Exam II Week 7: Common Hip Disorders
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
Match the sxs to the condition:
Antalgic gait
Decreased ROM of hip and/or knee
Pain with active motion
Pain with passive stretch
Edema– Variable ecchymosis (24-48 hours)
Focal tenderness to palpation
Severe cases: palpable defect
Muscle Strain

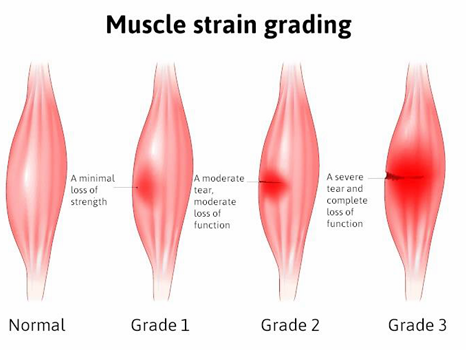
What muscle strain GRADE is this referring to?
Min tissue disruption
Low-grade inflammation
Strength: good w/ pain
No loss of ROM
Grade I
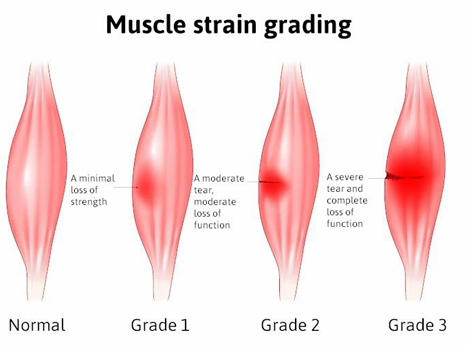
What muscle strain GRADE is this referring to?
Some disruption of tissue
↓ strength & ROM
Significant Pain
Grade II
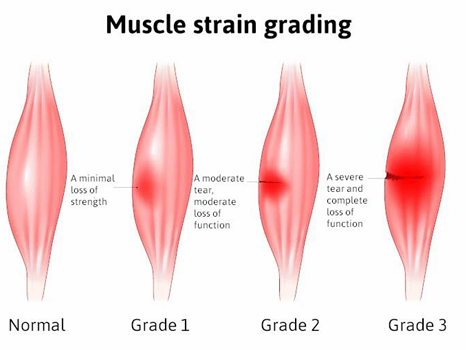
What muscle strain GRADE is this referring to?
Complete disruption
Complete loss strength
Palpable defect
Grade III
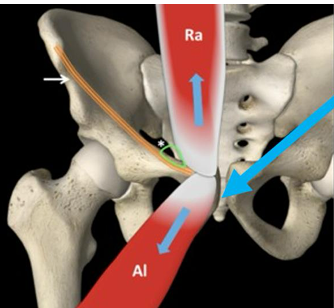
What is the most frequently strained muscle?
Hamstrings! → specifically biceps femoris
What two conditions can be confused for a gluteus medius strain?
***GTPS*** and GT bursitis
GTPS is believed to the a tendinopathy of the…
gluteal tendinopathy → usually gluteus medius

At what stage of healing of a muscle strain is it ESSENTIAL to avoid streching the injured tissue (esp HS)?
Stage II (~48-72 hrs)
What is an ESSENTIAL part of the acute treatment of a quadriceps contusion?
Knee brace positioned of maximally tolerated flexion
24 hrs in 120 degrees flexion
Better if initiated within 10 minutes of injury**
Avoid massages and NSAIDs

“Development of heterotopic bone formation in the muscle belly, possible complication of a contusion injury”
Myositis Ossificans

When will radiographs show myositis ossificans signs?
7-10 days signs of early ossification
Heterotopic bone formation 2-3 wks
What are some important treatment considerations for Myositis Ossificans?
POLICE acute injuries
Protected weightbearing (Crutches)
Start with gentle ROM exercises → Isometrics after swelling resolves
NSAIDS/corticosteroids for persistent swelling
Avoid: heat, massage, premature return to aggressive stretching, strengthening, or return to sport
Return to activity does not occur until after bony growth subsides

