Looks like no one added any tags here yet for you.
Review mechanisms for regulation of vascular tone
GPCRs: beta- adrenergic receptors coupled with adenylyl cyclase that converts ATP to cAMP (adenosine monophosphate) once activated by a ligand. INCREASE in cAMP > activates PKA (protein kinase A) > activates calcium channel that enhances release of calcium > calcium + calmodulin complex formation
CARDIAC MYOCYTES, beta-1 receptors
calcium + calmodulin > phosphorylates MLC
with phospate = inactive = vasodilation
without phosphate = active = contraction
SMOOTH MUSCLES, beta-2 receptors
Calcium + calmodulin activates MLC-kinase (enzyme) to add phosphate so results in contraction of smooth muscles.
MLC with phosphate = active = SM contraction
MLC without phosphate = inactive/less myosin cross-bridges = vasodilation
caused by INCREASE IN cAMP > activated PKA leads to inhibitition of MLCK > no phosphorylation > vasodilation
target for beta blockers —> want to increase cAMP
nitric oxide:
activates guanylyl cyclase > deactivate myosin
Explain Mechanism of action of ACE inhibitors (-prils)
ACE-i targets at: RAAS, specifically the inhibiting the ACE enzyme from converting angiotensin 1 to angiotensin 2 (the active form)
effects ACE-i: decrease in vasoconstriction, decrease in aldosterone secretion = less water and sodium retention
also inhibits the degradation of BRADYKININ > activates the prostaglandins and nitric oxide > vasodilation
ARBs target at:
clinical uses of ACE-i
hypertension
cardiac failure
following myocardial infarction - reduces its workload
renal insufficiency - reduces the aldoesterone and retention, helps the kidney!
adverse effects of ACE-i
severe hypotension
acute renal failure
hypokalemia
angioedema and dry cough (more of bradykinin and substance P will induce inflammation-like responses including vasodilation and plasma extravasation —> angioedema. also idiosyncratic action that contributes to dry cough)
contraindication: pregnancy
Explain MoA of beta blockers and the difference between specific and non-specific beta blockers
targets at:
cardiac myocytes: inhibits the beta 1 receptors to reduce adenylyl cyclase action (reduces cAMP formation and ultimately reduces contractility = lower heart rate)
specific vs non specific: specific will only target the beta 1 receptors, will have less off-target effects but selectivity can be lost at higher doses
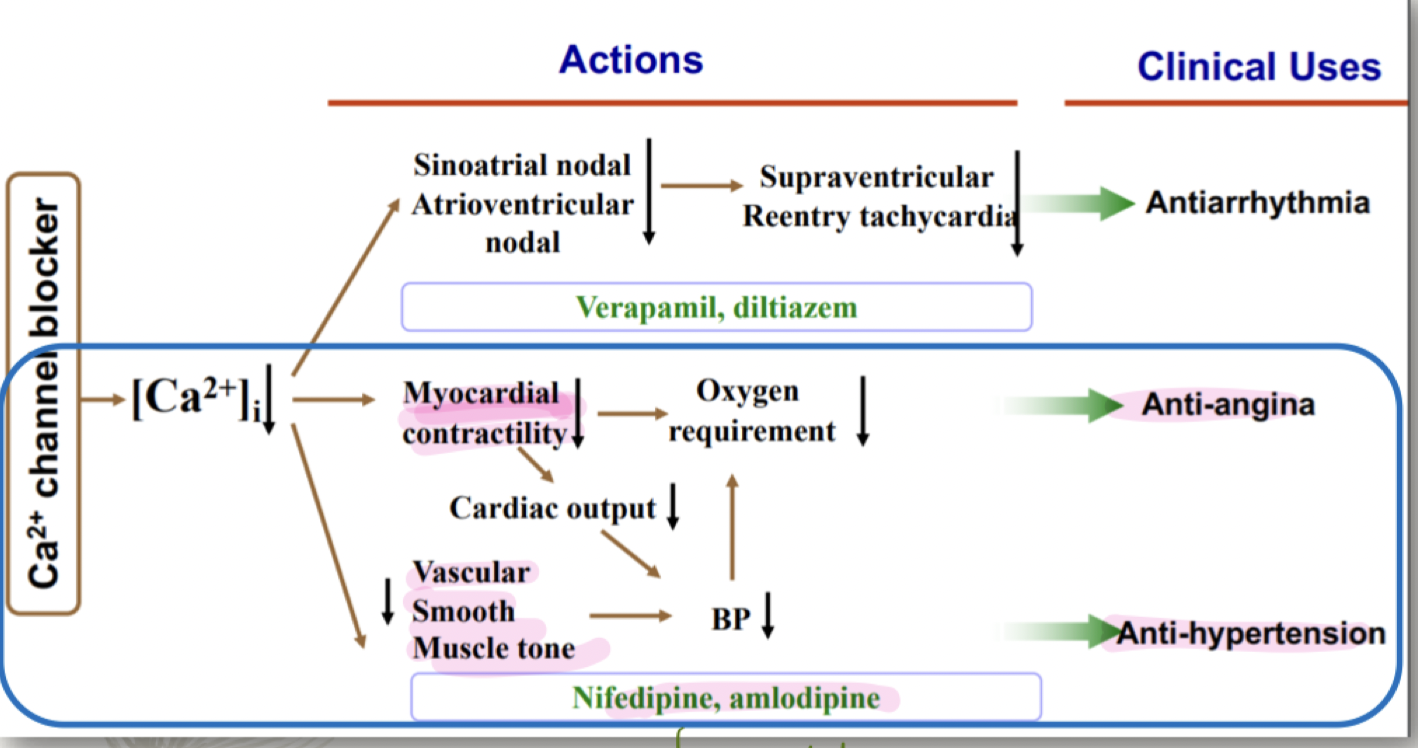
Explain MoA of calcium channel blockers
targets at: the calcium channel, prevents binding of calcium to calmodulin
prevents less calcium influx > prevention of calcium + calmodulin complex > inactivates MLCK > decrease contraction of smooth muscles > decrease BP > ANTI-HYPERTENSION
less calcium influx > decrease in myocardial contractility > decrease in cardiac output and oxygen requirement > ANTI-ANGINA
in the myocardial cell calcium is stored in the sarcoplasmic reticulum which plays a role in the actin myosin complex?
