Dermatology I
1/118
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
119 Terms
Acne Vulgaris Pathophysiology: 4 main factors:
hyperkeratinization, increased sebum, cultibacterium acnes overgrowth, and inflammatory response
Acne Vulgaris Tx mild comedonal Acne
1st line: topical retinoid monotherapy
ex: tretinoin, adapalene, tazarotene,trifarotene
S/E: erythema,dryness, flaking,pruritus, stinging
alternatives: azelaic acid,salicyclic acid, glycolic acid
Acne Vulgaris Tx mild papulopustular and mixed acne
1st line: topical retinoid and topical antimicrobial
options: benzoyl peroxide +- clindamycin
alternatives: benzoyl peroize + toical antibitoic or topical dapsone
Acne Vulgaris Tx Moderate
consider systemic therapy (oral antibiotics,hormonal agents, oral isotretinoin)
oral antibiotics: always combine w benzoyl peroxide to reduce resistance. limit to 12 weeks. 1st line minocycline and doxycycline
oral contraceptives can be used to tx inflammatory or noninflammatory acne in women w adult onset acne or perimenstrual flare ups.
Acne Vulgaris Tx severe
isotretinoin-teratogenicity so must be on oral contraceptives or signed pledge prior to initiating period adverse effects include dry skin comma cracked lips comma increase triglycerides and cholesterol comma and possible psychiatric effects like depression and suicidial ideation period.
Rosacea
Adult acne
More common in women
H&P: flushing, persisent erythema, telangiectasias, papulopustular lesions;ocular symptoms. absence of comedone and presence of neurovascular symptoms (flushing,feeling of warmth or burning or stinging sensation) distinguish rosacea from acne. phymatous change: rhinophyma (enlarged nose)
Rosacea Tx
1st step: lifestyle modifications, avoid triggers-(alcohol, hot/cold weather, hot drinks, hot baths, spicy food, sun exposure
Mild-moderate papulopustules: topical metronidazole, azelaic acid, ivermectin
moderate to severe papulopustules:oral tetracycline,doxycycline,laser for telengiesctasias.
facial erythema: topical brimonidine 0.33% gel
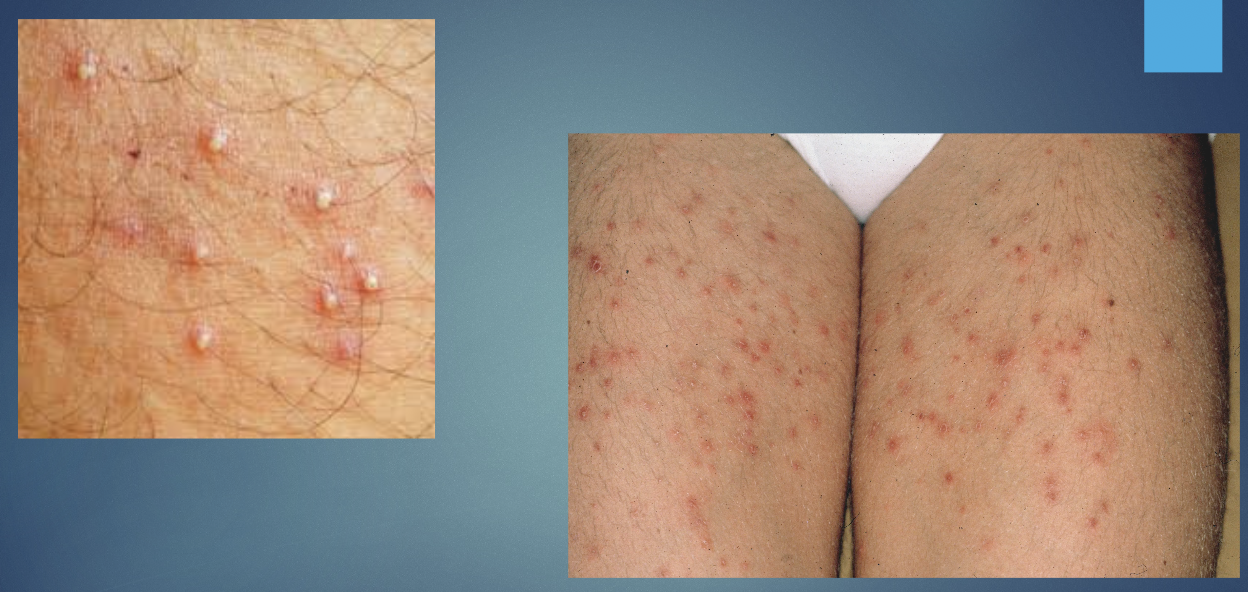
Folliculitis
Inflammation of a hair follice
Bacterial S. aureus most common cause;or fungal causes; hot tub exposure (psuedomonal folliculitis; commonly seen after hot tub, pool contamination)
H&P: single or clusters of perifollicular papules or pustules w/surrounding erythema at base of hair, often pruritic.
Folliculitis Tx
gentle cleansing, compresses.
mild: mupirocin (bactroban), topical clindamycin.
in more severe cases, oral antibiotics may need to be used (Keflex, Doxy). Fluroquinolone if hot tub folliculitis is severe (ciprofloxacin).
Folliculitis
Perioral dermatitis
Associated w topical steroid use.
H&P: Erythematous papules/pustules around mouth and periorificial areas sparing vermilion border.
Perioral dermatitis Tx
stop topical steroids, avoid skin irritants like makeup/skin products, topical metronidazole or pimecrolimus, oral tetracyclines if needed. oral tetracyclines if severe.

