Psychology: MCAT
1/97
Earn XP
Description and Tags
Psychological, Social, and Biological Foundations of Behavior Section
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
98 Terms
List out the different types of Experimental Design
Descriptive Experiments
Aim to describe a phenomenon
Focus on detailing and characterizing observed phenomena without necessarily testing specific hypotheses
Provide comprehensive descriptions
Inferential Experiments
Seek to draw conclusions and make predictions based on collected data
Focus on testing hypotheses based on collected data, often manipulating variables to examine cause-and-effect relationships
Employ statistical analysis to determine significance of results and generalize findings
Observational Studies
Involve observing and analyzing existing data
Analyze existing data or observations WITHOUT directly intervening
Try and identify patterns as they are
Experimental studies
Involve actively manipulating variables and collecting new data
Try and identify cause-and-effect relationships under controlled conditions and the use of treatments
Cross-Sectional Studies
Collect data from a SINGLE point in time, providing a snapshot of a population or phenomenon at a specific instant
Longitudinal Studies
Extend over an extended period of time, repeatedly collecting data from the same individuals or subjects at multiple time points
Case-Control Studies
Compare individuals with a specific condition to a control group of individuals without it
Good for identifying risk factors
Cohort Studies
Follow a group of individuals over time that share a common characteristic to assess the development of a condition
Valuable for assessing the incidence and causation of diseases or conditions in a population
Confounding Variable
Linked to independent and dependent variables, potentially distorting their genuine relationship
Experimenter Effect
Influence that researchers’ expectations, behaviors, biases, and credentials may have on participants’ behavior in a study
Demand characteristics
Involve cues or expectations from participants that can influence their behavior or responses in a study
Demand characteristics are cues in a study that lead influence participants’ responses or behavior in order to fit or contradict the research purpose and change their behavior accordingly.
For example, if participants in a memory study realize the researcher is testing the effects of caffeine, they might try harder on memory tasks, skewing the results.
Socialization
The process thorugh which individuals learn and internalize the values, beliefs, and norms of their society or immediate surroundings
Adopting and internalizing views of those around them
Cultural diffusion
Spread of cultural items such as ideas, styles, religions, techonlogies, and languages between indiviudals whether within a single culture or from one culture to another
Role strain
Arises when there’s tension due to conflicting demands within a single societal role, or between different roles one may occupy
Roles of different parts of the brain
Hypothalamus
Homeostasis
Regulation of body temp, thirst, hunger, sleep, circadian rhythm, autonomic regulation of heart rate & breathing
Cerebellum
Coordination of different parts of the body
Pre-central gyrus:
Primary motor cortex
Post-central gyrus:
Somatosensory cortex
Posterior Pituitary Gland
Vasopressin
Oxytocin
Hippocampus
Memory, learning, and emotion
Hold on to short-term memories and then transfer them to long-term storage in the brain
What are the sensory receptors?
Where are receptors in the skin? Are there any in the epidermis?
Exteroceptors (Location)
-Sensitive to stimuli arising from outside the body located at or near body surfaces
1. Touch
2. Pressure
3. Pain
4. Temperature
Interoceptors (Location)
-Receive stimuli from internal viscera, located in digestive tube, tongue, bladder, and lungs to monitor
1. Changes in [chemical]
2. Taste stimuli
3. Tissue stretching
4. Temperature
Proprioceptors (Location)
-Monitor degree of stretch and send inputs on body movements to the CNS
-Located in skeletal muscles, tendons, ligaments, and joints
Mechanoreceptors (Type of Stimuli)
-Respond to mechanical forces
1. Touch
2. Pressure
3. Stretch
4. Vibration
5. Itch
Baroceptors (Type of Stimuli)
-Monitor blood pressure
Thermoreceptors (Type of Stimuli)
-Respond to temperature changes
Chemoreceptors(Type of Stimuli)
-Respond to chemicals in solution
Photoreceptors(Type of Stimuli)
-Respond to light, located in eye
Nociceptors(Type of Stimuli)
-Respond to harmful stimuli that result in pain
Where are receptors in the skin? Are there any in the epidermis?
Yes, receptors do exist in the epidermis:
Free nerve endings penetrate the epidermis.
Merkel cells are literally in the basal layer of the epidermis.
But most of the bigger mechanoreceptors (Meissner, Pacinian, Ruffini) live in the dermis or deeper.
What are the main types of Mechanoceptors to know about?
Receptor | Stimulus | Adaptation | Skin Layer | Fiber Type | Key Features |
|---|---|---|---|---|---|
Meissner’s Corpuscle | Light touch, flutter | Fast-adapting | Papillary dermis | Aβ | Detects gentle, changing stimuli (e.g. brushing, putting on clothes) |
Pacinian (Lamellar) Corpuscle | Deep pressure, vibration | Fast-adapting | Hypodermis | Aβ | Deepest mechanoreceptor, detects vibration & poke |
Merkel’s Disc | Sustained light touch, texture | Slow-adapting | Stratum basale + papillary dermis | Aβ | Specialized epidermal cell, used for reading Braille, shape & edge detection |
Ruffini Ending | Sustained deep stretch/touch | Slow-adapting | Reticular dermis | Aβ | Responds to skin stretch, collagen deformation, good for grip stability |
Hair Follicle Receptor | Hair movement/light touch | Fast-adapting | Anchored in reticular dermis | Aβ | Detects hair displacement, great for sensing insects or breeze |
Fast-Adapting (Detect Change):
Meissner’s corpuscle
Pacinian (Lamellar) corpuscle
Hair follicle receptor
Slow-Adapting (Detect Sustained Pressure):
Merkel’s disc
Ruffini ending
Adaptation matters: fast = change detection; slow = continuous pressure detection
Location matters: deeper mechanoreceptors (e.g., Pacinian, Ruffini) respond to stronger stimuli
All touch receptors use Aβ fibers, which are fast, myelinated afferent fibers
Hair follicle receptors are superficially stimulated but anchored deep
Meissner’s = light, changing touch → fast-adapting, superficial
Pacinian = deep pressure/vibration → fast-adapting, deep
Merkel’s = constant touch/pressure → slow-adapting, mid-layer
All use Aβ fibers for touch; pain uses Aδ or C fibers
Adaptation: fast-adapting = respond only to change; slow-adapting = respond continuously
Mechanism of Activation (for all of them):
Mechanical pressure deforms receptor → Na⁺ channels open
Sodium influx causes graded potential
If strong enough → triggers action potential in afferent Aβ fiber
What are the types of afferent fibers to know for MCAT?
Types of Afferent Fibers:
Fiber Type | Speed | Function |
|---|---|---|
Aβ fibers | Fastest | Touch, pressure, proprioception |
Aδ fibers | Medium | Sharp pain, temperature |
C fibers | Slow | Dull, lingering pain |
What are the heat transfer mechanisms you shoudl know about?
Radiation
Description: Transfer of heat through electromagnetic waves, without the need for direct contact.
Example: The sun's heat warming your skin.
Conduction
Description: Transfer of heat through direct contact between molecules in solids or liquids.
Example: A metal spoon heating up in a hot cup of coffee.
Convection
Description: Heat transfer through the MOVEMENT of FLUIDS (liquids or gases), where warm particles rise and cool particles sink.
Example: Warm air rising and being replaced by cooler air near a fan.
Example 2: In a pot, warm water at the bottom rises due to reduced density, while cooler water moves down to replace it
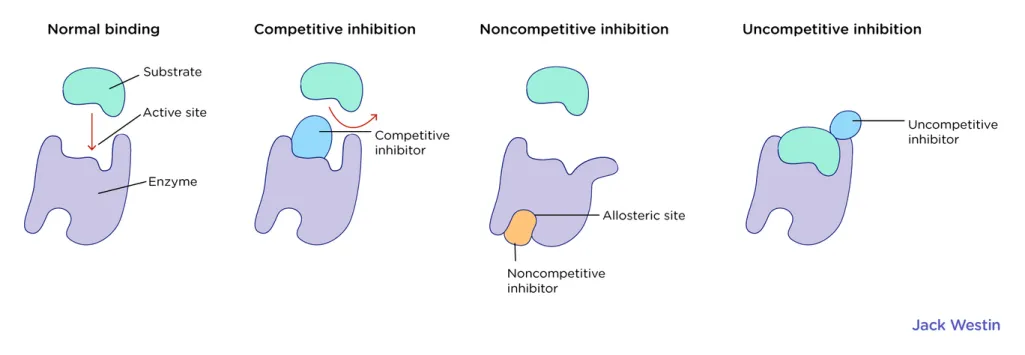
What are the three different types of inhibition in enzymatic kinetics and how does this affect Km and Vmax?
Competitive Inhibition: The inhibitor competes with the substrate for binding to the active site, increasing the apparent Km but leaving Vmax unchanged.
IN COMP you get “more Kills/Km”
Higher Km, same Vmax
Uncompetitive Inhibition: The inhibitor binds only to the enzyme-substrate complex, lowering both Km and Vmax.
UNCOMP, trying new characters so you’re lower at everything
Lower Km, lower Vmax
Non-competitive Inhibition: The inhibitor binds to an allosteric site, not affecting substrate binding (Km remains unchanged) but decreasing the enzyme's maximum activity (Vmax).
Non-Comp, non-Muslim dunya stays same but akhira decreases
Same Km, lower Vmax
Competitive: Increases Km, Vmax unchanged.
Uncompetitive: Decreases Km, Vmax decreases.
Non-competitive: Km unchanged, Vmax decreases.
So, Vmax CAN increase, but not due to inhibition — only through activation or increased enzyme concentration.
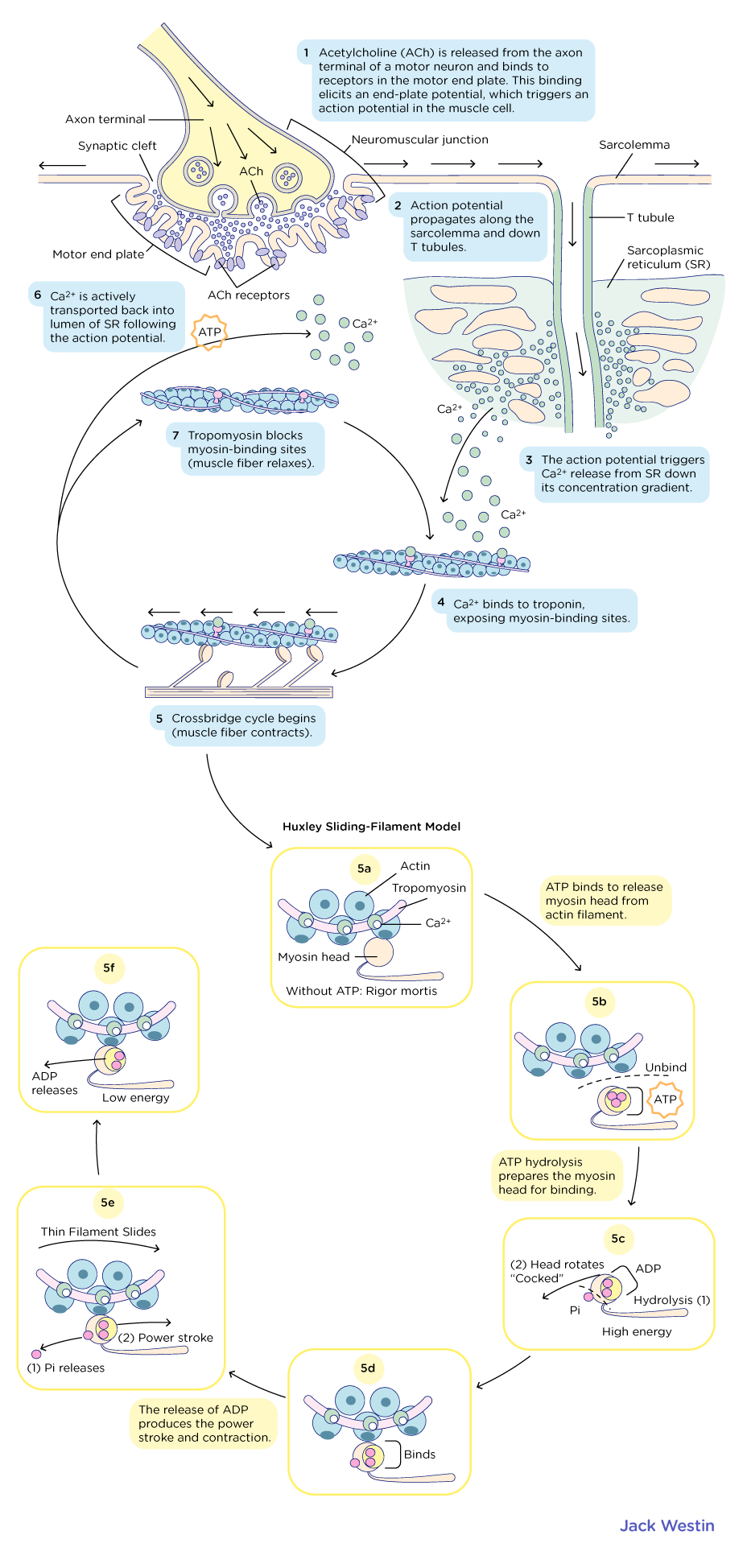
Describe step by step how the contraction of muscle is initiated
ATP has three phosphates
Alpha
Beta
Gamma
The gamma phosphate of ATP is the one that is terminal to the chain of triphosphates which, when RELEASED from ATP forms ADP
The release of the gamma phosphate from ATP promotes the cocking of the myosin head which allows for the myosin head to form a new cross-bridge
THe opening of voltage-gated calcium channels allows for the free passage of calcium into the sarcoplasm (passive)
During contraction, muscle tissue shortens due to the overlap of contracticle units within the muscle
Depolarization of the sarcolemma would result in muscle SHORTENING
Describe Carl Rogers’ theory of personal development in a nutshell
Carl Rogers' Theory of Personal Development (Humanistic Perspective)
Core Idea: Personal growth happens when an individual strives for self-actualization, aiming to align their actual self with their ideal self through positive experiences and personal insight.
Key Concepts for the MCAT:
Ideal Self:
The person you aspire to be based on personal goals and societal expectations.
Example: Wanting to be a kind, successful doctor.
Perceived Self:
How you see yourself based on experiences and feedback from others.
Example: Believing you are hardworking but struggling with confidence.
Actual Self:
Your true characteristics and behaviors at any given moment.
Example: Your current abilities, emotions, and self-awareness.
Self-Concept:
The overall image and understanding of yourself, shaped by experiences.
Includes self-esteem, self-worth, and identity.
Congruency:
When the ideal self and actual self are aligned, leading to fulfillment and self-actualization.
Example: You see yourself as compassionate and actively engage in helping others.
Incongruency:
When the ideal self and actual self do not align, leading to discomfort or dissatisfaction.
Example: Wanting to be confident but struggling with self-doubt.
Self-Esteem:
Your overall evaluation of your self-worth.
Higher when congruency is present, lower when there is incongruency.
Existential Self:
The understanding that you are a separate, distinct being with your own experiences.
Example: Recognizing “I am me” and separate from others.
Categorical Self:
The understanding of yourself in relation to different categories, such as age, gender, or roles.
Example: Identifying as a student, daughter, or future doctor.
MCAT Relevance:
Ties into self-concept, self-esteem, and identity theories.
Important for understanding human motivation and personal growth.
Contrasts with Freudian and behaviorist perspectives
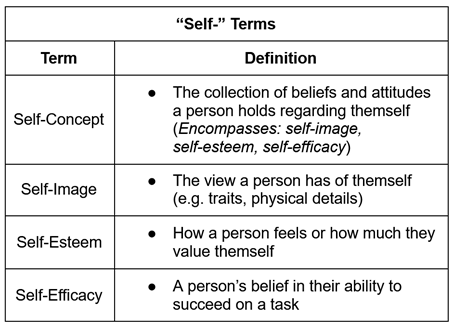
What are the different selfs?
Self-worth
Refers to one’s recognition that they are unique, valuable, and worthy of love
Self-concept
Describes how one thinks about themself overall
Self-verification
Refers to the idea that individuals want to be perceived as they see and express themselves
Self-efficacy
Refers to one’s belief in their own COMPETENCE and ability to succeed in a given SITUATION
NOT to be confused with self-esteem
Self-esteem
Describes an individual’s thoughts, feelings, beliefs about themselves and their VALUE
You can have high self-efficacy and low self-esteem and vice versa
Key Theories of Identity & Self-Concept for the MCAT
1. Erikson’s Psychosocial Development (Lifespan Identity Formation)
Identity develops through eight life stages, each with a key social conflict.
Example: Adolescence (Identity vs. Role Confusion) is when individuals explore and form their personal identity.
8 Life Stages:
Trust vs. Mistrust (0-1 yr)
If caregivers are reliable, the infant develops trust; if not, mistrust forms.
Virtue developed: Hope
Autonomy vs. Shame & Doubt (1-3 yrs)
Developing independence (e.g., walking, making choices); over-control leads to shame/doubt.
Virtue developed: Will
Initiative vs. Guilt (3-6 yrs)
Children begin planning activities and showing initiative; if discouraged, they feel guilt.
Virtue developed: Purpose
Industry vs. Inferiority (6-12 yrs)
Success in school and social tasks leads to competence; failure results in inferiority.
Virtue developed: Competency
Identity vs. Role Confusion (12-18 yrs)
Adolescents explore who they are; success leads to strong identity, failure to confusion.
Virtue developed: Fidelity
Intimacy vs. Isolation (18-40 yrs)
Forming deep relationships leads to intimacy; avoiding connection results in isolation.
Virtue developed: Love
Generativity vs. Stagnation (40-65 yrs)
Helping the next generation (career, family) leads to fulfillment; failing to contribute leads to stagnation.
Virtue developed: Care
Integrity vs. Despair (65+ yrs)
Reflecting on life with satisfaction leads to integrity; regret leads to despair.
Virtue developed: Wisdom
2. Freud’s Psychosexual Development (Childhood Stages & Personality Formation)
Identity and personality develop through five psychosexual stages, where libido (sexual energy) focuses on different body parts.
Fixation at a stage can lead to personality issues.
Example: A person fixated at the oral stage (0-1 yr) may develop habits like nail-biting or overeating.
5 Stages: (OLD AGED PEOPLE LOVE GRAPES)
Oral (0-1 yr) → Mouth (sucking, biting) → Dependency issues if fixated.
Anal (1-3 yrs) → Bowel control → Orderliness/messiness fixation.
Phallic (3-6 yrs) → Oedipus/Electra complex → Sexual identity formation.
Latency (6-12 yrs) → Dormant libido → Social & intellectual development.
Genital (12+ yrs) → Maturity & adult relationships.
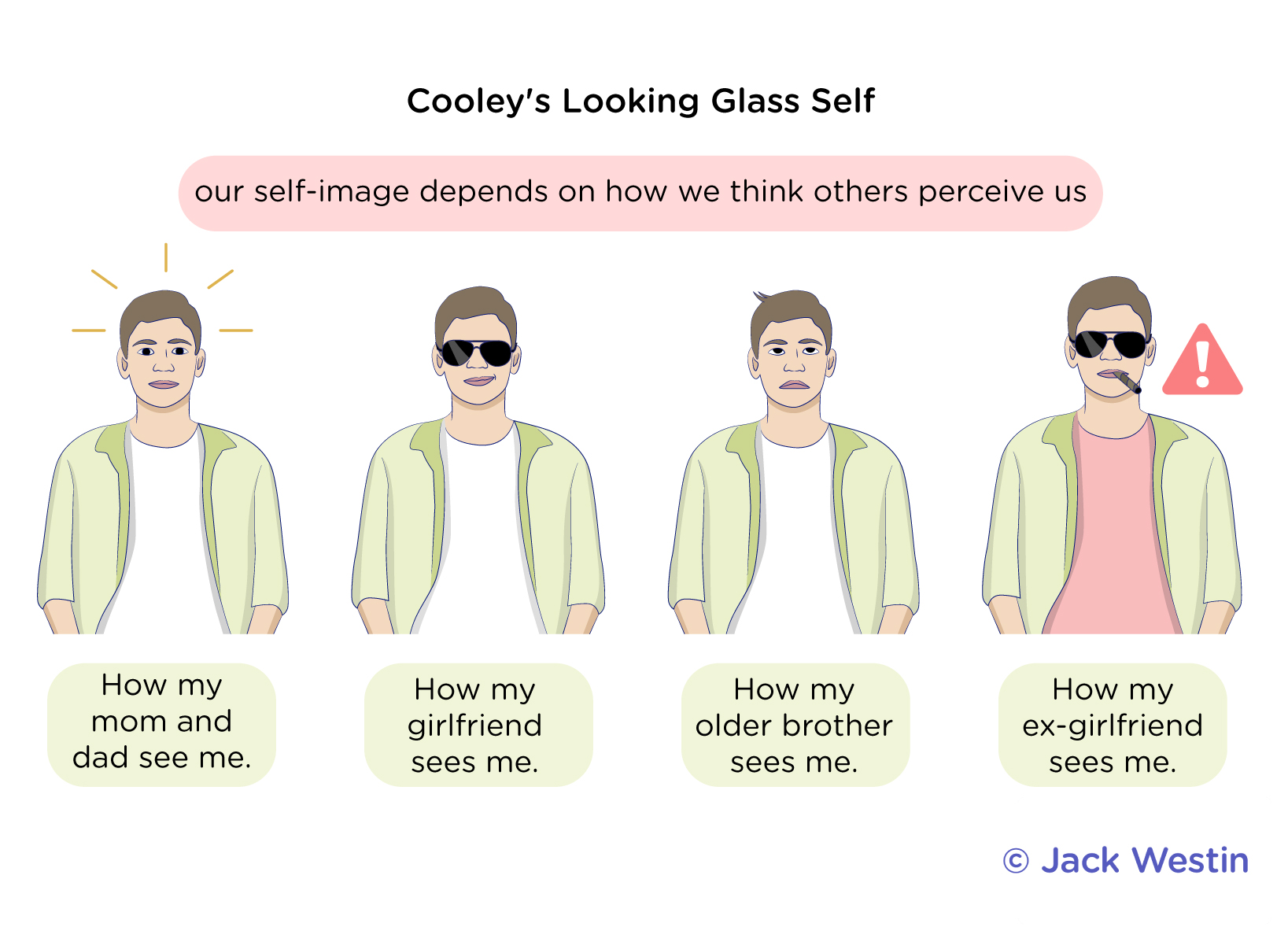
3. Cooley’s Looking-Glass Self (Self-Concept from Social Perception)
We see ourselves based on how we think others see us.
Three Steps:
Imagine how we appear to others.
Imagine their judgment of us.
Develop feelings about ourselves based on this perceived judgment.
Example: If people treat you as smart, you start seeing yourself as intelligent.
4. Meltzoff’s Imitation Theory (Infants Learn by Copying Others)
Even newborns imitate behaviors, showing early social learning.
Key Idea: Imitation helps form self-concept and social identity.
Example: A baby sticking out its tongue after seeing an adult do the same.
MCAT Takeaways:
Erikson → Identity develops throughout life via social conflicts.
Freud → Identity & personality form through childhood psychosexual stages.
Cooley → Self-concept is shaped by how we think others perceive us.
Meltzoff → Imitation plays a key role in early identity development.
Let me know if you need a mnemonic or deeper explanation! 
Describe Kohlberg’s theory of moral development
Kohlberg’s Theory of Moral Development
Kohlberg proposed that moral reasoning develops through three levels, each containing two stages, resulting in six stages total.
1. Preconventional Level (Self-Interest, Young Children)
Stage 1: Obedience & Punishment → Right and wrong are based on avoiding punishment.
Example: “I won’t steal because I don’t want to get in trouble.”