Match the sxs to the condition:
Trunk flexed/toward injured side
Ecchymosis/swelling
Pain w/ use of muscles attached to iliac crest
Focal TTP
Iliac Crest Contusion: Hip Pointer

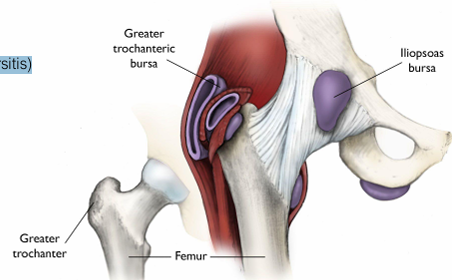
What is the most common bursa affected by hip bursitis? What is the most common cause?
Trochanteric bursa
Often d/t inflammatory arthritis, it can also be d/t trauma and repetitive activity
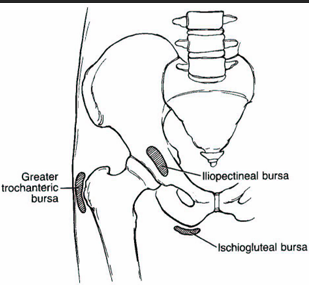
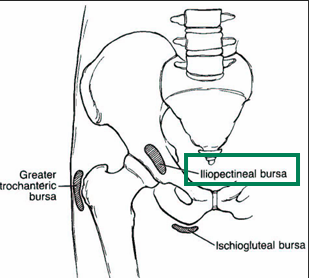
Match the sxs to the condition:
TTP femoral triangle
Pain with active hip flexion, passive extension
MMT: pain with hip flex
(+) Thomas test, FABER
Iliopectineal Bursitis
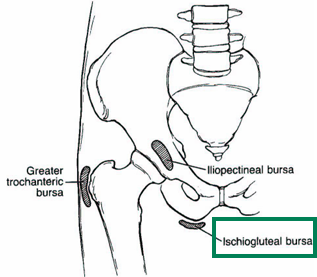
Match the sxs to the condition:
Prolonged sitting or direct blow to tuberosity
Agg: Sitting, direct palpation, HS stretch
Ischiogluteal Bursitis “Weaver’s Bottom”
What are some important treatment considerations for Myositis Ossificans?
Remove source of irritation to bursa
Activity Modification
Avoid lying on affected side (trochanteric bursitis)
Pillow between knees
Treat relevant impairment (Strengthening, mobility, etc.)
Modalities for inflammation
NSAIDS, local injections
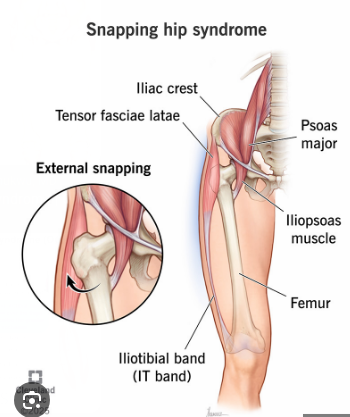
Match the sxs to the condition:
“Snapping” or clicking w/ repetitive movement
Clicking is the primary complaint
Evaluate the structure involved
Snapping Hip Syndrome
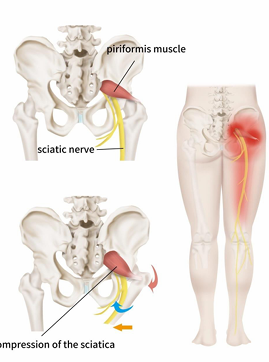
Match the sxs to the condition:
Buttock pain can radiate to the posterior thigh, calf
Sharp, burning, unilateral pain and paresthesia of LE
AGG: Walking (swing to heel strike)
Ascend stairs
Hip IR & ADD
Sitting on a firm surface
TTP at sciatic notch/piriformis
Piriformis Syndrome (sciatic nerve) - rritation of sciatic nerve between piriformis/ischial tuberosity
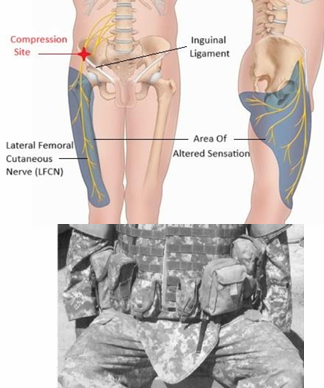
Match the sxs to the condition:
Irritation of lateral femoral cutaneous nerve next to ASIS
Paresthesia in antero-lateral thigh
Cutaneous distribution anterolateral thigh (no motor innervation)
Caused by compression: tool belts, obesity, pregnancy
Lateral Femoral Cutaneous Nerve (Meralgia Paresthetica)
T/F: Hip labral pathology and FAI could be asymptomatic
True, especially in people
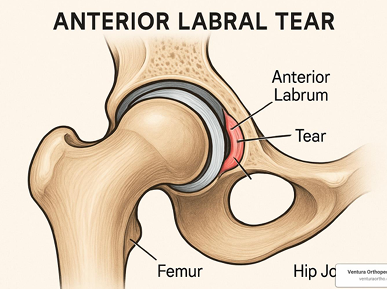
Match the sxs to the condition:
Catching/clicking w/ pain in hip
Groin pain, flexed/IR/ADD
ROM restrictions
Confirm with MRA and diagnostic injection
Insidious onset or traumatic
Labral Pathology
Match the sxs to the condition:
Anterior/groin pain (C-Sign) with prolonged sitting, walking, squat
May have clicking/popping
Pain with Flex, IR, ADD, may have bony endfeel
Femoroacetabular Impingement Syndrome (FAI)