Perioral dermatitis
Acanthosis nigricans ON TEST
associated w obesity (most common cause), insulin resistance, and malignancy in adults (rarely-gastric adenocarcinoma, uterine, lung,breast, ovarian)
Pathophysiology: Insulin/IGF-mediated keratinocyte proliferation causing hyperpigmented VELVETY plaques.
H&P: Symmetric hyperpigmented velvety plaques in neck/skin folds.
Acanthosis nigricans TX ON TEST
Treat underlying cause, weight loss, topical retinoids, or vitamin D analog (calcipotriene) for faster resolution.

Acanthosis Nigricans
Hidradenitis suppurativa (Acne Inversa)
Pathophysiology: follicular occlusion/obstruction leading to inflammation,sinus tracts in apocrine-bearing areas and intertriginous areas (axilla most common)
H&P: painful inflamed nodules, abscesses, draining sinus tracts in axillae/groin.
Smoking/obesity are risk factors
Hidradenitis suppurativa (Acne Inversa) TX
Hygiene,weight loss, lifestyle changes
Hurley stages:
I: topical clindamycin first line,oral tetracycline if no improvement
II: oral doxy first line
III: clindamycine + rifampin
if above fail: consider biologics, wide surgical excision as last resort.

Hidradenitis suppurativa (Acne Inversa)
Hidradenitis suppurativa (Acne Inversa) 3 STAGES
Hurley stages:
I: inflammatory lesions WITHOUT sinus tracks or scarring
II and III= inflammatory lesions WITH tracs and scarring
Lipomas
Benign, soft, mobile, any size