Stage 2: Self-Interest (Instrumental Relativist) → Moral decisions are based on rewards and personal gain.
Example: “I’ll help if I get something in return.”
2. Conventional Level (Social Order, Adolescents & Adults)
Stage 3: Interpersonal Accord (“Good Boy/Good Girl”) → Right and wrong are based on seeking approval and maintaining relationships.
Example: “I’ll be honest because I want people to like me.”
Stage 4: Law & Order → Morality is based on following rules and maintaining social order.
Example: “Stealing is wrong because laws must be followed.”
3. Postconventional Level (Abstract Ethics, Some Adults)
Stage 5: Social Contract → Laws should be followed, but can be questioned if they violate rights or justice.
Example: “Laws should protect people, but unfair laws should be changed.”
Stage 6: Universal Ethical Principles → Morality is guided by internal ethical principles, even if they conflict with laws.
Example: “I would break an unjust law to uphold human rights.”
MCAT Takeaways:
Preconventional → Self-focused (Avoid punishment, seek reward).
Conventional → Society-focused (Follow rules, seek approval).
Postconventional → Ethics-focused (Justice > Laws).
What are the six major PERSONALITY theories, their key proponents, assumptions, overall view, assessment methods, and an example of each?
1. Psychoanalytic Theory
Key Proponent: Sigmund Freud
Assumptions: Personality is shaped by unconscious conflicts and childhood experiences.
View of Personality: The id (pleasure-driven), ego (rational), and superego (moral) interact to create behavior. Unresolved conflicts lead to defense mechanisms.
Assessment Methods: Projective tests like the Rorschach inkblot test or Thematic Apperception Test (TAT) to uncover unconscious motives.
Example: A person with repressed childhood trauma develops an anxious or avoidant personality.
Unconscious mental life and the results of the ID/ego/superego struggle = personality
2. Humanistic Theory
Key Proponents: Carl Rogers, Abraham Maslow
Assumptions: People have free will and an innate drive toward self-actualization.
View of Personality: Personality is shaped by self-concept and the presence of unconditional positive regard.
Assessment Methods: Self-report questionnaires and interviews focusing on self-perception.
Example: A person raised with unconditional love and support develops high self-esteem and confidence.
Free will actions to improve self = personality
3. Trait Theory
Key Proponents: Gordon Allport, Raymond Cattell, Hans Eysenck
Assumptions: Personality is made up of stable traits that can be measured and categorized.
View of Personality: Traits exist on a continuum and influence behavior across situations.
Assessment Methods: Personality inventories like the Big Five (OCEAN) test or 16 Personality Factors (16PF).
Example: A person high in extraversion enjoys social interactions and thrives in leadership roles.
Categorizable traits = personality
4. Social-Cognitive Theory
Key Proponent: Albert Bandura
Assumptions: Personality is shaped by observational learning, cognitive processes, and environment (reciprocal determinism).
View of Personality: Personality develops through interactions between personal factors, behavior, and social influences.
Assessment Methods: Observation-based assessments and self-efficacy tests.
Example: A child who watches their parent handle stress calmly learns to do the same.
4 Stages of Observational Learning According to Albert BanduraAttention: Observer must pay attention to behavior in environment
Memory: Observer must REMEMBER how to perform observed behavior
Motor Capability: Observer must be physically capable of performing action
Motivation: Observer must be motivated to perform the learned behavior
Interplay between personal choice and environment influences behavior = personality
5. Behavioral Theory
Key Proponents: B.F. Skinner, John Watson
Assumptions: Personality is learned through conditioning (rewards, punishments, and reinforcement).
View of Personality: There is no innate personality—it is shaped by environmental stimuli.
Assessment Methods: Behavioral observation and controlled experiments (e.g., Skinner boxes, operant conditioning studies).
Example: A child praised for politeness develops a kind and considerate personality.
CONDITIONED behavior = personality
6. Biological Theory
Key Proponents: Hans Eysenck, Jeffrey Gray
Assumptions: Personality is influenced by genetics and neurobiology.
View of Personality: Certain traits (e.g., extraversion, neuroticism) are heritable and linked to brain structures and neurotransmitters.
Assessment Methods: Twin studies, genetic research, neuroimaging (fMRI, PET scans).
Example: A person with a naturally low dopamine response may seek excitement and be highly extraverted.
GENES = Personality
MCAT Takeaways:
Psychoanalytic → Unconscious conflicts (Freud).
Humanistic → Free will, self-actualization (Rogers, Maslow).
Trait → Stable personality traits (Allport, Cattell, Eysenck).
Social-Cognitive → Learned behavior & environment (Bandura).
Behavioral → Personality is shaped by rewards/punishments (Skinner, Watson).
Biological → Genetics & brain chemistry influence personality (Eysenck, Gray).
What is attachment theory as proposed by Mary Ainsworth?
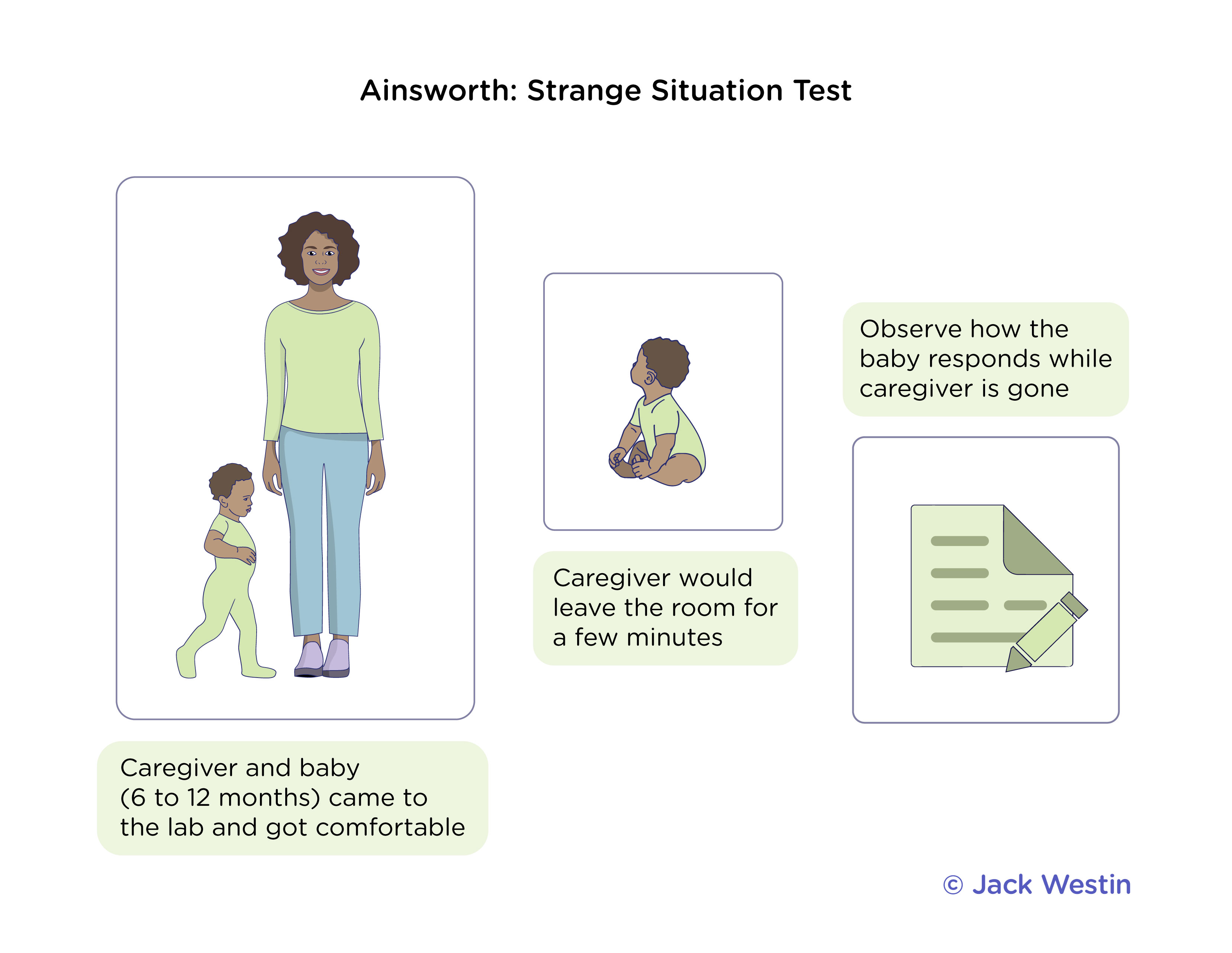
Attachment Theory (Mary Ainsworth)
Mary Ainsworth expanded on John Bowlby’s attachment theory by studying how infants form emotional bonds with caregivers. She identified four attachment styles based on the "Strange Situation" experiment, where a child’s reaction to separation and reunion with their caregiver was observed.
A CHILD REQUIRES ATTACHMENT TO AT LEAST ONE CAREGIVER FOR SUCCESSFUL SOCIAL AND EMOTIONAL DEVELOPMENT
Strange Situation Experiment
Ainsworth’s experiment involved a mother, an infant (12-18 months), and a stranger in a controlled setting with eight episodes of separation and reunion. The child’s responses were used to classify their attachment style.
Secure Attachment → The child is distressed when the caregiver leaves but is quickly comforted upon return.
Example: A baby cries when their mom leaves but calms down when she returns and seeks comfort.
Insecure-Avoidant Attachment → The child is indifferent to both the caregiver's departure and return, avoiding contact.
Example: A baby shows little reaction when their mother leaves or returns, avoiding eye contact.
Insecure-Ambivalent (Resistant) Attachment → The child is extremely distressed when the caregiver leaves and remains upset, even when comfort is offered.
Example: A baby cries when their mom leaves, but when she returns, they resist being comforted.
Disorganized Attachment → The child exhibits confused, fearful, or erratic behavior, often due to inconsistent caregiving (e.g., neglect or trauma).
Example: A baby seems fearful of their caregiver and shows mixed signals (approaching but then pulling away).
MCAT Takeaways:
Secure attachment → Healthy emotional bonds; confident in caregiver’s return.
Insecure attachments → Can lead to anxiety, avoidance, or disorganized behavior in relationships.
Strange Situation → Used to assess attachment styles in infants
What is fertility rate, population momentum, and fecundity?
Key Population Terms for the MCAT
Fertility Rate → TOTAL NUMBER OF CHILDREN BORN DIVIDED BY POPULATION SIZE OF WOMEN IN THEIR REPRODUCTIVE YEARS OVER A GIVEN TIME PERIOD
Example: A fertility rate of 2.1 (replacement level) is needed to keep a population stable without immigration.
THUS, population momentum can be attributed to increases in the number of women of reproductive age because as they increase in number the population still grows but if they don’t give birth then that is lowering fertility rate
Population Momentum → The tendency of a population to continue growing despite a drop in fertility rates due to a large proportion of young individuals who will still have children.
Example: Even if a country lowers its birth rate, its population may still grow for decades due to many young people entering reproductive age.
Fecundity → The biological potential to reproduce, referring to the maximum possible number of children a woman could have under ideal conditions.
Example: A woman’s fecundity may decline with age, even if fertility rates remain high in a population.
What is dependency ratio?
Dependency Ratio (MCAT Definition)
The dependency ratio of a population is the ratio of unemployed individuals to employed individuals within a population
INCREASES in ratio when:
Size of population outpaces # of available jobs
# of available jobs decreases
# of working age individuals decreases
In population momentum, population size is INCREASING meaning more children are being born that are not yet old enough to work meaning that fraction of population who is part of labor force will DECREASE thus causing dependency ratio to further INCREASE
Formula:
Dependency Ratio= # of dependents (minors and seniors)/ # of working age individuals
MCAT Relevance:
High dependency ratio → Greater strain on workers due to increased social and healthcare costs.
Low dependency ratio → More workers supporting fewer dependents, which can boost economic productivity.
What are some prominent populational trends and theories?
1. Preventative Check (Malthusian Theory)
Definition: A factor that prevents overpopulation by limiting birth rates, such as moral restraint, delayed marriage, or family planning.
Example: In societies with access to contraception or cultural norms favoring smaller families, birth rates decrease, thus preventing population explosion.
2. Positive Check (Malthusian Theory)
Definition: A factor that increases death rates when population growth exceeds resources, such as famine, disease, or war.
Example: In history, the Black Death in Europe (14th century) dramatically decreased the population due to the spread of plague, which acted as a positive check on population growth.
3. Demographic Transition
Definition: The shift from high birth and death rates to low birth and death rates as a country industrializes and develops economically.
Example: Japan and South Korea went through a demographic transition, where initially high birth and death rates were replaced by lower rates due to urbanization, healthcare improvements, and women's empowerment.
4. Malthusian Theory
Definition: The idea that population growth will outstrip food and resource production, leading to starvation and death, unless controlled by preventative or positive checks.
Example: Malthus predicted that unchecked population growth would lead to widespread poverty and famine, though modern technological advancements (e.g., agricultural innovations) have prevented this to some extent.
MCAT Takeaways:
Preventative Check → Limits birth rates (family planning).
Positive Check → Increases death rates (famine, disease).
Demographic Transition → Population shifts from high birth/death rates to low ones with development.
Malthusian Theory → Population grows faster than resources, leading to crises unless checks occur.
List out Jean PIaget’s Stages of his Theory of Cognitive Development
1. Sensorimotor Stage
Age: 0–2 years
Key Concepts:
Learning through senses and movement
No mental representation yet (early on)
Object permanence develops (things still exist even if not seen)
Stranger anxiety may begin
MCAT Tip:
Object permanence is the hallmark milestone.
2. Preoperational Stage
Age: 2–7 years
Key Concepts:
Development of symbolic thinking (use of words, images)
Pretend play
Egocentrism (can’t take another’s point of view)
Centration (focus on one aspect of a situation)
MCAT Tip:
No understanding of conservation (e.g., pouring water into different shaped glasses — they think amount changes)
3. Concrete Operational Stage
Age: 7–11 years
Key Concepts:
Can think logically about concrete events
Conservation develops (understands quantity doesn’t change with shape)
Mathematical operations understood
Loss of egocentrism
MCAT Tip:
Conservation is the hallmark milestone. Kids can do basic logic, but only with concrete (real) objects.
4. Formal Operational Stage
Age: 12+ years
Key Concepts:
Abstract reasoning
Hypothetical thinking (what if...?)
Moral reasoning emerges
MCAT Tip:
Teens in this stage can use logic without concrete objects.
What is kinesthetic sense?
What does totipotent refer to?
What Is Kinesthetic Sense?
Definition: The ability to sense the position and movement of your body parts through receptors in muscles, tendons, and joints.
It tells you where your limbs are without looking at them.
Also called proprioception (though some sources use “proprioception” more broadly to include balance and spatial awareness).
Totipotent
Referring to stem cells capable of giving rise to any cell type or a complete embryo
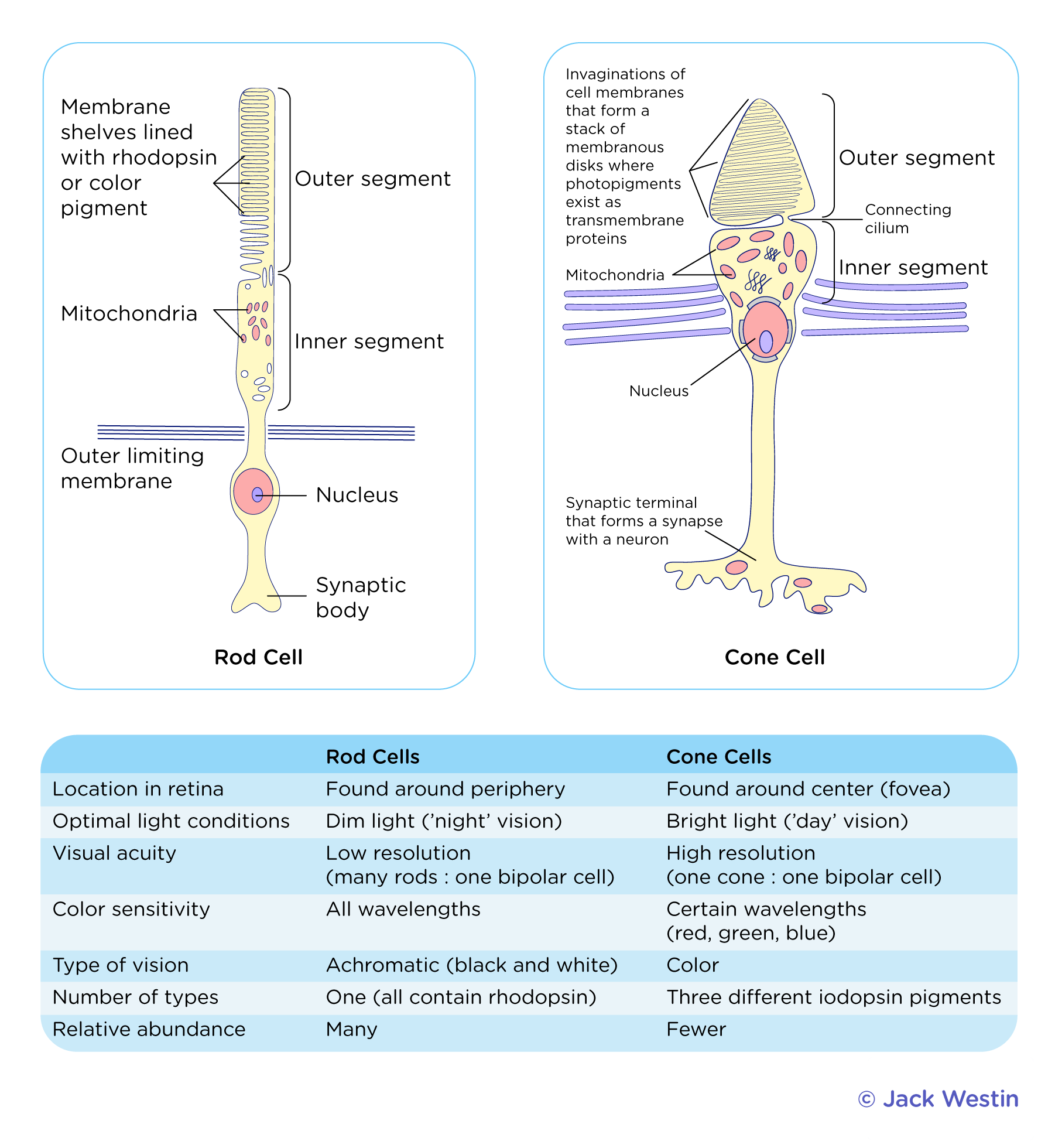
Compare and contrast vision as it pertains to rods and cones
Rods:
Highly photosensitive and densely clustered around the PERIPHERY of the retina outside the fovea
Achromatic: Black and White
ONE TYPE: All contain Rhodopsin
MORE rods than cones
Cones:
Concentrated in the FOVEA in the CENTER of the retina and are lowly photosensitive
There are THREE different iodopsin pgiments, each responsible for detecting one of three frequency bands or colors of light:
Red
Green
Blue
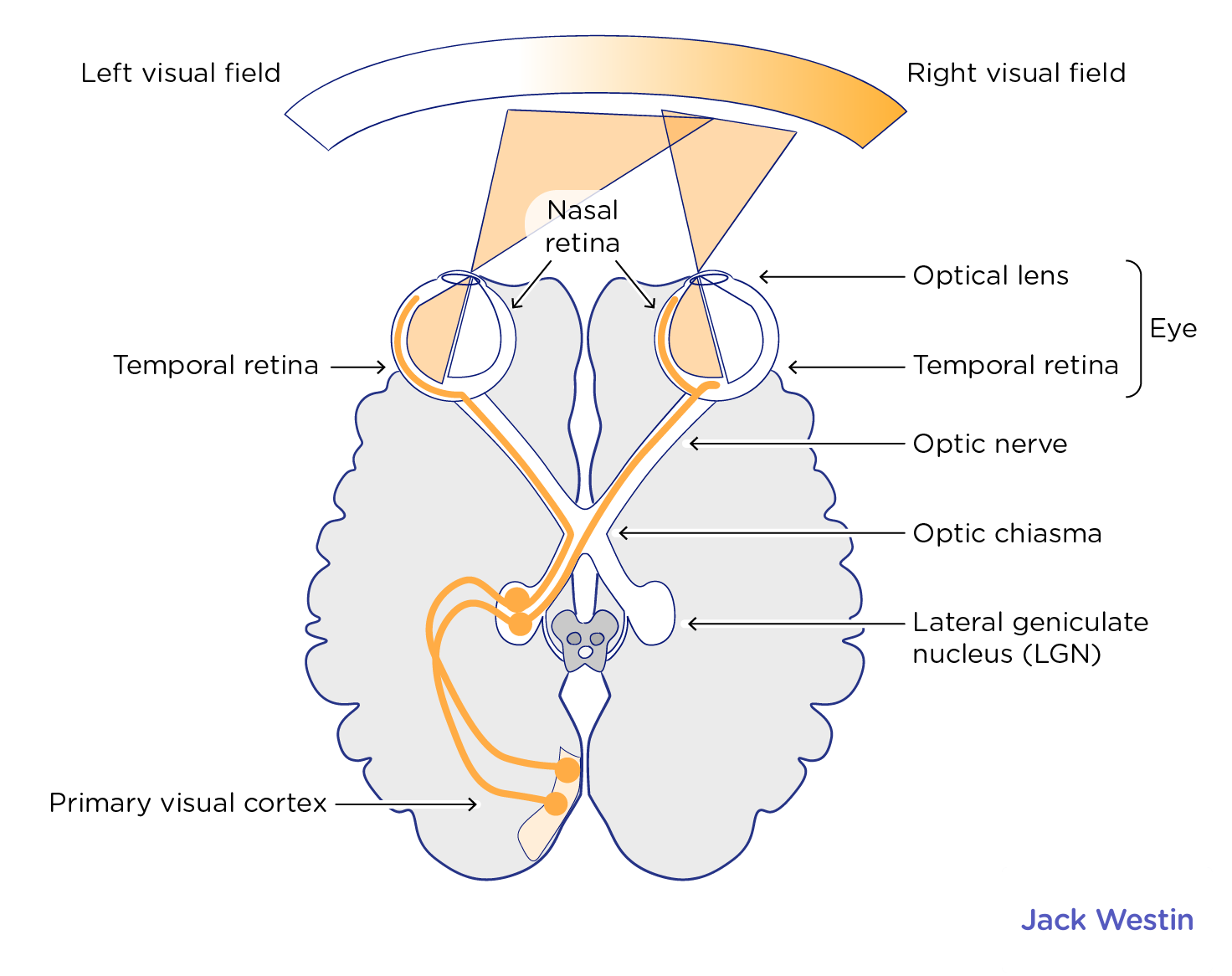
How is visual data collected?
