proto 1
1/23
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
24 Terms
1. Trypanosmosis in humans
phy EUGLENOZOA →
family rtypanosomatida →
class KINETOPLASTEA →
TRYPANOSOMATIDA (Trypanosoma, Leishmania)
-
Human African Trypanosomes
Sleeping sickness
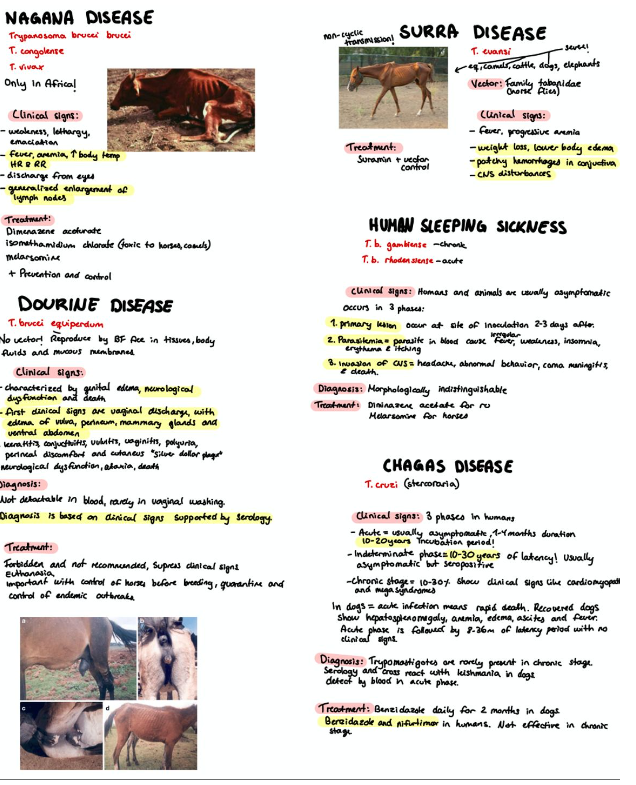
T. brucei rhodesiense – Acute - Asymptomatic animals, -important reservoir hosts.
First symptom - few months or weeks. Develops rapidly and invades the CNS.
T. brucei gambiense – Chronic - Infected for months + years no major symptoms. Already advanced stage when CNS is affected.
FH: Humans, cattle, pig, carnivores. Zoonotic!
Location: Extracellular, in plasma, lymph, cerebral fluid and organs of respiratory system.
Vector: Tsetse fly (Glossina spp). Cyclic transmission
Life cycle:
Pathogenesis and clinical signs: 3 phases:
Primary lesion: Site of inoculation 2-3 days after bite -> raised cutaneous inflammatory swelling. - pentamidin gamb — suramin rhon
Parasitemia: parasite in bloodstream produce irregular fever, insomnia, erythema and itching. enlarged lymph - nifortimox gamb — melasoprom rhon
Invasion of CNS: headaches, abnormal behaviour, meningitis - ensephalitis, coma, death.
Diagnosis: cannot distinguish the 2. Giemsa staining of blood, lymph, bone marrow or cerebrospinal fluid.
HCT – hematocrit centrifugation technique.
Treatment: ru: Diminazene acetutate – therapy. Isometamidium – prophylaxy.
Long lasting efficacy 2-6 months. Camels, horses, dogs: Melarsormine (diminazene is toxic)
Control and prevention: Control of the principal reservoirs of infection – livestock (cattle) and wild (antelopes). Reduce of vectors – destruction of the flies’ habitats or use insecticides (can cause ecological changes), fly traps, male flies sterilized in laboratory.
STERCORARIA
American trypanosomes
Chagas disease
T. cruzi
FH: Human, car, rodents, opossum and amardillo are reservoirs. Zoonotic! infect 150 species.
Vector: Triatoma (kissing bug, blood-sucking), rhodnius + panstrongylus genus.
Location:
Extracellular trypomastigotes are found in blood.
Intracellular amastigotes are found in tissue.
Epimastigotes in the intestine of vector.
Metacyclic trypomastigotes in rectum of vector.
Life cycle:
Pathogenesis and clinical signs:
3 phases of disease:
Acute phase: Most asymptomatic (children most likely to be symptomatic)
Humans may have edema in eyelids, lymphoid swelling, inflammatory nodule at biting site
Indeterminate phase: 10-30 years of latency. Relatively asymptomatic
no detectable parasitemia. Seropositive.
Chronic phase: 10-30% of infected exhibit cardiomyopathy or megasyndromes, like visceromegaly (enlargement of internal organs, dilation of esophagus -> food regurgitation, megacolon).
Damage and loss of neurons -> heart stress -> magnification of the heart -> degenerati
Damage and loss of neurons -> heart stress -> magnification of the heart -> degeneration -> forming granuloms and fibrous bearings -> depletion of myocard -> failure of heart -> death.
Ro-magna sign – oedema of the eyelids
Chagoma – oedema of the satelit lymph node – local reproduction of the parasite
Dogs up to 1 year: Acute infection is death.
Surviving dogs: hepato-splenomegaly, anemia, edema, ascites, respiratory symptoms and fever
Acute phase is followed by (laten) 8-36 months no clinical signs. Progressive clinical form show myocarditis and destruction of ganglia cells.
Diagnosis:
Dogs:
acute - thin and thick blood smear, concentration techniques.
chronic- no trypomastigotes or rarely. Alternative methods are PCR and ELISA, BUT can cause cross reaction with Leishmania in dogs!
Humans:
Acute, detect by blood.
Chronic, detect by serological test.
Treatment: Chemotherapy in Dogsis difficult.
Benzidazole daily for 2 months in acute cases, soften the clinical course but do not prevent subsequent chronic cardiac disease. Can be effective is treated earily in acute phase. Blood transfusion and vector control by insecticides may help.
In Humans, acute stage - benzidazole and nifurtimox, allopurinol and azole antifungal agents are just experimental. chronic stage - only symptoms
2. Trypanosmosis in animals
SALIVARIA
Animal African Trypanosomes
Nagana disease – chronic
T. congolense
T. vivax
T. brucei brucei
FH: Bo, Eq, Pig, Car, Camel (wild African game). Mainly affect cattle.
Vector: Tsetse fly (glossina spp). Cyclic transmission. Glossina flies are viviparous, lifespan 14 days.
Location: Blood vessels
Life cycle: Vector takes a blood meal from infected FH -> Ingestion of infective trypomastigote -> develops into Epimastigote and binary fission -> migrate salivary glands -> trypomastigote -> inject the parasite into the blood stream of FH -> multiplies by binary fission in blood, lymph and spinal fluid.
equi- paralysis facialis , edema in scrotum (ventral idema general)
Pathogenesis and clinical signs: weakness and lethargy → weight loss and anaemia
Increased body temperature, HR and BR.
Discharge from eyes.
enlargement of lymph nodes. - prescapular lymph in bo
eq- edema pre + paralys of facialis
Diarrhea may be present at initial stage. Disease occurs about 7-10 days after infection.→ death.
Diagnosis: Low haematocrit (decreased amount of RBC), leukopenia, thrombocytopenia.
Microscopic detection in blood, spinal fluid or lymph node aspiration -> Giemsa-stained smears.
Serology: ELISA. PCR.
Treatment: Diminazene aceturate, isometamidium chlorid (toxic for horses and camels), melarsomine.
some breeds of bo, -trypano-tolerance. eks: dama
T. brucei brucei is a natural parasite of wild Africa - non-infective to humans. Prevention is control of vector (insecticides) and permanent monitoring.
Surra disease – chronic
Surra and Dourine – are listed by WOAH
T. brucei evansi
FH: Eq, camel, dog, cattle and elephants
Vector: Tabanidae (horse fly), vampire bats.
Location: Extracellular
Epizootology: Non-cyclic transmission (no parasite development inside vector). Mainly transmitted by vector sucking blood and iatrogenic (reuse of needle).
BUT in dogs, ingestion of contaminated meat or blood.
Life cycle:
Pathogenesis and clinical signs:
Camels, dogs and horses - susceptible usually severely affected.
Fever, progressive anemia + weakness and weight loss, lower body edema, patchy haemorrhages in conjunctiva, vaginal mucosa etc. locomotor disturbances, CNS disorders (Paralysis, paresis).
Dogs: rapid acute course: Death within a week or month.
Diagnosis: Blood smears, lymph node aspiration. Haematocrit. ELISA, PCR.
Treatment: Suramin + vector control.
Dourine disease – chronic
T. brucei equiperdum
FH: Horse, equids
Location: free in mucous membrane, tissue, bloodstream and cerebrospinal fluid.
Vector: none!
Transmission: Sexual transmission by breeding.
Life cycle: Binary fission in various tissues.
Pathogenesis and clinical signs:
genital edema, neurological dysfunction and death.
First signs: vaginal discharge + edema of vulva, perineum and mammary gland and ventral abdomen.