Lipomas
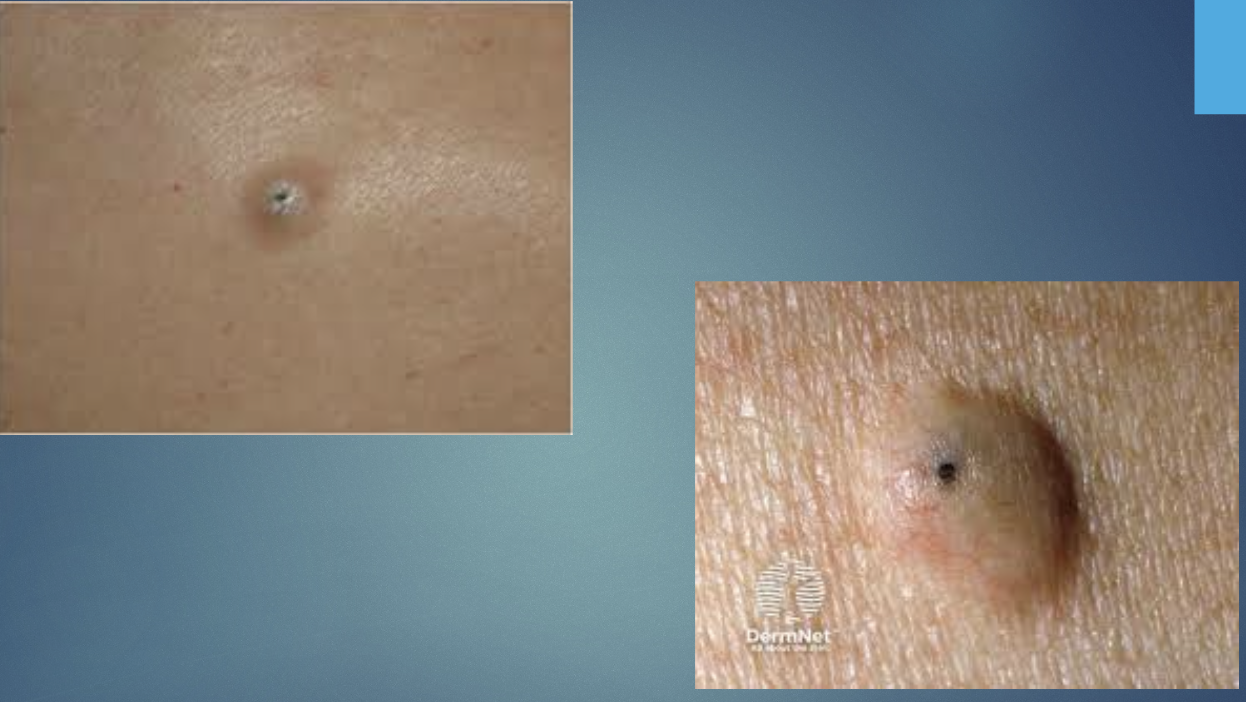
Epidermal Inclusion Cysts
Benign encapsulated subepidermal nodules filled w/fibrous tissue and keratinour (cottage cheese like) material. cysts result from plugging of folliculat orifices. original from the epidermis.
Pathophysiology: follicular occlusion w keratin-filled cyst (thick,cheesy)
H&P: FIRM, MOBILE NODULE W CENTRAL PUNCTUM (DARK COMEDONE OPENING); CAN BECOME INFLAMED/INFECTED. RUPTURED, INFECTED SYSTS; FLUCTULANT, PAINFUL, LARGE, ERYTHEMATOUS, FOUL SEMLLING YELLOWISH CHEESE-LIKE DISCHARGE.
Epidermal Inclusion Cysts TX
Observation, incision and drainage for acute infection, surgical excision for definitive treatment (usually done when not infected)
Epidermal Inclusion Cysts
Photosensitivity reactions
Pathophysiology: UV- triggered skin reaction via phototoxic or photoallergic mechanisms.
H&P: sun-exposed distributions of erythema, blistering, or eczematous lesions
Photosensitivity reactions TX
avoidance, photoprotection, topical steroids, stop offending drug
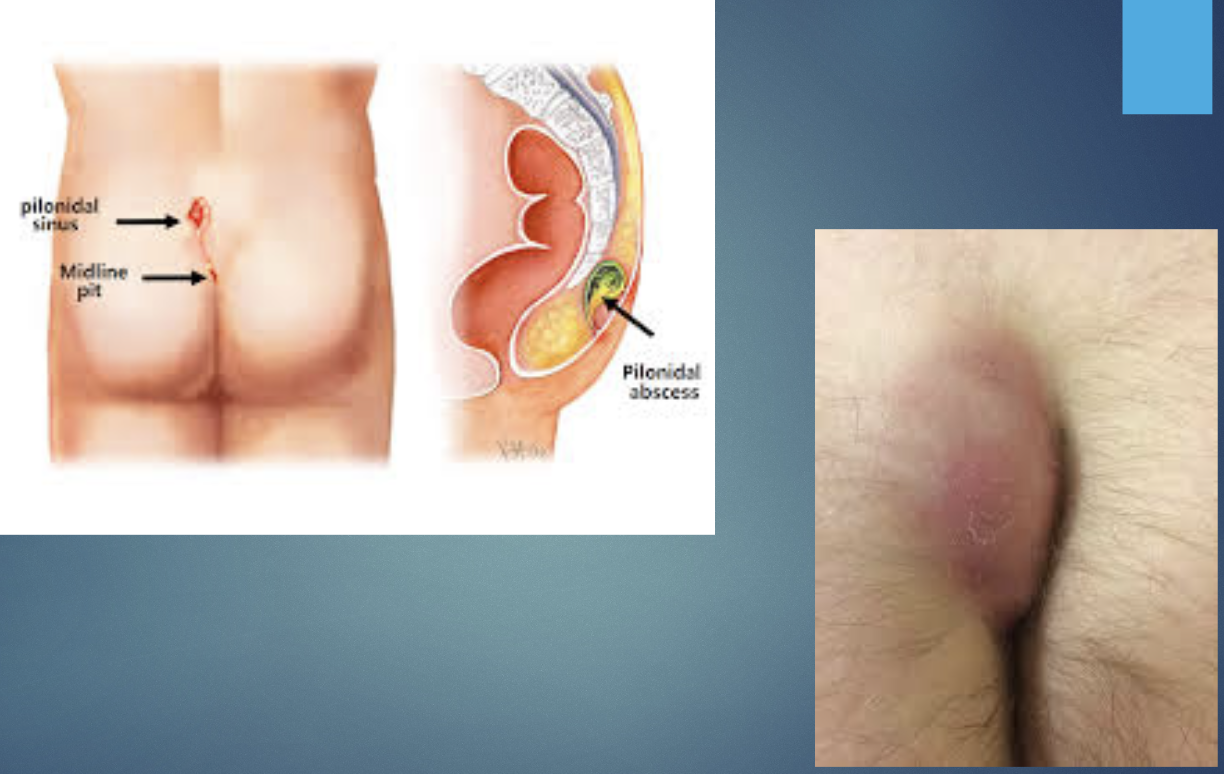
Pilonidal disease (cyst)
Pathophysiology: hair penetration and foreign body reaction in natal cleft leading to sinus formation.
H&P: painful medline sacrococcygeal abscess or draining sinus
Pilonidal disease (cyst) TX
Incision & drainage for acute abscess, surgical excision for chronic disease; hair removal measures
Pilonidal disease (cyst)
Urticaria (Hives)
Histamine related increased vascular permeability.
Common; acute often post-infection or drug;chronic > 6 weeks in some
Pathophysiology: release of vasodilators (histamine,bradykinin,prostalgnadins) from mast cells and basophils in the skin.
H&P: Pruritic transient wheals with central pallor; angiodema possible.
Urticaria (Hives) TX:
2nd gen antihistamines H1 blockers as less sedative ; consider sedating H1 antihistamine at nighttime in healthy individulas. avoid triggers, oral corticosteroids for severe flares. epinephrine if concern for airway compromise.

Urticaria (Hives)
Hyperhidrosis
Pathophysiology: overactivity of eccrine glands; sympathetic overactivity
H&P: excess focal sweating (palms,soles,axillae) impairing daily activities.
Hyperhidrosis TX
Topical aluminum chloride, iontophoresis,botulinum toxin, anticholinergics, surgery
Eczema
Pathophysiology: skin barrier dysfunction and inflammation
H&P: pruritic,erythematous,scaly patches; distribution depends on type.
Eczema TX
Emollients, topical steroids, treat triggers, and infections
Atopic dermatitis
Pathophysiology: barrier dysfunction, disordered immune response
Atopic traid: atopic dermatitis (eczema) + allergic rhinitis + asthma
H&P: pruritic, exzematous lesions in FLEXURAL areas
Atopic dermatitis TX
Chronic management: restore skin barrier/maintain skin hydration (skin emollients BID and within 3 mins of exiting bath. pat skin, dont rub dry.
Pruritis: nonsedating antihistamines
avoid triggers: heat, perspiration, wool, nickel,foods, allergens
Acute management:
topical corticosteroids first line often used w/emollients. antihistamines for itching. west dressings.
topical calcineurin inhibitor (tacrolimus,pimecrolimus) alternative to low potency steroids on face or skin folds
Moderate to severe disease: phototherapy, dupilumbad