Visual information is collected from the left-and-right visual fields in a CONTRALATERAL MANNER
Both eyes can pick up visual information from BOTH the L+ R visual fields, PROCESSING however is contralateral
Data from the RIGHT visual field will be processed by the LEFT temporal retina which will be processed by LEFT hemisphere and vice versa
Light that hits Nasal Retina is Processed CONTRALATERALLY
Light from RIGHT side of visual field strikes RIGHT nasal retina
Information from RIGHT nasal retina (same side of retina as nose) will cross at optic chiasm to opposite side
Will be processed by LEFT occipital lobe
Light that hits Temporal Retina is Processed IPSILATERALLY
Light from RIGHT side of visual field strikes LEFT temporal retina
Information from the LEFT temporal retina (same side of retina as ear) DOES NOT cross at optic chiasm
Will pass through optic nerve staying at same side through optic chiasm to the LEFT occipital lobe
THIS IS BECAUSE MEDIAL FIBERS (closer to center, like nasal) CROSS WHILE LATERAL FIBERS (further from center, like temporal) STAY ON THEIR SIDE THROUGH THE OPTIC CHIASM
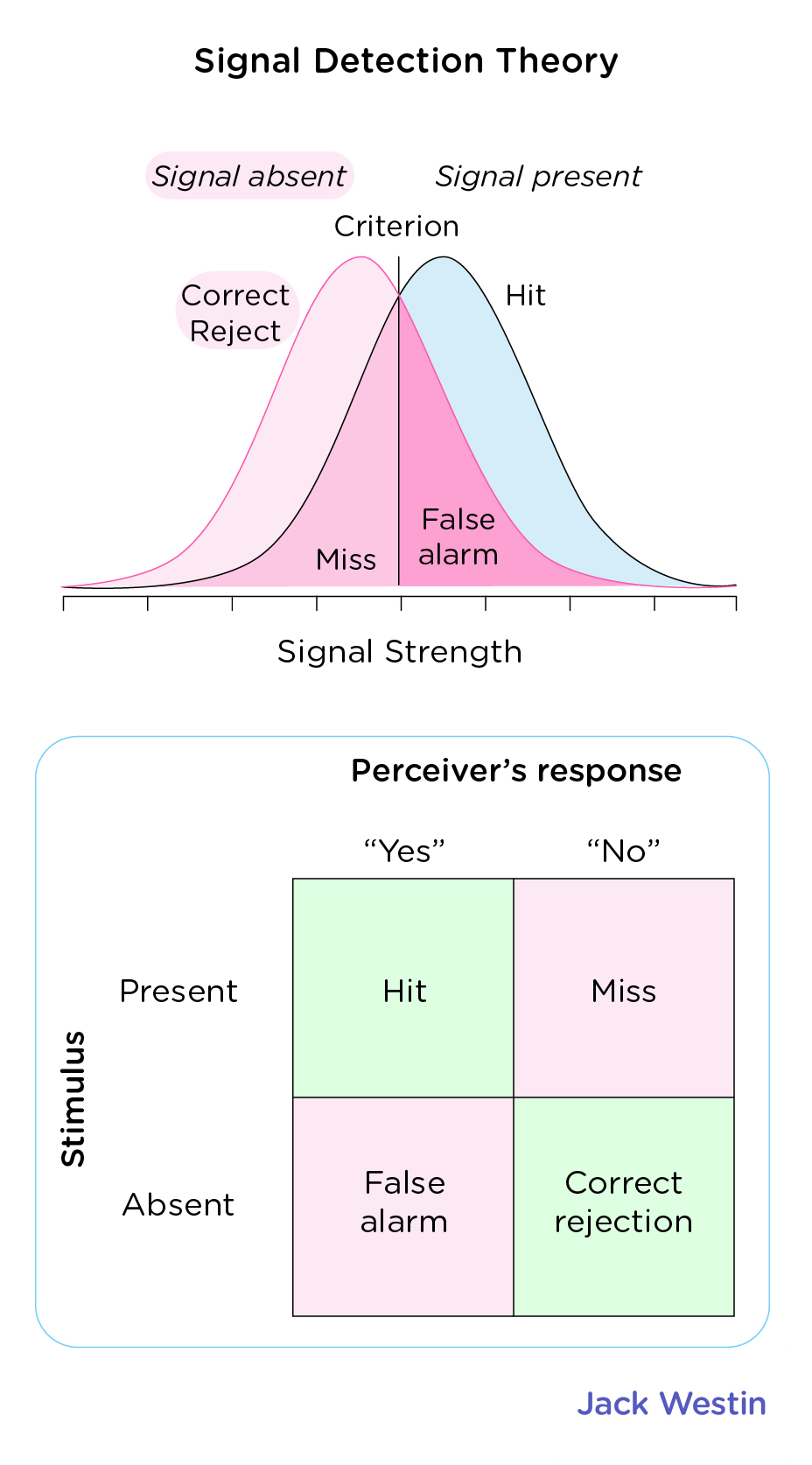
What is Signal Detection Theory?
Signal Detection Theory
Describes whether stimuli have been correctly perceived as present or absent
Signal: Actual stimulus you’re trying to detect
Noise: Background information or distractions that could interfere with distraction
POSSIBILITIES:
Hit: Signal is PRESENT and DETECTED (true positive)
False Alarm: Signal is ABSENT but DETECTED (false positive)
Miss: Signal is PRESENT but MISSED (false negative)
Correct Rejection: Signal is ABSENT and MISSED (true negative)
PICTURED CURVE: Receiver Operating Characteristic (ROC) Curve
Helps visualize sensitivity independent of criterion
d’=sensitivity=how well you tell signal from noise
Beta or c=decision criterion=your personal bias or threshold
What do insulin, glucagon, somatostatin, and aldosterone stimulate; respectively?
Insulin
Decreases blood sugar levels by prompting cells to take up glucose
Stimulates glycogenesis in liver and muscles
Promotes conversion of excess glucose into fatty acids for storage as adipose tissue in the liver (lipogenesis)
INHIBITS breakdown of stores glycogen (glycogenolysis) and gluconeogenesis
PROMOTES protein synthesis
Glucagon
Increases blood sugar levels by prompting glucose release
Gluconeogenesis in liver where glucose is synthesized from non-carbohydrate biomolecules like amino acids and lactates
Glycogenolysis, breaking down glycogen and liberating it into blood stream
Prompts BETA-OXIDATION of fatty acids into acetyl-CoA primarily in liver
Somatostatin
Secreted by delta cells of the pancreas concurrently with insulin and produces a predominantly INHIBITORY EFFECT across different systems
Inhibits GI, endocrine, exocrine, pancreatic, and pituitary secretions
Such as GH, TSH, prolactin, gastrin, secretin, insulin, and glucagon
Aldosterone
Released from adrenal gland in response to low blood volume, blood pressure, or sodium levels.
Activates mineralocorticoid receptors in various tissues
In the KIDNEY, aldosterone acts on the cells of the distal tubules and collecting ducts triggering a signal that causes sodium REABSORPTION and potassium EXCRETION
Promotes WATER REABSORPTION increasing blood volume and pressure
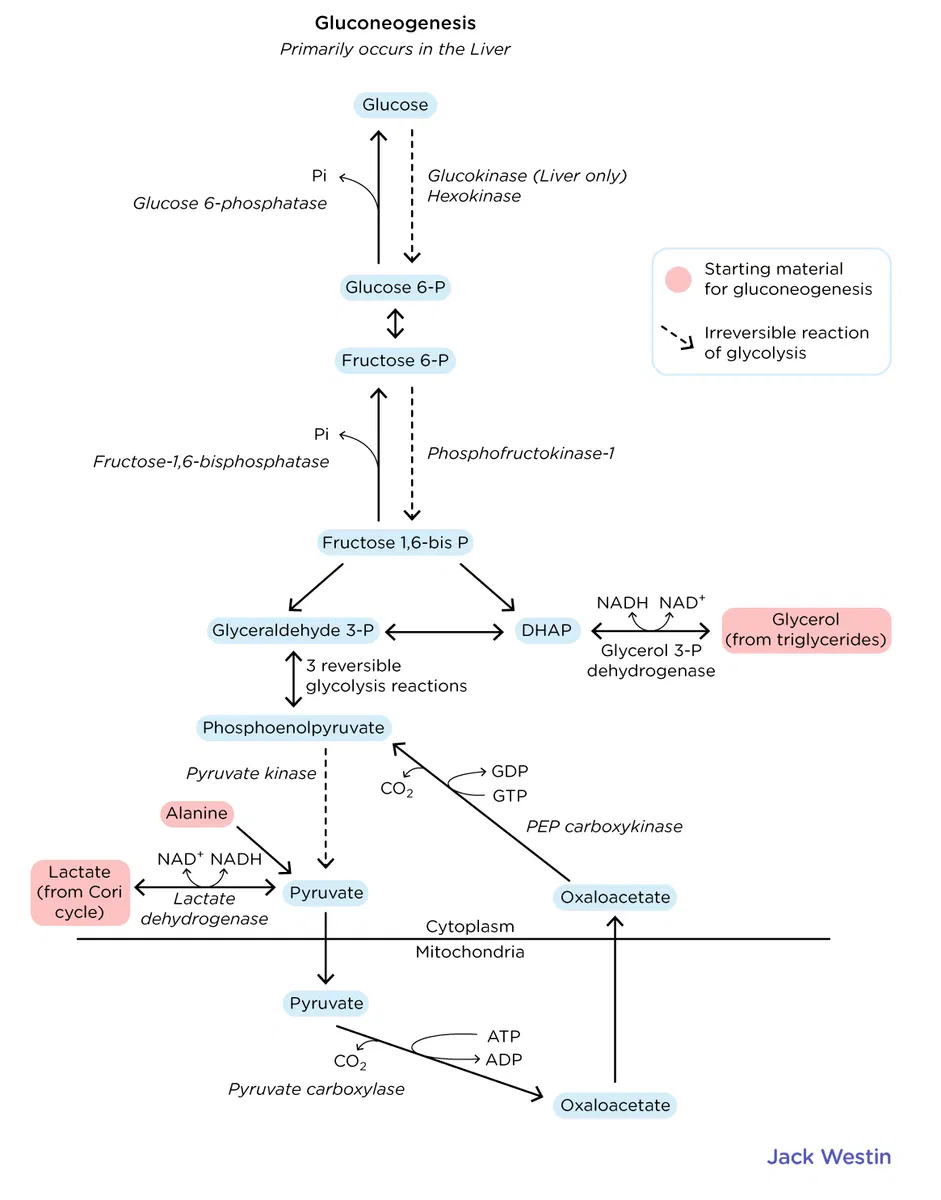
What is the importance of phosphoenolpyruvate carboxykinase (PEPCK)?
It is an important enzyme for GLUCONEOGENESIS
In low blood glucose levels, glucagon stimulates glucose production from NON-CARB substrates like LACTATE
The steps for gluconeogenesis are essentially the same as those for glycolysis EXCEPT for the three irreversible steps of
Hexokinase
PFK-1
Pyruvate Kinase
If PEPCK is nonfunctioning, gluconeogenesis will NOT occur leading to the build-up of gluconeogenic substrates like lactate in the blood thus RAISING the acidity of the blood
What is the blood-testis barrier?
Blood-Testes Barrier
Physical barrier between blood vessels and the seminiferous tubules of the testes where sperm production occurs
This barrier prevents antibodies and immune cells from entering the testes in the blood since because sperm are unlike any other cells in the body the immune system could MISTAKENLY TARGET them as foreign cells
Leydic Cells
Produce and release testosterone in the interstitial tissue surrounding the seminiferous tubules
What are the differences between displacement, projection, reaction formation
Projection
Fault lies WITHIN you but is by you to avoid blame
Defense mechanism in which a threatening urge or quality (e.g., affect, responsibility) is ascribed to others rather than to oneself.
You are stupid so you call others stupid
Displacement
The fault lies OUTSIDE of you but is shifted by you to DISPLACE blame
Defense mechanism in which an individual discharges tensions by taking them out on a less threatening target.
A student who is angry with her professor takes it out on her very understanding boyfriend because it avoids the anxiety that would arise from attacking her professor
Reaction Formation
Defense mechanism where OPPOSITE of true feelings are expressed sometimes to exaggerated degree
A man who feels overly gay may act overly MASCULINE
A drug addicted woman may EXTOL reacthe virtues of ABSTINENCE
Very stressed about the MCAT yet approach it CALMLY
Sublimation
Channeling unwanted/unhealthy desires into something that is accepted by society
Working out when you’re angry at someone
Becoming a surgeon because you like to mutilate people
What are the two types of immunity that exist?
Active Immunity
When our own immune system is responsible for a pathogen
Passive Immunity
When we are protected from a pathogen by immunity gained from someone else
What are the different types of conditioning?
Operant Conditioning: Defined by CONSEQUENCES
Punishment: Decrease undesirable behavior
POSITIVE: Introduces consequence to deter behavior
NEGATIVE: Takes something away to deter behavior
Reinforcement: Increase desirable behavior
POSITIVE: Reward to encourage behavior
NEGATIVE: Take away negative to encourage behavior
Classical Conditioning: Defined by ASSOCIATION
A neutral stimulus becomes associated with an unconditioned stimulus, eventually triggering a conditioned response.
What is Weber’s Ideal Bureaucracy? What are vertical and horizontal mobility?
Weber’s Ideal Bureaucracy
Formal Selection: Employment based on TECHNICAL qualifications
Formal Rules: Employees follow STANDARD operating protocol
Impersonality: Protocol is IMPERSONAL, same hierarchy same rulez
Career Orientation: Follow the rules, stay. Break them, ur FIRED
Division of Labor: Each position has a clear job description. Employees don’t take up a variety of tasks
Hierarchy: Only big dawgs at the top call the shots and make decisions; NO EMPLOYEE CONSENSUS
Horizontal Mobility
Definition: A change in occupation or role without a change in social class or status.
Key Idea: Lateral movement; same socioeconomic level, just a different position.
Example: A schoolteacher becomes a police officer — different job, but same social class.
MCAT Tip: Think of horizontal = sideways movement in society.
Vertical Mobility
Definition: A change in a person's social class, either upward or downward.
Key Idea: Movement up or down the socioeconomic ladder.
Example (Upward): A factory worker earns a medical degree and becomes a doctor.
Example (Downward): A corporate executive loses their job and becomes unemployed.
MCAT Tip: Vertical = change in status or income level.
MCAT Takeaway:
Horizontal mobility = same class, different role
Vertical mobility = change in class (up or down)
What is the life course approach? What is the front stage self v. looking glass self?
Life Course Approach
Definition: A perspective that considers how early life experiences (biological, psychological, social) influence health outcomes and behaviors across a person’s entire life.
Focus: Long-term effects of childhood, family, education, socioeconomic status, trauma, etc.
MCAT Angle: Health is shaped not just by current status, but by cumulative life experiences over time.
Example: A child growing up in poverty may have poorer health in adulthood due to chronic stress and limited healthcare access.
Life course approach = long-term, whole-life view of health/behavior
Front Stage Self (from Goffman’s dramaturgical theory)
Definition: The persona you intentionally perform in social settings, where you're being watched and judged.
Behavior: Polished, controlled, socially acceptable.
Example: Acting professional during a job interview, even if you’re nervous or tired.
Front stage self = your “performance” in public
Looking Glass Self (from Cooley)
Definition: The idea that our self-concept develops through how we believe others perceive us.
Process:
We imagine how others see us
We imagine how they judge us
We develop feelings about ourselves based on that imagined judgment
Example: A teen thinks others see them as awkward, so they start to view themselves as awkward.
Hawthorne Effect
Definition: People change their behavior when they know they’re being observed.
MCAT Relevance: Important in research design — can bias results.
Example: Workers become more productive when they know a supervisor is watching, even if working conditions haven't changed.
Social Identity
Definition: The part of your self-concept that comes from belonging to social groups (like race, gender, religion, nationality, occupation).
You define who you are partially based on group membership.
Comes from Social Identity Theory, which includes:
Social categorization (labeling groups),
Social identification (adopting group norms),
Social comparison (comparing in-group vs. out-group).
Example: Someone sees themselves as a “Latina scientist” — blending ethnicity and profession into their identity.
Stereotype Threat
Definition: When someone feels at risk of confirming a negative stereotype about their social group, and this pressure impairs performance.
Often subconscious, and can create anxiety or self-doubt.
Example: A woman underperforms on a math test after being reminded of the stereotype that “women are bad at math.”
Self-Fulfilling Prophecy
Definition: A belief or expectation that influences behavior, causing it to become true.
Can be based on others’ expectations or your own.
Example: A teacher expects a student to fail, so they give them less attention → the student performs poorly → confirming the original expectation.
Social identity = how you define yourself based on group membership.
Stereotype threat = internalized fear of fulfilling a negative group stereotype.
Self-fulfilling prophecy = expectations lead to behavior that makes the expectation come true.
What is the Elaboration Likelihood Model (ELM)?
Elaboration Likeihood Model (ELM)
Explains how attitudes are formed and changed through persuasion.
Focuses on how deeply a message is processed based on motivation and ability.
Central Route
Involves deep, careful thinking about the content of the message.
Used when a person is motivated and has the ability to focus.
Leads to stronger, more lasting attitude changes.
Example: A student changes their opinion on a health topic after reading well-reasoned scientific evidence.
Peripheral Route
Involves shallow processing of cues that aren't directly related to the message's content (like tone, appearance, or emotion).
Used when a person is not motivated or lacks the ability to pay close attention.
Leads to more temporary or superficial attitude change.
Example: Someone buys a product because a celebrity endorses it, not because they evaluated its benefits.
Central route = logic, evidence, deep thinking
Peripheral route = emotion, popularity, superficial cues
The route taken depends on the listener's motivation and ability to process the message.
What is cortical activity?
Cortical Activity
Cortical activity refers to the electrical and functional activity of the cerebral cortex — the outermost layer of the brain responsible for higher-level processing.
Cortical Lobes and Their Functions (Know These!):
Frontal lobe: decision-making, planning, motor control, personality
Parietal lobe: touch, spatial processing
Temporal lobe: auditory processing, memory, language
Occipital lobe: vision
Context Where MCAT Mentions Cortical Activity:
EEG & Sleep:
Different sleep stages show different patterns of cortical activity (e.g., beta waves = alertness, delta = deep sleep)
Consciousness:
Higher cortical activity = wakefulness or REM sleep
Lower cortical activity = deep sleep, coma
Sensory Processing:
Sensory info from eyes, ears, etc., is ultimately processed in specific cortical regions
Motor Function:
Primary motor cortex in frontal lobe controls voluntary movement
Somatosensory cortex in parietal lobe processes touch
Cortical activity refers to the brain's processing power for conscious awareness, perception, and voluntary behavior. It varies across sleep stages and is central to sensation, movement, and higher thinking.
What are the two types of deafness and how do they come about?
1. Conduction Deafness (Conductive Hearing Loss)
Definition: A problem with conducting sound waves from the outer ear to the inner ear (cochlea).
Cause: Physical blockage or damage to the outer or middle ear.
Examples:
Earwax buildup (cerumen impaction)
Ruptured eardrum
Otitis media (middle ear infection)
Damage to ossicles (malleus, incus, stapes)
Treatment: Often treatable with medication or surgery (e.g., hearing aids, ear tubes)
2. Sensorineural Deafness (Sensorineural Hearing Loss)
Definition: A problem with the inner ear (cochlea) or the auditory nerve (cranial nerve VIII).
Cause: Damage to hair cells in the cochlea or the auditory nerve itself.
Examples:
Aging (presbycusis)
Loud noise exposure
Certain drugs (ototoxic)
Genetic conditions or congenital defects
Treatment: Often permanent; cochlear implants may help in severe cases.
Conduction = mechanical/outer or middle ear
Sensorineural = nerve/inner ear
Different causes, different treatments
Rinne and Weber tests can help distinguish between them
Rinne Test:
Compares air conduction to bone conduction of sound using a tuning fork; in normal hearing, air conduction is greater than bone conduction (AC > BC).
Weber Test:
Places a tuning fork on the forehead to see if sound lateralizes (is heard more in one ear); helps distinguish between sensorineural and conductive hearing loss.
What are the big 5 OCEAN personality traits?
Big Five Personality Traits (OCEAN)
These are the five major dimensions of personality used in trait theory:
Openness to Experience
Imagination, creativity, willingness to try new things
High = curious, open-minded
Low = conventional, routine-loving
Conscientiousness
Organization, discipline, responsibility
High = dependable, careful
Low = careless, disorganized
Extraversion
Sociability, energy from social interaction
High = outgoing, talkative
Low = reserved, quiet
Agreeableness
Compassion, cooperation, kindness
High = warm, helpful
Low = antagonistic, suspicious, uncooperative
Neuroticism
Emotional stability vs. tendency toward negative emotions
High = anxious, moody
Low = emotionally stable, calm
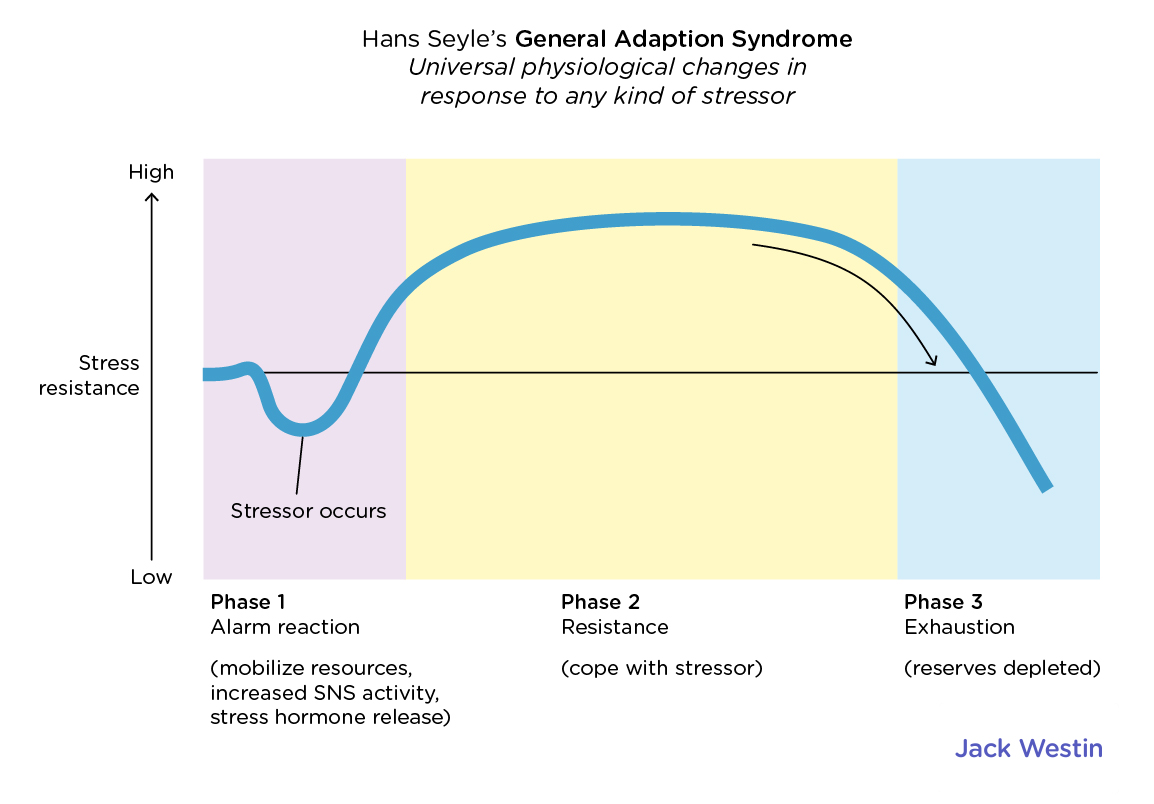
What is the General Adaptation Syndrome?
General Adaptation Syndrome
Hans Selye postulated the General Adaptation Syndrome, describing the body's UNIVERSAL response to stress in three stages: alarm, resistance, and exhaustion
GAS describes how the body responds over time to sustained stress — initially rising to the challenge, adapting, and eventually breaking down if the stress continues too long.
Three Stages of GAS (BIOLOGICAL PERPECTIVE)
Alarm Stage
Initial reaction to the stressor
Fight-or-flight response: adrenaline and cortisol released
Increased heart rate, energy, alertness
Resistance Stage
Body tries to adapt to the stressor
Prolonged release of stress hormones (like cortisol)
Body remains alert but begins to wear down
Exhaustion Stage
Body’s resources become depleted
Increased risk of illness, fatigue, burnout, and other health issues
Example of GAS: College Student Facing Final Exams Alarm Stage:
The student finds out they have 3 final exams in 2 days.
