2nd/3rd Trimester Cervix and Amniotic Fluid (Ch. 51 & 58)
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
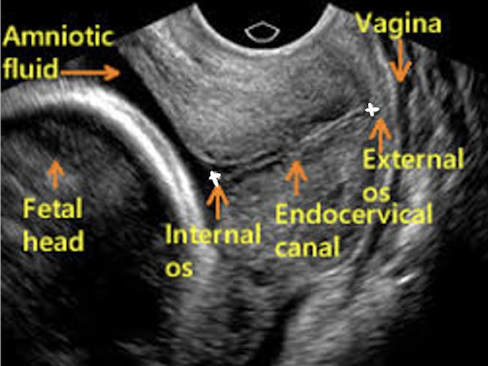
cervical length
CL = distance between internal os and external cervical os
normal length (gravid uterus) is at least 3 cm
cervical incompetence is CL less than 2.5 cm
short CL is marker for increased preterm birth loss
risk of loss inverselt proportional to CL
normal CL vs. cervical incompetence CL
normal is at least 3 cm
cervical incompetence is >2.5 cm
cervix: transabdominal technique
scan through amniotic fluid/bladder to image cervix
measure length of cervix from internal os to external os
do not include vaginal canal in measurement
pitfalls:
maternal body habitus
full bladder can compress LUS and mimic a long closed cervix
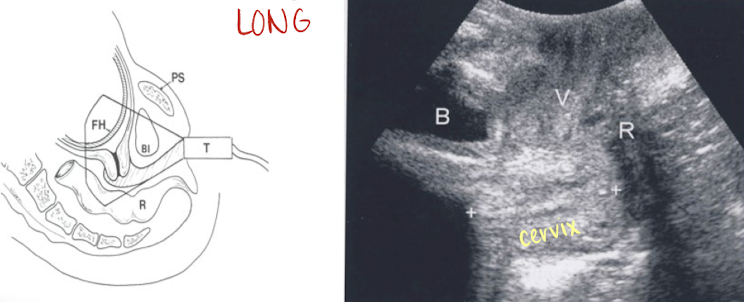
cervix: translabial technique
alternative technique for assessing cervical length
curvilinear transducer placed over labia
less accurate than TV technique
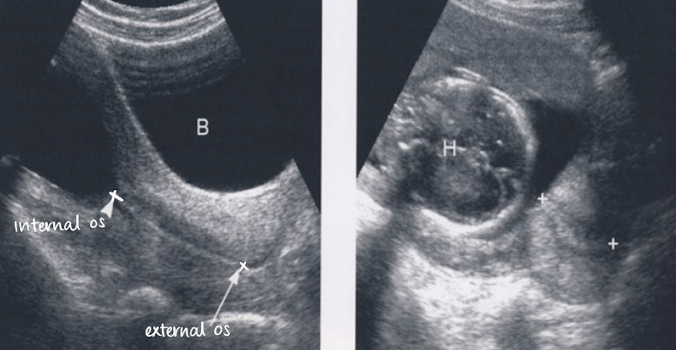
cervix: transvaginal technique
GOLD STANDARD method
bladder is empty
define cervical canal—take close-up shot (75% of screen)
measure length from internal os to external os
if cervix is curved, use trace or obtain two or more linear measurements then add them together
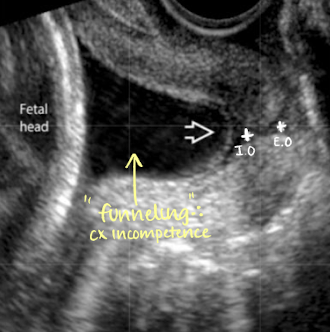
what is cervical incompetence
when CL is less than 2.5 cm
cervix does not remain closed
causes and S/S of cervical incompetence
causes:
lacerations
uterine anomalies
previous trauma
symptoms:
asymptomatic
painless dilation
recurrent 2nd trimester loss
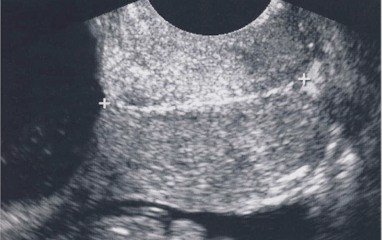
is this normal or cervical incompetence?