Other: abortion, conjunctivitis, keratisis, vulvitis, vaginitis, polyuria,
Second stage 4-6 weeks - skin plaques . Muscular paralysis begins -nostrils and neck, extends to the pelvic limbs, and finally to all muscles;
Third/End-stage is manifested by severe nervous disturbances - hyperalgesia, especially to pressure on the withers. Paralysis of the cranial nerves, facialis.
from mare to foal is transmitted via mucous membranes such as conjunctivae. Mare's milk ialso infectious. Semen and vaginal excreta highest numbers of parasites.
Diagnosis: Usually undetectable in blood. Rarely in urethral/vaginal mucus washing or scraping. Clinical signs supported by serology: ELISA, IFA, CFT
Treatment and control: In many countries, treatment is forbidden and is not recommended because is can suppress clinical signs.
Melarsomine can be used. Examine horses before breeding, quarantine and euthanasia of horses with clinical symptoms. Control outbreaks, quarantine and eliminate infected equines.
3. Leishmaniosis (cutaneous, visceral, mucocutaneous).
Phylum: EUGLENOZOA
Class: KINETOPLASTEA
Order: - + Family: rypanosomatida
Genus: Trypanosoma, Leishmania
50 Leishmania species - humans 20 are zoonotic and morphologically indistinguishable. Their differentiation- host + vectors and molecular characteristics.
Main species:
Visceral: - liver, spleen, and bone marrow
L. donovani Dog, fox
L. infantum dog kid
Cutaneus: - skin at the site of a sandfly bite
L. tropica Rodents, dog
L. major Rodents, dog
L. aethiopica Rodents, dog
Mucocutaneus: - mucous membranes of the mouth and nose after spread from a nearby cutaneous lesion
L. Mexicana Rodents
L. brasiliensis Rodents
Routes of infection Vector bite Needle sharing Blood transfusion Transplacental Oral
Morphology: Ovoid organisms. Rod-shaped kinetoplast and a rudimentary flagellum.
Location: macrophages, reticuloendothelial cells in skin, liver, spleen, bone marrow, lymph nodes and mucosa, may also be found in leukocytes.
FH: Dogs, humans and rodents
Vector/IM: Sandflies of genus Phle-botomus in old world and Lut-zomyia in new world.
Epizootology: Cyclic transmission by vectors.
Life cycle:
Pathogenesis and clinical signs:
In dogs: 2 chategories suseptible + resistent
activation of Th2 cells -
high production non-specific Ab -
lack of cell-mediated immunity
Resistants
activation of Th1 cells
- low level of specific Ab
- efficient cell-mediated response genetic factors factors related to parasite
Diagnosis: Direct confirmation - amastigotes under microscopes from FNA of skin lesions and lymph nodes.
Serological:, IFAT, ELISA, western blotting, PCR.
Isolation in vitro or in vivo: This method is useful when the infection is low grade. In vitro cultures become positive after 5 – 30 days, in contrast to months for lesions to appear on an animal. M2
Cytology The samples are taken from the lymph nodes, spleen, skin impressions, bone marrow, or joint fluids stained with Giemsa stain or a quick commercial stain.
Intradermal test - Positive reaction: erythema
Treatment:
Most cutaneous - heal without treatment, will be immune to further infection.
Other forms - difficult to treat, long course and relapses.
Milteforan, + allopurinol. Therapy in dogs have negative side effects, high cost, long term and often relapses.
Supportive treatment and ATB'
no eradication canine leishmaniosis but control reduce.
Avoid bites - repellents and insecticides (spot on, collar, spray, solution), can be effective inside and around kennels, killing symptomatic and seropositive dogs but no symptomatic dogs are source of infection,
vaccination (CaniLeish) against leishmaniosis.
Visceral leishmaniosis (most severe form)
fever, weight loss, big spleen + liver.
Anemia, leukopenia and thrombocytopenia + hypoalbuminaemia
Lymphadenopathy may be present.
Symptoms months after sandfly bite. Because symptoms are non-specific and often start after redeployment there is usually a delay in diagnosis. Should be considered in any chronic fever patient returning from an endemic area (Mediterranean region).
post-kala-asar - after “good“ relapse
renal failure with proteinuria increased urination and drinking
Cutaneous form – most common
sores, papules and nodules on skin. + (starting in the head)
excessive growth of claws
looking somewhat like a volcano + raised edge and central crater.
Sores usually painless -painful if secondarily infected.
Swollen lymph npresent near the sores. ‘
sores within a few weeks - can appear months after. Skin sores heal on their own - can take months /years, can leave scars. L. tropica infections can spread to from upper lip to nose.
20% of dogs are resistant - reservoirs - source of infection Skin changes do not itch!
muscle atrophy. + massive hair loss; + dandruff
eratoconjunctivitis + uveitis + nose bleeds
can become mucocutaneus
Mucocutaneous
Sores usually painless -painful if secondarily infected - pneumonia septicemia- necrotic crust
Giardiosis and spironucleosis.
GIARDIA
Phylum: Meta-monoda
Order: Diplo-monidida
Family: Hexa-mitidae
Genus:Giardia,Spironucleus
Main species:
G. duodenalis – mammals (paired median bodies, lie transversally). Divided into 8 genotypes.
G. enterica
G. canis - cati
G. bovis
G. simondi
G. agilis – ampibia, birds, reptiles
G. muris – rodents, birds, reptiles
Morphology:
Cysts: Oval 12-14 um. Each 2 trophozoites. 12 um in size.
Location: Small intestine
FH: Mammals, birds and reptiles. Zoonotic!
Epizootology: spring and autumn.
Life cycle: Direct – sometimes in acute cases trophozoits can also be found in feces. Cysts are infectious when passed in feces and person-to-person transmission is possible shortly after.
Pathogenesis and clinical signs: Opportunistic infection.
catarrhal gastroenteritis, especially in young
Infection causes severe intestinal disorders, diarrhoea and other symptoms include abdominal distension, nausea and weight loss.
Attachment of the trophozoite to the mucosal surface by means of the adhesive disc cause shortening of the villi of the small intestine, inflammation of the crypts and lamina propria, and lesions on the mucosal cells.
reduction secretion of small intestinal digestive enzymes.
human rarly fatal in developed countly
Clinical signs:
Acute giardiosis develops after incubation period of 5-6 days and lasts 1-3 weeks. CS: diarrhea, abdominal pain, bloating, nausea and vomiting.
Chronic giardiasis have recurrent symptoms and malabsorption and debilitation may occur.
Diagnosis: By recognition of trophozoites or cysts. Only cysts passed in feces but trophozoites may be found, flotation method and zinc sulphate solution (FAUST). 3 fecal exams should be performed in 5-7 days.
PCR can be used
Treatment: Fenbendazole or febantel (panacur), repeated application for at least 3 days. Prognosis is very good.
metronidazol
Post-treatment feces examination is essential. Cysts can survive in the environment for months.
SPIRONUCLEUS (Hexamita)
Main species:
Hexamita melagridis (turkey, quail, pheasant, duck).
H. columbae (pigeons)
H. muris (mice, rats, voles, hornet)
H. salmonis + truttae (fish)
Morphology: Trophozoites are binucleated + 8 flagella (6 anterior, 2 posterior), adhesive disk is absent.
Cysts have 8 nuclei. Longitudinal division
Location: in liberkuhn crypts of small intestine, cecum, fabrici stock, liver and abdominal cavity.
FH: mainly birds, turkey, quail, pheasant, duck but also some fish.
Epizootology: Way of transmission is ingestion of cysts.
Life cycle: Trophozoites undergo binary fission in intestine, cysts passed in feces. Forms oval 8-nuclei cyst. Same as giardia.
Pathogenesis and clinical signs:
characterized by duodenitis, enterititis
Signs nonspecific and include:
watery diarrhoea that may be yellowish later in the disease
dry, unkempt ruffled feathers
listlessness
rapid weight loss despite continuing to eat
Birds may die in coma or convulsions.
Bulbous dilatations of the small intestine
enteritis, dehydration,
Disease of young animals (e.g. turkeys at 10 weeks old) has 80% mortality.
Diagnosis: find trophozoites and cysts in droplets of intestinal contents after staining, for example with haematoxylin.
Post mortem examination, catarrhal inflammation of small intestine with a lot of spilled fluid.
Treatment: Not known. Can prevent by good hygiene, nutrition and separate breeding of young turkeys.
Cysts are the infective form
5. Histomonosis
Phylum: Metamonoda
Order: Tricho-monadide → genital or digestive tract + Hydrogenosomes in place of mitochondria
Family: Monoero-moadidae
Genus: Histomonas, Dientamoeba
Family: Trichomonadidae
genus: Trichomonas, Tritrichomonas, Pentatrichomonas
Main species: Histomonas melagridis “Black head disease”
Morphology: Morphology is similar to Trichomonas in the way that they have axostyl, nucleus and flagellum. But it posses different stages of development.
Laminal: in cecal lamina of birds, variable in shape, 1 flagella.
Transitional: tissue invasive – spheroid, no flagella, have pseudopodia
Spheroid resting stages – in Heterakis eggs, non-flaggelated, smaller.
Location: Cecum and liver
FH: Mainly turkeys. Occasionally chickens, guinea fowl.
Vector/IM: Heterakis gallinarum as paratenic host.
