Lecture 11: Non-Neoplastic Bone Diseases
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
Achondroplasia
Autosomal Dominant (AD)- Gain-of-function mutation in FGFR3 gene
↑ FGF effect → ↓↓ enchondral growth → long bones are short
Intramembranous bone formation is not affected – flat bones not affected
Disproportionate short-stature dwarf
Short arms & legs but Trunk of relatively normal length
Normal size/relatively enlarged head with bulging forehead
Depression of the root of the nose/flat nasal bridge
Mildly delayed motor milestones
High risk for osteoarthritis
Thanatophoric dysplasia
Lethal form of dwarfism- Incompatible with life beyond infancy
Gain-in-function mutation in FGFR3 gene
Micromelic shortening of limbs- extremely short limbs
Frontal bossing
Relative macrocephaly
Small chest (pulm. hypoplasia)→ respiratory insufficiency → death
Bell shaped abdomen
Usually die at birth or soon after birth
Osteogenesis imperfecta Type-1
Mutations in alpha1 & alpha 2 chains of type-I collagen (COL1A1 & COL1A2)
Decreased synthesis of type-I collagen (osteopenia)
AD: Qualitatively normal type-1 collagen in ↓ amounts → mild skeletal defects
↓ bone mass → extreme bone fragility
Frequent fractures (often with little or no trauma) since birth & bone deformities
Blue sclera due to visualization of underlying choroid vessels through thinned sclera → Vision problems
Hearing loss; conductive and/or sensorineural
Small misshapen blue yellow, opalescent teeth due to deficiency in dent
Osteopetrosis
AKA Marble bone disease, Albers-Schonberg disease
Hereditary
Impaired osteoclasts b/c impaired acidification of resorption pits → ↓ osteoclast bone resorption → diffuse symmetric skeletal sclerosis → stone-like bones/ abnormally radio-dense
↑ abnormal bone mass, brittle bones which break like chalk
Sclerotic/marble like thick, heavy but brittle bones → Fracture easily
Ends of bones are bulbous → Ehrlenmeyer flask deformity
Bones lack medullary canal (Primary spongiosa persists) → ↓ hematopoiesis → Leukopenia, anemia, thrombocytopenia (pancytopenia)
Extensive extramedullary hematopoiesis → hepatosplenomegaly
Small neural foramina → compression of nerves → blindness, deafness, facial paralysis
Roots of teeth are difficult to visualize
Dx: radiographs showing abnormally dense bones/diffuse symmetric sclerosis
Osteoporosis
Decreased bone mass/density
Primary generalized osteoporosis:
Postmenopausal (cancellous compartment of vertebral bodies)
Senile osteoporosis (cortex is thinned)
Senile osteoporosis
Osteoclasts are working at their normal rate, but osteoblasts are not forming enough bone → ↓ bone mass
Age-related changes in bone
Postmenopausal Osteoporosis
↑ bone loss due to ↓ estrogen
↓ in Estrogen → ↑ tumor necrosis factor (TNF), interlukin-1, & interlukin-6 release from monocytes → ↑ levels of RANK-L & RANK & ↓OPG → ↑ osteoclast recruitment & activity
↓ estrogen ↑ bone resorption & formation but more resorption
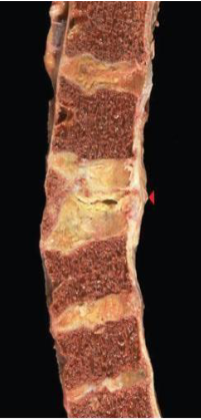
Osteoporosis Morphology
Normally mineralized bone that is ↓ in quantity
Entire skeleton is affected
Postmenopausal osteoporosis:
Vertebrae more affected because have greater surface area
Micro-fractures lead to vertebral collapse
Senile osteoporosis: Cortex is thinned by sub-periosteal resorption