Atopic dermatitis
Dyshidrotic eczema
affects palms/soles; recurrent
pathophysiology: unknown; possible atopic association and sweat-related triggers.
H&P: pruritic vesicles on lateral fingers, palms, soles.
Dyshidrotic eczema TX
topical steroids, emollients, cold compresses; severe cases may need systemic therapy

Dyshidrotic eczema
Contact Dermatitis
Pathophysiology: Irritant:direct damage. allergic:delayed hypersensitivity (type IV).
H&P: Erythema, vesicles, pruritus in exposed distribution.
Contact dermatitis TX
AVOIDANT MEASURES, EMOLLIENTS, TOPICAL STEROIDS; FOR ALLERGIC IDENTIFY/REMOVE ALLERGEN
Drug eruptions
pathophysiology: immune-mediated or toxic drug reactions.
H&P: morbilliform rash commonl can be urticarial, fixed, or severe (eg., SJS/TEN).
Drug eruptions TX
Stop culprit drug, supportive care; systemic steroids for severe reactions.
Lichen Planus
autoimmune disorder in patients with a genetic predisposition but may be caused by medications or be associated w disorders such as hepatitis c.
Lichen Planus 6 p’s
Purple, polygonal, planar, pruritic (itchy), papules, plaques w/fine scales
Lichen Planus- wickham striae
fine gray white lines on the skin lesions or oral mucosa mucosal involvement possible.
Lichen Planus TX
topical/systemic steroids (high or super high potency) is mainstay tx of LP w/occulsive dressings for trunk and extremity; intralesional corticosteroids for hypertrophic LP, retinoids, immunosuppressants for refractory disease.

Lichen Planus
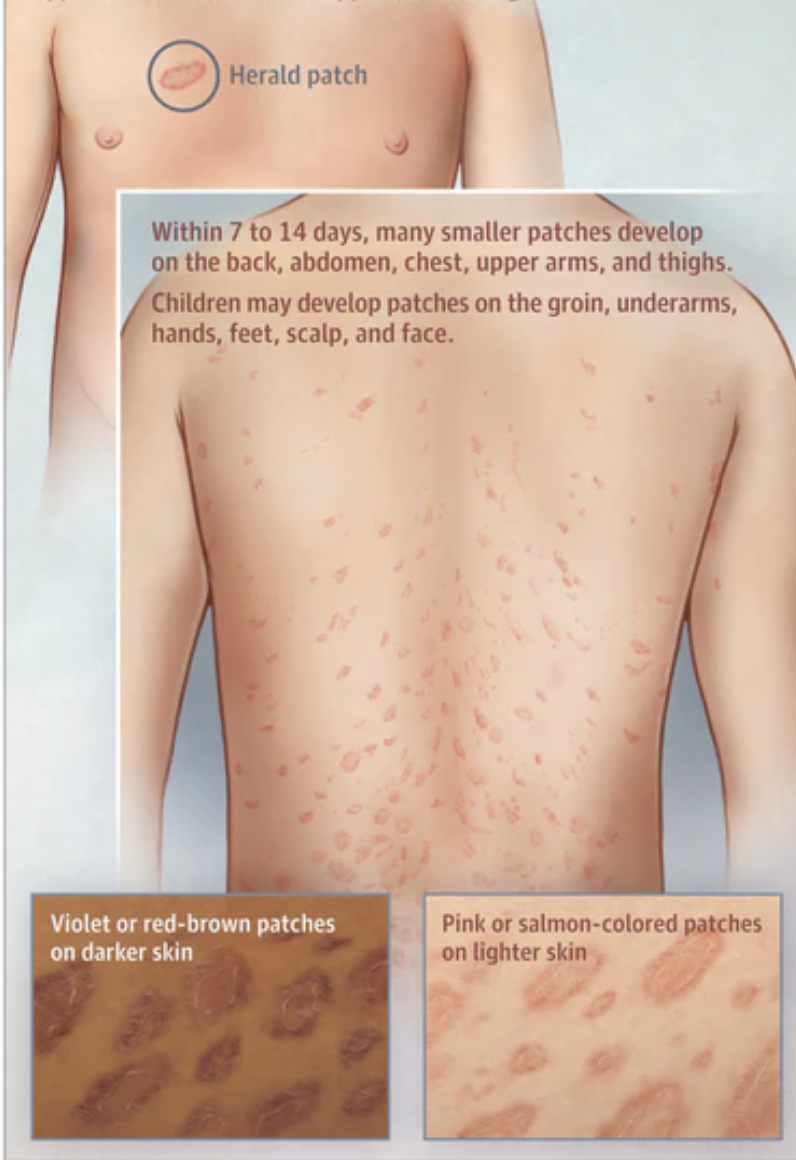
Pityriasis Rosea ON TEST
Pathophysiology: likely viral (HHV-6/7) association.
H&P: Herald patch (solitary salmon colored, red or brown macule) followed by CHRISTMAS-TREE trunk distribution of oval scaly plaques. pruritis common but mild. usually confined to trunk and proximal extremities.
Pityriasis Rosea TX
no management needed for most.
supportive: emollients, topical steroids, oral antihistamines, oatmeal baths for pruritus; resolves in week-months.
Pityriasis Rosea
Psoriasis ON TEST
autoimmune related
chronic management
pathophysiiology: keratinocyte hyperproliferation. this results in greater epidermal thickness and accerlaerated episdermis turnover.
H&P: well-demarcated erythematous plaques w/ silvery scale; nail changes; possible arthritis. plaques most common on EXTENSOR surfaces of elbows, knees,scalp,nape of the neck, gluteal cleft.
Psoriasis common signs ON TEST
Auspitz sign- bleeding w/removal of plaque or scales.
Koebners phenomenon-new lesions at the site of trauma
Nail involvement- nail pitting; yellow-brown discoloration under the nail (oil spot) is pathognomonic.
Psoriasis TX ON TEST
mild moderate:
limited disease: topical corticosteroids, emollients, maintain proper skin hydrate to help prevent irritation
Alternative topical agents: vitamin D analogs, retinoids/vitamin A analogs
Topical calcineurin inhibitors (tacrolimus, pimecrolimus: use for involvement of face, genitals, delicate areas.
Moderate-severe:
Phototherapy: narrow-band UVB
Severe:
Systemic tx: cyclosporine, oral retinoids (acitretin), biologic agents (tnf-inhibitors). inhibitors of the IL-17 pathways and IL-23. methotrexate.