Epizootology: no cyst.
Indirect transmission – H. melagridis can survive in embryonated heterakis spp. eggs- 2 years in soil and in earthworms.
Direct – histomonas free tukeys and infected turkeys are in same cage, birds sit on fresh feces “cloacal drinking”
Life cycle:
Pathogenesis and clinical signs: high morbidity and mortality.
14 week old 100% mortality+ acute.
recover may have permanently scarred cecum and liver.
turkeys become apathic, ruffled feathers. Feces are sulphur-yellow in color.
Circulation disorders, cyanosis of the skin, comb, wattles and head.
Chickens more resistant can be asymptomatically infected, but severely as result of liver infection.
thickened mucosa→ necrotic, exudate→ solidify into hard, cheesy plugs
Diagnostics: Post mortem – cecum and liver has necrotic lesions, must differentiate from other -confirmed by histological examination.
PCR
cultures.
Treatment: No specific antihistomonal drugs
can Paromomycin, alternative ATB.
Turkeys separate from chicken. Hygiene. Cecal worm control is necessary to reduce blackhead incidence.
6. Bovine and avian trichomonosis
Phylum: PARABASALA
Order: Tricho-monadida
Family: Tricho-monadidae
Genus: Tritrichomas, Trichomonas, Pentatrichomonas
Main species:
Tritrichomonas foetus B
T. gallinae
T. foetus C (cats)
Morphology.
Hydrogenosomes instead of mitochondria
anaerobic + Oppertunistic .
Bovine – 3 anterior free flagella and 1 posterior
Avian – 4 anterior flagella
Some species T. foetus and T. muris- form pseudocysts.
Location: Extracellular, parasites of genital or digestive tract of vertebrates.
FH: Highly species dependent.
Bovine trichomonosis
Tritrichomonas foetus B
Location: Reproductive tract
FH: Cattle.
Epizootology: Sexually transmitted, coitus, AI and gynaecological examinations. Bulls acts as reservoirs. OIE-listed disease.
Life cycle: Direct LC. No environmentally resistant stages.
trophozoites multi binary fission. Transmitted sexual -> multiply in vaginal mucosa -> migration cervix -> infect bull mating, trophozoites → preputal mucosa.
Can form pseudocyst.
Clinical signs:
Inflammation of genitals, early abortion (first 2-4 months), foetal death, uterine discharge, sterility, pyometra, endometeritis.
cow usually recovers and is immune post-partum.
Bulls asymptomatic,- inflammation of preputial sac, small nodules. Semen quality not affected. Bulls
older than 3-4 years spontaneous recovery but lifelong carriers.
younger than 3-4 years – transient infection (short time).
Diagnosis: Clinical history.
Stained smear from genital fluid, placenta fluid, contents of aborted fetus, uterine washing, pyometra discharge in case of abortion.
Number paras highest 14-18 days post infection
Can be seen in native preparations, stained smears, culture and PCR.
Treatment: WOAH-listed
No treatment. Artificial insemination free bulls, only symptomatic treatment.
Nitro-mi-dazoles, - Metro-ni-dazol; Dime-tri-dazol
not registered drug! Resistant to pencillins, streptomycin and other antibiotics. Prevntion, control of bull and AI instruments, clean urine and manure daily as they can survive there for multiple days. Biosecurity is important, workers can transfer.
vaccine (Trichguard).
Avian trichomonosis
Trichomonas. gallinae (most dangerous)
Tetratrichomonas gallinarum
Tetratrichomonas anatis
Location: In the cranial part of GIT (mouth, crop, proventriculus).
FH: Pigeons, birds. turkeys, domestic chickens are rare.
Epizootology: 80% asymptomatically
mother feeding offspring or drinking contaminated water from the beak cavity of infected birds, or birds of prey that ingest captured birds, or by contaminated drinking water.
Life cycle: Direct.
Pathogenesis and clinical signs:
Lesions yellow and necrotic in the beak, esophagus and crop of birds.
T. gallinae can fatal pigeons (2-4 weeks old), infection via regurgitated crop contents from adult birds. necrotic areas of liver, heart and navel rarely other organs. -„ yellow buttons
Recovered pigeons may remain asymptomatic but are reservoirs.
salivate excessively;
Emaciation, ruffled and dull;
Difficulty closing their beak, display repeated swallowing movements, exhibit open mouth and noisy breathing;
Have diarrhoea, + sufication
Acute phase: First lesions mouth, pharync, esophagus and crop.
inflammation and creamy-white, wet and sticky exudate.
lesions become small, well-defines raised yellow-white ulcers
Chronic phase: mucosal lesions become yellow, larger hard, caseous masses may invade sinuses extend→ beak and eyes, penetrate → brain and viscera causing necrotic areas in the liver, spleen, pancreas, heart, lungs and air sacs
Diagnosis: Crop swab -> direct smear on slide -> microscopy -> see moving protozoa.
dead, smears layer between normal and affected tissue or from exudate
Treatment: Nitroimidazol compunds, only for birds not used for food production, such as carrier pigeons.
Metronidazole, dimetridazole, ronidazole.
sanitation, prevention of contact between pigeons and other domestic wild birds.
cat - Ronidazole
7. Pathogenic and potential pathogenic Amoebae.
Phylum: Amoebozoa
Order: Enta-moebida Family: same
Genus: Entamoeba, Endolimax
Entamoeba histo-lytica (colon liver) – hum, car, pigs, rats
Naegleria spp. nasal cavity, olfactory nerves, meninges
Acanthamoeba spp. skin, respir. tract, urogenital, meninges
Balamuthia spp. subacute, chronic form (Acanthamoeba like)
moves around pseudopodia + feeds by phagocytosis.
are all heterogenous. Divided into parasitic and free-living. Many species forms cysts.
Entamoeba histolytica (pathogenic)
Trophozoites has 2 forms:
Forma minuta – small, non-pathogenic, chronic latent stage, forms cyst (4 nuclei, rod-shaped chromatin body)
Forma magna – larger, pathogenic, dysenteric stage and no cyst.
Location: Large intestine, colon (forma minuta), extraintestinal hapatitti abses + icter(forma magna)
FH: Dogs, cats, pigs, humans. Zoonotic!
Life cycle: Direct. Ingestion of cysts-> excyst in small intestine and the trophozoite enter colon where they multiply by binary fission ->
new cysts are released with feces. They will multiply in colon for months without causing harm, but may invade intestinal wall and cause disease (enter blood and liver, brain, lungs)
Pathogenesis and clinical signs: Most infections are asymptomatic.
ntestinal: Acute Dysenteric + Chronic Non-Dysenteric (“self-cured”)
Extra-Intestinal: Amoebic Liver + Pulmonary Abscess Other sites (brain, skin, GU, ?)
develop invasive disease (young adults) and produce small ulcers, colitis, perforation of intestine, acute, fatal amoebic dysentery, liver abscess.
Metastasis via bloodstream, ameba-free feces is common.
liver abscess — chocolate-colored pus, necrotic material, bacteria free.
Inflammatory thickening of intestinal wall around the abscess, can be confused with tumor. + can be seen brain
Pulmonary amebosis is rarely primary, usually secondary to rupture of liver abscess through abdomen. Symptoms are fever, cough, dyspnea, pain and vomiting.
Cutaneous amebosis is due to intestinal or hepatic fistula.
Diagnosis: feces for trophozoites or cysts.
Serological tests (IHA, ELISA). Cathterize abscess and aspirate, check for trophozoites and serologic testing of amebic antigens. E. histolytica phagocytize RBCs – blood cell count coulture.
Treatment: Nitroimidazoles, chloroxin, paromomycin.
Avoid fecal contamination + proper hygiene. Drinking water treated with 9 drops of 2% tincture of iodine. Cleaning of uncooked fruits and vegetables. Prevention of contamination of foods.
Naegleria fowleri - free living brain eating
mostly young immunocompetent
Morphology: Both trophozoite and cyst, but also flagellate form.
Trophozoite form can be present in human tissue (infective form), flagellate form -cerebrospinal fluid
Location: Nasal cavity, olfactory nerves, meninges
FH: Humans- warm waters 46°C. + freshwater.
Life cycle: Trophozoite nasal cavity → migrate via olfactory nerves to brain → brain eating amoeba → phagocytize RBCs and WBCs, destroys tissue. Trophozoite is infective stage, can turn into flagellated & cysts if conditions are poor. Trophozoite replicate by binary fission with the nuclear membrane intact, a process called promitosis
Pathogenesis and clinical signs: PAM (primary amoeboid meningoencephalitis), sore throat, intense headache, fever, vomiting, blocked nasal passage, coma in 3-4 days.
Diagnosis: biopsy, CT
Treatment: Disease if fatal. None are effective, few survives.
Acanthamoeba spp.
immunodeficient, weakened individuals
Morphology: trophozoite + cyst stage.
Location: brain and eye
FH: Humans
Epizootology: Enters through the skin, respiratory - urogenital track - bloodstream→ brain and meninges.
found in swimming pools, hot tubs and drinking water
Life cycle: Two stages, cysts (1) and trophozoites (2). trophozoites replicate by mitosis
trophozoites infective form, but both stages can enter the humans in various ways.
