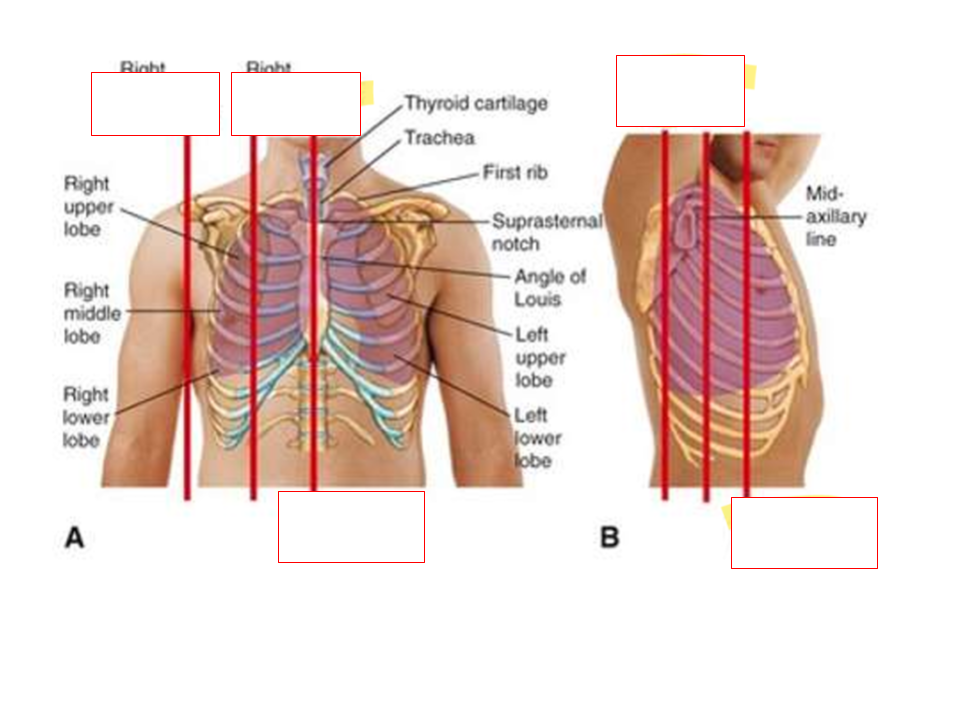
What are the anterior vertical lines for lung assessment?
A.
Anterior axillary line
Midclavicular line
Midsternal line
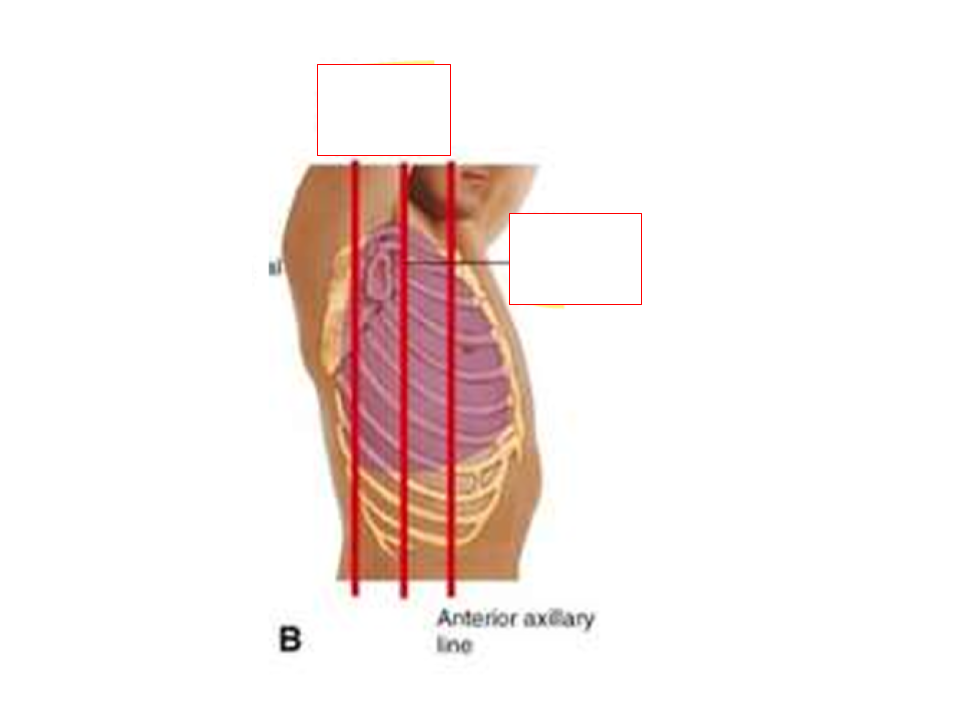
B
Posterior axillary line
Anterior axillary line
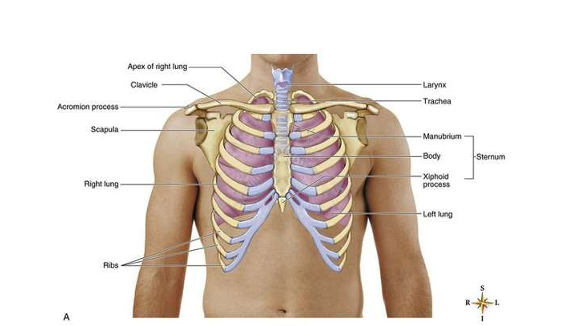
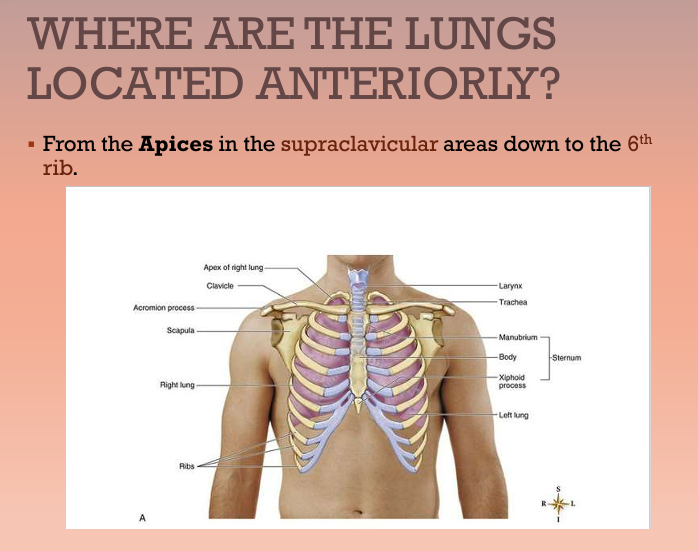
