OCR A Level Bio. 3.1.2 Transport in Animals
1/99
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
100 Terms
what organisms need transport systems?
complex multicellular organisms
why would an organism need a transport system? (x3 factors)
• size - large - have lots of cells far from the surface so diffusion pathway is increased.
• SA:V - small - have lots of cells in body compared to SA so diffusion distance increases & diffusion rate wouold be to slow for survival w/o t.s
• metabolic rate - high - need rapid supply of O2 & glucose to have energy & remove waste
why may an organism not need a transport system? (x3 factors)
• size - small - all cells = surrounded by/close to environment they live in
• SA:V - high - increases diffusion rate
• metabolic rate - low - small so not need so much energy
what are the features of an effective transport system?
• transport fluid - carries nutrient, O2 etc.
• pump - creates pressure
• exchange surfaces (high SA:V) (high conc.n grad across) - increase diffusion rate
what are the features of an efficient transport system?
• vessels - carry fluid
• 2 circuits - 1 to pick up O2 & 1 to deliver O2 to tissues
what are the 4 types of circulatory system?
open, closed, single, double
what is an open circulatory system & where does it occur?
• fluid isn't always enclosed in vessels - can flow freely in the body cavity
• in some invertebrates
what is a closed circulatory system & where does it occur?
• fluid is always enclosed in vessels
• in all vertebrates
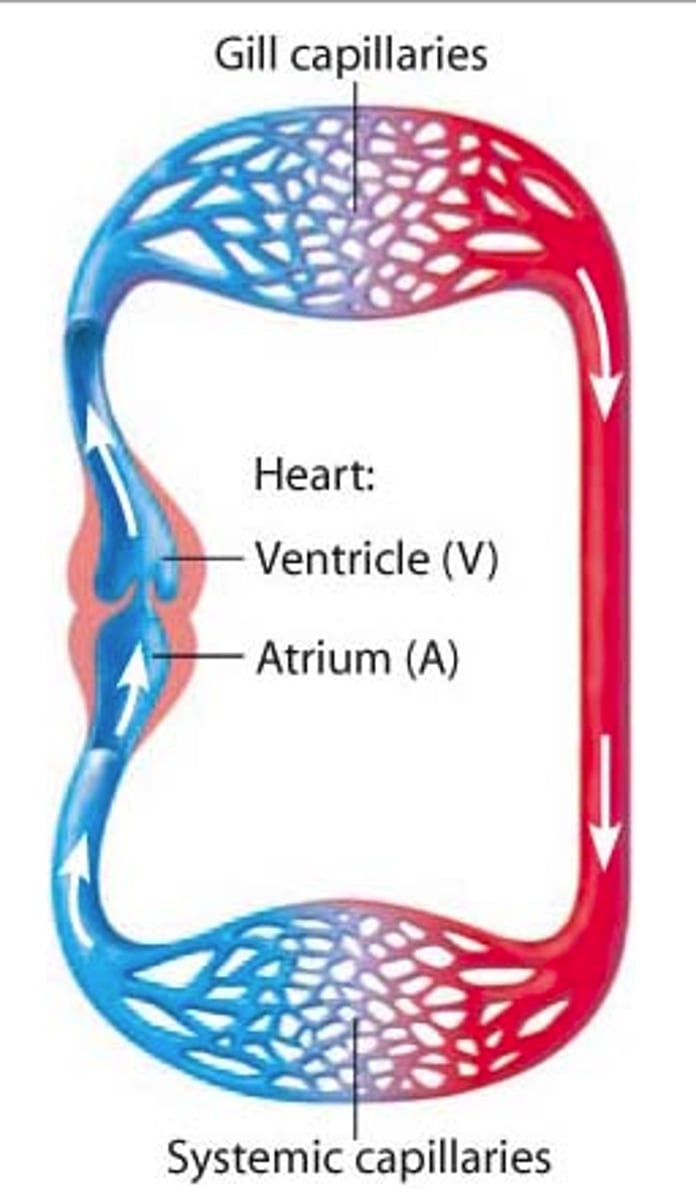
what is a single circulatory system & where does it occur (eg)?