Pathogenesis and clinical signs: Incubation period: unknown,
infection through respiratory system → reach CNS.
GAE (granulomatous amoebic encephalitis) and keratitis (cornea).
Cutaneous papules, nodules, ulcers, sinusitis, cephalagia, meningeal signs, often infect ocular cornea, uveitis, blindness ect.
Diagnosis: By scraping sample of the eye. GAE is harder to diagnose, CT or biopsy.
Treatment:Can be difficult to treat. GAE is fatal.
8. Eimeriosis of cattle + SHEEP AND GOAT
Phylum: Alveolata
Subphylum: Apicomplexa
Class: Coccidea
Family: Eimeriidae
Genus: Eimeria
Apicomplex explain
Main species:
E. bovis - Located in endothelial cells of ileum, cecum and colon. Very pathogenic!
E. zuernii
E. auburnensis
Morphology:
Cysts:
Location: Intracellular, in intestines.
Life cycle: Monoxenous direct life cycle.
Exogenous Sporogony: The unsporulated oocyst is excreted into the feces -> sporulation happens outside host -> good condition -> sporulation -> form sporocyst with sporozoites inside.
Merogony: after intake of sporulated oocyst -> release of sporocyst -> travel to intestine -> sporozoites hatch from sporocyst -> invade epithelial cell (now known as trophozoite) -> multiply by binary fission -> produce merozoites -> multiply until cell ruptures -> release merozoit into blood stream or have multiple rounds of merogony that re-invade other cells and start new rounds of merogony. Gamonts in epithelial cells of large intestine.
B. bovis –
1st: gen endothelial cells of posterior half of SI.
2nd: gen epithelial cells in cecal and colonic epithelium.
Gamonts in epithelial cells of cecal and colonic glands.
B. zuerni – 1st: SI. 2: LI.
Gametogomy: Sexual reproduction. Merozoits→ gamonts through gametogony. Then a female macrogamete and a male microgamete undergo karyogamy -> diploid Zygote -> forms oocyst wall -> unsporulated oocyst are set free via feces.
Pathogenesis and clinical signs:
E. bovis
- Death withnin month
- Diarrhea, fever, congested muco-saedematous and hemorrhage
- Partial immunity following recovery
E. zuernii
- Bloody diarrhea!
- Death begin 7 days of onset of symptoms, may not be passing oocyst at this time.
damage to intestinal tract.
calves unthrifty and have fecal-stained perineal areas.
May develop fever, anorectic, depressed, dehydrated and lose weight.
Nervous signs and a high mortality rate, 80-90% are seen in some calves with acute clinical coccidiosis.
Diagnosis: Flotation method.
Treatment: Sulfa-quino-xaline, sulfa-methazine, amprolium for 5 days. Eimeria is self-limiting, spontaneously ending their life cycle within few weeks unless chronic conditions.
vacine - bovatec, monsinrumensin
-
SHEEP & GOAT
Sheep:
E intricata (bigger than the rest, easily identified)
E. ovina – cecum
E. ovinoidalis – colon
E. clandalis
E. granulosa
E. parva
Goat:
E. arloingi – intestinal crypts
E. ninakohlyakimovae – intestinal crypts
E. christenseni
Epidemiology: Lambs very susceptible. Eimeria host specific + not transmitted from sheep to goats.
, older sheep having become immune through previous contact with the parasite
Pathogenesis and clinical signs:
dirtiness around tail due to diarrhea. - Blood severe dehydration.
lose appetite, weak and unthrifty.
Some goats constipated + die acutely without diarrhea.
Eimeria destroys the epithelium of intestines, decrease their ability to absorbs food and cause dehydration, diarrhea, severe hemorrhage.
Diagnosis: fecal flotation methods and post mortem scrapings from the GIT. Because oocysts are prevalent in feces of sheep of all ages, coccidiosis cannot be diagnosed based on just findings of occyst.
Peack oocyst count of over 100 000/g of feces have been reported in 8-12 weeks old lambs that appeared healthy. Diarrhea with oocyst counts of pathogenic species of > 20 000/g is characteristic of coccidiosis in sheep.
Treatment and prevention: sulfamide for treatment, monensin as prevention.
Clean pens and good hygiene, do not mix different age groups.
9. Eimeriosis of rabbits and hares.
Rabbit
Main species:
E. intestinalis – Intestinal. Highly pathogenic!
E. magna
E. media
E. piriformis – Cecum
E. flavescens – Highly pathogenic! Cecum
E. stiedai – Located in liver
Location: intestine and liver
FH: rabbits
Life cycle: Same
Epizootology: Occur commonly during time of weaning and in high populations like rabbit farms.
Pathogenesis and clinical signs: Highly contagious,
enteritis, hepatitis and high young rabbit mortality.
Typically, infections with intestinal coccidosis are mild, and often no clinical signs. T
dehydrated, anorexic, diarrhea and large intestine is more commonly affected, may be hemorrhagic or edematous.
E. stiedai: Invade intestinal mucosa - enter blood vessel - transported to liver - bile ducts. Cause hepatic infection, icterus, edematous enlargement and blockage of bile duct. Small white nodules can be found on the liver parenchyma. Hepatomegaly may be seen.
Diagnosis: Oocyst in feces or by post mortem.
Treatment: Diclazuril, Monensin, Toltrazuril, Sulphonamids. Good hygiene.
Hare
Main species:
E. townsendi
E. leporis
Clinical manifestation in wild hares are rare, but may occur in wet season in young hares.
10. Chicken eimeriosis. (poultry)

acervulina - small
maxima, - largst
tenella appear to be most prevalent;
mitis smallest

Location: Intestines
Epizootology: placed in high concentrations on small areas, most frequently young.
Life cycle: Same as in cattle. 3 generations of merozoites.
Pathogenesis and clinical signs: Characterized by decreased growth,
catarrhal-hemorrhagic enteric diseae, formation of nodules, diarrhoea,
CNS disorders and anaemia.
Diagnosis:
intra vitam -coprological examination, flotation method to find oocysts.
Post-mortem, look for scratches of the epithelial layers of the intestine, histological sections. Can de differentiated based on where in the intestine they cause damage.
Treatment: Anticoccidal - amprolium, sulphonamides, inophores or toltrazuril.
Antibiotics – tylosin or amoxicillin.
Supportive care.
Environmental/management changes – slow down oocyst sporulation by removal of the feces and soiled bedding, ensuring it is kept dry. Can also be
vaccinated (livacox).
TURKEY
3 important between 3 and 10 weeks of age.
meleagrimitis - upper and middle intestine
adenoeides
gallopavonis - multiplies in the caecal pouches
GEESE
danilovi Ducks / ileum 8-day pre-patented period highly pathogenic
Perniciosa (ileum)
E. anseris (ileum)
E. nocens (ileum)
E. parvula (ileum)
E. truncata (kidney)
11. Eimeriosis and cystoisosporosis (isosporosis) of pig.
Main species:
E. debliecki
E. scabra
E. neodebliecki
E. spinosa
E. poliata
E. suis
Location: Small intestine
Life cycle: Same
Pathogenesis and clinical signs: Typically affect piglets.
acute enteritis limited to lower small intestine, loss of condition, perianal staining.
Characteristic yellow fibronecrotic pseudomembrane often accompanied by bloody diarrhea.
Diagnosis: Fecal floation.
Treatment: Anticoccidials.
Pig cystoisosporosis/isosporosis – Cystoisospora suis
Morphology: Oocyst with 2 sporocysts with 4 sporozoites each (8 in total). Small, oval, 2 thin shell, unsporulated, transparent. No stieda body.
Location: small intestine
FH: Pigs, commonly piglets
Epizootology: Fecal-oral route. Short development cycle of C. suis and high susceptibility in young!.
Life cycle: Occur in mucosa of small intestine in piglets. Heteroxenous! Can also be monoxenous.
Sporogony phase – sporulate rapidly in temp 20 – 40 degrees in the environment. Once the oocyst is sporulated it is very resistant to most disinfectants. Can have paratenic host (rodent). 16 h (1-3 days in Eimeria).
Merogony – oocyst is ingested and release the sporozoites. They penetrate the villous epithelium -> merogony. 3 generations.
Gamogony – gametocytes -> Gametogony -> oocyst is released to the lumen of the intestine and shed with feces to the environment.
Pathology and clinical signs: cells of intestinal epithelium destroyed due → merozoites.
villous atrophy and fusion, necrotic enteritis, enterocyte metaplasia, crypt hyperplasia and lesions.
Lesions→ secondary pathogens (enterotoxins)
Digestive function impaired longer that clinical disease → time for villi to grow back t
Piglets have pasty to watery diarrhea, yellow-gray in color, perineal staining, weight loss, blood never present. Adults are asymptomatic.
can also be seen respirtory
Diagnosis: Direct examination of fecal smear, Mc master counting chamber. Since developmental cycle is so short, the piglets may already be dead before clinical signs occur. Therefore necropsy is a better determination .