Explain MoA of thiazides
inhibit the reabsorption of NaCl back into the body by blocking the NaCl transporter > HIGHER salt content in urine > LESS water reabsorption in the collecting duct and more water peed out > REDUCTION in blood volume
also enhances calcium reabsorption in the DCT via apical calcium channel and basolateral Na/Ca exchanger
can be dependent on renal PGs synthesis
can you explain the 3 types of diuretics and their targets for anti hypertension
loop diuretics (works at ascending limb e.g. furosemide, bumetanide)
e.g. hydrochlorothiazide and indapamide
thiazides: works at the distal convoluted tubule, inhibit the transporter
potassium sparing diuretics: works at the end of the DCT and collecting duct, inhibits sodium reabsorption
factors influencing blood pressure
arterial blood pressure = cardiac output x peripheral resistance
cardiac output affected by heart rate, contractility and filling pressure
filling pressure determined by blood volume (how much blood that goes into the ventricle also determines the force of contraction, ventricular muscles stretch out more) and venous tone (affects preload!!! higher venous tone = a lot of contraction to push blood back to the heart because blood goes from higher to lower pressure)
peripheral resistance (associated with afterload which is the force against which that the heart has to pump to contract to eject blood. Arteriolar tone: high tone = low diameter, contraction)
rapid mechanism for controlling a decrease in BP
body senses a drop in BP therefore want to increase CO. increase in sympathetic activity mediated by adrenergic system - neurotransmitter noepinephrine/adrenaline.
in the heart: binds to beta 1 adrenergic receptors in cardiac myocytes = increase in cardiac output by increase in contraction
in the smooth muscles (want to increase peripheral resistance so that there would be more blood outflow to the critical organs): binding to ALPHA 1 adrenergic receptors = vasoconstriction = increase peripheral resistance
long term mechanism for controlling BP/ Review the renin-angiotensin aldosterone system (RAAS)
through the RAAS : one of the first organs to detect drop in BP is kidneys.
= decrease in GFR + kidneys secrete renin in response
increase in renin = converts the now activated angiotensinogen to angiotensinogen 1 which is then converted to angiotensinogen 2 = vasoconstriction and increase in aldosterone secreted by ADRENAL GLAND = increase in sodium retention = water retention = increase in blood volume = increase in BP
decrease in GFR = increase in sodium retention = water retention = increase in blood volume = increase in BP
mechanism of ARBs (-sartan)
blocks the angiotensin 2 AT1 receptor itself, preventing angiotensin 2 from sending down signals to receptors and exerting its effect
because of the MoA, there is less/no dry cough
contraindication = pregnancy
give examples of beta blockers
specific: atenolol, bisoprolol, metoprolol (A-M except carvedilol and labetalol)
non-specific: propranalol, pindolol, carvedilol (N-Z)
mixed: nebivolol (includes vasodilation via higher NO release) - beta 1 selective in LOW doses
bolded ones can be used for heart failure
clinical uses of beta blockers
hypertension (heart can relax)
cardiac failure
following myocardial infarction
abnormal heart rhythm
anxiety disorders (blocks adrenaline from binding)
adverse effects of beta blockers
hypotension
bradycardia
AV nodal block (when anti-arrythmia works too well)
reduced exercise capacity
relative contraindication: bronchoconstriction (esp. asthmatics)
for nonspecific blockers, might be blocking the beta 2 receptors at the lungs. since cAMP is blocked, MLCK not activated —> more likely to trigger bronchoconstriction , can’t be dilated so astha is more easily triggered
CNS: vivid dreams, clinical depression
clinical uses for calcium channel blockers
hypertension
stable angina (Amplodipine)
myocardial infarction and stroke prevention (amplodipine)
explain the two types of calcium channel blockers
Dihydropyridines (DHPs): act on peripheral blood vessels for vasodilation, less effect on the heart. Examples include amlodipine and nifedipine.
good for anti-angina and anti-hypertention
Non-dihydropyridines (non-DHPs): more effective in heart function, . They slow down the heart rate and are used to treat arrhythmias. Examples include verapamil and diltiazem.
reduce SA nodal conduction - good for atrial filibration
adverse effects of CCB
Hypotension
Heart failure
Myocardial infarction
adverse effects of thiazides
HYPOkalemic metabolic aklalosis
hyperuricemia
hyperglycemia (contraindicated with DIABETIC patinets?_
hyperlimidemia (???)
hypercalcemia (can be used to treat, but might also cause)
HYPOnatremia (because less sodium being absorbed)
clinical uses of thiazides
hypertension
congestive heart failure
nephrolithiasis due to idiopathic hypercalciuria (enhance the reabsorption of calcium to reduce formation of minerals and stones in kidney)
nephrogenic diabetes insipidus
what are some second line anti-hypertensives?
potassium sparing diuretics / mineralcorticoid receptor agonists, alpha-blockers and hydralazine