Psoriasis ON TEST
Seborrheic dermatitis
Pathophysiology: malassezia species, sebum, and host response
H&P: erythematous, greasy scales in seborrheic areas.
Seborrheic dermatitis TX
antifungal shampoos/creams, topical steroids for flares, ultraviolet radiation, ketoconazole and selenium shampoo
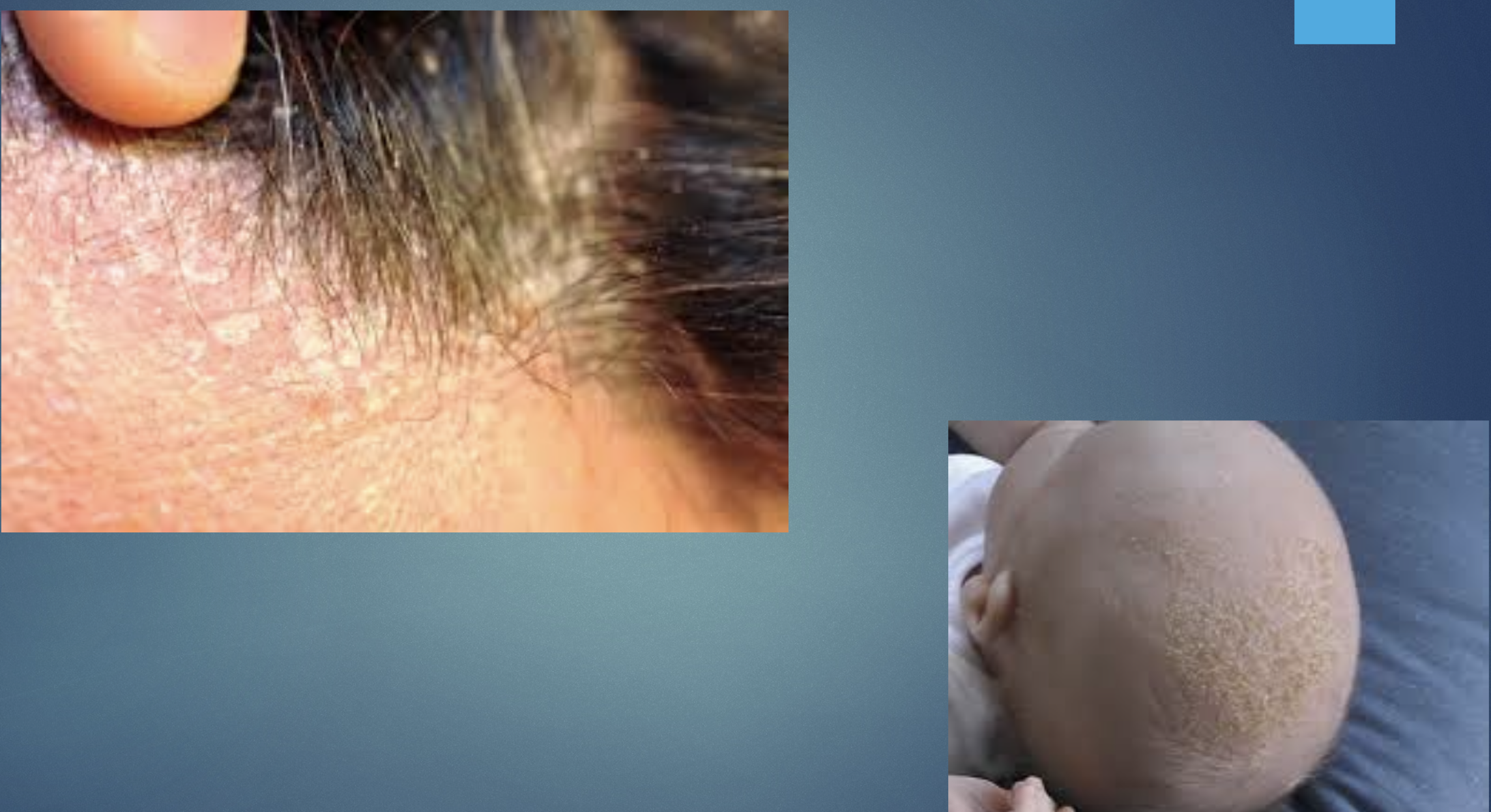
Seborrheic dermatitis
Erysipelas
Pathophysiology: superficial dermal lympathic infection
group A strep
H&P: well-demaracted, raised erythematous plaque w systemic symptoms.
Erysipelas TX
Penicillin or appropriate antibiotics for streptococcal coverage