Treatment:Coccidiosis in piglets unresponsive to antibiotics.
Toltrazuril 5% suspension (against neonatal),Ponazuril, Diclazuril, Sulphidamidine.
Hygiene measures
Single oral treatment with Baycox in the first week after birth is necessary.
ecoli-corona diferentiation
12. Cystoisporosis of carnivores.
Phylum: Alveolata
Subphylum: Apicomplexa
Class: Coccidea
Order: Eimeridae
Genus: Cystoisospora
Main species:
Dog:
C. canis (36um)
C. ohioensis (24um)
C. burrowsi
C. neorivolta
Cat:
C. felis
C. revolta – Larger oocyst than felis.
Morphology: Sporulation dependent -humidity, temperature and oxygen. Once the oocysts are sporulated, they are resistant to disinfectives.
Location: epithelium of small intestine
FH: Dog, Cat. (Not found in horses, ruminants and domestic poultry)
Vector/IM: Rodents as paratenic host.
Epizootology: fecal oral route, ingestion of cyst. Occur in combination with Eimeria canis, feline and cati.
Life cycle: Heteroxenous or monoxenous!
Sporogony (exogenous) – unsporulated oocysts are shed in feces of final host and sporulates in the environment. The sporulated oocyst is ingested by a final host and will excyst in the small intestine, releasing 4 sporozoits that invade the epithelial cells. Sporozoits are able leave intestine and form hypnozoite in paratenic host.
Merogony – in epithelial cells, they become merozoits and reproduce by binary fission. The epithelial cells rupture and release merozoits which infects new cells.
Gametogony – merozoits can become macrogametes and microgametes which penetrate and fuse to form a zygote -> usporulated oocyst shed in feces (infective stage).
IM/paratenic host – can invade rodents, and produce a single dormant cyst without causing any harm – hypnozoite. But final host can eat rodent and become infected.
Pathogenesis and clinical signs:
Weak-moderate inf - usually asymptomatic in young & old.
Heavy inf: (C. canis) clinical disease in puppies (3-4 weeks) -> Bloody diarrhea, vomiting, anorexia, apathy, impaired growth, abdominal pain, sometimes fever, haemorrhagic enteritis, anemia, polyuria, dehydration. ‘
May seem like parvovirus.
Diagnosis: Coproscopy detection of unsporulated oocyst.
Flotation method with FAUST.
Treatment: Sulfa-dimethoxine, amprollium, toltrazol, didazuril, ponazuril. Hygienic measures, remove feces, disinfection of breeding areas, not feed with raw meat.
13. Cryptosporidiosis of mammals and birds.
Phylum: Alveolata
Subphylum: Apicomplexa
Class: Coccidea
Order: Cryptosporidae
Family: Cryptospoididae
Genus: Cryptosporidium
Main species: zoonotic
Mammals: total of 18 species.
C. hominis – Humans
C. parvum – Ruminants, human, rodent
C. bovis – cattle, sheep
C. andersoni – Ruminants (located in abomasum)
C. suis – pig
C. canis / felis
C. muris – mice, birds
Birds: 3 species
C. baileyi – chicken (located in respiratory tract, intestine, bursa fabricii)
C. galli – chicken (located in stomach)
C. meleagridis – turkey (located in intestine, also other organs)
Morphology: Within the genus we distinguish two morphologically different groups:
smaller oocysts and affinity for intestinal eneterocytes:
- C. parvum- canis- hominis- bovis- suis
larger oocyst, stomach glands
- C. muris -galli
have no host specificity and no sporocyst.
smaller than Eimeria
Location: Invade and replicate microvillous region (brush border) of epithelial cells, lining the digestive and respiratory organs.
FH: Mammals and birds
Epizootology: C. parvum, C. hominis (Zoonotic!) dangerous for immunosuppressed humans. C. parvum also for healthy people.
Life cycle: Similar to intestinal coccidia, but differs somewhat from other monoxenous coccidia.
Monoxenous life cycle – all 3 phases are endogenous
Endogenous sporogony – oocyst undergo sporulation while they are still within the host cells and are only infective when they are released in the feces. A thick walled (sporulated) oocyst or a thin walled (causes autoinfection, infects host again) are shed with the feces. The thick walled oocyst is ingested or inhaled, excystation occurs in the microvilli of the intestines of the vertebrate host. 4 sporozoites are released.
Special tissue localization: microvilli of the digestive tract (intestine and gastric wall), respiratory tract. The development takes place in the parasite-form vacuole resulting from inversion of zoit after invasion by host cell excicison called “intracellular extracytoplasmic” localization.
Endogenous merogony – sporozoites become merozoits, which will asexually reproduce by binary fission for 2 generations.
Endogenous gametogony – merozoites form macrogamont (female) and microgamonts (male) which form a zygote. The zygote -> oocyst.
Pathogenesis and clinical signs:
Hypertrophy of crypt cells, abbreviation of villuses, inflammation of lamina propria mucosae.
Cause secretion of water by cells →diarrhea without participation of enterotoxin.
Neonatals has profuse diarrhea and complete destruction of microvilli of intestine, light-yellow feces, anorexia, dehydration, acidosis, fever, apathy, weakness, frequent defecation, malodorus, watery feces with fibrin and mucous.
human → young immunodis
bird
. baileyi - Bursa of Fabricius, conjunctiva, kidneys, respiratory tract, cloaca, rectum
Diagnosis: No fecal flotation method - too small, stain instead, appear pink/red-ish. Stained by Ziehl-Nielsa stain or Kinyoun (pink on blue background),
ELISA, PCR.
Birds – scarping of trachea.
Treatment: Halofuginone for calves,
Nitazoxanid, azithromycin, pyrvinium pamoate for dogs and cats.
Symptomatic treatment is IV fluids, electrolytes and good nutrition.
There is no drug to cure cryptosporidiosis, healthy individuals will heal without treatment. Prevention is highly important! Adequate sanitation and hand washing. If local outbreak, boil drinking water, eat only cooked foods, avoid unpastureized milk and juice.
14. Neosporosis
Phylum: Alveolata
Subphylum: Apicomplexa
Class: Coccidea
Order: Eimeridae
Family: Sarcocystidae
Genus: Neospora
Bovine neosporosis – caused by Neospora caninum
-
Main species: Neospora caninum
Morphology: oocyst with 2 sporocysts with 4 sporozoites each.
Location: Multiply in the intestine enterocytes. Forms cysts in muscle tissue and neural tissue.
FH: dog, coyotes, wolves
IM: ruminants, horses. Mainly cattle.
Epizootology: Fecal-oral route and Transplacental infection in dogs and cattle.
Life cycle: Indirect. Life cycle similar T. gondii but in dogs.
IH (Cattle) – becomes infected by ingestion of sporulated oocysts or by transplacental transmission. The sporozoites invade intestinal transform to tachyzoites and can reach various organs like muscle tissue and become bradyzoites.
FH – dog can ingest muscle tissue cyst and become infected. The bradyzoites are released in the small intestine where they will multiply by merogony and gametogony forms an unsporulated cyst which is passed in feces and sporulate in environment.
horizontal and verical trans
Pathogenesis and clinical signs:
- Adult cow: Abortion is the only sign in adults. Fetus can be absorbed, mummified, autolyzed, stillborn or clinically normal but chronically infected.
Calves: visible younger than 2 months.
Limbs flexed or hyper-extended, ataxia, decreased patellar reflexes,
exophthalmia or asymmetrical appearance of eyes
underweight, unable to rise and with neurologic signs
Dogs: Paresis and paralysis of hind limbs, rigid muscle contraction, muscle atrophy, nerve and cardiac deficits,
skin ulceration due to infection in other organs systems. Can also induce abortion.
prenatal infection – young dogs – focal necroses – brain, spinal cord and nerves;
Diagnosis: Serology Immunohistochemistry PCR Histopathology - fetus - clinical
Treatment: Sulfonamides, pyrimethamine and clindamycin, toltrazuril:
No drug effective against tissue cysts + vertical transmission
Cattle: No drugs or treatment. Prevent contamination of farm animal feed by dog feces. Prevent contact with aborted material.
15. Sarcocystosis of mammals, characteristic, life cycle, species of animals
Phylum: Alveolata
Subphylum: Apicomplexa
Class: Coccidea
Order: Eimeridae
Family: Sacrocystidea
Genus: Sacrocystis
Main species:
Sarcocystis bovihominis
S. bovicanis (S. cruzi)
S. bovifelis (S. hirsuta)
S. suihominis
S. suicanis (S. miescheriana)
S. Suifelis (S. porcifelis)
S. ovicanis (S. tenella)
S. ovifelis (S. gigantica)
S. capracanis
S. equicanis
S. neurona
Characteristics: Named after IM host.
Morphology: Some can form macrocysts - visible with naked eye. Oocysts contain 2 sporocysts with 4 sporozoites.
Location: Intracellular, develop cysts in striated muscles of IM host.
FH: dog, wolf, coyote, raccoon, fox and hyenas, and humans
IM: ruminants, pigs, horses
Epizootology: Zoonotic: S. suihominis, S. bovihominis.