Osteoporotic vertebral body (right)
Advanced osteoporosis
Diminished quantity of normal bone
Cortical bone + Trabecular bone thinned
Osteoporosis
Paget’s disease of bone (Osteitis Deformans)
Chronic disorder of increased , but disordered bone mass due to disordered remodeling (rapid breakdown & faulty rebuilding) due to osteoclast dysfunction
Elderly white
SQSTM1 mutations → ↑ NF-kb activity → ↑ osteoclast activity
Infection of osteoclast precursors with viruses
Paramyxovirus such as Measles, RSV
Diseased osteoclasts are hyper-responsive to: Vitamin D & IL-6 → ↑ osteoclast recruitment & bone resorption
Paget’s disease of bone Stages
Osteolytic: ↑ osteoclast activity – abnormally large osteoclasts with many nuclei
Numerous resorption pits
Mixed osteoblastic-osteoclastic stage: Prominent osteoblasts → new bone woven or lamellar which is eventually remodeled to lamellar bone
Osteosclerotic stage: Osteoblastic & osteoclastic activity cease → thickened trabeculae which lack structural stability → fractures easily
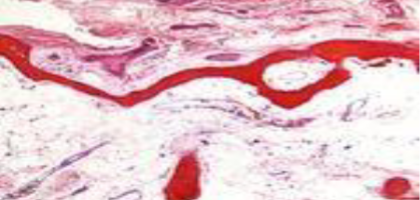
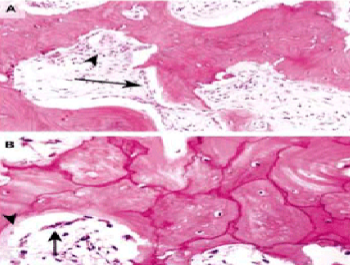
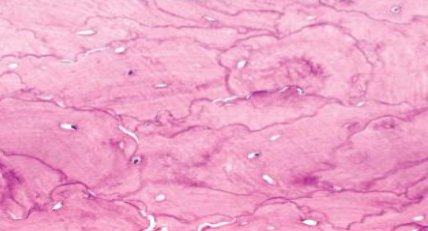
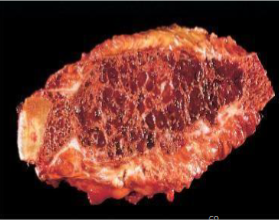
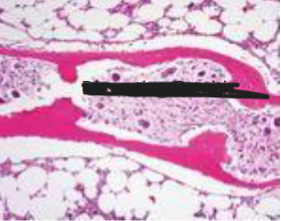
Paget’s disease of bone Morphology
Mosaic pattern of dense lamellar bone in sclerotic phase
Prominent irregular cement lines & haphazard orientation of lamellar bone
Sclerotic phase: bones are thicker than normal but structurally unstable & fracture easily

Paget’s disease of bone
Paget’s disease of bone
Paget’s disease of bone
Paget’s disease of bone Clinical
Monostotic
Mostly Polyostotic
Axial skeleton or proximal femur
Not a serious life-threatening condition & progresses over many years
Onset late adulthood (>50) & more common with increasing age
Asymptomatic + X-ray as thick sclerotic coarse bone
Symptoms are usually mild:
Bone pain at site of affected bone due to micro-fracture or overgrowth causing nerve impingement → hearing loss, numbness
Enlargement of craniofacial skeleton (lion face), Bowing of leg bones, Painful jaw enlargement with separation of teeth
Anterior bowing of the femur → distorts femoral head → secondary osteoarthritis

Paget’s disease of bone
Paget’s disease of bone Complications
Severe secondary osteoarthritis due to abnormal joint alignment
Chalk-stick bone fractures in long bones due to weaker bones of lower extremity
Compression fractures of spine → kyphoscoliosis
Hypervascularity of pagetic bones makes overlying skin warm
↑ blood flow due to ↑ bone remodeling acts as arteriovenous shunt → high- output congestive heart failure → left ventricular hypertrophy
Tumors & tumor-like conditions develop in pagetic bone
Benign: giant cell tumor, extraosseous masses of hematopoiesis
Malignant: osteosarcoma
elevated serum alkaline phosphatase