a system where blood passes through the heart once per complete circuit of the body
• eg/ fish (heart -> gills -> body -> heart)
what is a double circulatory system & where does it occur (eg)?
a system where blood passes through the heart twice per complete circuit of the body
• eg/ mammals (heart -> body -> heart -> lungs -> heart)
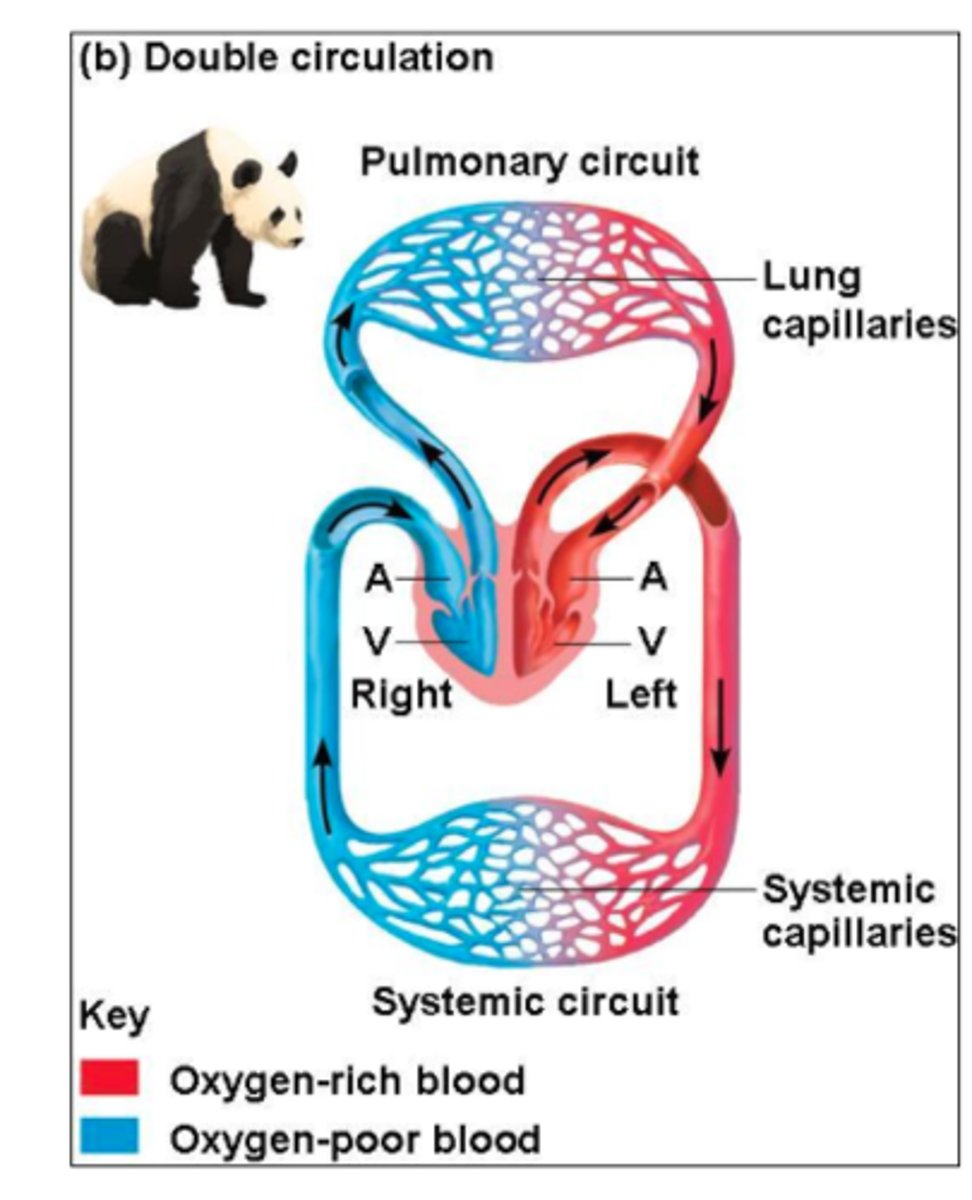
what are the advantages of double circulatory systems? (x4)
• blood flows quicker
• blood transported at higher pressure (in systemic circuit)
• O2 transported quicker
• 2 blood pressures
what are the disadvantages of single circulatory systems? (x3)
• blood pressure drops as passes through capillaries
• blood flow = slow
• rate at which substances are delivered to tissues = limited
what are the disadvantages of open circulatory systems?