Sarcocystis with dogs or cats as FH are not zoonotic. Species transmitted by dogs - more pathogenic to IM host
Life cycle: Heteroxenous life cycle. Both host-development is endogenous.
Intemediate host – become infected by ingestion of sporocysts shed in the feces of FH. The cysts will excyst in the intestine of IH where they will go through merogony 3 generations, in the endothelial cells of blood vessels. Then the merozoits are named metrocysts (young cysts) and will be transferred to the muscles by lymphocytes and is now called bradyzoits (mature cells). Bradyzoits are infective for the final host.
Final host – becomes infected when ingesting cysts from muscles of IH. Gametogony occurs. Bradyzoits in the lamina propria of small intestine become macrogametes and microgametes and form a zygote. Zygote form oocyst which through sporogony will be sporulated, sporogony occur inside the final host and is shed through feces.
Pathogenesis and clinical signs
No pathology in definitive host - Can be asymptomatic, rarely diarrhea.
dogs more pathogenic to IH
Intermediate host has acute and subacute sacrocystiosis.
Symptoms – fever, apathy, anorexia, pyrexia, anemia, weight loss, decreased milk production, generalized lymphadenopathy, abortion. Causes the formation of macrocysts.
Chronic– clinically inconspicuous, generalized myostitis, degenerating cysts are enclosed by granulomas and mononuclear infiltrations.
Diagnosis: Detection of oocysts/sporocysts in feces - fecal flotation in FH with Faust, digestive method in IH, detection of microcysts!
Serology, meat inspection (some can have microcyst visible),
post mortem of IM.
Treatment: No therapy for IH
FH: toltrazuril, diclazuril
Do not allow dogs to feed on raw meat, most common where home slaughter occurs. Prevent contamination of feed with dog feces containing sporocysts.
16. Equine protozoal myeloencephalitis EPM (S. neurona).
Sarcocystis neurona
Location: cysts in striated muscles. Brain and spinal cord of aberrant horse.
FH: Possum
IM: Small mammals. Horse is aberrant host.
Epizootology: Horses get infected when ingesting possum feces.
Life cycle: FH-opossum release sporulated oocyst to environment -> usually an IH (cat, raccoon) ingest oocyst -> form sarcocysts -> opossum (FH) ingest IH -> gametogony and sporogony.
If a horse ingest the oocyst from environment -> only merogony (no cyst formation!). Horse is not able to infect other horses (dead-end host). Meronts develop in CNS.
Pathogenesis and clinical signs: Meronts develop in neural cells of the brain and spinal cord, causing focal bleeding, necrosis, and myeloencephalitis (inflammation of spinal cord and brain).
Weakness, gait abnormalities, lameness, head tilt, paralysis muscles of the face, partial paralysis of the tongue, ataxia, spasms, paresis and recumbency.
Diagnosis: Clinical presentation, and necropsy. Serology, western blot cerebrospinal fluid is required for the diagnosis, detection of Ab. PCR. Seroprevalence apparently high (close to 50%) – latency, subclinical infection?
Treatment: During 4-12 weeks administrated trimethoprim/sulfadiazine and pyrimethamine in feed.
The therapy can result in side effects such as leukopenia, therefore, it should be given with vitamin B complex. More recently, also served diclazuril, toltrazuril and ponazuril. Anti-inflammatory drugs and vitamin E. Decrease exposure to possum feces.
17. Toxoplasmosis of animals and humans, characteristics, life cycle.
Phylum: Alveolata
Subphylum: Apicomplexa
Class: Coccidea
Order: Eimeridae
Family: Sacrocystidea
Genus: Toxoplasma
Main species: Toxoplasma gondii
Morphology:
· Sporozoite – oocyst. Highly resistant, infective for IH. Can remain in warm, moist soil for more than 1 year. Shed in cat feces.
· Tachyzoite – pseudocyst IH. Rapid growing, observed in early stages of infection. Located free intracellularly. Most common in brain, skeletal muscle and cardiac muscle.
· Bradyzoite – tissue cyst IH. Slow growing (dormant stage). Infective form! brain, skeletal muscle and cardiac muscle. Marks beginning of chronic phase of infection. Resistant to low pH and digestive enzymes. Protective wall is dissolved and bradyzoites infect tissue and transform into tachyzoite.
Location: Intracellular. Infect nucleated cells, not erythrocytes.
FH: Felines
IM: Birds and mammals, humans are aberrant host. Zoonotic!
Fecal-oral route. Ways of human infection – contact with cat feces, raw vegetables, gardening, human contamination from raw or undercooked meat -> vertical transmission to fetus if human is pregnant (rare in cats). 15-70% of the population is chronically infected.
3 situations can lead to severe disease:
- congenital toxoplasmosis
- ocular toxoplasmosis in immunocompetent adults
- loss of a functional immune system.
Life cycle: Heteroxenus, but can have direct life cycle if cats ingest infective oocyst.
Pathogenesis and clinical signs:
Cats – Effects young and immunocompromised, most common in 2 year old’s.
Most cats are asymptomatic.
Cause enteritis, lymphadenopathy, pneumonia, encephalitis, nephritis, anorexia, weight loss, lethargy.
Clinical signs fever, reduced appetite, lethargy and diarrhea.
eye form - retinitis(retinal inflammation), uveitis, chorioretinitis;
-
Dogs – Acute: fever, lymph node enlargement, nose and eye discharge, tonsillitis, dyspnoea, diarrhea, progressive weight loss, pneumonia (most common).
Chronic: hepatitis, myocarditis, pneumonia, nerve symptoms during CNS involvement (apathy, tremor, ataxia, hemiparesis, paresis, paralysis)
Pigs – fever, enlarged lymph nodes, nose and eye discharge
Horses, race game and poultry - Asymptomatic
Large ruminants - abortions.
Small ruminants - abortions and CNS disorders.
Humans – Tachyzoites directly destroy host cell, especially parenchymal and reticuloendothelial cells. Most human infections are asymptomatic or only benign symptoms (headache, sore throat, lymphadenitis, fever).
- Prenatal toxoplasmosis - Abortion, stillbirth, intracerebral calcification, hydrocephaly/microcephaly, neurological damage, learning difficulties.
- Postnatal toxoplasmosis - Rare in healthy humans
1-2 weeks incubation period
Diagnosis: Detection of oocysts in FH is difficult as the eggs are shed before the clinical signs. Serology in FH. PCR. Tissue biopsy, examination of body fluids.
Treatment: Cats: Toltrazuril, Clindamycin + trimethoprim.
Dogs: Sulfonamids + trimetoprim.
Human: Spiramycin until delivery if pregnant.
Combination therapy of pyrimethamine + sulfadiazine or trisulfapyrimidines.
Avoid contact with cat feces, change cat litter daily, avoid raw or undercooked meat. Wash raw fruits and vegetables well before eating. Keep cats indoors to prevent hunting.
18. Plasmodiidosis of human and animal.
Phylum: Alveolata
Subphylum: Apicomplexa
Class: Haenatozoea
Order: Haemospoidia
Family: Plasmodidae
Genus: Plasmodium, Leucocytozoon, Haemoproteus
Main species:
P. brasilianum – Monkeys
P. vivax – humans
P. ovale – humans
P. falciparum – most pathogenic! Humans
P. malariae –
Morphology and cysts: Young trophozoites are called ring form, has nucleus, ribosomes, cytoplasma and a ring cavity (cytoplasm with vacuoles, hemoglobin digestion and malarial pigment).
In merozoites, the nucleus is repeatedly divided and we can see hemozin – malarian pigments.
No sporocysts, sporozoites lie in oocyst. Zygote is motile (ookinete).
Location: Intracellular in RBC, liver cells and macrophages.
FH: Mosquitoes – Anopheles most common in mammals.
IM: Reptiles, birds, rodents, monkey, humans
Life cycle: 1sexual + 3asexual stages. Moment of erythrocytic cycle decay and release of merozoits -> triggers a feverish malaria attack. All are heteroxenous.
IH – merogony
FH – Gametogony (occur in mosquito gut) and sporogony
mosquito give sporozoits into the human. Sporozoits infect the liver cells and go through exo-erythrocytic stage. In the liver cells they mature into schizonts, through merogony and release merozoites. P. vivax an P. ovale can form hypnozoites in liver if untreated and cause relapse by invading bloodstream weeks or even years later.
Merozoits invade the blood cells in the liver and can undergo another round of asexual multiplication (merogony) inside the erythrocytes by become immature trophozoites (ring stage).
Some merozoites develop into gametocytes (last asexual stage). These are ingested by mosquito during blood meal. In the gut of the mosquito, Gametogony occurs and they form a motile zygote (ookinete) which invade the midgut wall and develop into oocyst. Oocyst grow, rupture and release sporozoites (sporogony) which travel to salivary glands and can be inoculated into a new IM host.
Pathogenesis and clinical signs: Clinical presentation is acute febrile illness, may have periodic febrile paroxysms every 2-3 days with afebrile asymptomatic intervals.