normal

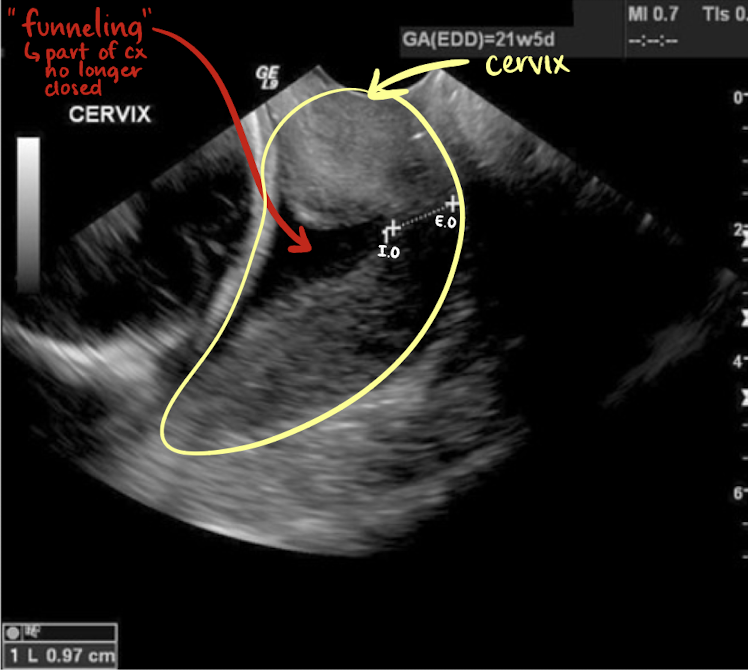
is this normal or cervical incompetence?
incompetence
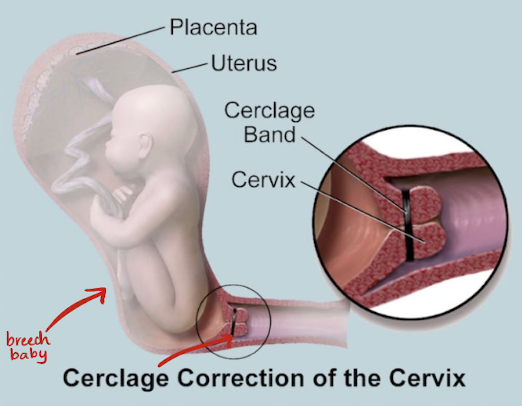
cervical cerclage
tx for cervical incompetence
cervix is stitched closed to prevent preterm birth
cerclage removal:
removed around 36-37 weeks GA for planned vaginal delivery OR
left in place and removed at time of planned cesarean delivery (c-section)
SONO: cervical cerclage
post-cerclage procedure; imaged transvaginally
cerclage stitches are echogenic with posterior shadowing
serial scans may be done to ensure cerclage remains secure and cervix is closed
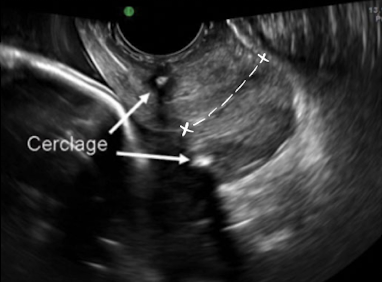
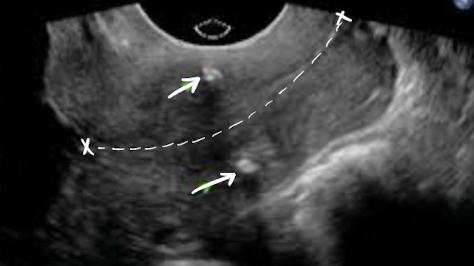
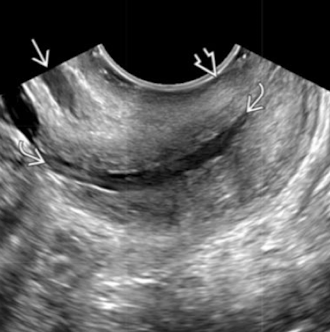
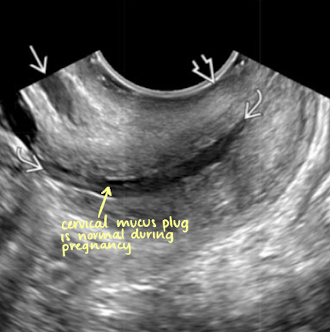
what are the arrows pointing to?