• blood pressure is low
• blood flow is low
• circulation may be affected by body movements/ lack of-
what is the circulatory system of fish?
single
what is the circulatory system of mammals
double
what is the circulatory system of insects? (describe)
open -
• has heart-like organ that opens into body cavity
• blood goes into heart through ostia pores
• blood goes to body at head end of heart - opens into b.c. - by peristalsis
what blood vessels make up the human transport system? (flowchart)
[heart ->] arteries -> arterioles -> capillaries -> venules -> veins [-> heart]
what is the function of the arteries?
take blood away from heart
what is the pressure like in arteries?
high
is blood oxygenated/deoxygenated in arteries?
oxygenated except pulmonary artery
describe & explain the interior of an artery (lumen->outside incl. tissues)
• small lumen - maintain high pressure
• folded endothelium - allows expansion & maintain pressure
• thin elastic layer - allows stretch & recoil to maintain pressure
• thick muscle layer - to withstand high pressure
• thick collagen & elastic outer layer - strength to withstand pressure & recoil to maintain pressure
how are arteries near the heart adapted compared to those further from the heart?
they contain lots of elastic tissue to counter blood pulse (fluctuations from each heart beat)
describe arterioles compared to arteries
• arterioles are smaller
• their walls contain less elastic & less muscle
what is the function of the smooth muscle layer in arteriole walls?
control blood flow to tissues - contracts to reduce the arteriole diameter => increases resistance to flow => decreases blood flow => can divert blood to tissues needing more blood
what is the function of the capillaries?
substance exchange
how are capillaries adapted to their function? (x3)
• narrow lumen - decreases diffusion distance => increases diffusion rate (O2)
• walls = 1 cell thick endothelium - reduces diffusion distance
• walls = leaky - allow blood plasma & dissolved substances to leave blood
describe & explain the walls of capillaries
one cell thick - decreases diffusion distance for substance exchange so increases diffusion rate
what is the function of venules?
start taking blood back to heart (from capillaries)
is blood in venules oxygenated/deoxygenated?
deoxygenated
describe the interior of venules?
• thin muscle layer
• thin elastic layer
• thin collagen outer layer
what is the function of veins?
take blood back to the heart from venules
what is the blood pressure in veins like?
low
is the blood in veins oxygenated/deoxygenated?
deoxygenated except for pulmonary vein
describe & explain the interior of veins (inside->outside)
• wide lumen - decrease resistance to blood flow so = low blood pressure
• very little elastic, muscle & collagen - no need for thick walls - no need to stretch & recoil & aren't restricted to reduce blood flow
how are veins adapted to take blood back to the heart at a low pressure? (x2)
• skeletal muscles contract and push blood along veins
• contain valves - blood is forced through valves (muscles push it) and valves close behind blood
what is the function of valves in veins?
prevent backflow of blood
what does blood consist of?
plasma, dissolved substances - O2, CO2, minerals, amino acids, hormones, plasma proteins - & blood cells - red, white, platelets
what is tissue fluid?
the fluid that surrounds cells in tissues
what does tissue fluid consist of?
water, dissolved solutes, small proteins & few white blood cells
why does tissue fluid not contain red blood cells/large proteins/platelets?
they are too big to filter out of the capillaries, into surrounding space to become tissue fluid
how is tissue fluid formed from blood?