Erysipelas
Cellulitis
Infection of the skin happens w a breach in integrity of the skin.
Lower extremities are the most common site
beta hemolytic streptococci
staph aureus

Cellulitis
Impetigo ON EXAM
Superficial epidermal infection w HONEY-COLORED CRUSTS.
H&P: vesicles/pustules that rupture forming crusts; pruritic.
Impetigo TX ON EXAM
Topical mupirocin for limited disease; oral antibiotics for widespread disease.

Impetigo ON EXAM
Candidiasis
Anywhere you have body folds
Pathophysiology: overgrowth of candida species
H&P: erythematous, moist patches w satellite pustules.
Candidiasis TX
Topical or oral azoles; address predisposing factors.

Candidiasis
Fungal-Dermatophyte infections
epidemiology: tinea corporis,pedis,capitis
Pathophysiology: keratinophilic fungi invade stratum corneum
H&P: annular, scaly plaques w central clearing (ringworm); pruritus.
Fungal-Dermatophyte infections TX
topical or oral antifungals depending on site and severity
Tinea Versicolor
Caught by yeast, found in the upper layer.
Fungal infection of the skin with overgrowth of Malassezia yeast
H&P: hyper or hypopigmented well demarcated round or oval macule or patch that can have erythema and a fine scale. most common on upper trunk. involved skin fails to tan w sun exposure.
Tinea Versicolor TX
topical antifungals, ketaconazole, selenium sulfide lotion
Lice
pathophysiology: pediculus species infestation of hair/scalp or body.
H&P: Pruritus, nits on hair shafts.
Lice TX
topical permethrin or oral ivermectin;treat contacts and fomites.
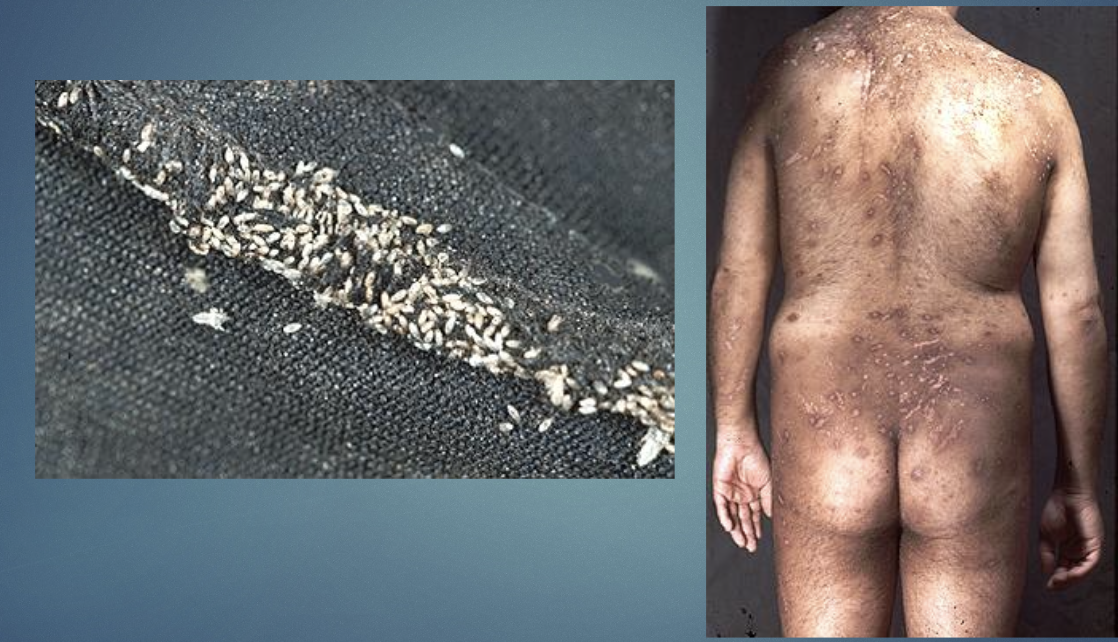
Pediculosis Corporis
Pediculosis pubis
crabs result from sexual contact
itching in pubic area but also in axillae
Pediculosis pubis tx
permethrin 1% cream rinse or pyrethrins w piperonyl butoxide applied to the affected areas and washed off after 10mins
Scabies
Burrows in the skin
CONTAGIOUS;CLOSE CONTACT SPREAD
prominent feature is itching
H&P: intense noctural pruritus, linear burrows in webs of fingers, wrists.
Scabies tx
topical permethrin or oval ivermectin;treat household contacts

Scabies
Condyloma Acuminatum (genital warts)
STI due to HPV
H&P: flesh =-colored verrucous papules in anogenital region
Condyloma Acuminatum (genital warts) TX
topical agents (imiquimod,podophyllotoxin),cryotherapy, surgical removal.

