CBCT and other imaging modalities
1/59
Earn XP
Description and Tags
lectures given 3/26/2026
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
cone beam CT
recent technology developed for angiography in 1982 and was subsequently applied to maxillofacial surgery
heralded a shift from a 2D to a volumetric approach to maxillofacial imaging
what does CBCT have that radiographs do not?
3D ability to view the buccal and lingual
*what is the physics behind a CBCT?
uses a diverget cone-shaped or pyramid shaped source of ionizing radiation and a 2D area detector fixed on a rotating gantry to provide multiple sequential transmission images that are integrated directly, forming volumetric information
detector may be a flat panel or image intensifier
what are the principles of CBCT?
all ct scanners consist of an x ray source and dectector mounted on a rotating gantry
during rotation of the gantry, the receptor detects x rays attenuated by the patient
these recordings consititue raw data that is reconstructed by a computer algorithm to generate cross sectional images whos component picture element (pixel) values correspond to linear attenuation coefficients
ct ca be divided into 2 categories based on acquisition of the x ray beam geometry- fan beam and cone beam
how is a patient positioned in a CBCT?
seated, standing, or supine
head is positioned and stabilized between the x ray generator and detector
how long does a CBCT take?
can be as fast as 5 sec
what are the principle determinants of nominal voxel size in CBCT?
x ray tube focal spot size, x ray geometric configuration, the matrix and pixel size of the solid state detector
what are the limiting factors of CBCT image spatial resolution?
focal spot size and geometric congfiguration of the x ray source
(they both determine the degree of unsharpness)
the smaller the focal spot size is, the _____ the cost of the x ray tube
more
what can minimize geometric unsharpness?
reducing the object to detector distance and increasing the source to object distance
why is the detector position limited in maxillofacial CBCT?
it must be located far enough from the patient’s head so that it can freely rotate around shoulders
*grayscale
the ability of CBCT to display differences in attenuation is related to the ability of the detector to detect subtle contrast differences
this parameter is called the bit depth of the system and determines the number of shades of gray available to display the attenuation
a basic image has a grayscale value that is related to…
the intensity of the photons incident on the detector
reflects tissuses attentuation which is measured by the residual x rays recieved on the detector
t/f we can give pts CBCT just because its fun
false- ALARA, there should be justification of the exposure to the patient
what is CBCT commonly used for?
assessment of pathologic conditions and structural maxillofacial deformity, preoperative assessment of orthodontics, and in the assessment of available bone for implant placement
image artifact
any distortion or error in the image that is unrelated to the subject being studied
what are the different classifications of artifacts?
acquisition, patient related, scanner related, cone beam related
acquisition artifacts
artifacts that arise from limitatins in the physical processes involved in the acquisition of CBCT data
beam hardening
as an x ray beam passes through an object, lower energy photons are absorbed in preference to higher energy photons
results in 2 types of artifacts- distortion of metallic structures as a result of differential absorption (cupping effect), and streaks/dark bands that can appear between 2 dense objects
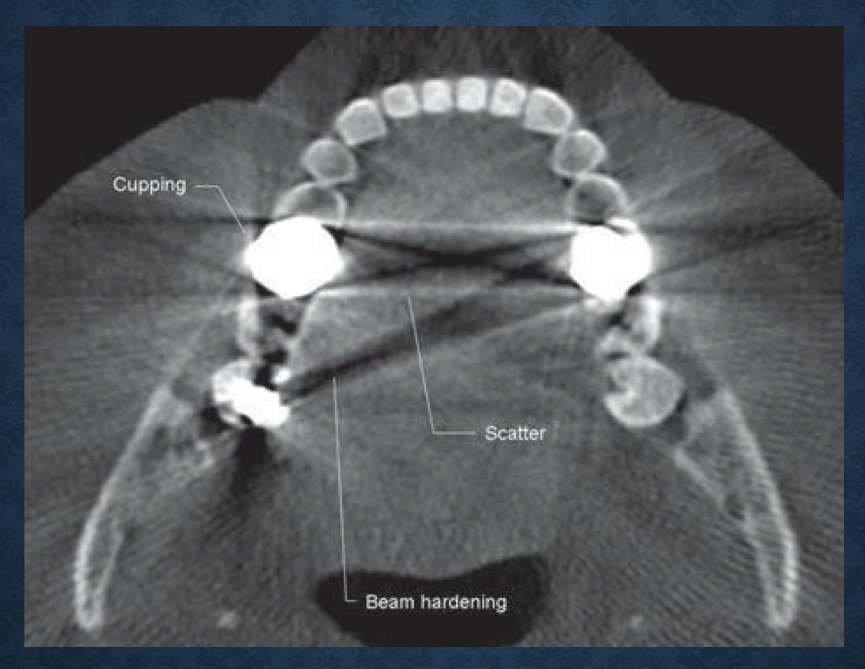
what is this?