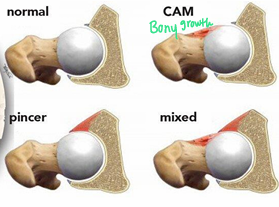
What are the differences between FAI pincer and cam deformities?
Cam Deformity:
Bony growth at the femoral head/neck junction
Repetitive stress/contact of the head/acetabular rim
Developmental condition
Pincer Deformity:
Overcoverage of the acetabulum
The acetabular rim impinges on the femoral neck
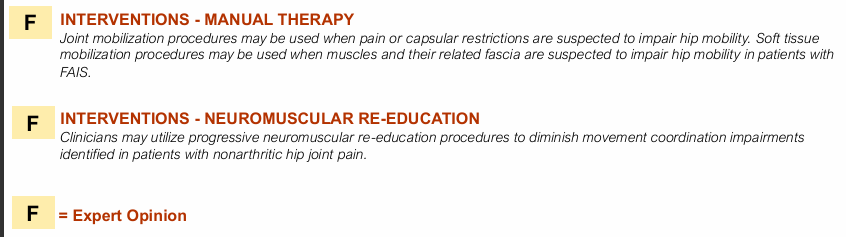
What TWO interventions are classified as “F” for nonarthitic hip pain in the 2023 CPG?
Manual therapy
Neuromuscular re-education
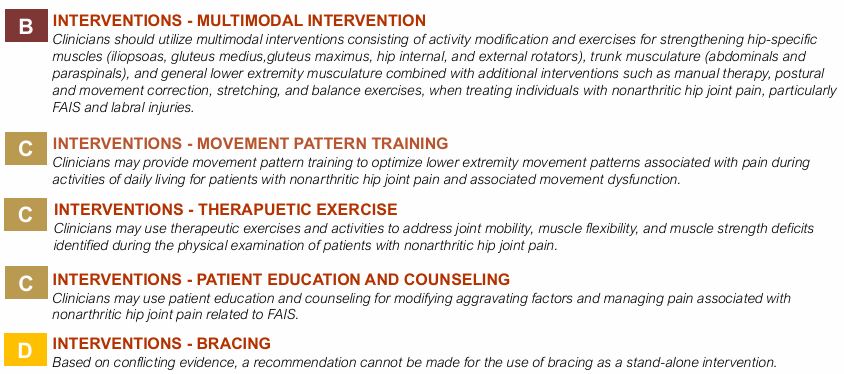
According to the 2023 CPG, what is the BEST intervention for NonArthritic Hip Pain?
Multimodal interventions
Clinicians should utilize multimodal interventions consisting of activity modification and exercises for strengthening hip-specific muscles (iliopsoas, gluteus medius,gluteus maximus, hip internal, and external rotators), trunk musculature (abdominals and paraspinals), and general lower extremity musculature combined with additional interventions such as manual therapy, postural and movement correction, stretching, and balance exercises, when treating individuals with nonarthritic hip joint pain, particularly FAIS and labral injuries.
Match the sxs to the condition:
Insidious onset anterior hip/groin pain, stiffness
More common > 50 y/o
AM stiffness < 60 minutes
Pain with WB, end of day, cold weather
Improves with rest
May refer to knee (rarely below)
Capsular pattern ROM limitation (flex < 115°, IR < 15°)
Hypomobile accessory motion(s)
(+) FABER, (+) Scour
Hip Osteoarthritis
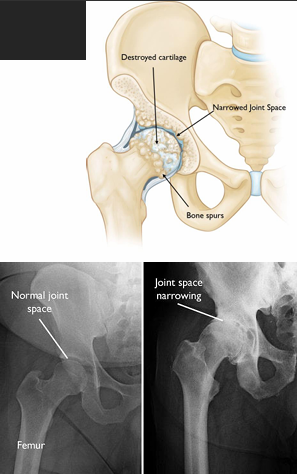
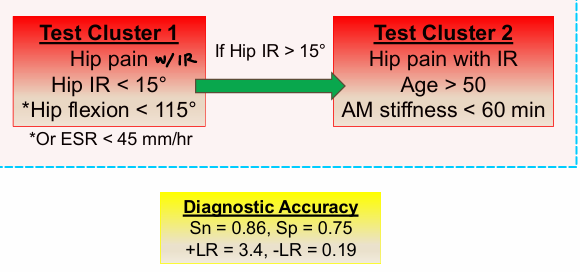