Condyloma Acuminatum (genital warts)
Viral Exanthems
viral mediated skin eruptions
H&P: diffuse maculopapular rashes often w systemic symptoms.
Viral Exanthems TX
Supportive care
Erythema Infectiosum
parvovirus B19
viral infection causing immune mediated rash
Erythema Infectiosum TX
supportive, parvovirus IgM if needed
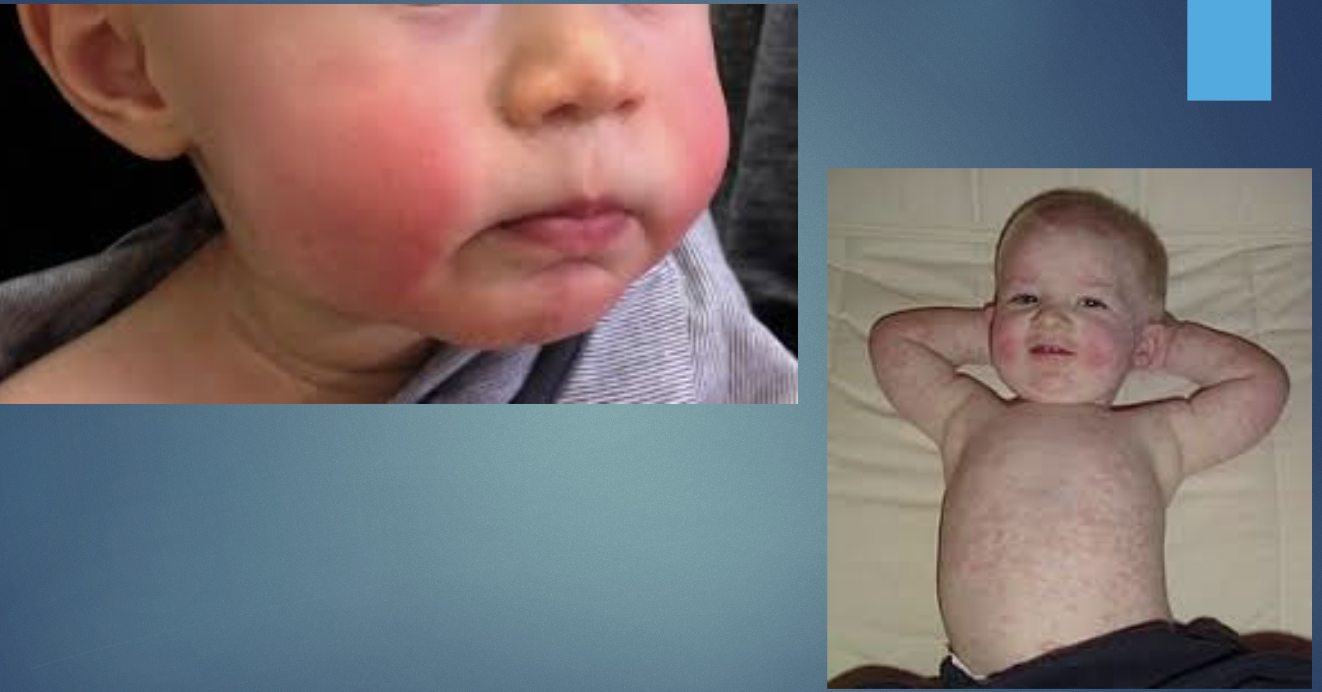
Erythema Infectiosum
Hand foot and mouth disease
primarily fecal oral
viral infection causing mucocutaneous lesions. enterovirus (coxsackie,type A16)