cervical cerclage stitches
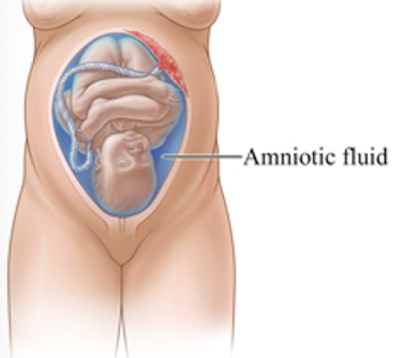
amniotic fluid
fluid surrounding fetus within amnion
plays vital role in fetal growth and allows fetus to move freely
produced by umbilical cord, membranes, lungs, skin, kidneys, and mostly by urinary tract
early 1st trimester: fetal membranes
late 1st trimester: skin
2nd/3rd trimester: kidneys (urine)
amniotic fluid function
protection
allows for fetal movements
prevents adhesions
allows symmetric growth
maintains temperature
acts as reservoir to fetal metabolites before excretion
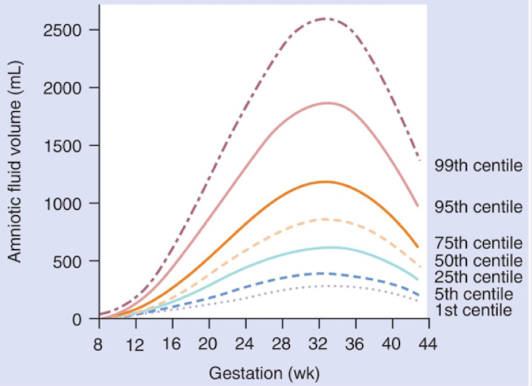
amniotic fluid volume
amount of fluid is a balance between production and consumption
volume of AF increases until about 33 weeks
25 mL per week (11w-15w)
50 mL per week (15w-28w)
volume doubles until week 28 (declines after that)
adequate volume is critical for lung development
by the end of pregnancy there is sharp decline in amount of amniotic fluid
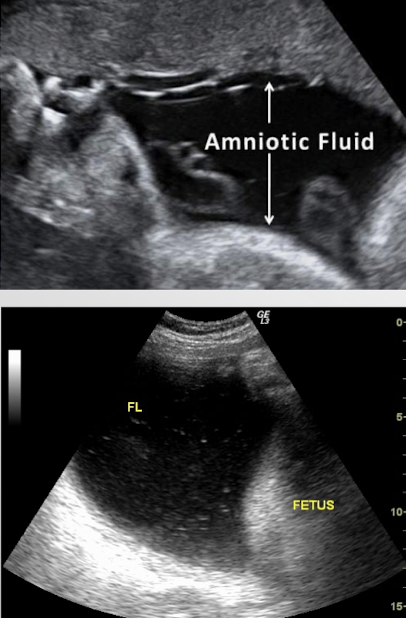
SONO: amniotic fluid
generally echo-free
can sometimes see tiny echogenic particles
blood, normal variant, vernix caseosa, meconium
presence of a dense collection, or sludge, could indicate infection
3 amniotic fluid measurement methods
subjective
amniotic fluid index (AFI)
single pocket
AF measurement methods: subjective
eyeballing
amniotic fluid index (AFI)
single pocket
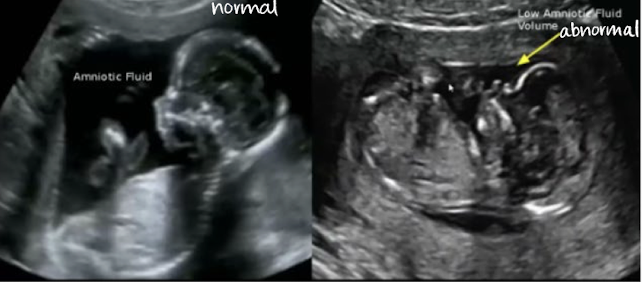
AF measurement method: subjective
“eyeball” assessment of amount of fluid
no actual measurements
better used early in gestation
successful with more experienced sonographer