ALARM REACTION (mobilize resources)
→ Immediate stress response kicks in: heart rate increases, adrenaline and cortisol are released.
→ Fight-or-flight mode: they feel alert, anxious, and jittery.
RESISTANCE STAGE (cope with stressor)
Over the next week, the student stays up late studying, drinks lots of coffee, and pushes through the stress.
→ The body adapts to the stress, but cortisol remains elevated.
→ They stay focused but start feeling irritable and tired.
EXHAUSTION STAGE (reserves depleted)
After finals are over, the student crashes.
→ Their immune system is weakened, and they catch a cold.
→ They feel mentally and physically drained — classic signs of burnout.
What is the difference between educational segregation and educational stratification?
Educational segregation is when different areas that are physically separated have UNEQUAL educational resources and facilities and that social stratification is when we group people in different hierarchical categories based on their education level and view and treat them differently based off how educated they are.
What are the three types of stress to know?
Eustress
Positive stress that enhances motivation, performance, and focus.
Helps with personal growth, resilience, and goal achievement.
Generally short-term and perceived as within one’s coping abilities.
EXAMPLE: Associated with beneficial challenges like exams, competitions, or public speaking.
Neustress
Neutral stress that does not directly affect the individual emotionally or physically.
Often results from information that is perceived as irrelevant or non-threatening.
Does not trigger a significant physiological stress response.
Example: hearing about a natural disaster in a distant country with no personal connection.
Distress
Negative stress that can impair functioning and well-being.
Can be acute (short-term crisis) or chronic (ongoing pressure or trauma).
Often leads to anxiety, decreased performance, and physical health issues.
Occurs when demands exceed coping resources.
Example: Failing an important exam despite weeks of studying, leading to feelings of hopelessness and anxiety.
Difference between moderating, mediating, confounding, and continuous variable with definition and example each:
Moderating Variable
Definition:
A variable that affects the STRENGTH or direction of the RELATIONSHIP between an independent and a dependent variable.Example:
The effect of stress on depression depends on social support (moderator).High support weakens the link; low support strengthens it.
Mediating Variable
Definition:
A variable that EXPLAINS the MECHANISMS through which the independent variable affects the dependent variable.Example:
Stress leads to poor sleep, which then leads to depression. The stress impacts depression through sleep.
Confounding Variable
Definition:
A variable that is RELATED to BOTH the independent and dependent variables, potentially giving a FALSE IMPRESSION of their relationship.Example:
People who carry lighters appear to have more lung disease.But SMOKING is the CONFOUNDER—it causes both.
Continuous Variable
Definition:
A continuous variable is a measurable variable that can take on an infinite number of values within a given range, including fractions and decimals.Example:
Person's height is a continuous variable because it can be measured as 170 cm, 170.5 cm, or 170.532 cm—there's no fixed limit to how precisely you can measure it.
Discrete Variable
Definition: A variable that can only take on specific, separate values, usually whole numbers.
Example: Number of siblings (you can have 2, not 2.4).
Ordinal Variable
Definition: A variable with ordered categories, but the intervals between them are not necessarily equal.
Example: Pain scale rating (1 = mild, 2 = moderate, 3 = severe).
COCOS SPICY RATING
Nominal Variable
Definition: A variable that consists of categories with no intrinsic order.
Example: Blood type (A, B, AB, O).
What is the synaptonemal complex?
Synaptonemal Complex
A protein structure that forms between homologous chromosomes during prophase I of meiosis
It physically holds homologs together to allow synapsis (alignment) and crossing over (genetic recombination).
APPEARS specifically during zygotene stage of prophase I.
Structure:
Two lateral elements (along each homolog)
One central element (connecting the homologs)
Resembles a zipper under electron microscopy—because of course chromosomes need formalwear for recombination.
Importance:
Ensures accurate recombination and segregation of homologous chromosomes.
Failure to form properly can result in aneuploidy (like Down syndrome).
Difference between phosphorylase and phosphatase?
A “phosphatase” takes a phosphate OFF of a substrate, hydrolyzing it to yield phosphoric acid.
ASE, get yer ass on back home chicken bone
A “phosphorylase” puts a phosphate ONTO a substrate, in a special way.
What is a p-value?
What is a p-value?
The probability that the observed results (or more extreme) would occur by chance if the null hypothesis were true.
In plain terms: "How likely is it that what I’m seeing is just a fluke?"
MCAT-Relevant Thresholds
p < 0.05 → Statistically significant (the default threshold)
p < 0.01 → Highly significant (stronger evidence against the null)
p > 0.05 → Not statistically significant (you fail to reject the null)
What cancer genes to know for the MCAT?
p53 (TP53)
Tumor suppressor known as the “guardian of the genome”; activates DNA repair, cell cycle arrest, and apoptosis in response to DNA damage.
Mutated in over 50% of human cancers, leading to uncontrolled cell division.
p21 (CDKN1A)
Activated by p53, inhibits cyclin-CDK complexes → causes G1 cell cycle arrest to allow DNA repair.
Acts as a checkpoint regulator; loss removes brake on cell cycle progression.
BAX
Pro-apoptotic protein from the BCL-2 family; promotes mitochondrial outer membrane permeabilization (MOMP) and cytochrome c release.
Also regulated by p53, helps eliminate cells with irreparable DNA damage.
Retinoblastoma protein (Rb)
Tumor suppressor that inhibits E2F, blocking G1 → S phase transition.
Inactivated by phosphorylation (by CDKs); mutations → loss of cell cycle control, seen in retinoblastoma and other cancers.
BRCA1 / BRCA2
Tumor suppressors involved in homologous recombination repair of double-stranded DNA breaks.
Inherited mutations dramatically increase risk of breast, ovarian, and other cancers.
BCL-2
Anti-apoptotic protein; prevents mitochondrial cytochrome c release and apoptosis.
Overexpression seen in some B-cell lymphomas, helping cancer cells evade death.
MYC
Proto-oncogene that encodes a transcription factor promoting cell growth and proliferation.
Dysregulated in Burkitt lymphoma (t(8;14) translocation).
RAS
Proto-oncogene coding for a GTPase involved in growth factor signaling.
Mutations lock it in active (GTP-bound) form, promoting unchecked proliferation.
APC (Adenomatous Polyposis Coli)
Tumor suppressor that regulates β-catenin in the WNT signaling pathway.
Loss of APC function leads to colon cancer, especially familial adenomatous polyposis (FAP).
MCAT Takeaways
Know p53, Rb, and BRCA for tumor suppression.
Know BCL-2, MYC, RAS as common oncogenes.
Understand their role in cell cycle control, apoptosis, and DNA repair.
What are the different VISUAL CUES to know for the MCAT?
Binocular Cues
Used for depth perception
Retinal Disparity:
Each eye sees a slightly different image.
Eyes are 2.5 inches apart
The brain uses this difference to compute depth.
Convergence:
Eyes turn inward more when looking at close objects.
The degree of inward movement helps estimate distance.
Monocular Cues (require one eye only)
Used for form, depth, motion, and constancy
Form & Depth:
Relative Size:
Closer objects appear larger.
Interposition (Overlap):
If object A blocks object B, then A is closer.
Relative Height:
Objects higher in the visual field are seen as farther away.
Shading & Contour:
Use of light and shadow to perceive depth and form.
MOTION PARALLAX
Things further away move SLOWER
Perceptual Constancy (brain corrections to maintain consistency) ; our perception of object doesn’t change even if it looks different on retina
Size Constancy:
Even if an object moves closer or farther, we perceive its size as unchanging.
Shape Constancy:
An object rotated at different angles is still perceived as having the same shape.
Color Constancy:
We perceive colors as consistent even under different lighting.
What are the facts to know on SENSORY ADAPTATION for the MCAT?
Sensory Adaptation (MCAT Scope)
Definition:
A decrease in responsiveness of sensory receptors to a constant stimulus over time.
1. Hearing (CONTRACT WHEN LOUD)
Inner ear muscle (stapedius) contracts in response to LOUD sounds.
Purpose: dampen vibrations to protect the inner ear.
Takes time to engage → can't protect from sudden sounds like a gunshot.
Works better for sustained loud noises (e.g., loud music).
2. Touch (DESENSITIZE OVER TIME)
Continuous pressure (e.g., wearing clothes, holding a cup) becomes less noticeable over time.
Mechanoreceptors fire less as stimulus continues → adaptation.
3. Smell (DESENSITIZE TO MOLECULES):
Strong smells (e.g., perfume, garbage) become less intense after prolonged exposure.
Olfactory receptors reduce firing → sensory adaptation.
4. Proprioception (YOUR MIND FLIPS)
Your body's awareness of its position in space.
Adaptation example: Being upside down for a prolonged time may adjust your internal sense of "upright."
5. Sight (UPREGULATION IN DARK, DESENS IN LIGHT):
Light adaptation: In bright light, rods and cones desensitize to prevent overstimulation.
Dark adaptation: In low light, rhodopsin regenerates in rods → increased sensitivity to light.
Key MCAT Takeaways
Sensory adaptation = decreased receptor response over time
Inner ear muscle contracts to protect from loud noise, but not sudden ones
Touch and smell fade with constant exposure
Vision adapts to light levels by up/down-regulating sensitivity
Proprioception adjusts to unusual body positions
What is Weber’s Law in terms of what needs to be known for the MCAT?
Just Noticeable Difference (JND/ΔI)
Definition: The smallest change in stimulus intensity that a person can detect 50% of the time.
Example: If you’re holding a 100g weight, and you can only detect a difference when 5g is added, the JND is 5g.
Background Intensity (I)
Definition: The initial stimulus level you're starting from (also called baseline or original intensity).
Example: If you’re lifting a 100g weight, then 100g = background intensity.
Weber’s Law (K * Original Intensity = JND Amount)
Definition: The ratio of the JND to the original stimulus is constant:
Weber’s Constant/K = ΔI/I
ΔI: Just noticeable difference/JND
I: Original intensity
Example:
If you can detect a 5g difference at 100g, what is the JND at 200g?
K=5g/100g=0.05
K x Original Intensity = JND, so
100 × 0.05 = 5 g
200 × 0.05 = 10 g
What is the difference between absolute threshold and Weber’s JND?
Absolute threshold = intensity needed to detect a stimulus AT ALL 50% of the time
JND = smallest CHANGE/DIFFERENCE in intensity you can notice between two stimuli
Absolute threshold is about detection, JND is about discrimination
Absolute threshold can be influenced by a # of factors,
ex. Psychological states.
Expectations'
Experience (how familiar you are with it)
Motivation
Alertness
Subliminal stimuli – stimuli below the absolute threshold.
What do you need to know about the vestibular system for the MCAT?
Vestibular System (MCAT Summary)
Overall Function
Maintains balance and spatial orientation
Located in the inner ear
Main Structures Involved (Inner Ear)
1. Semicircular Canals (for rotational motion)
Three canals, each aligned to one orthogonal plane
X (lateral/horizontal)
Y (posterior)
Z (anterior)
The canals are filled with endolymph (fluid):
When head rotates, endolymph lags behind → bends hair cells
SPEED and DIRECTION of ENDOLYMPH movement tells brain how SPEED and DIRECTION in which the head is turning
2. Otolithic Organs (for LINEAR acceleration & head position)
Utricle = detects horizontal motion (e.g., walking forward)
Saccule = detects vertical motion (e.g., jumping or falling)
These organs contain:
Calcium carbonate crystals (CaCO3 otoliths) attached to hair cells embedded in gel
When you move, crystals shift → drag hair cells
Bending of hair cells triggers action potentials
Nerve Pathway:
Signal from vestibular system is sent via:
Vestibulocochlear nerve (CN VIII) → brainstem → cerebellum, thalamus, and other regions
Common MCAT Clinical Tie-ins:
Vertigo (DISPLACED CaCO3/OTOLITHS)
Caused by displaced otoliths or misfiring of hair cells → brain receives conflicting signals about motion
Results in dizziness, nausea, balance issues
Motion Sickness ((ENDOLYMPH INERTIA, KEEPS MOVING AFTER YOU STOP ROTATING)
Caused when visual input doesn't match vestibular input (e.g., reading in a moving car)
Endolymph keeps moving even after you stop → lingering sense of motion → nausea
Key MCAT Takeaways
Semicircular canals → detect rotational acceleration (endolymph movement)
Utricle (horizontal) and saccule (vertical) → detect linear acceleration & head position
Otoliths (CaCO₃ crystals) drag hair cells when you move → trigger action potentials
Signal sent via vestibulocochlear nerve (CN VIII)
Disorders like vertigo or motion sickness arise from otolith displacement or endolymph inertia
What is signal detection theory in as much detail as is needed for the MCAT but not more?
Signal Detection Theory (SDT)
SDT quantifies decision-making under uncertainty. It applies to perception (e.g., detecting faint signals), medicine (e.g., test results), and attention tasks.
FOUR POSSIBLE OUTCOMES
Actual Signal | You Respond “Yes” | You Respond “No” |
|---|---|---|
Signal Present | Hit | Miss |
No Signal | False Alarm | Correct Rejection |
Two Key Variables in SDT:
1. d′ (d-prime) = Sensitivity (strength of signal)
Measures how well you can distinguish signal from noise
High d′= strong signal, EASY to detect
Low d′ = weak signal, HARD to distinguish from background noise
Not “percent correctness”, but more like signal strength vs. noise overlap
2. C (Criterion) = Decision strategy/bias
Determines how you choose to say yes or no
Independent of d′ (you can be BIASED regardless of how clear the signal is)
Greater C, more conservative, more misses, less false alarms
Strategy | Bias | Tendency |
|---|---|---|
Liberal | C < 0 | Say “yes” more often → more hits, more false alarms |
Conserv | C > 0 | Say “no” more often → fewer false alarms, more misses |
Neutral | C ≈ 0 | Balanced yes/no based on evidence |
You think there's no car (no signal), but you go anyway without checking = Liberal strategy(C<0)→ risk of false alarm, less misses
You think there's no car, but stop and look again = Conservative strategy (C>0) → may miss opportunities, but safer
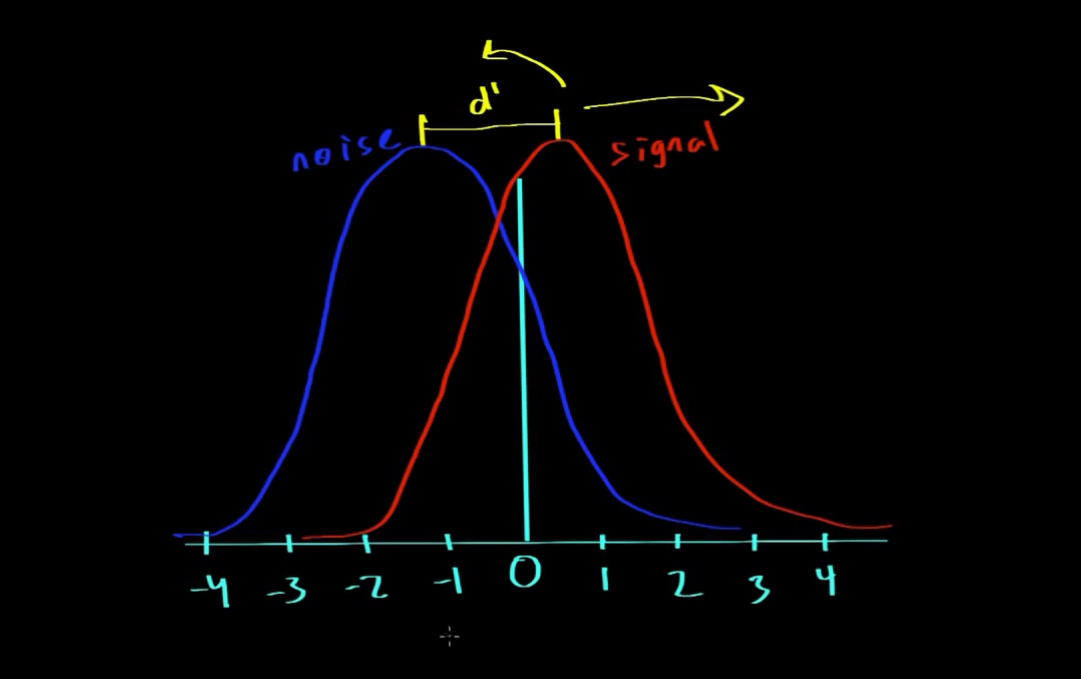
Signal Detection Theory (SDT) GRAPH
Larger d′ = less overlap = higher accuracy, fewer errors
Smaller d′ = more overlap = harder to tell signal from noise = more errors
The LEFT blue curve = noise only
The RIGHT red curve = signal
d′ is the horizontal distance between the two peaks:
If d′ is large, you can separate hits from false alarms more easily.
If d′ is small, the curves overlap, and you’re more likely to make misses or false alarms.
d′ = sensitivity (not precision, not error)
Large d′ = better signal detection, fewer errors
Small d′ = more overlap = more decision errors (false alarms/misses)
VERTICAL LINE on graph= decision threshold (your response criterion) (C=STRATEGY)
C>0 (further to right) is more conservative; MISS more of noise, less likely to make false alarm
C<0 (further to left) is more liberal; more likely to hit but also more likely for false alarm
C=0; IDEAL OBSERVER, BALANCED
Bottom-Up v. Top-Down: Dawn of Processing
Bottom-Up Processing
Definition: Processing based entirely on incoming sensory input, without prior knowledge
You start from the stimulus and build the perception
Analogous to: Inductive reasoning (start with data → build a conclusion)
Example: Seeing a strange fruit for the first time and using its features (color, texture) to figure out what it is
Top-Down Processing
Definition: Processing that uses prior knowledge, expectations, or experiences to interpret sensory input
You start with what you know and apply it to make sense of the stimulus
Analogous to: Deductive reasoning (start with concept → apply it to details)
Example: Reading messy handwriting more easily if you already know the sentence context
Feature | Bottom-Up | Top-Down |
|---|---|---|
Driven by | Stimulus | Expectations/Knowledge |
Speed | Slower (more data-driven) | Faster (uses shortcuts) |
Flexibility | Good for novel info | Can be biased by assumptions |
Reasoning Type | Inductive | Deductive |
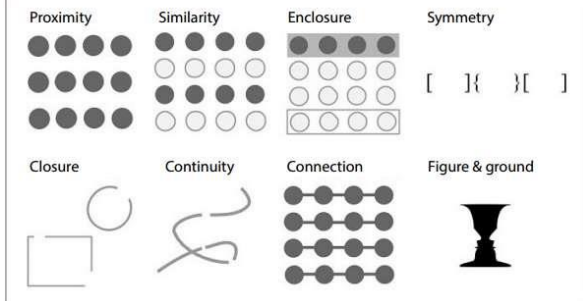
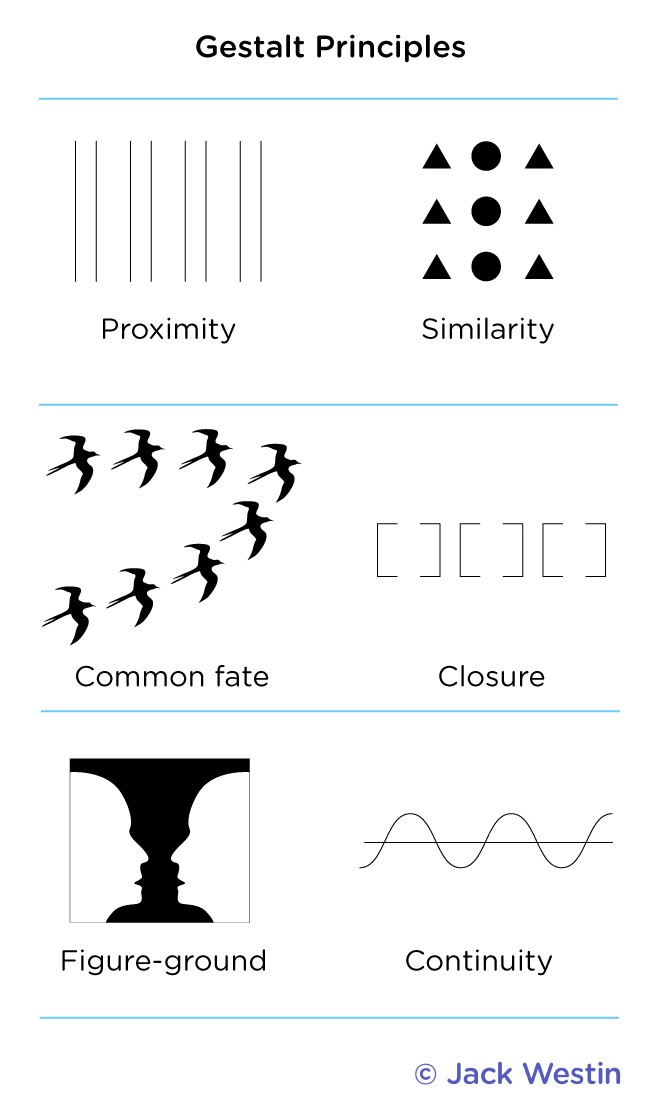
What are Gestalt’s Principles and what are the 7 types?
Gestalt’s Principles
Describe how our brains tend to organize visual information into whole forms ("gestalts") rather than perceiving isolated parts.
Based on the idea that "the WHOLE is GREATER than the SUM of its parts."
Applies mostly to visual perception, but also to auditory and cognitive grouping
Key figures: Max Wertheimer, Wolfgang Köhler, and Kurt Koffka; COGNITIVE APPROACH
Principle | Definition | Example |
|---|---|---|
Similarity | We group similar elements together | Columns of circles vs triangles seen as groups, not rows |
Proximity | We group objects that are close together | Dots that are near each other are perceived as one group |
Continuity | We perceive lines and patterns as continuing smoothly | A curved line crossing a straight one is seen as two continuous paths |
Closure | We fill in missing parts to perceive a complete, whole object | A triangle formed by broken lines is still seen as a triangle |
Prägnanz (Simplicity) Common Fate ______________ Figure Ground | We perceive complex images in the simplest form possible _____________________________ Elements that move together are perceived as part of the same group. ____________________________ We tend to separate a visual scene into a figure (object of focus) and a background. | Five interlocking rings are seen as five circles (not complex shapes) ________________________________ A flock of birds flying in the same direction looks like one unit.