axial view demonstrating beam hardening, scatter, and cupping artifacts
aka acquisition artifacts
patient related artifacts
patient motion can cause misregulation of data, which appear as unsharpness in the reconstructed image
this can be minimized by restraining the head and using as short a scan time as possible
it is also important to remove metallic objects like jewlery before scanning because of the beam-hardening artifacts
*scanner related artifacts
circular or ring streaks resulting from imperfections in scanner detection or poor calibration
these problems will result in a consistent repetitive reading at each angular position of the detector, resulting in a circular artifact
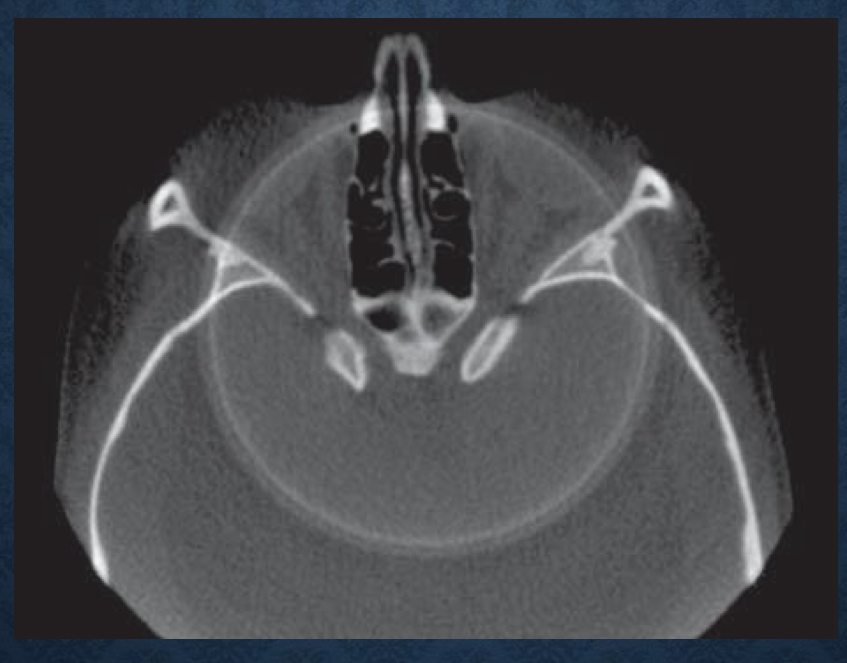
*what is this?