What is the Altman’s criteria for hip OA diagnosis?
Test Cluster 1
Hip pain with IR
Hip IR < 15°
Hip flexion < 115°
If hip IR >15°…
Test Cluster 2
Hip pain with IR
Age > 50
AM stiffness < 60 min
According to the 2017 CPG for hip OA, what are the BEST interventions to use (“A”)?
Manual therapy
Flexibility, strengthening, and endurance exercises
Class B: Patient education, modalities
Match the sxs to the condition:
Anterior hip/groin pain
Possible referral to thigh/knee
Vague, deep, dull, aching pain
Intermittent progresses to constant pain
AGG: WB Activity
EASE: Rest, NWB
24 Hr: Better in AM, worse with activity (WB)
Antalgic gait
Pain at higher ROM
Possibly TTP deep anterior hip
Femoral Neck Bone Stress Injury (BSI)

Which type of BSI is worse? Tensile or compressive?
Tensile! High risk in anterior tibial cortex → NWB does not fully decrease the tensile forces, so they need surgery!
What is the gold stander to diagnose a femoral neck BSI? Why?
MRI = gold standard (high Sn/Sp)
Radiographs high false negative
Healing not visible until ~14-21 days
Match the sxs to the condition:
Groin pain
Same hx as Femoral Neck/other BSIs
TTP pubic ramus
Pain with adductor stretch & resisted ADD
Pubic ramus BSI

Match the sxs to the condition:
Deep anterior thigh pain
Same Hx as Femoral Neck/other BSIs
(+) fulcrum test
Femoral Shaft BSI
Match the sxs to the condition:
Pain in pubic symphysis region, lower abdominal/groin
Post op, pregnancy/delivery
Athletes, especially kicking sports, hockey
Clicking/popping
TTP
Painful/weak ADDs/Abdominals
AGG: Running, SL pivoting, kicking, stairs, compression of pelvis
Osteitis Pubis