In the Rubin vase illusion, you either see a vase (figure) or two faces (ground), depending on what you focus on. |
Pathway of Light Through the Eye and Its Parts:
1. Cornea (part of outer tunic)
through the
2. Anterior chamber
Contains aqueous humor for nourishment since cornea has no blood vessels
Provides PRESSURE to maintain shape of eyeball
through the
3. Pupil (controlled and hole made by the iris)
through the
4. Posterior chamber (also aqueous humor)
through the
5. Biconvex Lens (bends/focuses light rays)
Fine tunes light onto retina (ACCOMODATION)
Suspensory Ligaments:
-Thin, white fibers that attach the lens to the CILIARY MUSCLE, suspensory ligaments also adjust its shape for focusing by changing the TENSION
through the
6. Vitreous body/humor in the Posterior Segment/Cavity
Gel that holds retina in place
through the
7. Retina (inner tunic of eye)
Within the retina, light waves pass
8. Ganglionic layer (outer layer of cells)
Axons bundle to form CN II (Optic Nerve)
to the
9. Bipolar layer (middle layer of cells)
Intermediate neurons that relay signal from photoreceptors
Have axons coming along from both sides of the cell which makes snese since they are in the middle and receive signals to-and-fro, receiving from photoreceptor cells in particular POST-stimulation
to the
10. Photoreceptor layer (which transduces the light, before this step, brain does not understand light as it is not yet transduced into info)
Contains rods and cones
Action Potentials then pass from the photoreceptor layer
to the
9. Bipolar cell layer
to the
10. Ganglionic cell layer, the axons of which form the
11. Optic Nerve CN II which has some of its fibers cross in the
12. Optic chiasm
Nasal/Medial fibers CROSS to opposite side, temporal/lateral fibers STAY same side
to the
13. Optic tract
Then in a three-step pathway from
14a. Thalamus (Lateral Geniculate Nucleus/LGN)
14b. As optic radiation to the
14c. Visual Cortex (occipital lobe)
OR TO
15. Superior colliculi of the corpora quadrigemina of the mesencephalon (midbrain) for VISUAL REFLEXES
Key structures of eye to know for the MCAT
Choroid (eye) = rich in blood vessels, nourishes the retina (especially peripheral parts)
A Black/dark-brown layer depending on concentration of melanin
Macula Lutea: Area of retina with most acute vision (broadly in center), upon macular degeneration a person will lose their sharp/acute vision
Fovea Centralis: Central pit of macula lutea; Ganglionic, bipolar, and even rods of photoreceptor layer are pushed aside
ONLY MADE UP OF CONES, EXCLUSIVELY, NO RODS ALLOWEDDDD
Ciliary Body: Ciliary Muscle + Suspensory Ligaments
Secretes the vitreous humor for the posterior chamber
Sclera
Whites of the eye, thick fibrous tissue that covers posterior 5/6th of eyeball.
Attachment point for muscles.
What are the 4 Key Visual Processes for Focus and Depth Perception?
Process | Definition | Function / Relevance |
|---|---|---|
Accommodation | Lens shape changes via ciliary muscles and suspensory ligaments | Focuses light on the retina (near vs. far objects) |
Convergence | Both eyes rotate inward when focusing on a near object | Binocular depth cue—helps determine object distance |
Pupillary Constriction | Iris muscles constrict pupil to limit light entry and improve depth of field | Helps with sharpness and clarity of near vision |
Lens Constriction / Refraction | Light bending by cornea and lens to direct image onto the fovea of retina | Critical for focusing light precisely on photoreceptors |
Key MCAT Takeaways
Accommodation = lens thickness adjustment
Convergence = eye rotation inward for close objects
Pupil constriction = sharper focus for near objects
Refraction = bending of light via cornea & lens to focus on retina
How do we see? What is the phototransduction cascade?
Light comes in, goes through pupil, and hits rod.
Normally rod is turned on, but when light hits turns off.
When rod is off, it turns on a bipolar cell, which turns on a retinal ganglion cell, which goes into the optic nerve and enters the brain.
Phototransduction Cascade
PURPOSE: Convert light into electrical signal in the retina (specifically in RODS)
1. In Darkness (Rhodopsin is by DEFAULT inactive due to high cGMP)
Rhodopsin is inactive
High [cGMP] keeps Na⁺ channels open
Na⁺ flows into rod → rod is depolarized
Rod releases glutamate continuously
Glutamate inhibits ON bipolar cells
Glutamate excites OFF bipolar cells
2. Light Enters the Eye (Light causes tautomerization of rhodopsin to ACTIVATE IT)
Light hits the retina and reaches rods
Retinal (inside rhodopsin) changes shape:
11-cis-retinal → all-trans-retinal
Rhodopsin changes shape and becomes activated
3. Signal Transduction Begins (Transducin/G ACTIVATED)
Activated rhodopsin activates transducin (G-protein)
Transducin = α, β, γ subunits
α-subunit of transducin binds and activates phosphodiesterase (PDE)
4. Activated PDE breaks cGMP down into GMP
PDE breaks down cGMP → GMP
[cGMP] drops, so Na⁺ channels close
Rod becomes hyperpolarized (more negative inside) STOPPING glutamate release
5. Signal Sent to Brain
ON bipolar cells disinhibited → they depolarize and fire
ON bipolar cell ACTIVATES retinal ganglion cell
Ganglion cell sends signal via optic nerve to brain (occipital lobe)
Rods N Cones Fun Facts
A photoreceptor is a specialized nerve that can take light and convert to neural impulse.
Inside rod/cones are thousands of OPTIC DISCS
In membrane of each optic disc are proteins that fire APs to the brain.
Rods: Rhodopsin, Cones: Photopsin
Cones: 60% Red, 30% Green, 10% Blue
Rods: SLOW recovery time, Cones: FAST recovery
Rods v. Cones: Dawn of Sight
Feature | Rods | Cones |
|---|---|---|
Photopigment | Rhodopsin | Photopsin |
Function | Night vision (scotopic), low light | Day vision (photopic), color vision |
Number | ~120 million | ~6 million |
Sensitivity | Very sensitive (work in dark) | Less sensitive (need more light) |
Adaptation Speed | Slow to adapt to light | Fast adaptation to changes |
Color Detection | No | Yes (RGB types: red, green, blue) |
Location in retina | Periphery | Concentrated in fovea |
Visual acuity | Low (blurrier) | High (sharp detail) |
Saturation | Easily saturated (bleached in light) | Less easily saturated |
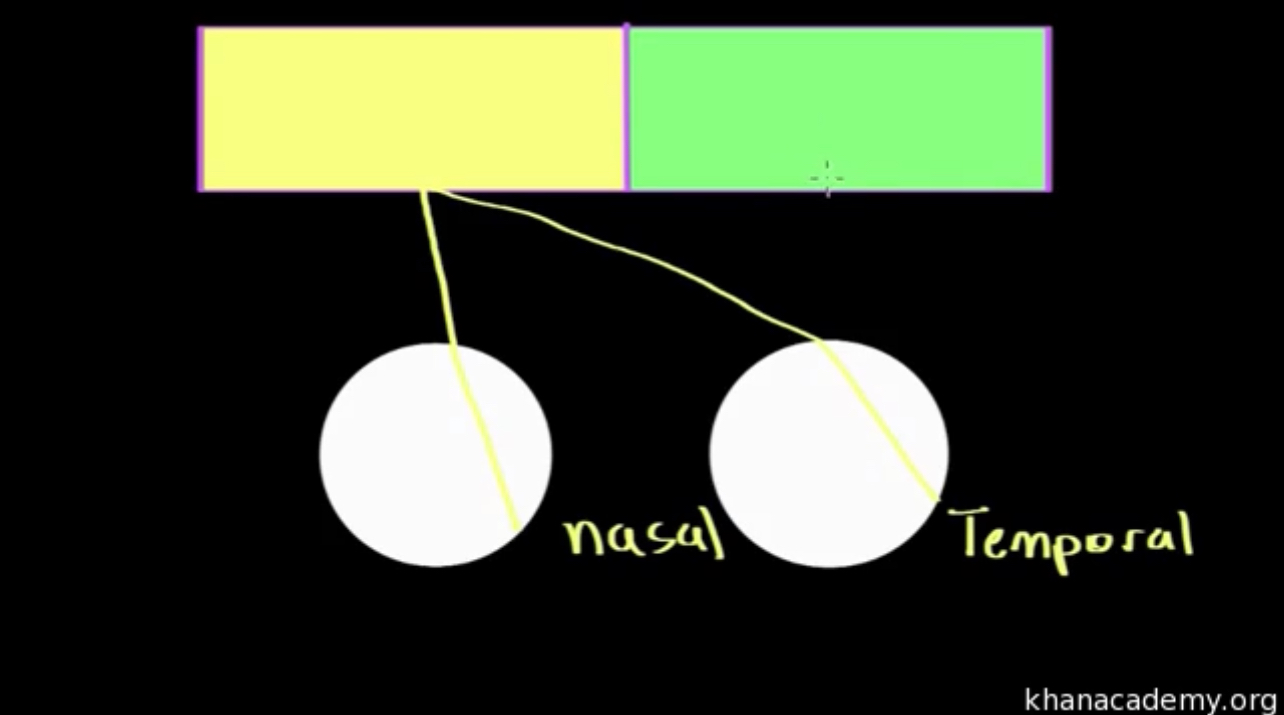
How does visual field processing occur? Describe FEATURE DETECTION of visual stimuli:
Understanding the Diagram (MCAT Style)
The yellow box on the left represents the left visual field.
The green box on the right is the right visual field.
The white circles are the retinas of each eye.
Light from the LEFT visual field hits the NASAL retina of the LEFT eye and the TEMPORAL retina of the RIGHT eye.
Both are processed in RIGHT occipital lobe
Nasal/medial retina CROSSES OVER
Temporal retina STAYS SAME SIDE
The image is flipped and inverted on the retina, so field and retinal side are opposites
Feature Detection (MCAT Summary)
Your brain detects three key features of visual stimuli:
Color, Form, and Motion
1. Color
Detected by cones
Based on Trichromatic Theory:
Red cones (long wavelength) → most abundant (60%)
Green cones (medium wavelength, 30%)
Blue cones (short wavelength) → ~10% of cones
Works best in bright light conditions
2. STILL Shape & Detail: PARVOCELLULAR PATHWAY
Specializes in:
High SPATIAL resolution → clear detail, sharp edges
Low temporal resolution → does not work well with motion
Activated by stationary objects
3. MOVING Shape & Detail: MAGNOCELLULAR PATHWAY
Specializes in:
High temporal resolution → detects motion well
Low spatial resolution → blurry image, low detail
Does NO detect color
Describe the pathway of sound along with the important structures of the ear to know for the MCAT
Sound Wave Entry
Sound = pressurized wave (areas of high and low pressure)
1. Pinna (Auricle) → collects sound
2. External Auditory Canal → channels wave inward
3. Tympanic Membrane (Eardrum) → vibrates with sound
Middle Ear Ossicle Vibration (AMPLIFY vibrations)
4a. Malleus/Hammer
4b. Incus/Anvil
4c. Stapes/Stirrup: Attached to OVAL WINDOW
5. Oval window (membrane between middle and inner ear)
Stapes pushing it creates waves in perilymph in SV
6. Scala vestibuli (perilymph-filled space in inner ear)
Perilymph moves here vibrating the
7. Organ of Corti which contains the BM and TM
8. Basilar membrane (membrane in organ of corti)
HIGH frequencies displace BASE of basilar membr
LOW frequencies displace APEX of basilar membr
Vibration here causes perilymph here to move and DISPLACE
9. Hair cells
Contain stereocilia bundles made of kinocilia and are embedded in the
10. Tectorial membrane (stiff)
Movement of the stereocilia OPENS K+ channels, influx of K+ TRIGGERS Ca2+ influx GENERATING ACTION POTENTIAL
This transduces sound into action potentials transmitted through the vestibulocochlear nerve (CN VIII) to the
11. Inferior colliculi (of corpora quadrigemina of mesencephalon) for AUDITORY REFLEXES
to
12. Thalamus (relay station)
to
13. Auditory cortex of the temporal lobe (final destination in brain)
ALSO
Vibrations pass from the basilar membrane into the
14. Scala tympani (fluid-filled space/lower chamber of cochlea)
to
15. Round window (membrane between inner ear back to middle ear)
Bulges outwards to RELEASE pressure
MCAT Takeaways
Organ of Corti = functional unit of hearing
K⁺ and Ca²⁺ ions initiate the neural signal
Hair cells transduce mechanical → electrical energy
Sound frequencies are separated via basilar membrane tuning
Final destination = temporal lobe of the brain
So with basilar tuning, brain can distinguish dif frequencies – tonotypical mapping
How do we know where we are and feel ourselves (pause)?
Post-Central Gyrus/Somatosensory Cortex
Somatosensory Homunculus (MCAT Scope)
It’s the brain’s map of the body’s sensory input.
Each body part sends touch, pressure, pain, and temperature info to a specific area of the brain.
Receives input mapped by body region (homunculus)
More sensitive areas (e.g. lips, hands) take up more cortical space
More sensitive areas (like lips and hands) have larger representation.
Feature
Proprioception
Kinesthesia
Definition
Sense of body position in space
Sense of body movement
Focus
Static awareness (e.g., where your arm is)
Dynamic awareness (e.g., how your arm moves)
Balance-related?
Yes—helps with balance and posture
No—not involved in balance
Receptors
Muscle spindles, joint stretch receptors
Also muscle/joint receptors, but focus on motion
Conscious?
Mostly subconscious
More conscious awareness of motion
Example
Knowing your foot is behind you while standing
Adjusting your arm mid-throw
Proprioception = position + BALANCE (e.g., standing on one leg with eyes closed)
Kinesthesia = movement (e.g., learning to shoot a basketball), BEHAIVORAL, NO balance
Proprioception is more about "where", kinesthesia is more about "how it moves"
How do we feel pain?
Pain and Temperature Sensation (MCAT Summary) TRPV1 Receptor
TRPV1 = transient receptor potential vanilloid 1
A membrane-bound receptor that responds to:
Heat
Tissue damage (pain)
Chemical signals (e.g., capsaicin from spicy food)
Mechanism: Binding of stimulus → conformational change in receptor → activates sensory neuron → signal to brain
Capsaicin Example
Capsaicin binds to TRPV1, mimicking heat damage.
Results in a "burning" pain sensation, sweating, etc.
Doesn’t convert pain—just triggers the same receptors that heat or injury would.
Aβ fibers: FAST reflex—pull hand away
THICC, myelinated, high conductance
Aδ fibers: MEDIUM sharp, localized pain
Med-diameter, less myelin
C-fibers: SLOW, throbbing, lingering pain
SMOL-diameter, UNMYELINATED
Key MCAT Takeaways
TRPV1 = ion channel involved in pain and heat sensing
Capsaicin binds to TRPV1 → mimics pain/heat
Aβ, Aδ, and C fibers transmit pain at different speeds
Nociceptors ≠ thermoreceptors, but they can overlap
TRPV1 = a receptor used by both nociceptors and thermoreceptors
What are the two olfactory pathways to know?
System | Used For | Detected Molecules | Bulb |
|---|---|---|---|
Main olfactory system | General smell | Volatile odorants (e.g., perfume, food) | Olfactory bulb |
Accessory olfactory system | Pheromone detection | Pheromones (social/sexual signals) | Accessory olfactory bulb |
Pheromones are usually non-volatile, detected via direct contact or close proximity.
Humans may not have a functional accessory olfactory system like some animals do—this is still debated but fair game for MCAT-level conceptual understanding.
OLFACTION OVERVIEW
Olfaction = sense of smell, involving detection of airborne chemicals.
Closely linked to taste (why food tastes bland with a cold).
Two main pathways:
Main olfactory system – general smells
Accessory olfactory system – pheromones (mostly functional in animals)
Main Olfactory Pathway (General Odors) 🔬 Structures Involved
Olfactory epithelium – in nasal cavity; contains receptors for different odor molecules
Cribriform plate – porous bone separating nasal cavity from brain
Olfactory bulb – brain structure sitting above the cribriform plate; receives input from receptors
Mechanism of Signal Transduction
Odor molecules bind to GPCRs on olfactory sensory neurons.
G-protein dissociates → activates cascade → opens ion channels → depolarization → action potential (AP)
AP travels through axons to olfactory bulb, where:
Neurons converge in glomeruli (each glomerulus = 1 odor type)
Synapse on mitral/tufted cells, which relay signals to:
Piriform cortex (odor identity)
Amygdala (emotional relevance)
Orbitofrontal cortex (conscious perception of smell)
Key Points
Olfactory nerve (CN I) transmits signals.
Each olfactory receptor responds to one type of molecule (e.g., benzene).
Brain decodes smell by combinatorial receptor activation patterns.
Accessory Olfactory Pathway (Pheromones) – Animals Structures Involved
Vomeronasal Organ (VNO) = accessory olfactory epithelium
Contains apical cells and basal cells, each with specific pheromone receptors
Accessory Olfactory Bulb
Receives axons from VNO → sends signals to amygdala and hypothalamus
Mechanism of Detection
Pheromone binds to apical/basal cell receptor
AP travels through vomeronasal nerve → accessory olfactory bulb
Synapse in glomerulus → amygdala → hypothalamus
Triggers innate behavioral and hormonal responses (e.g., mating, aggression)
Important Notes
Humans have a vomeronasal organ, but no functional accessory olfactory bulb, making the pathway likely vestigial.
Amygdala = major target for both general odors (emotional response) and pheromones (instinctual behavior)
MCAT Key Takeaways
Main olfactory system detects general smells through GPCRs and glomerular mapping.
Accessory system (in animals) detects pheromones through apical and basal cells in the VNO.
Amygdala is a common target for emotional and behavioral response.
Humans lack a functional accessory olfactory bulb, making our pheromone response minimal.
Describe GUSTATION in as much detail as is needed for the MCAT:
Taste | Receptor Type | Mechanism |
|---|---|---|
Sweet | GPCR (T1R2 + T1R3) | G-protein → depolarization |
Umami | GPCR (T1R1 + T1R3) | G-protein → depolarization |
Bitter | GPCR (T2R family) | G-protein → depolarization |
Sour | Ion channel (H⁺) | Protons enter cell → depolarization |
Salty | Ion channel (Na⁺) | Sodium enters cell → depolarization |
Key MCAT Takeaways
Each taste bud contains receptors for all 5 basic tastes
Papilla type ≠ taste type specialization
Sweet, bitter, and umami use GPCRs
Sour and salty use ion channels
Taste info is carried via cranial nerves VII, IX, and X to the gustatory cortex
Where is the Gustatory Cortex?
Located in the INSULA (deep within the cerebral cortex) and extends into the frontal operculum.
It receives taste signals from the thalamus after synapsing from cranial nerves.
Labeled Lines Model
Each taste bud has EVERY taste receptor cell
Each taste receptor cell is specialized for only one taste (sweet, salty, sour, bitter, or umami).
These cells send signals via dedicated axons to specific regions of the gustatory cortex.
This is known as the labeled lines model:
Each taste is carried by its own “line” (pathway).
So stimulating a sweet receptor’s pathway, even with a salty stimulus, would make the brain perceive sweetness.
Brilliant Logic You Noted (MCAT-Backed)
Salty and sour = ion channels:
Salty = Na⁺ influx
Sour = H⁺ (protons) enter and alter internal charge
Sweet, bitter, and umami = GPCRs:
Signal via secondary messengers (slower but more sensitive)
Key MCAT Takeaways
Gustatory cortex is in the insula and frontal operculum
Labeled lines model: each taste cell → its own axon → brain interprets based on which pathway fires
Salty & sour = ion channels
Sweet, umami, bitter = GPCRs
Swapping receptor mechanisms can trick the brain into misidentifying tastes
E.g. Glucose binds GPCR, conformational change, G-protein dissociates, opens ion channels, cause cell to depolarize and fire an AP
If a salty receptor is placed in a sweet cell, the brain will interpret the salty stimulus as SWEET because the axon pathway remains the same, causing the SAME action potential and perception.
What to know about sleep and conscoiusness for the MCAT
5 LEVELS OF CONSCIOUSNESS & EEG/BRAIN PATERNS
Level | Description | Associated Brain Waves |
|---|---|---|
Alertness | Fully awake, aware of self and environment | Beta |
Daydreaming | Relaxed, awake, lightly distracted (e.g., meditation) | Alpha |
Drowsiness | On the verge of sleep or just waking | Alpha → Theta transition |
Sleep | Unconscious but brain still active (non-REM & REM stages) | Theta, Delta, and Beta (in REM) |
Coma | No awareness or responsiveness | Varies or flat EEG |
4 STAGES OF SLEEP
Sleep Cycle Structure
Each sleep cycle lasts ~90 minutes
A full night includes 4–6 cycles, increasing in REM as the night goes on
General progression:
N1 → N2 → N3 → N2 → REM → repeat
(Your “N-Woo before REM” mnemonic = gold)
NREM 1 SLEEP
Wave Type | Theta (4–7 Hz) |
|---|---|
Features | Light sleep, drifting off, hypnic jerks, hypnagogic, hallucinations |
Transition | From wakefulness (alpha) → sleep (theta) |
NREM 2 SLEEP
Wave Type | Theta (4-7 Hz) + Sleep Spindles + K-Complexes |
|---|---|
Features | Light sleep but harder to wake; memory consolidation begins |
Sleep Spindles | Burst of high-frequency waves, keep you ASLEEP |
K-complexes | Sharp, high-amplitude waves, SUPPRESS arousal to keep you asleep |
NREM 3 / SLOW-WAVE SLEEP
Wave Type | Delta (0.5–4 Hz) (low frequency, high amplitude) |
|---|---|
Features | Deepest sleep, difficult to wake, sleepwalking, night terrors |
Functions | Physical recovery, GH/Pessiii release, immune function |
REM SLEEP
Wave Type | Beta-like (similar to wakefulness) (13-30 hz) |
|---|---|
Features | Rapid eye movements, dreaming, muscle atonia (sleep paralysis) |
Also Called | Paradoxical sleep (brain active, body paralyzed) |
Memory | Important for emotional processing, procedural memory |
Sleep cycle = NREM 1 → 2 → 3 → 2 → REM, ~90 minutes per cycle
Stage 3 (Delta) = deep, restorative sleep
REM = vivid dreams, brain active, body paralyzed
Spindles/K-complexes = Stage 2
Beta in wakefulness and REM
Sleep Cycle Structure
Each sleep cycle lasts ~90 minutes
A full night includes 4–6 cycles, increasing in REM as the night goes on
General progression:
N1 → N2 → N3 → N2 → REM → repeat
(Your “N-Woo before REM” mnemonic = gold)
Circadian Rhythm
~24-hour biological cycle regulated by:
Light (especially sunlight)
Controlled by the suprachiasmatic nucleus (SCN) in the hypothalamus
Regulates:
Sleep-wake cycle
Body temperature
Hormone release from MELATONIN produced in the PINEAL GLAND
Can change as you age; old heads go to bed early
Dreaming
Everybody dreams during REM sleep.
Can tell someone is dreaming because eyes are moving rapidly under eyelids, and brainwaves look like they are completely awake (BETA)
Activity in prefrontal cortex during REM sleep is DECREASED– part responsible for logic. Why things in our things that defy logic don’t seem weird.
What are the different theories on dreams?
Freudian Theory
Component | Definition |
|---|---|
Manifest content | What you literally see in the dream (e.g., being chased) |
Latent content | Underlying meaning of dream (e.g., fear of failure) |
Purpose | Freud believed dreams were a way to express unconscious desires and repressed urges safely |
Other Theories
Theory | Main Idea |
|---|---|
Activation-Synthesis Theory | Brainstem activation during REM = random neural firing → Cortex synthesizes it into a storyline (dreams are meaningless "noise" interpreted) |
Problem-Solving Theory | Dreams allow you to work through real-life issues creatively or emotionally |
Cognitive Development Theory | Dreams reflect your current level of cognitive maturity and development |
Threat Simulation Theory | Dreams evolved as a safe space to rehearse survival-based threats (evolutionary psych) |
Continuity Hypothesis / Day Residue | Dreams reflect waking life, no hidden meaning |
DISORDERS LIKE SLEEP APNEA YOU DON’T GET ENOUGH N3 (Slow-wave/theta sleep)
Sleep walking and talking ALSO occur during N3, more often in children (who have more N3 sleep)
Hypnosis and Meditation
Hypnotism usually involves getting person to relax and focus on breathing, and they become more susceptible to suggestion in this state – but only if they want to.
MORE ALPHA waves in this stage – an awake but relaxed state.
What are the 4 classes of drugs?