scanner related artifacts- circular rings on axial image indicating imperfections in scanner detection as a result of poor calibration
cone beam related artifacts
the beam projection geometry of CBCT and image reconstruction method produce 3 types of artifacts- partial volume averaging, undersampling, cone beam effect
partial volume averaging
a feature of both conventional fan and CBCT imaging
occurs when the selected voxel size of the scan is larger than the size of the object being imaged
aka the borders are so thin that the voxel size gets both soft tissue and bone which it averages together
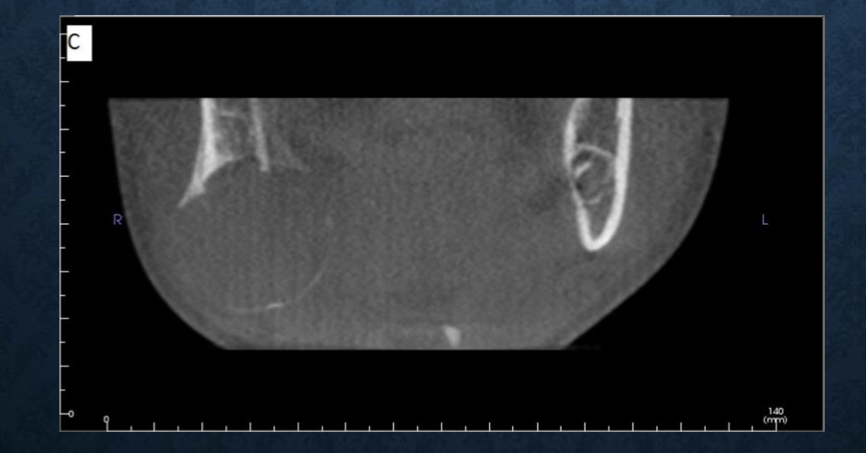
*what is this?
partial volume averaging
cone beam effect
seen in the peripheral portions of the scan volume
because of the divergence of the x ray beam as it rotates around the patient in a horizontal plane, structures at the top or bottom of the image field will only be exposed when the x ray source is on the opposite side of the patient
this results in image distortion, streaking artifacts, and greater peripheral noise
this effect is minimized by manufactures incorporating various forms of cone beam reconstruction
clinically it can be reduced by positioning the region of interest in the horizontal plane of the x ray beam
what are the uses of a CBCT in oral surgery/implants?
wisdom tooth (teeth) extraction, cyst (non / odontogenic), tumor (non / odontogenic), sinus lift surgery, bone graft surgery, orthognathic surgery (single jaw or double jaw), dento-alveolar trauma/fracture, zygomatic or orbital fracture, complex craniofacial fractures, space infections, tooth dislodged into the maxillary sinus/floor of the mouth, dystrophic calcifications in the floor of the mouth/salivary glands/lymph nodes/ducts, mandibular fracture
what are the uses of a CBCT in ortho?
pre treatment eval of pts with a developmental syndrom (cleft palate/turners/hemifacial microsomia), impacted canine evaluation, treatment progress evaluation, post treatment follow up
what are the uses of a CBCT in implants?
preoperative evaluation of the potential implant site, sinus augmentation (lift, uni or bilateral), block or particulate bone grafting, ramus of symphysis grafting, assessment of impacted teeth in the field of interest, evaluation of prior traumatic injury, postoperative evaluation of symptomatic implants (immediate/follow up), implant retrieval surgery
what are the uses of a CBCT in oral medicine?
osteoradionecrosis evaluation, temporomandibular disease (uni or bilateral), BRONJ, osteochemonecrosis, osteonecrosis, autoimmune disorders, sjogren’s, mickulizs’s, pre-malignant lesions
what are the uses of a CBCT in peds?
syndromic patients (pierre robin, ect), craniofacial anomalies, supernumerary teeth, anodontia, oligodontia
what are the uses of a CBCT in perio?
implant treatment planning, augmentation procedures (bone graft/sinus lift), postoperative evaluation of symptomatic implant (immediate/follow up), implant retrieval surgery, complications including nerve damage
*what are the strengths of CBCT?
size and cost, high speed scanning, low patient radiation dose, interactive analysis
*what are the limitations of CBCT?
image noise, poor soft tissue contrast
what are the 3 basic views in a CBCT?
axial- superior to inferior
sagittal- right to left
coronal- anterior to posterior
what is the history of CT scans?
introduced in 70’s- hounsfield and cormack
x ray tube emits fan shaped beam
early scanners would scan axial slices incrementally
in 1989 scanners scan in a helical fashion
current MDCT scanners have how many rows of detectors?