Paget’s disease of bone
Paget’s disease of bone Xrays
“Burnt out stage” - Pagetic bone typically are enlarged bone with thick, coarsened trabeculae – densely sclerotic bone
Mixed phase – osteosclerotic with osteolytic areas
Hyperparathyroidism
↑ production of parathyroid hormone (PTH) → ↑ osteoclast activity → ↑ bone resorption → osteopenia
Osteoporosis: generalized
More severe in phalanges, vertebrae & proximal femur
Dissecting osteitis: osteoclasts tunneling & dissecting through trabeculae (railroad tracks) → ↓ bone density → fracture
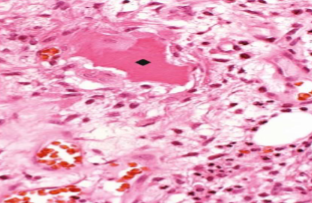
Brown tumor: mass of reactive tissue not a true tumor
Microfractures with secondary hemorrhage, influx of macrophages, ingrowth of fibrous tissue
Brown color is due to vascularity, hemorrhage, hemosiderin deposition
Radiolucent
Brown tumor can undergo cystic degeneration → osteitis-fibrosa-cystica
Brown tumor

Healing of fracture
Inflammatory (hours to 1 week): Hematoma forms immediately after fracture & fills the fracture gap. → inflammatory cells come
Soft callus (2 to 3 weeks): uncalcified, formed by fibroblasts & chondroblasts
Bony callus formation (3 to 12 weeks): formed by osteoblasts (woven bone)
Remodeling (months to years): osteoclasts remodel new bone
Lamellar bone laid down which increases the bone strength
Reduces the size of the callus
Medullary cavity formed
If nonunion fracture persists
malformed callus → cystic degeneration → pseudoarthrosis (false joint)
Osteonecrosis (avascular/aseptic necrosis)
Localized area of infarction/death of bone & marrow cells
Medullary cavity (most common) or in subchondral location
Mostly due to ischemia:
Vascular injury – trauma causing fracture
Corticosteroids
Systemic disease – hemoglobinopathies such as sickle cell disease/crisis; hyper-lipedemia
Radiation
Caisson disease – in divers - nitrogen bubbles can embolize to skeletal system causing bone ischemia
Pregnancy, Infection, Alcohol abuse
Osteonecroses of the jaw
Complication of long-term bisphosphonate therapy & more likely to occur if patient also on chemotherapy
Osteochondroses
Self-limiting, non-inflammatory, non-infectious developmental disorders in growing children & adolescents who are often athletes & is mostly related to repetitive injury
Caused by ischemic necrosis
Near joints/epiphyses
M > F
Pain, swelling & reduced function
Legg-Calve-Perthes disease: osteonecrosis of femoral head in children → osteoarthritis
Osgood-Schlatter disease: osteonecrosis of tibial epiphysis at knee
Osteomyelitis
Inflammation of bone & marrow
Secondary to infection:
Pyogenic bacteria & mycobacteria
Coccidiodomycosis (fungus)
Viruses & parasites
Hematogenous: metaphysis of long
Minor occult injury to skin, GIT
Involve vertebrae in adults & long bones in children
Extension from contiguous site:
sinus infection → orbital bones, cranium
Dental pathology/periapical abscess or procedure → maxilla/mandible
Infection of feet in diabetics
Direct implantation: After traumatic injury or orthopedic procedures
Staph aureus
Osteomyelitis Morphology
Acute phase:
Neutrophilic inflammatory reaction
Necrosis of bone & marrow → subperiosteal abscess
Dead bone is known as sequestrum
Rupture of periosteum → soft tissue abscess → draining sinus
In infants epiphysial infection → spread through articular surface → septic arthritis → destruction of articular cartilage and permanent disability
Chronic phase (after 1 week): cytokines from chronic inflammatory cells stimulate
Osteoclastic bone resorption
Reactive bone formation at the periphery – involucrum (sleeve of living tissue around dead infected bone)
Osteomyelitis
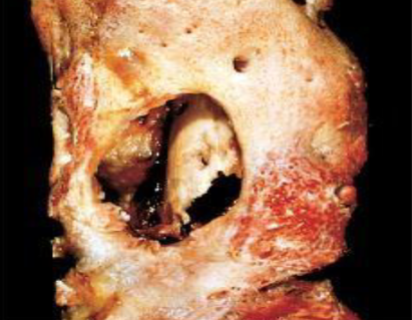
Osteomyelitis