Early symptoms: headache, fatigue, nausea, muscular pains, slight diarrhea, slight fever. Could mistake for influenza or gastrointestinal infection
Clinical signs are anemia, thrombocytopenia, hepatosplenomegaly, renal dysfunction, mental status changes. Prodromal symptoms can range from none to mild to severe, includes malaise, fatigue, headache, muscle pain, nausea, anorexia and flu-like symptoms, marks end of incubation period.
Immunity is acquired, can be transferred from mother to child
Infection in monkeys are generally asymptomatic, or cause mild symptoms.
Diagnosis: Stained blood smear, PCR, ELISA, IFAT
Treatment: Mefloquine, Doxycycline, Malarone (also as prophylaxis), Chloroquine, hydroxychloroquine
19. Avian malaria (Plasmodium, Hemoproteus, Leucocytozoon).
Family
genus
This disease is very similar to human malaria, and is transmitted by the bite of infected insects.
Life cycle is also very similar:
- Merogony occur first in reticuloendothelial system (mononuclear cells) and later in the erythrocytes.
- Gametogony and sporogony occur in vectors.
Wide range of symptoms from asymptomatic to drastic decline in population number.
Plasmodium
P. relictum – infect birds all over the world.
P. gallinaceum - hepato/splenomegaly, anemia and abdominal distension.
Many plasmodium species in birds rarely cause disease in their specific host, but for imported birds cause disease.
Pathogenesis and clinical signs: Plasmodium reproduces in RBC -> bursting of RBC case anemia (birds have nucleus in their RBC), hypoxia, progressive weakness and death.
intermittend fever, splenomegaly and secondary anemia.
Haemoproteus
H. meleagridis – Turkey
H. columbae – pigeon (pigeon malaria)
Intracellular parasites infecting erythrocytes. Called pseudomalaria, due to its similarity to Plasmodium spp.
Transmitted by various biting insects (Culicoides; avian keds (Ornithomyia, Lynchia, Pseudolynchia, Stilbometopa); horse fly (Chrysops)).
Birds and reptiles as vertebrate host.
Life cycle is similar to Plasmodium. FH infect birds with sporozoites -> merogony in tissues -> merozoites invade RBC and develop into gametocytes, infective stage for FH which ingest them with blood.
Pathogenesis and clinical signs: Subclinical infections, acute form – pigeon. Cause enlarged stomach, spleen, liver and kidney.
They may have a chocolate-brown color due to accumulation of hemozoin.
have movement pain, appearance of fluffy feathers, exhaustion, weakness, death, anemia.
Diagnosis: Finding only gametocytes inside RBC.
Treatment/control: Chloroquine. Control of vectors, insecticides.
Leucocytozoon
L. smithi – Turkey
L. simondi – waterfowl
L. caulleryi – chicken
Parasites wild sometimes in domestic poultry. Located in capillary endothelial cells, RES organs (liver and spleen), leukocytes and erythrocytes.
Vector and FH: Simulium spp. (black fly -> sporozoites).
Life cycle: similar to Plasmodium spp. Meronts develop in hepatocytes -> formation of merozoites -> enter blood stream -> infect leukocytes -> develop gamont -> ingested by blood-sucking black flies -> gametogony -> develop sporozoites.
Pathogenesis and clinical signs:
5 days after → cells rupture and there are many schizonts in hepatocytes.
7 days →, accumulation of gametocytes in liver, megaloschizons in spleen, lymphatic and other tissue.
12 days →hemorrhagic scars after megaloschizontal rupture. Most infected birds are asymptomatic.
They can show anorexia, anemia, weakness, depression, difficulty breathing and inability to fly, difficult to move, uncoordinated with manifestations of paralysis, granulomatous lesions are visible in the lungs, heart, brain and peripheral nerves. Young birds die within 24h. They acquire immunity after overcoming the disease, and adult birds are reservoirs.
Diagnosis: finding gametocytes -stained blood smears. They are large, lack pigment and distort the RBC and WBC, making it no longer identifiable.
Histopathological examination of the liver, spleen and brain with finding of megaschizonts. Pathological anatomical autopsy, enlargement of liver and spleen
Treatment: Therapy is usually not effective. We can give pyrimethamine, sulfadimethoxin and clopidol in feed. Vector control is important. Can use anti-Leucocytozoonous vaccine when parasitemia is reduced but infection is not obvious.
20. Babesiosis of ruminants and horse
Phylum: Alveolata
Subphylum: Apicomplexa
Class: Haenatozoea
Order: Piroplasmida
Family: Babesiidae
Genus: Babesia
Main species:
B. bovis – Texas cattle fever. Small
B. bigemina – Texas cattle fever. Large
- Vector – boophilus anulatus
- OIE-listed
B. divergens – cattle. Small. human clndamicin +quinune combo
B. major – cattle. Large
B.equi - ovis
Morphology: Pyriform, round and oval shape, can be small (1-2um) or large (2-5um). Large babesia is located in the central of blood cells, paires pyriform shape. Small babesia is found in the periphery of the cells, as single ring form. Free sporozoite, no sporocyst.
Location: Intracellular parasite, found in erythrocytes, lymphocytes, histiocytes and erythroblasts.
FH: Ticks
IM: Vertebrates, infect all cattle and domestic animals
Boophilus annulatus.- B. bigemina Transstadial + transovarial transmission.
Ixodes ricinus - B. divergens
Larval ticks transmit B. bovis, Adult and nymphal ticks transmit B. bigemina
Zoonotic: B. divergens, B. bigemina, B. equi, B. microti
Life cycle: FH and vectors – sexual reproduction (gametogony and sporogony). IM – asexual reproduction
Sporozoits are passed into the blood of IH by ticks taking a blood meal. They invade blood cells and go through merogony -> merozoits can affect new cells or develop into gametocytes, taken up by FH during feeding Inside FH they go through Gametogony -> kinete. Ookinete go to the eggs and transmit transovarially to next generation, so all stages of the tick will potiantially be infective OR it can transmit transstadial -> sporogony in mouth of tick.
Pathogenesis and clinical signs:
Severe in adult cattle than calves
Calves less 1 yr seldom affected
hemolotic anemia
B. bigemina: 2-3 weeks after tick infestation.
Cause anorexia, hemoglobinuria and fever up to 41.5C.
separate from herd, stand with arched back and display a roughened coat, dyspnea and tachycardia.
anemia → Jaundice Urine red Damage to internal organs
B. bovis takes slightly longer.
More virulent. Similar clinical signs, but they usually develop a higher fever, anorexia, depression, ataxia and circulatory shock.
Hemoglobinuria and hemoglobinemia less common.
Infected erythrocyte in brain capillaries → incoordination, teeth grinding and mania.
Animals may be found on the ground with the involuntary movements of the legs. Death often follows CNS signs. Can form post-mortem lesions. emboli throumus in brain
B. equi: Fever, hemolytic anemia and jaundice. Incubation 8 - 10 days, disease last for 10 days. Death may occur during first 24 - 48h.
Diagnosis: Stained blood smear or serology. Post mortem lesions in brain capillaries.
Treatment:Diminazine, tick control, regular dipping of cattle, vaccines.
21.Dog Piroplasmosis/babesiosis (babesia, hepatozoon).
Main species, morphology and epidemiology:
Species and vector ticks of LARGE babesia (2-5 μm)
Babesia canis canis- Dermacentor reticulatus
Babesia canis vogeli- Rhipicephalus sanguineus Less pathogenic!
- Often without clinical signs, but fatal in puppies
Babesia canis rossi - Haemaphysalis leachi Most pathogenic!
Pyriform organisms, pear-form in RBC.
Species and vector ticks of SMALL babesia (1-2 μm)
Babesia canis gibsoni - Rhipicephalus (Europe, Africa, Asia, America)
Single form organisms
Life cycle: Same as in cattle
infective sporozoites migrate from the tick’s salivary gland to the host’s blood.
Obligate intracellular parasites that invade, divide within and rupture RBCs → direct parasite-induced RBC damage.
Pathogenesis and clinical signs: Babesia canis (young dogs), Babesia gibsoni (all ages).
rupture RBCs → . Causes ischemia (hypoxic damage – RBCs cannot transport O2).- necrosis.
Anemia-lysis of RBCs.
Accumulation of toxin materials which affects CNS
Clinical symptoms are lack of energy and appetite, pale gums, fever, enlarged abdomen, colored urine, icterus, weight loss and discolored feces.
anemia, thrombocytopenia, hypoalbuminemia, and bilirubinuria.
severe icterus due to babesiosis. yellow
Acute form: general findings (fever, weakness, pale mucus membranes, depression). lymphadenopathy, splenomegal
Chronic form: irregular temp, variable appetite, loss of condition. Dogs are permanent carriers after infection. Brain necrosis post mortem.
Diagnosis: Examination of stained blood films – easiest (Giems-romanowski staining, Diff-quick).
Serology only show exposure.- ELIZa
Blood smear examination is useful for clinical babesiosis in dogs. However, the sensitivity of this method is very low.
Treatment: Preparations with active substance imidocarb at dose of 2-5mg/kg.
diminiazen-diaceturate and trypan blue.