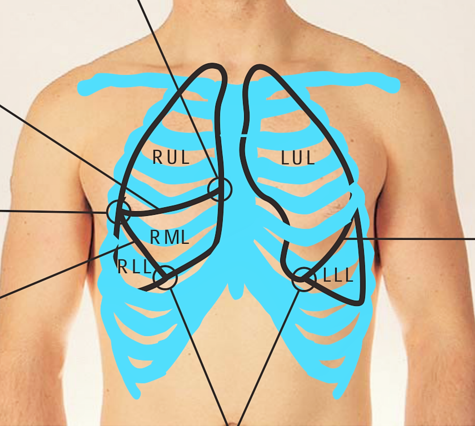
Where are the lungs located anteriorly?
Apices (top/apex plural) in the supraclavicular areas down to the 6th rib

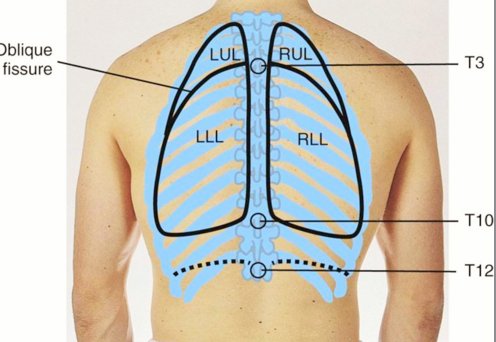
Where are the lungs located posteriorly?
Apices (top/apex plural) are at C-7 and extend to the Bases (around T-10)
What is the proper process/technique for auscultating lungs?