Drug Class | Primary Function | Key Examples | Mechanism | Distinguishing Features |
|---|---|---|---|---|
Depressants | ↓ CNS activity (sedation, slowed processing) | Alcohol, Barbiturates, Benzodiazepines | ↑ GABA activity (Cl⁻ influx) ↓ neural firing | Reduces inhibition, does not counteract stimulants—effects stack |
Stimulants | ↑ CNS activity (alertness, energy) | Caffeine, Nicotine, Amphetamines, MDMA | ↑ Dopamine, norepinephrine, serotonin | Alerting, ↑ heart rate & BP, nicotine = stimulant despite relaxing sensation |
Hallucinogens | Alter perception, sensory distortion | LSD, PCP, Psilocybin (shrooms) | Varies (often serotonin pathway, esp. 5-HT₂A receptors) | Effects are not classified by energy, but by perceptual change despite increased CNS activity (like stimulant) |
Opiates / Opioids | Pain relief, euphoria; CNS depressant too | Morphine, Heroin, Codeine, Fentanyl | Bind to endorphin (opioid) receptors, mimics endorphins in pain relief | Analgesic + euphoric, different from depressants, very addictive |
MCAT Tips
Depressants: GABA-based inhibition; think alcohol’s disinhibition.
Stimulants: Enhance excitatory neurotransmitters; do not cancel depressants.
Hallucinogens: Classified by sensory changes, not stimulation or sedation.
Opiates vs. opioids: Natural vs. synthetic, but both act on endorphin receptors.
GABA and Depressants (MCAT Breakdown) What is GABA?
Gamma-Aminobutyric Acid (GABA) = the brain’s primary inhibitory neurotransmitter
Structure: Simple amino acid derivative (similar to glutamate but with an amine group instead of carboxyl)
Normal Function:
Binds to GABA-A receptors (ligand-gated chloride channels)
Opens Cl⁻ channels → Cl⁻ flows into the neuron → hyperpolarization (makes the inside more negative)
Inhibits depolarization → decreases likelihood of firing an action potential
HOW DO DEPRESSANTS WORK?
Drug Class | Mechanism of Action |
|---|---|
Benzodiazepines | Enhance the effect of GABA by increasing Cl⁻ influx (via GABA-A receptor modulation) |
Barbiturates | Prolong GABA channel opening time |
Alcohol | Also enhances GABA activity and reduces glutamate excitability |
Key Concept:
The more chloride influx, the harder it is to depolarize the neuron → reduced CNS activity
Depressants = promote inhibition, sedation, anxiolysis (anti-anxiety), or sleep induction
Use | Type of Depressant |
|---|---|
Insomnia, short-term sedation | Short-acting benzos/barbs |
Anxiety, seizure control | Long-acting benzos/barbs |
WHAT NEUROTRANSMITTERS DO STIMULANTS AFFECT?
Main Neurotransmitters Affected by Stimulants | Effect |
|---|---|
Dopamine (DA) | ↑ Dopamine = reward, motivation, euphoria |
Norepinephrine (NE) | ↑ Norepinephrine = alertness, focus, increased heart rate |
Serotonin (5-HT) (to a lesser extent) | Can elevate mood slightly, but dopamine and norepinephrine are primary |
Why Stimulants Make You "Hyper"
Caffeine blocks adenosine receptors (adenosine promotes sleepiness)
Amphetamines, cocaine, MDMA = increase dopamine and norepinephrine availability (by preventing reuptake or promoting release)
Result = increased CNS activity, heightened alertness, mood elevation
HOW DO OPIATES WORK?
Drug Class | Mechanism of Action |
|---|---|
Opiates/Opioids | Mimic endorphins (natural painkillers) by binding to opioid receptors (μ-opioid receptor is key) |
Effect | Block pain signals, cause euphoria, sedation, slow breathing, high risk of addiction |
WHAT NEUROTRANSMITTERS DO HALLUCINOGENS AFFECT?
Hallucinogen Type | Main Neurotransmitter Affected | Effect |
|---|---|---|
LSD, Psilocybin, DMT | Serotonin (5-HT) | Distortions in perception, mood swings, hallucinations |
PCP, Ketamine | Glutamate (NMDA receptor antagonists) | Dissociation, hallucination, altered reality |
Serotonin and Hallucinations
Hallucinogens stimulate serotonin receptors (especially 5-HT2A subtype).
Leads to sensory distortions, emotional swings, and hallucinations.
Schizophrenia is more classically associated with excess DOPAMINE, not serotonin.
Serotonin is central for mood and perception, but dopamine drives psychosis symptoms.
Describe Drug Homeostasis for the MCAT
What Is Tolerance?
Tolerance = Needing increased amounts of a drug over time to achieve the same effect.
Happens because the body either:
Downregulates receptors (receptor desensitization)
Increases metabolism of the drug (enzyme induction)
Or, as you mentioned, prepares in advance through environmental cues.
Conditioned (Learned) Tolerance
Concept | Definition |
|---|---|
Conditioned tolerance | Body anticipates drug effects based on environmental cues (e.g., same room, same people, same ritual) |
Example | Taking a stimulant like cocaine in the same room daily → body lowers heart rate ahead of time because it "knows" the drug is coming |
Risk Factor | Taking the same dose in a new environment → body does not compensate → higher risk of overdose |
Your brain is always trying to maintain homeostasis.
If a drug increases CNS activity, your body compensates by dampening that activity when it senses the drug is coming.
If you suddenly remove the environmental cue, the body’s compensation doesn’t kick in → higher drug effect than expected → overdose risk.
Term | Definition (MCAT-Relevant) |
|---|---|
Tolerance | Needing higher doses of a drug to achieve the same effect due to receptor desensitization or metabolic adaptation |
Dependence (Physical) | Body physically adapts to drug → withdrawal symptoms when stopped (e.g., shaking, sweating) |
Dependence (Psychological) | Emotional need or craving for the drug (e.g., needing it to relieve stress) |
Withdrawal | Negative symptoms experienced when stopping a drug after dependence develops |
Addiction (Substance Use Disorder) | Compulsive drug-seeking behavior despite negative consequences |
Craving | Intense desire for the drug (can occur even after long abstinence) |
Relapse | Return to drug use after a period of abstinence |
Conditioned Tolerance | Environmental cues trigger the body to preemptively counteract drug effects (risk of overdose without cues) |
Sensitization (Reverse Tolerance) | Opposite of tolerance → increased response to the drug after repeated use (less common) |
Comorbidity | Having two or more disorders at the same time (e.g., depression and substance use disorder) |
Extinction | Gradual weakening of a conditioned response when the stimulus is no longer reinforced (e.g., craving goes down if drug is unavailable repeatedly) |
Reward Pathway | Dopamine pathway → VTA → nucleus accumbens → prefrontal cortex (key in addiction and reinforcement learning) |
POSITIVE Reinforcement | Using the drug because it produces pleasurable effects (dopamine release) |
NEGATIVE Reinforcement | Using the drug to remove unpleasant feelings (e.g., avoiding withdrawal symptoms) |
Substance Use Disorder (SUD) | Clinical diagnosis of addiction → characterized by tolerance, withdrawal, cravings, inability to stop despite harm |
Key MCAT Concepts to Focus On
Reward Pathway = dopamine → reinforcement of behavior
Addiction = compulsive use + tolerance + withdrawal/craving
Positive reinforcement = drug feels good → repeat behavior
Negative reinforcement = drug removes bad feelings (e.g., withdrawal relief)
Extinction = when reinforcement stops → behavior decreases over time
Comorbidity = overlapping mental health + substance use disorders
Why "CRASHES" Happen After Drug Use Stops (Compensatory Response)
When you frequently use a stimulant (like cocaine, nicotine, caffeine), your body adapts to the drug’s effect (↑ CNS activity).
The body, trying to maintain homeostasis, starts to counteract the drug:
Reduces natural stimulant neurotransmitters
Might lower heart rate, downregulate dopamine receptors, etc.
If the drug suddenly isn’t there (because you stopped taking it):
Your body is still in "counteracting mode", expecting the drug’s presence.
Result = below-normal baseline activity → feelings of fatigue, depression, low energy = "crash"
Taking amphetamines daily → body lowers baseline dopamine to compensate.
Stop taking amphetamines → dopamine stays low, but no drug to boost it → depressed mood, lethargy, anhedonia (no pleasure).
Key MCAT Takeaway
Crash = the result of compensatory downregulation combined with sudden drug absence.
The body prepares to fight the drug effect, but if the drug isn’t there, the compensation overshoots = withdrawal or crash.
Describe the different routes of Drug Entry for the MCAT
Oral
Ingesting something, one of slowest routes because goes through GI tract – half hour.
Inhalation
Breathing or smoking, because once you inhale goes straight to brain – 10 seconds.
Injection
Most direct, intravenous means goes right to vein. Takes effects within seconds. Can be very dangerous.
Transdermal
Drug is absorbed through skin, ex. Nicotine patch.
Drug in patch has to be pretty potent, released into bloodstream over several hours.
Intramuscular
Suck into muscle. Can deliver drugs to your system slowly or quickly.
Quick for example is epipen. Or vaccines, slowly.
Faster route of entry = more addictive potential.
Describe the REWARD PATHWAY IN THE BRAIN
The Brain’s Reward Pathway
1. Triggering the Reward Pathway (Cake Example)
You see the cake → Prefrontal cortex = decision-making (“I want it”)
You taste the cake → Sensory cortex (e.g., postcentral gyrus) processes the flavor
You feel pleasure:
Amygdala = emotion (“This is amazing!”)
Hippocampus = memory (“Remember this for next time”)
Your brain is flooded with dopamine → you feel reward
Core Structure: MESOLIMBIC DOPAMINE PATHWAY
Region | Function in Reward |
|---|---|
Ventral Tegmental Area (VTA) | Origin of dopamine release (in midbrain) |
Nucleus Accumbens | Motivation, pleasure (“I want more”) |
Prefrontal Cortex | Focus, planning (“Let’s get more cake”) |
Amygdala | Emotional response (“Yum!”) |
Hippocampus | Memory of the experience (“Remember the bakery”) |
All of these are part of or connected to the limbic system, which handles emotion, motivation, and memory.
3. Role of Dopamine (DA) and Serotonin (5-HT)
Neurotransmitter | Function | In Reward Context |
|---|---|---|
Dopamine | Pleasure, motivation, reinforcement | Increases in reward pathway → craving |
Serotonin | Mood, satiety, well-being | Decreases as dopamine rises → less satisfaction, more craving |
High dopamine + low serotonin = “It feels good, but I can’t stop”
HIGH DOPAMINE=HAPPY
LOW SEROTONIN=INCREASED CRAVING
Key MCAT Takeaways
Reward pathway = VTA → Nucleus Accumbens → Prefrontal Cortex (+ amygdala, hippocampus)
Limbic system = emotion, memory, reward (includes amygdala, hippocampus, nucleus accumbens)
Dopamine = drives reward and craving
Serotonin = regulates satiety → low serotonin = keep seeking reward
What are the Neurobiological Responses to Addiction?
Medication-Assisted Treatment
Approach
Explanation
Substitution therapy
Prescribe a weaker, safer version of the addictive substance to reduce cravings and withdrawal symptoms
Examples
- Nicotine patches/gum for smokers
Methadone or buprenorphine for opioid addiction |
| Goal | Prevent withdrawal, reduce relapse, and wean off dependence gradually
Cognitive Behavioral Therapy
Purpose | Cognitive re-training → patient learns to recognize, avoid, and cope with triggers for substance use |
|---|---|
Effectiveness | - Helps maintain long-term abstinence |
Especially useful for preventing relapse |
| MCAT Connection | CBT increases awareness of the underlying causes of substance use, not just treating symptoms |
| Common Pairing | Often combined with MAT for better outcomes |
12-Step Programs: GROUP MEETINGS
ADMIT the Problem
SURRENDER to higher power or support system
GIVE BACK to others (community support)
Body compensates by downregulating receptors
Fewer receptors = weaker response, even with same dose |
Key MCAT Takeaways
Tolerance = fewer receptors or faster metabolism → more drug needed
SUD = continued drug use despite negative consequences
Not all addiction-like behavior qualifies as a substance use disorder
Caffeine use shows tolerance and withdrawal, but not enough harm for clinical SUD diagnosis
What are the different things on attention we need to know for the MCAT?
Selective Attention
Selective attention = flashlight → whatever you shine it on is what you consciously process most
Types of Cues That Guide Attention
Cue Type | Definition | Examples |
|---|---|---|
Exogenous | External, automatic attention-grabbers | Loud noise, bright color, flash, sudden movement |
Endogenous | Internal, based on meaning or goals | Arrow on a sign, your name in a convo (cocktail effect) |
Cocktail party effect = endogenous cue (name = meaning), but if screamed, exogenous OVERRIDES endogenous due to intensity.
Types of Attention Failures
Type | Definition | Example |
|---|---|---|
Inattentional blindness | Missing something in plain sight because attention is elsewhere | Missing a clown while texting |
Change blindness | Not noticing a change between two visual scenes | Not seeing a haircut change |
Theories of Selective Attention
Theory | Core Idea | Weakness/Note |
|---|---|---|
Broadbent’s Early Selection | Sensory register → filter → perception → response | Can’t explain cocktail party effect |
Deutsch & Deutsch (Late) | Sensory register → perception of all input → filter → response | All input assigned meaning, then filtered; TOO MUCH BRAIN POWER |
Treisman’s Attenuation | Sensory register → attenuator → perception → response | Unattended info is weakened, not blocked (your name can still grab attention) |
Key MCAT Takeaways
Selective attention = limited processing capacity → prioritize based on cues
Exogenous = automatic, Endogenous = learned/meaningful
Treisman’s theory = best explains cocktail party effect
Attention failures = inattentional blindness & change blindness
What is the spotlight model of attention and its associated quirks?
Attention Models & Priming
Priming
Definition: Being more likely to detect or respond to a stimulus if you’ve recently encountered something related
Can be conscious or subconscious
Example: You're more likely to notice your name because it's been primed over your entire life
Spotlight Model of Attention
Attention = a focus beam on one area of interest
You process information more deeply when it falls within the spotlight
Explains why relevant stimuli are noticed faster
Resource Model of Attention
Brain has a limited pool of attention resources
Can only distribute so much at once → limits multitasking ability
Multitasking LIMITATIONS and IDEALISM
Factor | Effect on Multitasking |
|---|---|
Task SIMILARITY | Harder to multitask if tasks are too similar (e.g., writing + podcast) |
Task DIFFICULTY | Harder to multitask when tasks are mentally demanding |
Practice/familiarity | Easier to multitask if a task is well-practiced (e.g., folding laundry while talking) |
Bottom line: Even with practice, multitasking is almost always less efficient than single-tasking
Key MCAT Takeaways
Priming influences attention (especially to meaningful stimuli like your name)
Spotlight model = focus-driven attention
Resource model = attention is limited and shared
Multitasking efficiency decreases with similarity, difficulty, and inattention
What are the main things that you should know about memory for the MCAT?
Information Processing Model: Sensory, Working, Long-Term Memory
Proposes our brains are similar to computers.
We get INPUT from environment, PROCESS it, and OUTPUT decisions.
First stage is getting the input – occurs in sensory memory (sensory register).
Temporary register of all senses you’re taking in.
Memory Systems
1. Sensory Memory
Definition: Very short-lasting memory tied directly to your senses.
Types:
Iconic memory = visual → lasts ~0.5 seconds
Echoic memory = auditory → lasts ~3–4 seconds
Function: Longer sensory ECHOIC memory you to briefly retain sensory info (e.g., re-entering a conversation after zoning out).
2. Working Memory (Short-Term Memory)
Definition: What you’re actively thinking about; limited capacity and duration.
Capacity: 7 ± 2 items → known as Miller’s Law, proposed by George Miller
Duration: About 20 seconds without rehearsal
Components (from Baddeley & Hitch model):
Phonological loop: Handles verbal/auditory info (words, numbers)
Visuospatial sketchpad: Handles visual and spatial info (shapes, maps)
Episodic buffer: Integrates information from both systems and links it to long-term memory
Brain region: Working memory and episodic buffer are coordinated by the CENTRAL EXECUTIVE
located in the prefrontal cortex
3. Long-Term Memory
Explicit (Declarative) Memory
Requires conscious RECALL
Types:
SEMANTIC memory: Facts, vocabulary, general knowledge
EPISODIC memory: Personal experiences or life events (e.g., your 10th birthday)
Stored mainly in: Medial temporal lobe, especially hippocampus
Implicit (Nondeclarative) Memory
Does not require conscious recall
Types:
PROCDURAL memory: Skills and habits (e.g., riding a bike, typing)
PRIMING : Prior exposure influences response (e.g., if you research rabbits all day, the word “hare” brings up the animal instead of hair)
Stored in: Cerebellum (procedural) and basal ganglia
Key MCAT Takeaways
Sensory memory is ultra-short and tied to specific senses
Working memory = 7 ± 2 rule → George Miller
Baddeley’s model: phonological loop, visuospatial sketchpad, episodic buffer, central executive
Long-term memory splits into:
Explicit (semantic + episodic)
Implicit (procedural + priming)
Different brain regions support each system (prefrontal cortex, hippocampus, cerebellum, basal ganglia
DUAL CODING HYPOTHESIS
Says it’s easier to remember words ASSOCIATED with images than either one ALONE.
Can use the method of LOCI – imagine moving through a familiar place and in each place leaving a visual representation of topic to be remembered.
What are the encoding strategies to know for the MCAT?
Encoding Strategies (Working → Long-Term Memory)
Strategy | Description | Effectiveness |
|---|---|---|
Maintenance/ROTE Rehearsal | Repeating info (rote memorization) with no meaning attached | Least effective |
Chunking | Grouping items into meaningful categories (e.g., FBI-NBC-CIA) | More effective |
Mnemonics | Using images, acronyms, or funny associations (e.g., ligma = ligament = bone) | Strong tool |
Self-referencing | Relating new info to yourself or personal experience; good for preparing to TEACH | Very effective |
Spacing effect | Spreading out study sessions over time instead of cramming | Most effective long-term |
Retrieval Cues
Type | Definition | Example |
|---|---|---|
Free recall | Recall with no cues | “Name all 7 dwarfs” |
Cued recall | Recall with a prompt or category hint | “Name the dwarf whose name starts with ‘D’” |
Recognition | Choose the correct answer from a list | Multiple choice question |
Free recall < Cued Recall < Recognition in ease of retrieval
For Free Recall, there is something called the SERIAL POSITION CURVE/EFFECT
Best at remembering first (primacy) and last (recency), hardest in middle
Memory Distortion Concepts
Term | Definition |
|---|---|
Memory reconstruction | Memory is not a perfect playback—we fill in gaps based on expectations |
Source monitoring error | Forgetting where info came from (e.g., dream vs. real conversation); recognize someone but forget from where |
Flashbulb memories | Highly EMOTIONAL events remembered with vivid detail—but not always accurate; susceptible to reconstruction |
MCAT likes to test how emotions distort or strengthen memories.
Sometimes information we retrieve is based on a
SCHEMA
Mental blueprint containing common aspects of world, instead of reality
Long-Term Potentiation vs. Synaptic Plasticity
Feature | Long-Term Potentiation (LTP) | Synaptic Plasticity |
|---|---|---|
Definition | Strengthening of a synapse with repeated use | General ability of synapses to change strength |
Mechanism | ↑ neurotransmitter release & ↑ receptor sensitivity | Includes both LTP (strengthening) and LTD (weakening) |
Role in learning | Key basis for learning and memory formation | Broader concept: learning, memory, and forgetting |
THIS IS LEARNING
Aging & Memory
Memory Type | Effect with Age |
|---|---|
Semantic memory | Improves or remains stable (e.g., vocabulary) |
Crystallized intelligence | Peaks in mid-adulthood (~30s), then slowly declines |
Episodic memory | Declines (especially for recent events) |
Processing speed & working memory | Declines with age |
Procedural memory | Stays intact (e.g., riding a bike) |
Prospective Memory | Ability to remember to do things in the future also decreases with age |
DECAY
When we don’t encode something well or don’t retrieve it for a while, we can’t at all anymore.
Connections become weaker over time. Initial rate of forgetting is high but levels off over time
HERMANN EBBINGHAUS, first investigator of decay
Found his rate of forgetting very fast, but if he remembered it after initial stage it levelled out
Just because you can’t retrieve something doesn’t mean it’s completely gone – relearning.
Even if Ebbinghaus couldn’t reproduce everything, took less time to learn list second time around.
Called SAVINGS, like with relearning piano after it having been a minute
Key MCAT Takeaways
Encoding improves with meaning and strategy (mnemonics, spacing, self-reference)
Recognition is easier than recall; memory is reconstructive, not photographic
LTP = biological basis for learning; synaptic plasticity = broader umbrella
Interference + decay = forgetting; semantic memory is resilient with age
RETROGRADE AMNESIA is inability to recall info previously encoded,
ANTEROGRADE AMNESIA is inability to encode new memories.
Dementia is forgetting to point of interfering with normal life – results from excessive damage to brain tissue,
Most common form is Alzheimer’s Disease.
Neurons die off over time.
Earliest symptoms are memory loss, attention, planning, semantic memory, and abstract thinking.
As it progresses, more severe language difficulties and greater memory loss, emotional stability and loss of bodily functions.
Cause is unknown – have buildup of AMYLOID PLAQUES
AGGREGATES OF MISFOLDED PROTEINS THAT FORM IN THE SPACES BETWEEN NERVE CELLS
Korsakoff’s Syndrome – caused by lack of vitamin B1 or thiamine. Caused by malnutrition, eating disorders, and especially alcoholism.
Thiamine converts carbohydrates into glucose cells need for energy. Imp for neurons.
Damage to certain areas causes poor balance, abnormal eye movements, confusion, and memory loss.
At this stage called Wernicke’s encephalopathy – precursor to KS.
If diagnosed in time can prevent further damage. If untreated, will progress to Korsakoff’s.
Main symptom is severe memory loss, accompanied by confabulation (patients make up stories to fill in memories).
Treatment is healthy diet, abstain from alcohol, take vitamins, and relearn things
What is cognition and what did Piaget have to say about it
Piaget’s 4 Cognitive Development Stages**
Stage | Age Range | Key Characteristics | Milestones Achieved |
|---|---|---|---|
Sensorimotor | 0–2 years | Experience the world through senses and actions | Object permanence (understanding that objects still exist when out of sight); stranger anxiety |
Preoperational | 2–7 years | Use language, play, and imagination; thinking is symbolic but not logical | Pretend play, egocentrism, begin to understand symbols (e.g., words, images) |
Concrete Operational | 7–11 years | Begin logical thinking about concrete events | Conservation, water in different jugs is the same; mathematical transformations, reduced egocentrism |
Formal Operational | 12+ years | Abstract reasoning and hypothetical thinking | Abstract logic, moral reasoning, think about “what if” scenarios |
MCAT Notes
Object permanence = major milestone of sensorimotor stage.
Egocentrism is most notable during the preoperational stage.
Conservation and math skills solidify in the concrete operational stage.
Formal operational stage introduces abstract thinking and forming independent moral frameworks.
What are the different ways that we interpret or problem solve by?
