Module 9- forensic mental health
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
canadas forensic mental health system created to provide a special legal pathway for people who are
unfit to stand trial
not criminally responsible on account of mental disorder NCRMD
the goal is not punishment alone, the system is designed to balance
public safety
fairness to the accused
treatment and stabilization
gradual reintegration into the community
federal level
general mental health concerns who are accused
in patient clinics (psychiatric hospitals, secure facilities, regional facilities)
provincial level
provincially mandated services (in patient and out patient clinics)
private clinics
examples of FMH services
fitness to stand trial assessment
not criminally responsible assessments
presentence assessments
offender designation assessments
risk assessment (general recidivism, violence risk, sexual violence, spousal assault)
fitness restoration
counselling services
substance treatment service
who ends up in FMH system
“Mentally disordered accused”
• Reason to question mental state at trial
or during commission of offence
• Either unfit to stand trial
• Or Not Criminally Responsible due to
Mental Disorder
• Both can be raised at any point in court
process
unfit to stand trial (s. 2, CCC; s. 672.xx, ccc)
• Most frequently requested forensic evaluation in North America
• In US upwards of 120,000 annually (kois et al., 2024)
• Presumption of fitness, until concerns are raised
• Can be raised at any point in trial process (but focuses on “at trial”).
(a) understand the nature or object of the proceedings,
(b) understand the possible consequences of the proceedings, or
(c) communicate with counsel;
Recent change: “Limited cognitive capacity test” vs. “fitness to stand trial test”
NCRMD
mental health concerns at time of offence
“No person is criminally responsible for an act committed or an omission
made while suffering from a mental disorder that rendered the person
incapable of appreciating the nature and quality of the act or omission or
of knowing that it was wrong”
can include additional high-risk designation
process through the system
a concern is flagged
assessment is ordered
either questions NCRMD or fitness-related
takes part in assessment
makes decision: accepts assessment vs rejects
reject = continue through court process as normal
accept = put under purview of provincial / territorial review board
provincial/ territorial review board
• Made up of interdisciplinary panel who makes decisions regarding
the treatment or management of someone found unfit or NCRMD
• Review each case annually (or more frequent)
• Unfit: remain under board until determined to be fit
• “Naturally restored”
• Treatment order
• Permanently unfit
• NCMRD: remain until determined safe for self and public
review boards must choose
the least
restrictive, necessary and appropriate
disposition, while treating public safety
as the paramount consideration
review board dispositions
detention in hospital > conditional discharge (typically living in the community under conditions set by the RB) > absolute discharge
what do we know about forensic populations
• Huge focus on NCRMD in Canada, why?
• Fitness evaluations may be more common, but
smaller portion found unfit
• Of 1,240 people under Ontario RB from
2014-2015, only 104 unfit (Chaimowitz et al.,
2022)
• Those found unfit likely under RB for shorter
periods of time
• E.g., natural restoration/treatment orders
National Trajectory Project
retrospective analysis of those found NCRMD in ontario, quebec, and BC between 2000-2008G
Goal “To assess the presence of provincial differences in the application of the law, to examine the characteristics of people with serious mental illness who come into conflict with the law and receive this verdict, and to investigate the trajectories of NCRMD–accused people as they traverse the mental health and criminal justice
systems.”
demographics
Male (84.4%, n = 1519)
• 36 years old (M = 36.56, SD = 12.42)
• High school education (49.2%, n = 623)
• Born in Canada (66.0%, n = 746)
• Primary dx: psychotic spectrum disorders (70.9%, n = 1,268); mood
disorders (23.2%, n = 414), comorbid substance use disorder (30.8%, n =
550
• Only 2.9% (n = 70) identified as FNIM
demographics - crime
• Assault: 25-33%
• Threats: 23-29%
• Property: 10-20%
• Offences attempting or causing
death: 4-11%
• Victims most likely to be related
to accused: ~33%
Recidivism
• Overall recidivism: 16.7%
• Those who committed “severe offence”: 6%
had any recidivism
• Recidivism for severe violence: 0.6%
• Remained low following absolute
discharge: 22%
Controversy around NCRMD populations
• Fears that FMH populations are especially dangerous likely to
recidivate (e.g., “ticking time bombs”)
• “Getting off easy”
• High profile cases are notable because they are rare
• Particularly high-profile recidivism
• Fear are largely unsupported
• Recidivism generally low, particularly for violent offences
relationship to alcohol
• Consumption pretty foundationally baked into
our culture
• Most commonly used substance amongst
Canadians (Statcan, 2017)
• 75-78% of those 15 and older in past 12
months
• 83-86% of those 20-24 in past 12 months
• 63-68% in past 30 days
• 18% 15+ will meet criteria for AUD, and >50%
drink more than rec (CAMH, 2023)
alcohol and pregnancy
• Alcohol as a teratogen: a substance that interferes with normal
fetal development and causes congenital disabilities (Jones & Smith, 1973;
Lemoine et al., 1968)
• Impacts arise due to prenatal alcohol exposure
• Despite knowledge of harm, estimated 10% of Canadian women
consume alcohol during pregnancy
how is FASD defined
• Changing terminology over time and context
• Fetal alcohol syndrome (FAS), Fetal Alcohol Syndrome Disorder (FASD),
Neurobehavioural disorder associated with prenatal alcohol exposure (ND-PAE)
• Different diagnostic systems: Guidelines for the Diagnosis of FASD,
DSM-V, the Australian Guide, Institute of Medicine Diagnostic Criteria,
and the CDC guidelines
• All broadly referring to the neurodevelopmental impacts on the brain
and body of those prenatally exposed to alcohol
Assessment of FASD
• Guidelines for Diagnosis commonly used in Canada (Cook et al., 2016)
Assessment process requires:
- Review of social and medical history
- Physical examination carried out by physician/pediatrician
- Multidisciplinary assessment process that could include case
coordinators, occupational therapists, SLPs, psychologists,
psychiatrists, clinical geneticist, etc.