64 to 128
what defines the field of view (FOV)?
scout/localizer view
usually lateral projection of the head, used to estimate tube current (mA) based on patient size and anatomy
maxillofacial and mandibular ct protocols for FOV
7-18 cm
from cranial base to past mandibular inferior border
can be reconstructed into an image data set after acquisition
what are the exposure settings for ct exams on adult and children?
adult- 120 kVp
peds- 80-120 kVp
*as kVp increases…
contrast decreases
*as mA increases…
exposure time decreases, radiation dose increases, and noise decreases
t/f most ct units offer automatic exposure control, and mA is usually automatically adjusted based on patient size and body part being examined
true
*how is CBCT different conventional medical CT? (characteristics of conventional)
fan beam, multiple revolutions, unlimited scan volume, little scatter, soft tissue detail, higher costs, higher dose
*how is CBCT different conventional medical CT? (characteristics of cone beam)
cone beam, one revolution, limited scan volume, lots of scatter, hard tissues only, lower costs, lower dose
history of MRI
described in 1973, used clinically in 1980
*how does magnetic resonance imaging (MRI) work?
patient is placed in a strong magnetic field
magnetic dipole of specific atoms (particularly hydrogen) aligns with magnetic field
*an RF pulse (non-ionizing electromagnetic radiation) is directd at the patient, which causes some of the hydrogen nuclei to absorb the energy (resonate)
the RF pulse is turned off, the stored energy in the hydrogen atoms is released, which is detected as a signal in a receiver coil in the scanner
tldr characteristics of MRI
noninvasive, nonionizing radiation, excellent soft tissue resolution in any imaging plane, increased cost, increased scan time, metals cause artifacts, ferromagnetic objects may cause injury
what are the advantages of MRI?
non invasive, non ionizing radiaiton, high quality images of soft tissue resolution
what are the disadvantages of MRI?
high cost, long scan times, metals can distort image or move which can injure the patient
nuclear imaging
uses radioactive atoms or molecules that emit gamma rays, can be attached to carrier molecules depending on which organ is being imaged
patient is the source of radiation
allows measurement of tissue function in vivo, provide early marker of disease through detection of biochemical change
detection and monitoring of metastatic disease, bone tumors, skeletal growth disturbances, and infection
what are the applications of FDG-PET/CT imaging?
detect and monitor- metastatic bone disease, primary and recurrent malignancies, osteomyelitis, asymmetric growth, abnormal metabolic bone activity
ultrasonography
sound waves
1-20 MHz (greater than audible range), real time imaging
transducer- converts electrical energy into sonic energy
tissues of different acoustic impedance → reflect (echo) toward transducer → signal is amplified, processed, and displayed as a digital image
increased frequency of the sound wave increases image resolution and decreases penetration through soft tissue
what are the applications of ultrasonography?
evaluation of neoplasms of thyroid, parathyroid, salivary glands, lymph nodes
salivary stones
sjogren’s syndrome
vessels of neck
guide for fine needle aspiration in the neck
doppler for blood flow
tldr ct
uses: implant, bony pathology, TMJ, some soft tissue
advantage: resolution, images many structures
tldr CBCT
uses: implant, bony pathology, TMJ
advantage: low radiation, resolution, images many structures
tldr MRI
uses: TMJ, soft tissues, pathology, sinus
advantages: soft tissue visualization, nonionizing radiation
tldr nuclear medicine
uses: detecting/staging tumors, metastases, infections
advantages: detects functional changes, not macroscopic
tldr ultrasonography
uses: superficial neoplasms, salivary stones, arterial plaques
advantages: no radiation, quick