Evaluate presence and quality of normal breath sounds both anteriorly and posteriorly
Using flat diaphragm of stethoscope, listen to at least one full respiration (one inspiration/expiration cycle) in each location
Perform bilateral comparison (side to side comparison)
Note quality and location of breath sounds (Quality: clear, diminished, adventitious)
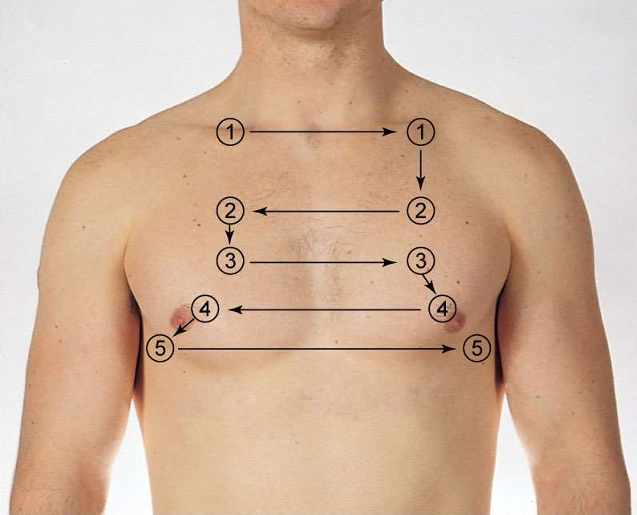
What are the proper placements and sequence for auscultating lungs anteriorly?
Above clavicle
2nd ICS
3rd ICS
4th ICS
5th ICS
6th ICS (midaxillary)
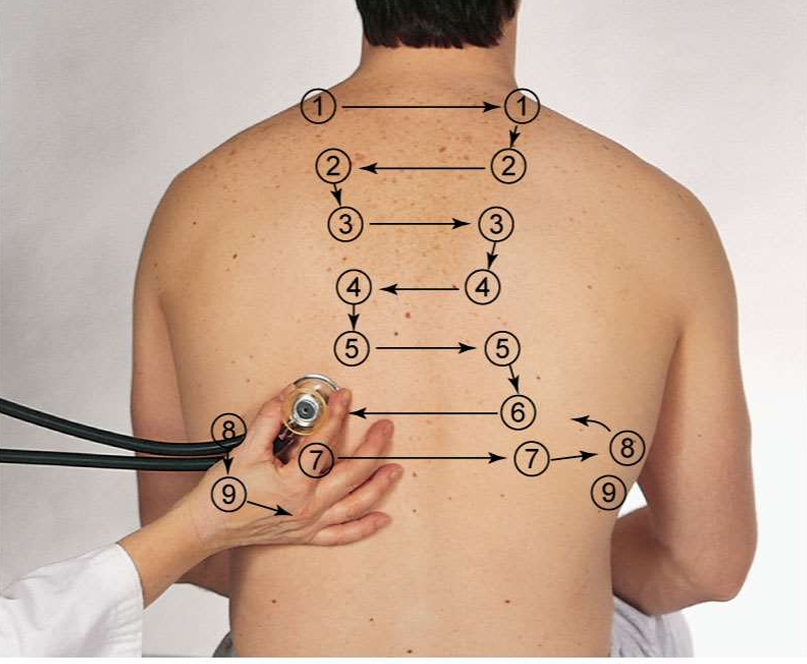
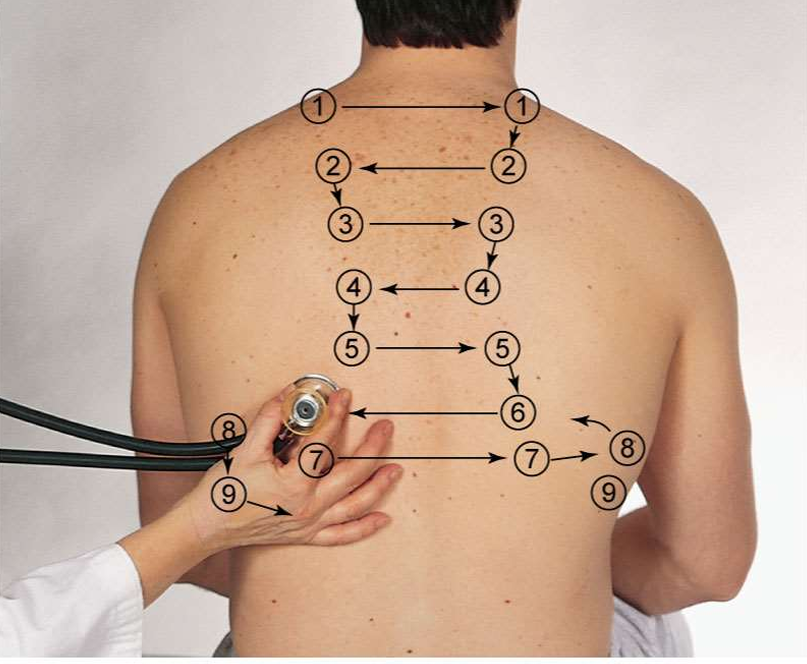
What are the proper placements and sequence for auscultating lungs posteriorly?