Assessment General overview
1. Evidence of PAE
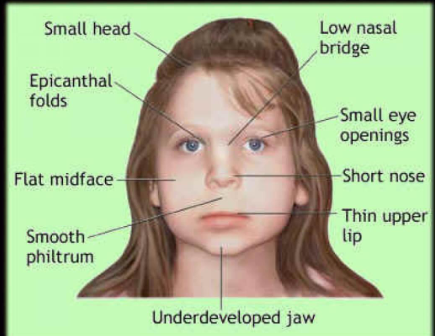
2. Presence of “sentinel facial features” (sometimes)
3. Severe impairment in three or more
neurodevelopmental domains
Evidence of PAE
• Self-report
• Other reliable source
• Institutional documentation
• Legal or medical problems r/d to alcohol at
time of pregnancy
• Both are often difficult to establish (or are
unaccepted)
sentinel facial features
1. Short palpebral
fissure
2. Smooth philtrum
3. Short upper lip
Problem: Only ~10% of
those with FASD have
sentinel facial features
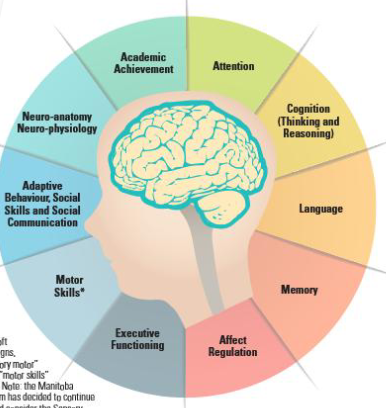
Neurodevelopmental domains
Severe impairment (greater than 2 SD from
mean) in at least three of these domains
Assessed through cognitive battery:
- Wechsler Intelligence Scale for Children
V/Wechsler Adult Intelligence Scale IV
- Wechsler Individual Achievement test
- Wide Range Assessment of Memory and
Learning or Wechsler Memory Scale
- Delis-Kaplan Executive Functioning
System
- Adaptive Behaviour Assessment System 3
Prevalence of FASD
• One of the most prevalent preventable neurodevelopmental disorders in the world (Lange et al.,
2017; Popova et al., 2018)
• Global estimate: 0.77% (22-61 million children and youth)
• South Africa ~11%
• Of 2555 students between 8 and 9, 2-3%
• Across entire population: ~4%
Higher in specific populations (Popova et al., 2019):
- Youth in care: 3.3%
- Correctional populations: 14.7%
- Indigenous communities: 7-18.8%
Barriers to assessment
Early identification is crucial, but often
not referred to assessment until age 9
• Domains tied to school
performance/only become obvious
at school age
• Family factors/stigma
• Lack of consensus about
identification and assessment
• Limited training or assessment
opportunities
• Costs (both time and money,
depending)
General impacts
Damage to central nervous system leading to (Popova et al., 2016, 2017):
• Craniofacial differences
• Restriction of growth
• Neurodevelopmental impairments
• Language and cognitive disorders
• Behavioural concerns
• Deficits in adaptive functioning
health and wellbeing
Identified over 400 comorbid conditions, most coming include (Popova et al., 2016;
Reid et al., 2023):
• Peripheral nerve dysfunction (90.9%)
• Impulse dysregulation (90.7%)
• Receptive (81.8%) and expressive (76.2%) language deficits
• Chronic ear infections (77.3%) and other hearing concerns (56.8-57.9%)
• Vision problems (54.1-71.4%)
• Chronic issues with sleep (55.0-85.0%)
• ADHD (51.2%)
environmental impacts
50-66% of children with FASD are exposed to Adverse Childhood
Events (ACES), reporting 3.4 on average (Flannigan et al., 2021; Reid et al., 2023)
• Compared to only 12% of general Canadians reporting 3+ (Joshi et al., 2021)
• Higher rates of substance use, risk-taking, worse mental health,
experiencing verbal, sexual or physical assault, classroom difficulties
(Flannigan et al., 2022; Gilbert et al., 2022; McLachlan et al., 2020; Reid et al., 2023)
societal impacts
$9.7 billion annually
in Canada; $3.9
billion associated with
legal system costs
• ~$1.1 million lifetime
costs
criminal legal involvement
• Having FASD does not directly lead you to legal involvement
• Increasing a cluster of risk factors that makes crime more
likely
prevalence
• 30-60% in trouble with law
• 19x more likely to be incarcerated to compared to youth without
• Rate 30x higher in correctional setting than general populations
• Majority of people identified upon exit were not previously diagnosed