H&P: mild fever, uri symptoms, malaise, anorexia, decreased appetite
Hand foot and mouth disease TX
Supportive, antipyretics;hydration and pain control
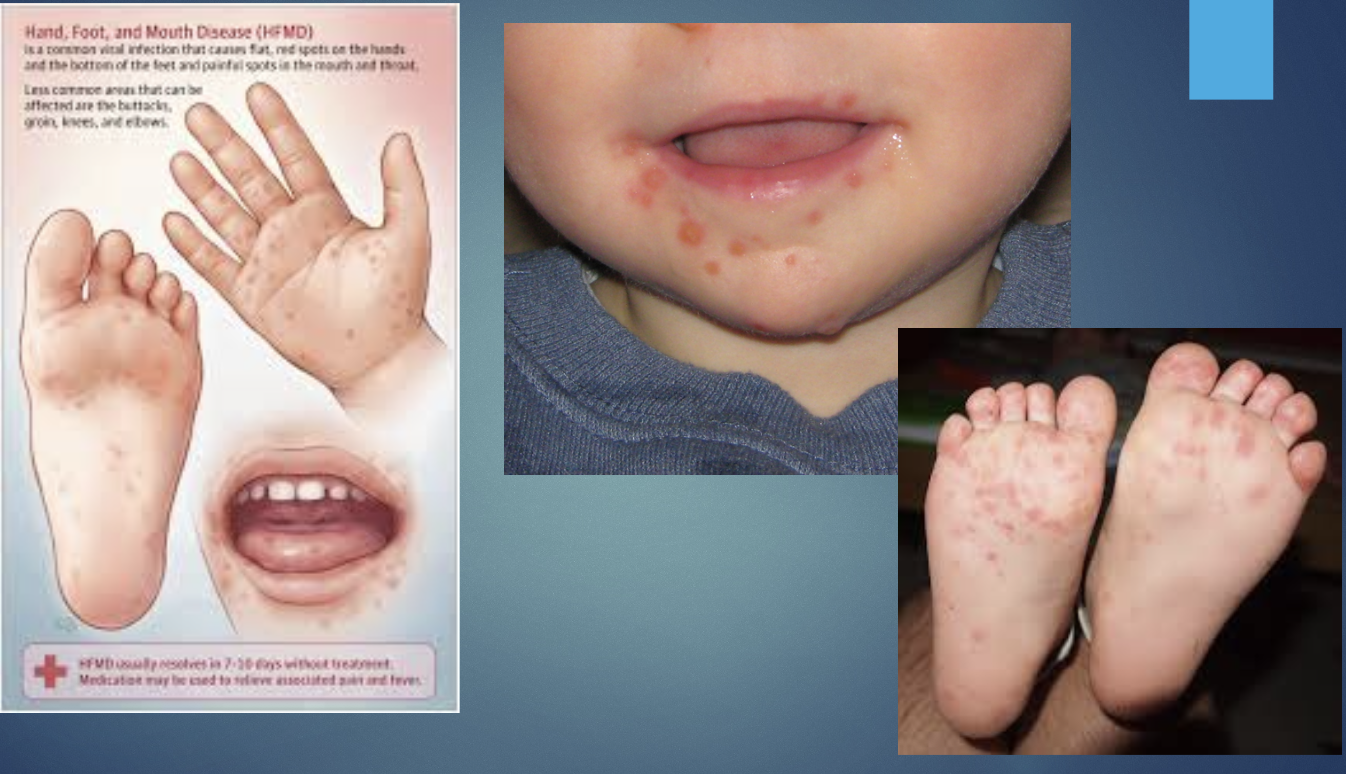
Hand foot and mouth disease
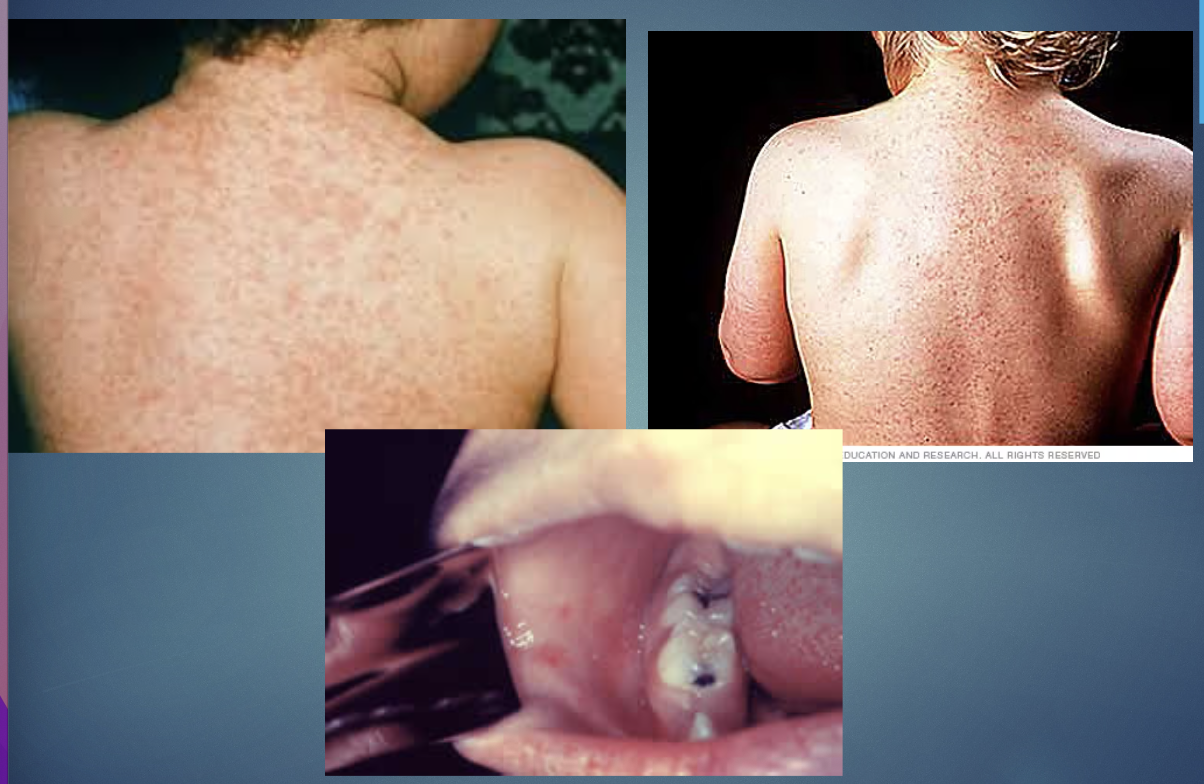
Measles
part of the paramyxovirus family
transmission by respiratory droplets person to person, airborne.
H&P: fever, cough,coryza, conjunctivitis, Koplik spot, maculopapular rash
Measles 3C’s
Cough, Kariza, conjunctivitis
Measles TX
supportive; Vitamin A in severe pediatric cases; isolation.
Measles