leads to a more quantitative assessment


which has subjectively less AF?
right image
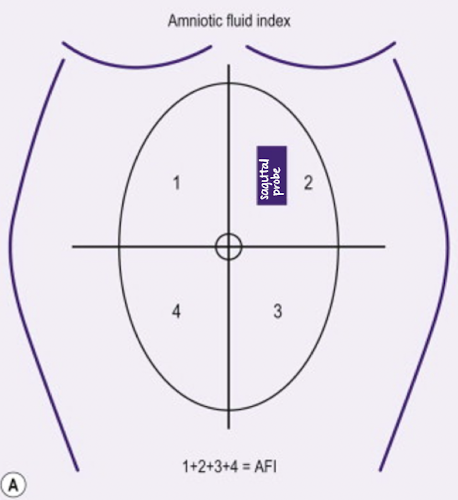
AF measurement method: amniotic fluid index (AFI)
most used method for quantifying amniotic fluid volume
uterine cavity is divided into 4 equal quadrants
largest pocket in each quadrant is measured (AP) in SAG plane and added together
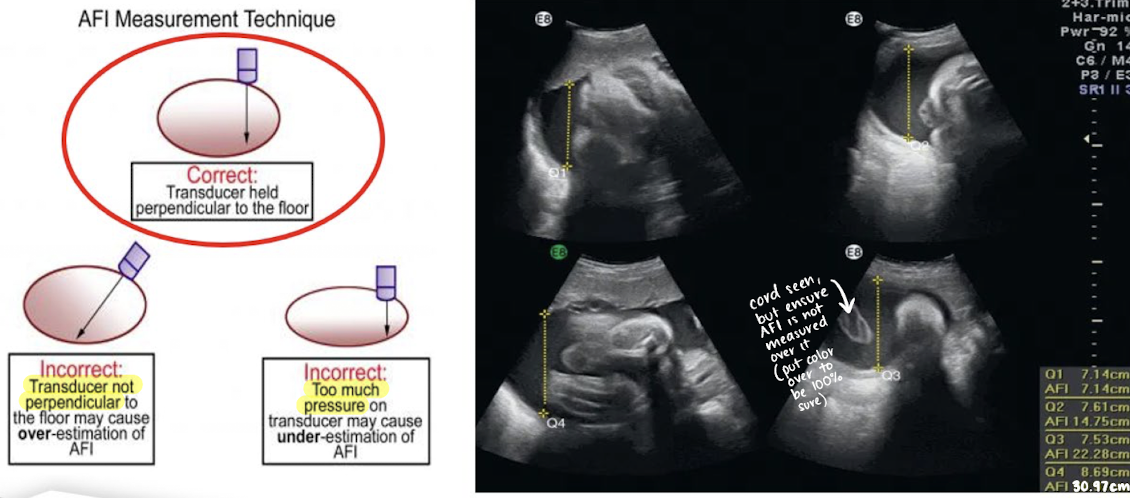
transducer should be perpendicular to table, not curved skin surface
exclude fetal limbs and umbilical cord loops )can use color Doppler)
do NOT measure through a structure
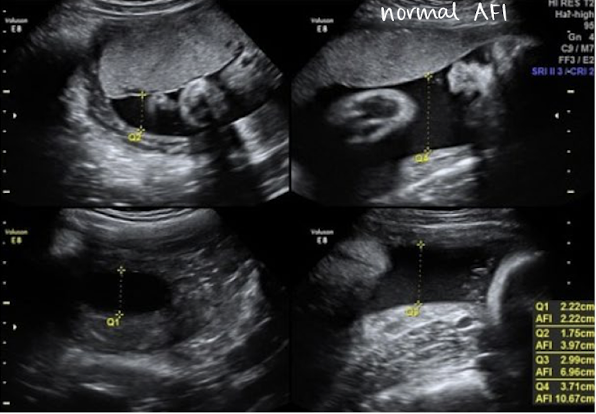
AF measurement method: AFI example
normal AFI values
10 cm < AFI < 20 cm
should be between 10-20 cm
borderline AFI values
5-10 cm (low side); 20-24 cm (high side)
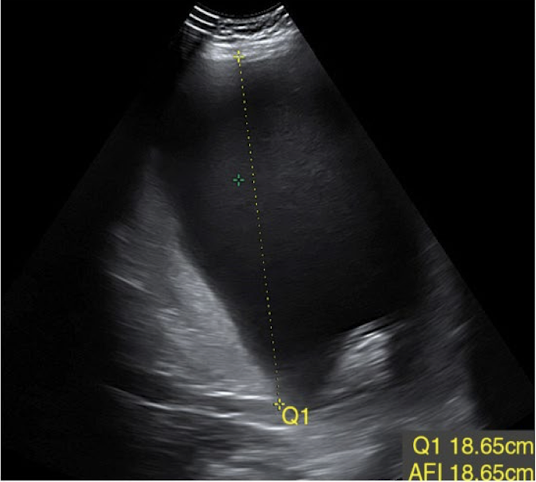
abnormal AFI values
oligohydramnios (too little)
AFI < 5 cm
polyhydramnios (too much)
AFI > 24 cm
AF measurement method: single largest pocket (MVP)
maximum vertical pocket assessment (MVP)
measure largest pocket in AP
pocket should be clear of fetal parts and umbilical cord
normal single pocket (SP or MVP) values
2 cm < SP < 8 cm
should be between 2-8 cm

abnromal single pocket (SP or MVP) values
oligohydramnios (too little)
SP < 2 cm
polyhydramnios (too much)
SP > 8 cm
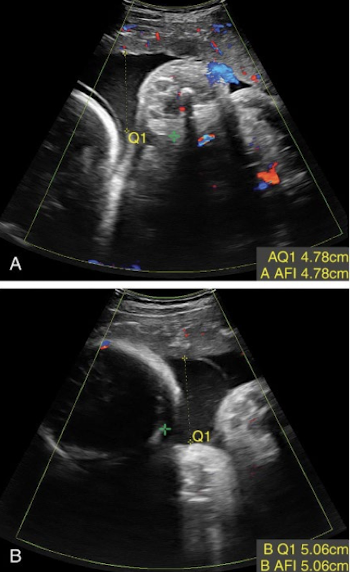
how to measure AFI for twins?
have a slightly lower AFI than singleton pregnancies
AFI gives overall assessment for pregnancy not search sac
assess each sac independently
largest vertical pocket is more accurate in polyhydramnios
most accurate is to use dye amniocentesis method