Above shoulder blade
C7 to T3 (assesses upper lobes)
T3
T4
T3 to T10 (assess lower lobes)
Almost midaxillary
Anterior Lobes (Right Lung/Left Lung)
Right
RUL
RML
RLL
Left
LUL
LLL
Posterior Lobes (Right Lung/Left Lung)
Left
LUL
LLL
Right
RUL
RLL
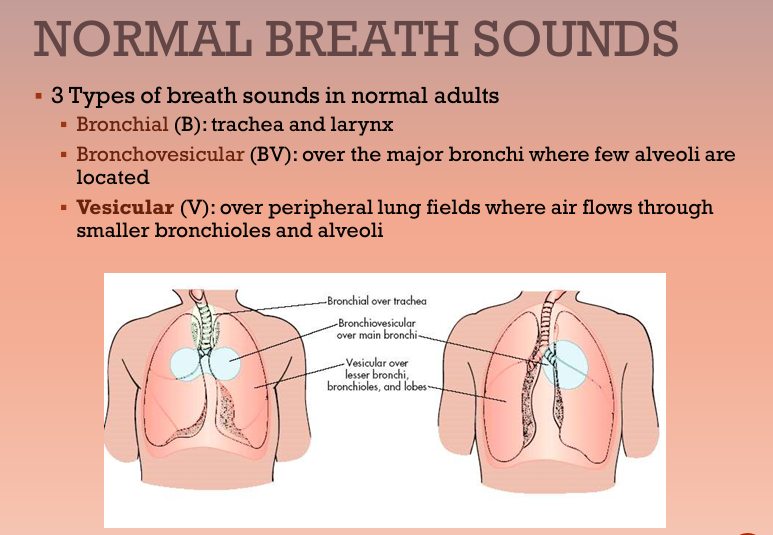
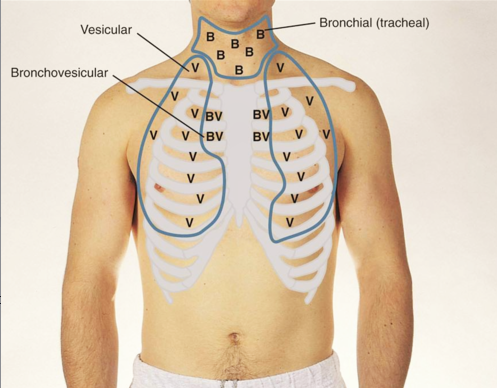
What are the 3 different normal breath sounds and where can you locate each one?
Bronchial (B) (trachea, larynx)
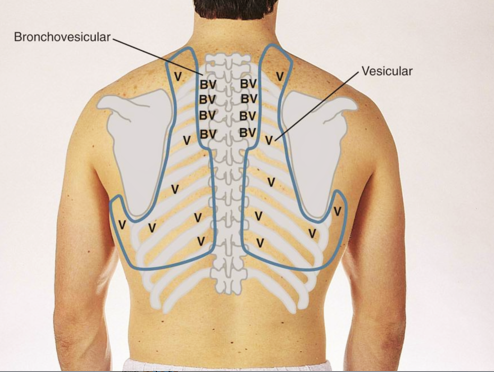
Bronchovesicular (BV) (major bronchi)
Vesicular (V) (peripheral lung fields)
Anterior Breath Sounds
B, BV, V
Posterior Breath Sounds
BV, V
Vesicular Heart Sounds
What it sounds like
Bro