Symptomatic therapy. - vitamins B + iron
Tick control, tablets, collars, sprays, shampoo.
hepatozoon
Phylum: Alveolata
Subphylum: Apicomplexa
Class: Haenatozoea
Order: Adeleida
Family: Hepatozoidae
Genus: Hepatozoon
Main species: Hepatozoon canis (old world), H. Americanum (new)
Rhipicephalus sanguineus (old world), Amlyoma maculatum (new world).
Morphology: It is more elongated.
Location: Gametocytes in circulating leukocytes and tissue “cysts” in muscle.
asymptomatic unless concurrently infected, immunosuppressed or younger than 4 m
FH: Rhipicephalus sanguineus (old world), Amlyoma maculatum (new world)
IM: Dogs
Life cycle: Dog ingest cysts, sporozoits release in GIT, they migrate by blood or lymph to muscles, spleen, liver, lymph nodes and bone marrow. Here they go through merogony. In muscle tissue, they can form cysts in which merogony occurs within. Meront rupture and merozoites are released. This caused inflammatory response, recruiting neutrophils and monocytes. The merozoits can repeat the asexual cycle or invade these leukocytes and develop into gametocytes, which is infective for feeding ticks -> Gametogony and sporogony. Dog ingest tick. Merozoites in WBC can also cause intrauterine transmission to puppies.
Pathogenesis and clinical signs:
fever, lymphadenopathy, ocular and nasal discharge,
anorexia, cachexia, anemia, leukocytosis, paraparesis, depression, muscular hyperesthesia and a reluctance to move.
The animal may develop severe cachexia, vasculitis and renal failure.
Cysts containing merozoites may be found in muscle biopsies. Leukocytes may contain gametocytes.
Diagnosis: By blood smear, - merozoites in neutrophils and muscle biopsy.
Treatment: Combinations of trimethoprim and sulfadiazine, imidocarb
( diproprionate, tetracycline, doxycycline, toltrazuril).
22. Theileriidosis of mammals.
Phylum: Alveolata
Subphylum: Apicomplexa
Order: Piroplasmida
Family: Theileriidae
Genus: Theileria
Main species:
Theileria parva parva – East coast fever (bw cattle)
T. parva bovis – bw cattle - January disease
T. annulata – Tropical theileriosis/ Mediiterranean theileriosis
T. lestoquiardi – sheep and goat, can have 100% mortality.
T. equi
Morphology:
Location: Found in predominantly in lymphocytes, where development occurs. Can be found in RBC-
Vector/FH: Ticks. Riphicephalus appendiulatus (T. parva), Hyalomma anticolicum (T. lestoquiardi) T. annulata – hylomma spp.
IM: Ruminants
Epizootology: Transstadial transmission by ticks (bw generations)
Life cycle: T. parva life cycle
IH – sporozoits are relased from the tick during feeding on a vertebrate host. The sporozoits become trophozoits, attach to the lymphocytes and enter by “zippering” mechanism and develop into merozoits. Merozoits multiply inside the lymphocyte (merogony) and the cell ruptures releasing merozoits to infect red blood cells and become piroplasms and are infective to ticks. They don’t multiply in RBC.
FH – tick larvae and nymphs are infected when they suck blood from an infected vertebrate IM. Piroplasm -> gametes and form a zygote, which develop into a kinete. Kinete travels to salivary glands where it will undergo sporogony and can infect new IM hosts during feeding.
Pathogenesis and clinical signs:
T. parva. - East Coast fever
High mortality rates in cattle
Enlarged, hemorrhagic and edematous lymph nodes. Just before death, pulmonary exudate from the nostrils. right before death drop of body temp
Necropsy show edema of lungs, hyperemia, infarcts, thrombosis and lymphoid hyperplasia in spleen.
fevr 42 - Lymph node swelling, Anorexia
lacrimation and nasal discharge may occur.
Post mortem findings Lymph node enlargement and massive pulmonary edema and hyperemia. Hemorrhages are common on the serosal and mucosal surface as well some organs
Anemia is not a major diagnostic sign
T. annulata cause mortality up to 90%.
fever, swollen superficial lymph nodes. Rapid loss of condition and hemoglobinuria.
Morphologically similar to T. parva.
Diagnosis of T. parva: demonstration of parasite in Giemsa-stained blood, lymph node and tissue impression smears. But it is difficult to differentiate between schizonts and piroplasms of different Theilieria species.
IFA, PCR and probing. Can be mixed infection of different species, which complicate the diagnosis of T. parva.
Treatment:T. parva. Parvaquone and its derivate buparvaquone, halofuginone. Treatment with these is highly effective when applied in early stages, less effective in advanced staged. Incidences can be reduced by tick control.
shee + goa
100% with T. lestoquardi → Hyalomma anatolicum
Nonpathogenic T. ovis) transmitted by R. evertsi tand Haemaphysalis punctata
23. Balantidiosis of pigs.
Phylum: Ciliphora
Class: Litostomatea
Order: Vestibulferida
Family: Balantidae (only one genus)
Genus: Balantidium
Main species: Balantidium coli
Morphology: Nuclear dimorphism = 2 nuclei: micronuclei and macronuclei. Macronucleus is typically elongated and kidney-shaped, micronucleus is spherical. Moves with cilia. The cyst is round or oval. Transparent. 2 prominent contractile vacuoles, indicating osmoregulation. Large size.
Has 2 forms:
· Infective cyst: Encapsulated form, non-mobile, but survives in environment.
· Trophozoite: Found in cecal area and throughout large intestine.
Location: Large intestine
FH: Pigs, wild boar and sometimes humans.
Life cycle: Oral ingestion of cyst -> trophozoite hatch in small intestine -> move and settle down in large intestine, where it feeds on bacteria and starch, or by invading the mucosal wall of the large intestine. Here they secrete a substance that destroys intestinal tissue and creates ulcers or abscesses.
Trophozoites multiply asexually (binary fission) or sexually (conjugation) -> form new cysts -> excreted in feces. Trophozoite can shed feces but disintegrate quickl.
Pathogenesis and clinical signs: Due to low virulence -> pigs are usually asymptomatic.
Trophozoites rarely invade the intestinal wall cause haemorrhagic diarrhea, lesions and ulcers of intestine.
can spread liver and lungs
Diagnosis: Flotation method. In acute diarrhea -> motile trophozoites are seen in direct smears. Trophozites are large and they only parasitite humans and pigs that have cilia. Infection may disappear spontaneously or the host may become asymptomatic and be carriers.
Treatment: Metronidazole, Tetracycline.
Encephalitozoonosis and nosematosis.(look it up for bees)
Phylum: Microsporidia
Rabbit
They are small, unicellular, spore-forming parasitic fungi with obligate intracellular development.
Main species: Encephalitozoon cuniculi ZOONOTIC
Morphology: The wall consists of an endospore and an exospore, enclosing the cytoplasm. Cytoplasm include 1 or 2 nuclei, a vacuole and an extrusion apparatus. No mitochondria. Polar tubule - coiled organelle that injects spore content into host cell.
Location: Unknown, but affects CNS and kidneys
FH: Rabbits.
Epizootology: Oral or transplacental transmission.
Life cycle: Infective form is the resistant spore. It is ingested or inhaled by rabbits. It uses its polar tubule to penetrate host cells and injects infective sporoplasm. Sporoplasm divides through merogony -> merozoites undergo sporogony -> sporonts -> sporoblasts -> spore. Spores increase in number and when cytoplasm is completely filled they released by the host cell. These spores can infect new cells, continuing the cycle, or they can be shed in feces or urine.
Pathogenesis and clinical signs: Merogony: microsporidia does not cause serious cell damage.
Sporogony: cause cell destruction and focal granulomatous inflammation of surrounding tissue. Immunosuppressed host may suffer serious disease with fatal outcome. Can cause keratoconjuctivitis, infection of respiratory and urogenital tract
Rabbits: Spread via blood to kidneys and brain. Clinical signs are head tilt, kidney lesions, damage to CNS, nonspecific neurological signs. Usually asymptomatic, but rabbits may develop mild, chronic renal disease. Some develop brain lesions -> head tilt, convulsions, tremors
manifets 3 ways
renal - ocular
cns
non spesific
Diagnosis: Light microscopic examination of stained fecal samples, identification of spore in feces. Transmission electron microscopy is standard and necessary to identify the species. IFA and PCR is also used.
Treatment: Fenbendazole, fumagiline, nitazoxanide.
Dogs
no synptoms
papies - from mother trans placenta
diagnosis difficult usually even healyhy dogs may have them antibody
spores cann mayby found kidney
very dame as up but not head tilting is seen
human - same as in rabbits usually immuno comprimized
nosematosis. - bees
2) Nosematosis (in honey bees)
Fungi - microsporida,
V. apis (dysentery)
restricted to midgut epithelium → digestive dysfunction, reduced lifespan, colony collapse effects in bees. It cause change in sugar metabolism & hormone levels.
CS: bee colony-level - weak growth, dysentery (V.apis), reduced foraging & behavior change, queen laying reduction.
Dg: bee gut microscopy, PCR, LAMP, DNA testing.