Assimilation v. Accomodation: Dawn of New Information
Term | Definition | Mnemonic | Example |
|---|---|---|---|
Assimilation | Interpreting new information by fitting it into an existing schema | Two S's = Same Schema | A child sees a raccoon and says “dog!” because it fits their preexisting schema of a dog. |
Accommodation | Changing an existing schema or creating a new one to incorporate new info | Two C's = Change/Create | After learning raccoons are different from dogs, the child forms a new schema for raccoons. |
Key MCAT Takeaways
Schemas = mental frameworks used to interpret information
Assimilation = new info fits existing understanding
Accommodation = new info modifies or creates schema
Correctness doesn’t matter—it’s about what happens to the schema
Problem Solving Strategies
Method | Definition | Example |
|---|---|---|
Trial and Error | Trying random solutions until one works | Typing random codes until one unlocks a phone |
Algorithm | Step-by-step method that guarantees a solution, but may be slow | Trying every possible key on a keyboard |
Heuristic | Mental shortcut that’s fast but can be error-prone | See below |
Intuition | Relying on instinct, high chance of effort | Type I error = false positive Type II error = false negative |
Heuristic Types
Type | Relies On | Definition | Example |
|---|---|---|---|
Availability Heuristic | Specific examples from memory | Judging likelihood based on how easily examples come to mind | Thinking sharks are more common than plane crashes after seeing a news story |
Representativeness Heuristic | Prototypes or general concepts | Judging likelihood based on how well something matches a prototype | Assuming someone is a librarian not a truck driver because they’re quiet and wear glasses |
Availability = Memory recall
Representativeness = Mental stereotype
But can lead to a CONJUNCTION FALLACY, which means co-occurrence of two instances is more likely than a single one
Other Problem Solving Concepts
Term | Definition |
|---|---|
Fixation | Getting stuck on a single approach that isn’t working |
Functional fixedness | Inability to see alternative uses for an object (e.g., not using a shoe as a hammer) |
Insight | Sudden realization of a solution (“Aha!” moment) |
Incubation | Stepping away from a problem; solution often arises after a break |
Confirmation bias | Favoring information that supports your preconceptions, ignoring contradicting evidence |
Belief perseverance | Clinging to a belief despite contradictory evidence |
Framing effects | The way a problem is presented can influence decisions (e.g., 90% survival vs. 10% death) |
Key MCAT Takeaways
Heuristics = mental shortcuts (Availability = ease of recall, Representativeness = match to prototype)
Fixation and functional fixedness can block creative problem-solving
Insight + incubation often lead to breakthroughs
Confirmation bias, belief perseverance, and framing affect how we interpret information
What are Semantic Networks and Spreading Activation***
Theoretical Framework
Cognitive Psychology: Collins & Loftus are part of this school, which emphasizes mental processes like memory, language, and perception.
Their model REPLACED earlier, hierarchically structured semantic networks (like the one proposed by Collins & Quillian).
Collins & Loftus – Modified Semantic Network
Concept | Definition |
|---|---|
Modified Semantic Network | Memory is organized based on individual EXPERIENCES, not strict hierarchies (like "animal → bird → canary") |
Spreading Activation | Activating one concept in memory activates related concepts via neural links |
Example: Thinking of “fire truck” might also activate “red,” “sirens,” or “emergency.”
Key MCAT Takeaways
Spreading activation = one idea triggers related ones; explains false memories
Modified networks = memory structure is flexible and personal, not rigid
Collins & Loftus = cognitive psychologists who challenged older hierarchical memory models
What are the different theories of intelligence?
Theories of Intelligence
Theory | Proponent | Key Idea |
|---|---|---|
General Intelligence (g-factor) | Charles Spearman | Intelligence is a single general ability. High performance in one area predicts performance in others. |
Triarchic Theory of Intelligence | Robert Sternberg | Intelligence has three components:
|
Primary Mental Abilities | L.L. Thurstone | Proposed 7 independent factors (e.g., verbal fluency, numerical ability, spatial reasoning)
|
Multiple Intelligences | Howard Gardner | Intelligence is not unitary. Includes 7–9 independent intelligences like musical, spatial, kinesthetic, etc. |
Emotional Intelligence | Daniel Goleman (popularized) | Ability to perceive, understand, and manage emotions in self and others. |
Fluid vs. Crystallized | Raymond Cattell | Fluid = problem-solving (declines with age). Crystallized = acquired knowledge (increases with age). |
MCAT Takeaways
Spearman's g-factor: Intelligence is a single, general capacity
Thurstone: Intelligence is made of several correlated abilities
Gardner: Intelligence includes a wide range of human talents, not all academic
Sternberg: Intelligence is what helps you succeed in real life
IQ Testing and Origins
Test | Creator | Purpose |
|---|---|---|
Binet-Simon Test | Alfred Binet | Designed to measure mental age to predict school performance in children. |
Stanford-Binet IQ Test | Lewis Terman | Adapted Binet's test for U.S.; used to quantify intelligence as a single score (IQ). |
Mindset and Intelligence
Test | Creator | Purpose |
|---|---|---|
Binet-Simon Test | Alfred Binet | Designed to measure mental age to predict school performance in children. |
Stanford-Binet IQ Test | Lewis Terman | Adapted Binet's test for U.S.; used to quantify intelligence as a single score (IQ). |
What is cognitive dissonance and what are some of the coping strategies we come up with to counter it?
4 Ways to Reduce Cognitive Dissonance
Strategy | Definition | Example |
|---|---|---|
1. Modify Cognition | Change your belief to match your behavior | “I don’t really smoke that much” (downplaying frequency) |
2. Trivialize | Make the conflict seem unimportant | “Smoking isn’t that bad for you anyway” |
3. Add Cognitions | Introduce new justifications to outweigh the conflict | “I smoke, but I also work out, so it balances out” |
4. Deny Conflict | Reject the facts that cause the dissonance | “There’s no conclusive evidence that smoking causes cancer” |
MCAT Tip
Dissonance creates mental discomfort, and people are motivated to reduce it—often irrationally.
Most likely to occur when behavior conflicts with strongly held beliefs, especially when personal choice is involved.
What is language, where does it take place in the brain, and what are the different prevailing theories concerning it?
Language and the Brain (MCAT Summary)
Structure | Location | Function | Damage Results In |
|---|---|---|---|
Broca’s Area | Left frontal lobe | Speech production | Broca’s (expressive) aphasia = broken, effortful speech but comprehension intact |
Wernicke’s Area | Left temporal lobe | Language comprehension | Wernicke’s (receptive) aphasia = fluent but nonsensical speech |
Arcuate Fasciculus | White matter tract between Broca & Wernicke | Connects comprehension & production | Conduction aphasia = fluent speech + comprehension, but inability to repeat words |
Corpus Callosum | Between hemispheres | Communication between hemispheres | If severed: left visual field info (processed in right hemisphere) can't reach left-side language centers → inability to verbally describe left-field objects |
MCAT Takeaways
Left hemisphere dominance: Especially for language in right-handed people
Broca = production, Wernicke = comprehension
Damage to connecting structures (e.g., arcuate fasciculus or corpus callosum) leads to disconnection syndromes
Use split-brain research to predict deficits in verbal reporting
Theories of Language and Thought (MCAT Summary)
Theory | Main Idea | Key Figure(s) | Example |
|---|---|---|---|
Universalism | Thought DETERMINES language—we all have the same underlying cognition | Jerry Fodor | You think about colors, and your language creates words for them |
Piaget’s Theory | Thought INFLUENCES language; Language develops as children’s cognition matures | Jean Piaget | Think first then develop language to describe those IDEAS |
Vygotsky’s Interactionist | Thought and language are INDEPENDENT at first, then MERGE via social interaction | Lev Vygotsky | Children use language to develop inner speech and structure thinking |
Linguistic Determinism (Weak) | Language influences thought—but does not determine it | — | Language direction (e.g., right-to-left) influences how we picture time flow |
Linguistic Determinism (Strong) | Language determines thought—you CAN’T think BEYOND what your LANGUAGE allows | Sapir-Whorf (Whorfian Hypothesis) | No words for past/future = cannot conceive time in that way |
MCAT Takeaways
Universalism → cognition first, language second
Piaget → cognitive development guides language development
Vygotsky → language and thought start separately, then integrate through socialization
Weak linguistic determinism = influence, strong = limitation of thought by language
Theories on Language DEVELOPMENT
Theory | Main Idea | Key Figure | Example |
|---|---|---|---|
Nativist (INNATENESS OF LANGUAGE) | We are born with a Language Acquisition Device (LAD)—an innate ability to learn grammar; there’s a critical period (0–8/9 yrs) | Noam Chomsky | A child picks up language rapidly in early years without formal instruction |
Learning (BEHAIVORIST) | Language is learned through reinforcement and imitation | B.F. Skinner | A baby says “mama,” mom smiles → positive reinforcement strengthens behavior |
MATERIALIST | Look at what happens in brain EXCLUSIVELY when people think/speak/write | ||
Interactionist | Language develops through a blend of biological capacity and social interaction | Lev Vygotsky | A child learns to speak through talking with caregivers and peers |
MCAT Takeaways
Nativist = innate grammar wiring + critical period
Learning = reward-based behaviorism (criticized for oversimplicity)
Interactionist = blend of biology + environment
What is the Limbic system and how does it regulate emotion?
HIPPO WEARING HAT (Structures of Limbic System)
Letter | Structure | Function | DAMAGED Effects |
|---|---|---|---|
H | Hypothalamus | Regulates the autonomic nervous system, emotions, hunger, thirst, sex drive, body temp; links brain and endocrine system via pituitary | Hormonal imbalance, disrupted homeostasis (e.g. extreme hunger, rage, etc.) |
A | Amygdala | Processes emotions, especially fear, aggression, arousal | Klüver–Bucy syndrome: hyperorality, hypersexuality, docility (tameness) |
T | Thalamus | RELAY station for SENSORY info (except smell) to the cortex | Loss of sensory integration; can lead to sensory confusion or hallucinations |
Hippo | Hippocampus | Converts short-term to long-term memory; involved in learning | Anterograde amnesia: inability to form new memories, old memories remain intact |
MCAT Takeaways
Amygdala = fear and anger: AMSITHDALA
Hippocampus = memory (damage = anterograde amnesia)
Hypothalamus = homeostasis and drives (Four Fs: fight, flight, feeding, fornication)
Thalamus = relay of all senses except smell
Emotions and the Brain
Hemispheric Specialization
Left Hemisphere: Associated with positive emotions (e.g., happiness, sociability).
Right Hemisphere: Associated with negative emotions (e.g., fear, sadness, withdrawal).
Prefrontal Cortex
Function: Regulates decision-making, social behavior, and impulse control.
Damage leads to: Disinhibition, inappropriate behavior, poor judgment (e.g., Phineas Gage case).
Paul Ekman's 6 Universal Emotions
These are seen across all cultures—even in infants and individuals born blind:
Happiness
Sadness
Anger
Fear
Disgust
Surprise
3 Components of Emotion
Cognitive – What you think (e.g., "I’m in danger").
Physiological – What your body does (e.g., increased heart rate).
Behavioral – What you do (e.g., run away, smile, freeze).
Cultural Differences in Emotion
While universal emotions are biologically innate, emotional expression can vary by culture. This is known as display rules.
Display rules: Cultural norms that dictate how and when emotions are expressed.
MCAT Tip
Know that blind individuals and infants express universal emotions despite no modeling, suggesting an innate biological basis.
Be able to distinguish universal emotions from culturally modulated expressions (display rules).
What are the key theories of emotion to know for the MCAT?
Major Theories of Emotion (MCAT Summary Table)
Theory | Order of Events | Example | Mnemonic / Tip |
|---|---|---|---|
James-Lange | Stimulus → Physiological response → Emotion | You cry → then feel sad | I am afraid because I have consciously assessed that I am trembling, thus I am experiencing FEAR. |
Cannon-Bard | Stimulus → Physiological response + Emotion | You see a cat → heart races and feel happy at the same time | “Cannon fires both at once” |
Schachter-Singer | Stimulus → Physiological response → Cognitive appraisal → Emotion | Heart races → you evaluate situation → if safe = happy, if danger = fear | “SCHACTERWATSKI: ANALYSIS”: Emotion comes from analysis |
Lazarus | Stimulus → Cognitive appraisal → Emotion + Physiological response | You label situation as dangerous → then feel fear and heart starts racing | “Body is a Lazy Lazarus”: Mind acts before the body |
MCAT Tips
Be ready to differentiate theories by order.
Know that James-Lange and Schachter-Singer both begin with physiological response but differ in the subconscious vs. conscious evaluation.
Lazarus theory is the only one where cognitive appraisal comes BEFORE anything else.
YERES-DODSON LAW: PEOPLE PERFORM BEST WHEN MODERATELY AROUSED
What to know about stress for the MCAT?
Lazarus’s Appraisal Theory of Stress (MCAT Version)
Same dude who said we cognitively label FIRST then have physiological response
Stage | Description | MCAT Example |
|---|---|---|
Primary Appraisal | You evaluate the nature of the stressor: | |
- Benign/Positive: No threat, or actually something good | Seeing your favorite wrestler return in the Royal Rumble = excitement! | |
- Neutral: Unimportant or irrelevant | A stranger walks past you with no eye contact = no emotional reaction | |
- Negative: Perceived as a threat | Seeing the Sigma Boy charging at you with a knife = stress trigger | |
Secondary Appraisal | You assess your resources and options to cope with the threat | |
- Can I handle this? What are the consequences? | “Can I run away fast enough?” “Can I hide behind the table?” | |
- Involves evaluating: harm, threat, and challenge | Harm = already injured; Threat = potential harm; Challenge = possible growth |
MCAT Takeaways
Stress is a two-stage process: Primary (what is it?) → Secondary (can I handle it?)
The Lazarus theory places stress as the result of appraisal, not the stimulus itself.
Use "Sigma Boy might stab me" as a vivid example of negative primary + urgent secondary appraisal.
4 MCAT Categories of Stressors
Category | Description | Example |
|---|---|---|
1. Significant Life Changes | Major transitions or shifts that require adjustment | Moving to a new state (e.g., Ohio), starting college, getting divorced |
2. Catastrophic Events | Large-scale, unpredictable disasters perceived as threatening by most people | Tornado, earthquake, or a sky-demon tearing through Ohioan infrastructure |
3. Daily Hassles | Minor, frequent irritations or demands of daily life | Running late, traffic, yelling at a dealership, or an Ohio goblin kidnapping your child |
4. Ambient Stressors | Global, background stressors that are chronic and often unnoticed | Noise, light pollution, smog in Beijing, or demons flying across the sky in Ohio |
MCAT Key Points
All four types can contribute to chronic stress and impact health.
Daily hassles and ambient stressors are often underestimated but most impactful over time.
Primary vs. secondary appraisal still applies to how each stressor is experienced.
Biological Responses to Stress Response
Neurotransmitters & Hormones of the Stress Response
Substance | Type | Released By | Function in Stress |
|---|---|---|---|
Epinephrine (Adrenaline) | Hormone & Neurotransmitter | Adrenal medulla (inner adrenal gland) | Increases heart rate, blood pressure, dilates pupils, bronchodilation |
Norepinephrine (Noradrenaline) | Hormone & Neurotransmitter | Adrenal medulla & sympathetic neurons | Vasoconstriction (especially in skin/GI), increases alertness, raises BP |
Cortisol | Hormone | Adrenal cortex (outer adrenal gland) | Increases glucose metabolism, suppresses immune system, longer-term stress |
Acetylcholine (ACh) | Neurotransmitter | Preganglionic neurons (both SNS & PNS) | Stimulates adrenal medulla to release epi/norepi (in sympathetic system) |
CRH (Corticotropin-Releasing Hormone) | Hormone | Hypothalamus | Signals anterior pituitary to release ACTH |
ACTH (Adrenocorticotropic Hormone) | Hormone | Anterior pituitary | Stimulates adrenal cortex to produce cortisol |
MCAT-Style Pathways to Know
Sympathetic Nervous System (Fast/Short-Term Stress):
Hypothalamus → Sympathetic nerves → Adrenal medulla
Releases epinephrine & norepinephrine
HPA Axis (Slow/Long-Term Stress):
Hypothalamus (CRH) → Pituitary (ACTH) → Adrenal cortex (Cortisol)
MCAT Flashcard Takeaways
Epinephrine = fight-or-flight; short-term
Cortisol = longer-term stress, glucose regulation, immune suppression
Adrenal medulla = catecholamines, adrenal cortex = cortisol
CRH → ACTH → Cortisol = classic HPA axis
Everything you need to know about stress for the MCAT
Stress Response Overview
Autonomic Nervous System (ANS) + Limbic System + Reticular Activating System (RAS) work together to process stress and emotions.
RAS (midbrain): Controls alertness and arousal.
Midbrain Structures: Cerebral peduncle, corpora quadrigemina, cerebral aqueduct.
Sympathetic Nervous System (Fight or Flight):
↑ Heart rate, ↑ respiration → more oxygen and energy
↑ Peripheral vasoconstriction → prioritizes core organ perfusion
↓ Digestion, ↓ immune activity
Adrenal Glands:
Adrenal medulla → Epinephrine & Norepinephrine (short-term stress)
Adrenal cortex → Cortisol (long-term stress)
Tend-and-Befriend Response:
Promotes seeking social support
Driven by oxytocin, especially in females (linked to estrogen)
General Adaptation Syndrome (Hans Selye)
Alarm: Acute stress kicks in (↑ HR, adrenaline spike)
Resistance: Prolonged cortisol release, coping mechanisms engaged
Exhaustion: Immune suppression, tissue damage, ↑ risk of illness
Physical Effects of Chronic Stress
System | Effects |
|---|---|
Cardiovascular | ↑ BP → vessel damage → ↑ risk of CAD (esp. coronary arteries) |
Metabolic | ↑ Cortisol & glucagon → ↑ blood glucose → ↑ diabetes risk |
Reproductive | ↓ Fertility in women (energy conservation); impotence in men |
Immune | Short-term = inflammation; long-term = suppressed immunity |
Brain & Behavioral Effects
Hippocampus: Memory → atrophies under chronic stress
Prefrontal Cortex: Judgment & control → atrophies → poor decision-making
Amygdala: Fear and anxiety → becomes hyperactive
Key emotional/behavioral consequences:
Depression: Anhedonia (↓ pleasure); perceive more stress
Learned Helplessness: Perceived loss of control → impaired coping
Anger: Type A personalities → ↑ risk of heart disease
Anxiety: Hyperactivation of amygdala
Addiction: Substance abuse as maladaptive coping → worsens stress cycle
Stress Management (Coping)
Psychological Strategies:
Perceived control → major factor in resilience
Optimism → improves outcomes and motivation
Social support → reduces cortisol, improves recovery
Behavioral Techniques:
Exercise → physical outlet, ↑ endorphins
Meditation → ↓ HR, ↓ BP, ↓ cholesterol
Religious/Spiritual involvement → lifestyle structure + community
Cognitive flexibility → reframing stressors; improved adaptability (CBT helps here)
Key MCAT Takeaways:
Stress hormones: Epinephrine (short-term), Cortisol (long-term)
Key brain areas: Hippocampus (memory), Amygdala (fear), PFC (judgment)
Stress = systemic: cardiovascular, immune, reproductive, metabolic impacts
General Adaptation Syndrome = alarm → resistance → exhaustion
Coping = protective: exercise, social support, CBT, optimism, control
What to know about the biological basis of behavior for the MCAT?
Muscle Stretch Reflex:
A monosynaptic reflex arc with:
Afferent neuron (stimulus): detects stretch via muscle spindle
Efferent neuron (response): causes same muscle to contract
Example: Knee-jerk reflex:
Hammer taps tendon → stretches quadriceps
Stretch sensed by muscle spindles
Signal sent to spinal cord → LMN activates quads
Simultaneously, antagonist muscle (hamstring) is inhibited to allow proper movement (reciprocal inhibition)
Major Neurotransmitters & Their Origins
Glutamate
Main excitatory NT in CNS
Involved in cortex activation via reticular activating system (RAS) → important for consciousness
GABA (brain) & Glycine (spinal cord)
Main inhibitory NTs
Acetylcholine (ACh)
Released by Basalis & septal nuclei to cerebral cortex
Used by lower motor neurons (LMNs) and autonomic nervous system (ANS)
Histamine
Produced by hypothalamus
Norepinephrine (NE)
Produced in locus coeruleus (pons)
Also involved in ANS, though less than ACh
Serotonin (5-HT)
Released by raphe nuclei (midbrain, pons, medulla)
Dopamine (DA)
Produced in ventral tegmental area (VTA) and substantia nigra
Involved in reward, motor control, and Parkinson’s pathology
Gene-Environment Interaction Nature vs. nurture. Ex. Attractive baby and hideous baby. As a result, attractive baby receives more attention and is more sociable and well-adjusted. But say both have genes that predispose for depression, that are triggered by environment. Beautiful baby’s genes are not activated, while ugly baby’s genes are making proteins all the time since his life is tougher.
What are the 5 theories of motivation?
Theory | Key Idea | Example |
|---|---|---|
Evolutionary | Behavior is driven by instincts that promote survival and reproduction. | Babies crying, sleeping, feeding instinctively. |
Drive-Reduction Theory | Needs cause drives (aroused states), which motivate behavior to restore homeostasis. | Thirst → drink water; Fatigue → sleep. |
Optimum Arousal Theory | Motivation to reach an optimal level of arousal (not too low or too high). | Going to an amusement park for stimulation. |
Cognitive Theory | Thoughts and expectations guide behavior (intrinsic/extrinsic motivation). | Studying because you enjoy learning. |
Maslow’s Hierarchy of Needs | Motivation progresses through a pyramid of needs: physiological → safety → love → esteem → self-actualization. | Seeking food before self-esteem. |
What is the ABC Model of Attitude?
What are the 4 theories on how our attitudes influence behavior?
Attitude = Affective + Behavioral + Cognitive
Component | Definition | Example |
|---|---|---|
Affective | Emotional reaction or feeling toward an object/event | "I love yoga." / "I’m frightful of rollercoasters." |
Behavioral | How you behave or act toward the object/event | "I go to class weekly." / "I will ride the carousel." |
Cognitive | Thoughts, beliefs, or knowledge about the object/event | "I believe yoga relaxes me." / "Rollercoasters are stupid." |
4 Theories on how our attitudes influence behavior
Theory | Core Idea | Key Components / Factors | Example |
|---|---|---|---|
Theory of Planned Behavior | Behavior is determined by intentions, which come from attitude, social norms, and control. | - Attitude toward behavior - Subjective norms - Perceived behavioral control | "I like studying (attitude), my peers value it (norm), and I can manage my time (control)." |
Attitude-to-Behavior Process Model | Event triggers attitude, which + knowledge = behavior | - Event → attitude - Attitude + stored knowledge → interpretation → behavior | Junk food seen as unhealthy → doesn’t eat chips due to past family health issues. |
Prototype Willingness Model | Behavior shaped by intentions, willingness, and social modeling (prototype behavior) | - Past behavior - Attitudes - Subjective norms - Intentions - Willingness - Prototypes (social role models) | Peer pressure and willingness lead teen to try vaping even without intent. |
Elaboration Likelihood Model | Persuasion route (central vs. peripheral) influences attitude and behavior change | Central route: QUALITY of arguments Peripheral route: cues like appearance, status | Convinced by a doctor's logical argument (central) or celebrity endorsement (peripheral). |
Freud’s Iceberg Theory of Personality (Psychodynamic Perspective)
Component | Location | Function |
|---|---|---|
Id | Unconscious | Primitive drives, pleasure principle, immediate gratification (e.g., hunger, libido) |
Superego | Mostly unconscious | Internalized morals, guilt, societal values (“shoulds”) |
Ego | Mostly conscious | Mediates between id & superego, based on the reality principle (what’s socially acceptable) |
Comparison of the 5 Personality Theories
Comparison of the 5 Personality Theories
Theory | Key Figures | Core Beliefs | Conscious vs. Unconscious | Key Concepts / Tools | MCAT Notes |
|---|---|---|---|---|---|
Humanistic | Abraham Maslow, Carl Rogers | People are inherently good and driven toward self-actualization | Conscious | Self-concept, genuineness, acceptance, hierarchy of needs | Emphasizes personal growth; contrasts with Freud's deterministic approach |
Biological Theory | Hans Eysenck, Jeffrey Alan Gray, C Robert Cloninger | Personality is genetically determined; brain systems influence behavior | Biological basis | Temperament, dopamine, twin studies, fight-or-flight systems | Genetics + brain structures shape traits; includes evidence from twin studies |
Behaviorist Theory | BF Skinner, Ivan Pavlov | Personality is learned from environment via conditioning | Neither (observable) | Operant (Skinner) and classical (Pavlov) conditioning | Deterministic and environment-based; focuses only on behavior, not thoughts |
Trait Theory | Gordon Allport Raymond Cattel
| Personality = patterns of stable traits | Descriptive only | Cardinal/Central/Secondary traits 16personality traits OCEAN, factor analysis | Trait categories describe but don't explain personality; Big Five often appears on MCAT |
Social Cognitive Theory | Albert Bandura | Behavior is a mix of cognition, learning, and environment (reciprocal) | Cognitive + Social | Observational learning, Bobo Doll, AMIM (Attention, Memory, Imitation, Motivation) | Bridges behaviorist and cognitive models; learning ≠ performance; emphasizes modeling effects |
Summarize the Three Clusters of Personality Disorders (A, B, and C)
MCAT Takeaways:
Personality disorders are long-term patterns of thoughts and behaviors that deviate from social norms.
Divided into three clusters (A, B, C) based on similar features.
Know the descriptive patterns of each cluster—not the specific disorders—for the MCAT.
Cluster | Description | Key Traits | Example Disorders (for context only) |
|---|---|---|---|
A | Odd or Eccentric | Social withdrawal, suspicion, peculiar thinking | Paranoid, Schizoid, Schizotypal |
B | Dramatic, Emotional, Erratic | Intense emotions, unstable relationships | Antisocial, Borderline, Histrionic, Narcissistic |
C | Anxious or Fearful | Anxiety, avoidance, obsessive behavior | Avoidant, Dependent, Obsessive-Compulsive |
What are the biological basises of 3 Major Neurological Disorders?
Biological Basis of Major Neurological Disorders
Disorder | Affected Brain Regions | Key Features & Symptoms | Biological Markers / Causes | Treatment / Notes |
|---|---|---|---|---|
Depression | ↓ Frontal lobe activity, ↑ Limbic system activityInvolves hypothalamus, raphe nuclei, locus coeruleus, VTA | Hopelessness, loss of interest, fatigue, appetite/sleep changes | - ↓ Serotonin (raphe nuclei) ↓ Norepinephrine (locus coeruleus) ↓ Dopamine (VTA)- Hypothalamic stress hormone imbalance (↑ cortisol)- Neural plasticity changes | SSRIs, SNRIs, MAO inhibitors (↑ monoamines in synapse) Psychosocial factors also play a role |
Alzheimer’s Disease | Atrophy of cerebrum, especially temporal → parietal/frontal lobesLoss of nucleus basalis (↓ ACh) | Memory loss, progressive cognitive declineLater loss of ADLs | - β-amyloid plaques (outside neurons)- Tau tangles (inside neurons)- ↓ Acetylcholine- ApoE4 mutation- High BP risk factor | No cure Higher education/mental stimulation protective Early synaptic dysfunction |
Parkinson’s Disease | Substantia nigra (in brainstem, part of basal ganglia) → ↓ dopamine to striatum | Tremor, rigidity, shuffling gait, bradykinesia Later cognitive & behavioral symptoms | - Loss of dopaminergic neurons (especially in SN) - Lewy bodies with clumped α-synuclein- Genetic mutations, toxins (e.g., pesticides) | L-DOPA, dopamine agonists Stem cell therapy under study |
Key MCAT Takeaways:
Depression: Monoamine hypothesis (↓ serotonin, dopamine, norepinephrine); abnormal limbic-frontal activity.
Alzheimer’s: Plaques (β-amyloid), tangles (tau), ↓ acetylcholine; starts in temporal lobe → spreads.
Parkinson’s: Dopaminergic neuron loss in substantia nigra; presence of Lewy bodies (α-synuclein); affects basal ganglia motor circuit.
Group Polarization vs. Groupthink
Group Polarization vs. Groupthink
Concept | Definition | Key Feature | Example |
|---|---|---|---|
Group Polarization | Tendency of a group to make decisions that are more extreme than the initial inclinations of its individual members. | Reinforces preexisting beliefs or attitudes → becomes stronger or more extreme. | A jury discusses a case where most members lean toward a light punishment. After discussion, they vote for a much harsher sentence than any initially proposed. |
Groupthink | When group members suppress dissenting opinions in order to maintain harmony and consensus, often leading to poor decisions. | Desire for unity overrides critical evaluation. | A government team ignores warnings from an engineer and launches a faulty space shuttle to avoid disagreement—Challenger disaster is a real-life example. |
MCAT Tip:
Group polarization = ideas get more EXTREME after discussion.
Groupthink = poor decisions made due to pressure to conform and avoid conflict.
Conformity v Obedience and different types of Conformity
Conformity vs. Obedience
Term | Definition | Example |
|---|---|---|
Conformity | Adjusting behavior/thought to match a group | Dressing casually because your friends do |
Obedience | Changing behavior in response to authority | Following a supervisor's instructions |
Types of Conformity
Type | Description | Example |
|---|---|---|
Compliance | Conforming to gain reward or avoid punishment; usually temporary | Paying taxes to avoid fines to COMPLY |
Identification | Conforming to be like someone you admire; dependent on continued respect | Dressing like a celebrity because you want to BE LIKE THEM |
Internalization | Integrating beliefs into your own value system; deepest and most lasting form of conformity | Adopting meditation because YOU BELIEVE IN IT |
Social Influence Types
Type | Definition | Example |
|---|---|---|
Normative Social Influence | Conforming to be LIKED/ACCEPTED even if you privately disagree | Laughing at a joke you don’t find funny |
Informational Social Influence | Conforming because others seem more knowledgeable | Following crowd during a fire drill because you think THEY KNOW WHATS UP |
ANOMIE= Breakdown of social bonds between individual and community (loss of norms → alienation)
Asch Conformity Study v. Milgram Obedience Experiment
Asch Conformity Study (1951)
Category | Details |
|---|---|
Researcher | Solomon Asch |
Purpose | To investigate the extent to which social pressure from a majority group could affect conformity |
Participants | Male college students |
Setup | Participants asked to match line lengths; confederates (actors) gave wrong answers intentionally |
Key Concept | Conformity — adjusting behavior to align with a group |
Findings | 75% conformed at least once; 37% conformed consistently |
Social Influence Types | - Normative Influence: desire to fit in - Informational Influence: assumption that the group is correct |
Reasons for Non-conformity | Confidence in personal judgment or resistance to social pressure |
Criticisms | - All male sample - Lab setting lacks ecological validity - Demand characteristics possible |
MCAT Takeaways | Group pressure can strongly influence perception and decision-making even without formal authority |
Milgram Obedience Experiment (1961)
Category | Details |
|---|---|
Researcher | Stanley Milgram |
Purpose | To test how far individuals would go in obeying an authority figure, even if it meant harming another person |
Participants | Adult male volunteers |
Setup | "Teacher" instructed to shock "learner" for wrong answers; shocks increased in voltage up to 450V |
Key Concept | Obedience — compliance with authority, even when it conflicts with personal morals |
Findings | 65% of participants delivered the maximum shock; many showed visible distress |
Mechanisms of Obedience | - Authority figure assumed responsibility - Gradual escalation - Lack of clear escape |
Psychological Factors | - Just World Phenomenon -Fundamental Attribution Error -Self-serving Bias |
Ethical Issues | Deception, emotional stress, questionable consent |
MCAT Takeaways | Authority can override morality; situational pressure often trumps individual character |
Zimbardo’s Stanford Prison Experiment
Category | Details |
|---|---|
Researcher | Philip Zimbardo |
Year | 1971 |
Purpose | To investigate how situational roles and authority influence behavior, particularly in prisons |
Participants | 18 healthy, middle-class male college students; randomly assigned as guards or prisoners |
Setup | Simulated prison in Stanford’s basement. Guards were told not to physically harm but could assert psychological control. |
Key Events | Day 1 uneventful Day 2: Prisoner rebellion Day 3–5: Escalation of abuse, hunger strikes, solitary confinement, psychological collapse |
Findings | -Guards quickly adopted authoritarian roles -Prisoners internalized submissive roles -Zimbardo lost objectivity by acting as warden |
Key Psychological Concepts | - Situational attribution over dispositional -Deindividuation (prisoners as numbers) -Cognitive dissonance in guards -Internalization of roles |
Ethical Issues | - Lack of informed withdrawal - Emotional trauma - Zimbardo’s dual role impaired objectivity - Poor operational definitions and controls |
Criticisms | - Demand characteristics - Selection bias (who volunteers to simulate prison?) - Small sample size |
MCAT Takeaway | Situations—not just personality traits—can powerfully influence human behavior, especially in authority-role dynamics and loss of personal identity. |
What are the different group behaviors for the MCAT:
Bystander Effect & Deindividuation
Concept | Definition | Key Mechanism | Example |
|---|---|---|---|
Bystander Effect | People are less likely to help when others are present | Diffusion of responsibility | Kitty Genovese case (38 witnesses, no help) |
Diffusion of Responsibility | People feel less personally responsible when in a group | Group size increases this effect | More bystanders = less individual action |
Deindividuation | Loss of self-awareness and restraint in groups, leading to deviant behavior | Anonymity within group | Black Friday riots, online trolling |
Social Facilitation vs. Social Loafing
Concept | Definition | Effect of Group Presence | Example |
|---|---|---|---|
Social Facilitation | Presence of others increases arousal, improving performance on easy tasks | Enhances DOMINANT RESPONSE | Practiced speech is delivered better in a crowd |
Social Loafing | People put in less effort in a group if individual performance isn’t evaluated | Reduces accountability | SLACKING during group projects |
Agents of Socialization
Agent | Role in Socialization | Example |
|---|---|---|
Family | Primary agent; teaches norms, values, language, caregiving | Parental influence on behavior, socioeconomic differences |
School | Teaches discipline, order, cooperation; includes hidden curriculum | Learning to obey authority, raise hand before speaking |
Peers | Influence identity, social interaction, preferences | Peer pressure, exposure to music/media/fashion |
Mass Media | Disseminates culture, norms, stereotypes; shapes expectations and beliefs | TV shows promoting gender roles, violence in media |
MCAT Key Takeaways
Bystander Effect is stronger with more people; reduced in smaller groups.
Social Facilitation improves simple tasks but worsens complex ones if you're unprepared.
Social Loafing is reduced when individual contributions are tracked.
Deindividuation lowers personal accountability → riskier behavior.
Socialization occurs across life stages and is shaped by family, school, peers, and media.
Types of Learning
Type | Definition | Examples |
|---|---|---|
Nonassociative | Learning from repeated exposure to a single stimulus | Habituation, Sensitization |
Associative | Learning from linking two stimuli or a behavior with consequence | Classical & Operant Conditioning |
Classical Conditioning: Ivan Pavlov
Term | Definition | Example |
|---|---|---|
Unconditioned Stimulus (US) | Naturally triggers a response | Carrot for a guinea pig |
Unconditioned Response (UR) | Natural response to US | Excitement |
Neutral Stimulus (NS) | Doesn’t trigger a response initially | Refrigerator door sound |
Conditioned Stimulus (CS) | NS becomes CS when it triggers same response as US after pairing | Refrigerator door (after conditioning) |
Conditioned Response (CR) | Response to CS | Excitement at door sound |
Extinction | CS presented without US → response fades | Door opens with no carrot → less excitement |
Spontaneous Recovery | CR returns after extinction | Suddenly excited again after hearing door |
Generalization | Similar stimuli elicit same response | Desk drawer also excites guinea pig |
Discrimination | Differentiation between similar stimuli | Doesn’t react to dresser drawer |
Operant Conditioning: BF Skinner
Type | Definition | Example |
|---|---|---|
Positive Reinforcement | Add something to increase behavior | Gas card for safe driving |
Negative Reinforcement | Remove something to increase behavior | Buzzer stops when seatbelt fastened |
Positive Punishment | Add something to decrease behavior | Speeding ticket |
Negative Punishment | Remove something to decrease behavior | License taken away |
Reinforcement Schedules
Schedule | Definition | Example |
|---|---|---|
Fixed Ratio | Reinforce after fixed # of behaviors | Bonus every 5 cars sold |
Variable Ratio | Reinforce after average # of behaviors | Slot machine |
Fixed Interval | Reinforce after fixed time interval | Paycheck every 2 weeks |
Variable Interval | Reinforce after varying time intervals | Surprise bonus |
FIXED INTERVAL: LEAST EFFECTIVE
VARIABLE RATIO: MOST EFFECTIVE
Shaping, Insight, and Latent Learning
Concept | Definition | Example |
|---|---|---|
Shaping | Reinforce successive approximations of a behavior | Teaching a headstand, rewarding steps |
Insight Learning | Sudden realization using previous knowledge | Aha! moment solving a puzzle |
Latent Learning | Learned behavior not demonstrated until needed | Knowing maze path but not showing it yet |
Shaping, Insight, and Latent Learning
Concept | Definition | Example |
|---|---|---|
Shaping | Reinforce successive approximations of a behavior | Teaching a headstand, rewarding steps |
Insight Learning | Sudden realization using previous knowledge | Aha! moment solving a puzzle |
Latent Learning | Learned behavior not demonstrated until needed | Knowing maze path but not showing it yet |
Aversive Learning
Type | Definition | Example |
|---|---|---|
Escape | Behavior eliminates EXISTING unpleasant stimulus | Fire alarm rings → run outside |
Avoidance | Behavior PREVENTS stimulus from occurring in the FIRST PLACE | Leave building when you smell smoke |
MCAT Takeaways
Classical Conditioning = automatic associations (Pavlov)
Operant Conditioning = behavior shaped by consequences (Skinner)
Reinforcement = increases behavior; punishment = decreases behavior
Variable ratio = most resistant to extinction
Escape = get away from stimulus; avoidance = prevent it entirely
Theories of Attitude and Behavior Change for the MCAT
Persuasion and the Elaboration Likelihood Model (ELM)
Path | Processing Style | When Used | Result |
|---|---|---|---|
Central | Deep, thoughtful, content-based | When topic is important or person is engaged | LASTING attitude change |
Peripheral | Surface-level, superficial cues | When uninterested or distracted | Temporary attitude change |
Persuasion Influencers:
Message Characteristics – clarity, logic, quality of arguments
Source Characteristics – credibility, trustworthiness, appearance
Target Characteristics – listener traits like mood, intelligence, self-esteem
Reciprocal Determinism (Bandura)
Key Idea: Behavior is shaped by a constant interaction between:
Cognition (thoughts, motivations)
Environment (social context)
Behavior (actions)
Example:
You like soccer → join a team → hang out with players
OR: You hang out with players → grow interest → join team
Personal Control
Type | Definition | Effect |
|---|---|---|
Internal Locus | You control your fate | Better stress coping, achievement, lower depression |
External Locus | Outside forces control outcomes | Higher stress, worse outcomes |
Learned Helplessness | Repeated failures → perceived loss of control | Passive, avoidant behavior |
Tyranny of Choice | Too many options → decision paralysis, regret | Less satisfaction, reduced well-being |
Self-Control
Definition: Ability to SUPPRESS short-term temptations for long-term goals.
Famous Experiment: Marshmallow Test – kids who delayed gratification had better outcomes years later.
Ego Depletion:
Self-control is a LIMITED RESOURCE (like a muscle).
Overuse weakens short-term capacity.
Training in one area can generalize.
Ways to Improve Self-Control:
Change Environment – e.g., remove temptations
Operant Conditioning – reinforce good behavior
Classical Conditioning – pair healthy substitutes
Avoid Total Deprivation – increases craving, risk of relapse
MCAT Key Takeaways:
Central route: Lasting persuasion from thoughtful engagement.
Reciprocal determinism: Tri-directional influence of behavior, thoughts, and environment.
Internal control improves outcomes; external worsens them.
Learned helplessness explains avoidance after uncontrollable events.
Too much choice → anxiety and regret.
Self-control can be trained but is exhaustible.
Self-Identity Concepts for the MCAT
Self-Concept and Development
Self-concept = How we perceive and evaluate ourselves (self-awareness)
Two components of development:
Existential self – awareness of being separate, constant (develops early)
Categorical self – understanding that we exist in categories (age, gender, traits, careers)
Carl Rogers' 3 Components of Self-Concept:
Component | Description |
|---|---|
Self-image | How we SEE ourselves (see an image) |
Self-esteem | VALUE we place on ourselves (esteemed value) |
Ideal self | Who we strive to become (what we IDEALLY will become) |
Congruence between REAL and IDEAL self → positive self-concept
Incongruence → leads to dissatisfaction or confusion
Social Identity Theory (Tajfel & Turner)
Two parts of identity:
Personal identity – traits unique to you (e.g., kind, funny)
Social identity – group memberships (e.g., student, athlete)
3 Steps in Social Identity Formation:
Categorization – GROUPING ourselves and others (e.g., race, profession)
Identification – adopting group identity and norms
Comparison – boosting self-esteem by comparing our group to others
→ Basis for in-group bias and prejudice
Self-Esteem vs. Self-Efficacy
Concept | Definition | High Level Traits | Low Level Traits |
|---|---|---|---|
Self-esteem | One's overall sense of self-WORTH | Self-accepting | Self-critical |
Self-efficacy | Belief in ability to succeed at tasks | Persistent, confident (RISE) | Doubtful, avoids challenges (FALL) |
Sources of Self-Efficacy (ALBERT BANDURA):
Mastery experiences (past success)
Social modeling (seeing others succeed)
Social persuasion (encouragement)
Psychological states (stress/mood management)
Key Insight: Self-esteem ≠ self-efficacy (e.g., a perfectionist may feel capable but not worthy)
MCAT Takeaways
Self-concept forms early, shaped by both personal and social identities.
Carl Rogers emphasized congruence between ideal and real self.
Self-efficacy is situational and can be strengthened; it is not the same as self-esteem.
Social Identity Theory explains how group affiliation contributes to self-concept and prejudice.
Locus of control affects motivation and resilience; internal locus promotes autonomy.
What are the different theories of development to know for the MCAT
Theories of Development – Comparative Table
Theory & Theorist | Focus of Development | Key Idea | Stages | Age Range | MCAT Notes |
|---|---|---|---|---|---|
Freud’s Psychosexual | Personality (unconscious) | Libido (sexual energy) focused on different body zones | 5 | 0 – puberty | Fixation if conflict not resolved; based on pleasure and tension |
Erikson’s Psychosocial | Personality (social conflicts) | Conflict between individual needs and societal demands | 8 | Entire lifespan | Successful resolution leads to virtue; failure leads to reduced functioning |
Vygotsky’s Sociocultural | Cognitive development through social context | Learning via social interaction, language, and culture | Not staged | Continuous | Zone of Proximal Development (ZPD), MKO, and internal speech |
Kohlberg’s Moral | Moral reasoning | Morality develops in stages through dilemmas and logic | 3 levels (6 stages) | Pre-adolescence → adulthood | Based on Heinz Dilemma; only some reach post-conventional morality |
Freud’s 5 Psychosexual Stages (Mnemonic: Old Age Parrots Love Grapes)
Stage | Age | Focus/Conflict | Fixation Outcome |
|---|---|---|---|
Oral | 0–1 yr | Mouth (feeding) | Dependency, aggression, nail-biting |
Anal | 1–2 yrs | Anus (toilet training) | Orderliness or messiness |
Phallic | 3–6 yrs | Genitals (Oedipus/Electra) | Sexual dysfunction, identification issues |
Latent | 6–12 yrs | None (social/exploration) | No adult fixation |
Genital | 12+ yrs | Genitals (mature sex) | Mentally healthy, other-focused |
Erikson’s 8 Psychosocial Stages
Stage | Age | Conflict | Virtue | Negative Outcome |
|---|---|---|---|---|
Trust vs. Mistrust | 0–1 yr | Are needs reliably met? | Hope | Mistrust, suspicion |
Autonomy vs. Shame/Doubt | 1–3 yrs | Can I act independently? | Will | Shame, low self-esteem |
Initiative vs. Guilt | 3–6 yrs | Can I initiate activities? | Purpose | Guilt, inhibition |
Industry vs. Inferiority | 6–12 yrs | Can I be competent? | Competence | Inferiority, modesty |
Identity vs. Role Confusion | 12–18 yrs | Who am I? | Fidelity | Confusion, rebellion |
Intimacy vs. Isolation | 18–40 yrs | Can I form close relationships? | Love | Isolation, loneliness |
Generativity vs. Stagnation | 40–65 yrs | Am I contributing? | Care | Stagnation, unproductivity |
Integrity vs. Despair | 65+ yrs | Was my life meaningful? | Wisdom | Regret, dissatisfaction |
Vygotsky’s Sociocultural Theory
Concept | Description |
|---|---|
Elementary Mental Functions | Attention, sensation, perception, memory (natural) |
Higher Mental Functions | Developed through social interaction with MKO |
Zone of Proximal Development | Range between what a child can do alone and with help |
Private Speech (Internal Speech) | Self-guidance through speech – vital for cognitive growth |
Kohlberg’s Moral Development Theory
Level | Stage | Focus |
|---|---|---|
Pre-Conventional | Obedience vs. Punishment | Avoid punishment |
Individualism & Exchange | Recognize different perspectives | |
Conventional | Good Boy/Good Girl | Conform to societal expectations |
Law and Order | Uphold law for social order | |
Post-Conventional | Social Contract | Laws may conflict with moral values |
Universal Ethical Principle | Follow internal moral principles (e.g., Gandhi) |
MCAT Key Takeaways
Freud & Erikson: Both emphasize early life stages, but Erikson extends into adulthood with social conflicts.
Vygotsky: Emphasizes social interaction and language in developing higher cognition.
Kohlberg: Focuses on how moral reasoning evolves, not behavior itself.
Vygotsky and Kohlberg are cognitive development theories
Freud and Erikson focus on personality development.
What to know on social influences for the MCAT?
Social Influences: Overview
Concept | Description | MCAT Key Examples/Associations |
|---|---|---|
Imitation | Basic form of social behavior, even in infants (e.g., sticking tongue out) | Mirror neurons, early development of empathy |
Roles | Social norms dictate expected behaviors by role (e.g., student, parent) | Zimbardo prison experiment, social scripts |
Reference Groups | Groups we compare ourselves to when shaping beliefs/behaviors | Political parties, religious groups, peer groups |
Culture & Socialization | Society/culture contributes to personal development through norms/values | Agents of socialization: family, school, media |
Social influences shape our identity, behaviors, and self-perception through:
Mead’s Theory of the Self (PPG)
George Herbert Mead proposed that the self develops through social interaction via 3 stages:
Stage | Description |
|---|---|
Preparatory | Imitation only; no understanding of others' perspectives |
Play | Role play; understands relationships and begins perspective-taking |
Game | Understands generalized other (society); recognizes multiple roles |
Mead’s “Me” v. “I” [How we’re perceived by society, our RESPONSE to society)
Component | Description | Analogy |
|---|---|---|
Me | The social self – how we think society sees us | "Me" = what society expects |
I | The response to the “Me” – our individual identity | "I" = my personal reaction |
Cooley’s “Looking Glass Self”
Step | Description |
|---|---|
1 | How do I appear to others? |
2 | What do others think of me? |
3 | Revise self-image based on perceived judgments |
Key Insight: We are shaped not by others' actual thoughts, but by what we imagine others think of us.
MCAT Key Takeaways
Imitation is observable in early infancy and may be tied to mirror neurons.
Roles and social expectations influence behavior (e.g., conformity in Zimbardo's study).
Reference groups serve as benchmarks for evaluating our own actions or beliefs.
Mead believed self-awareness develops through stages, culminating in the awareness of society’s views.
Mead's “I” = individual agency, “Me” = societal expectation.
Cooley’s Looking Glass Self emphasizes that self-image is socially constructed, but based on perceived, not actual, judgments.