• at arterial end of capillaries, blood has higher hydrostatic pressure in cap.s than outside in tissue fluid
• pressure forces fluid out through cap. walls (some components too large to pass through)
• tissue fluid now surrounds cells to exchanges gases & nutrients (O2 & nutrients in, CO2 & waste out)
through what process is blood pushed out of the capillaries
pressure filtration
how does tissue fluid re-enter the blood at the venule end of the capillaries?
• the tissue fluid has a higher water potential than the blood in the capillaries so tissue fluid is forced into the cap.s (high->low)
• the high oncotic pressure of the blood pulls water back into the blood
what happens to the tissue fluid that doesn't re-enter the capillaries?
it is directed into the lymphatic system:
• enters lymph vessels (fluid now = lymph)
• taken back to blood near the heart
• contains valves to prevent backflow
what is the function of the lymphatic system & why is it important?
drain away excess fluid - to prevent excess fluid building up to cause swelling
what does lymph consist of?
water, dissolved solutes, antibodies & white blood cells (produced in lymph nodes)
what valves separate the atria from the ventricles?
atrioventricular valves
what valves separate the ventricles from arteries (pulmonary & aorta)?
semi-lunar valves
what ensure the valves (in the heart) only open in one direction?
cords (valve tendons)
cardiac cycle def.
the sequence of contraction & relaxation of the heart
what are the 3 stages of the cardiac cycle?
• atriole systole
• ventricular systole
• diastole
what happens in the atriole systole stage of the cardiac cycle? (what happens, vol, pressure, valves, where blood goes)
• atria contract
• vol. of atria decrease
• pressure in atria increase
• atrioventricular valves open
• atria -> ventricles
what happens in the ventricular systole stage of the cardiac cycle? (what happens, vol, pressure, valves, where blood goes)
• ventricles contract
• ventricle vol.s decrease
• ventricle pressures increase
• atrioventricular valves shut
• semi-lunar valves open
• ventricles -> arteries
what happens in the diastole stage of the cardiac cycle? (what happens, vol, pressure, valves, where blood goes)
• atria & ventricles relax
• atria & ventricle vol.s increase
• atria pressure increases; ventricle pressure decreases
• semi-lunar valves close
• blood -> atria -> body/lungs
what is measured in cardiac output?
vol. blood leaving heart per min
how do you calculate cardiac output (cm3min-1)?
heart rate (bpm) x stroke volume (cm3)
what is measured in stroke volume?
vol blood leaving heart per heartbeat
what pressure difference causes valves (in heart) to open?
higher pressure behind the valve than in front
what pressure difference causes valves (in heart) to close?
higher pressure in front of valve than behind
myogenic def (hint: cardiac muscle is myogenic)
produce its own nerve signals (doesn't need to receive them from the brain)
what is the role of the sino-atrial node (SAN) in heart action?
it produces & sends out electrical impulses throughout the right atrial wall
what is the importance of non-conducting collagen tissue in heart action?
it stops electrical impulse from reaching the ventricle walls straight away - allows bloodflow into ventricles before they contract
what are the roles of the atrioventricular node in heart action?
pick up & send electrical impulse through bundle of His in septum of heart
what is the role of the Purkyne tissue in heart action?
carries electrical impulse to ventricle walls
outline the process of heart action (x7 steps)
1) SAN sends impuls throughout atria walls
2) impulse stopped temporarily, from reaching ventricle walls, by non-conducting collagen tissue
3) AVN picks up impulse
4) AVN sends impulse through heart septum to Bundle of His
5) Bundle of His sends impulse to Purkyne tissue
6) Purkyne tissue sends impulse to ventricle walls
7) ventricles contract simultaneously
what is an electrocardiograph?
the machine used to measure the heart's electrical activity/voltage/potential difference
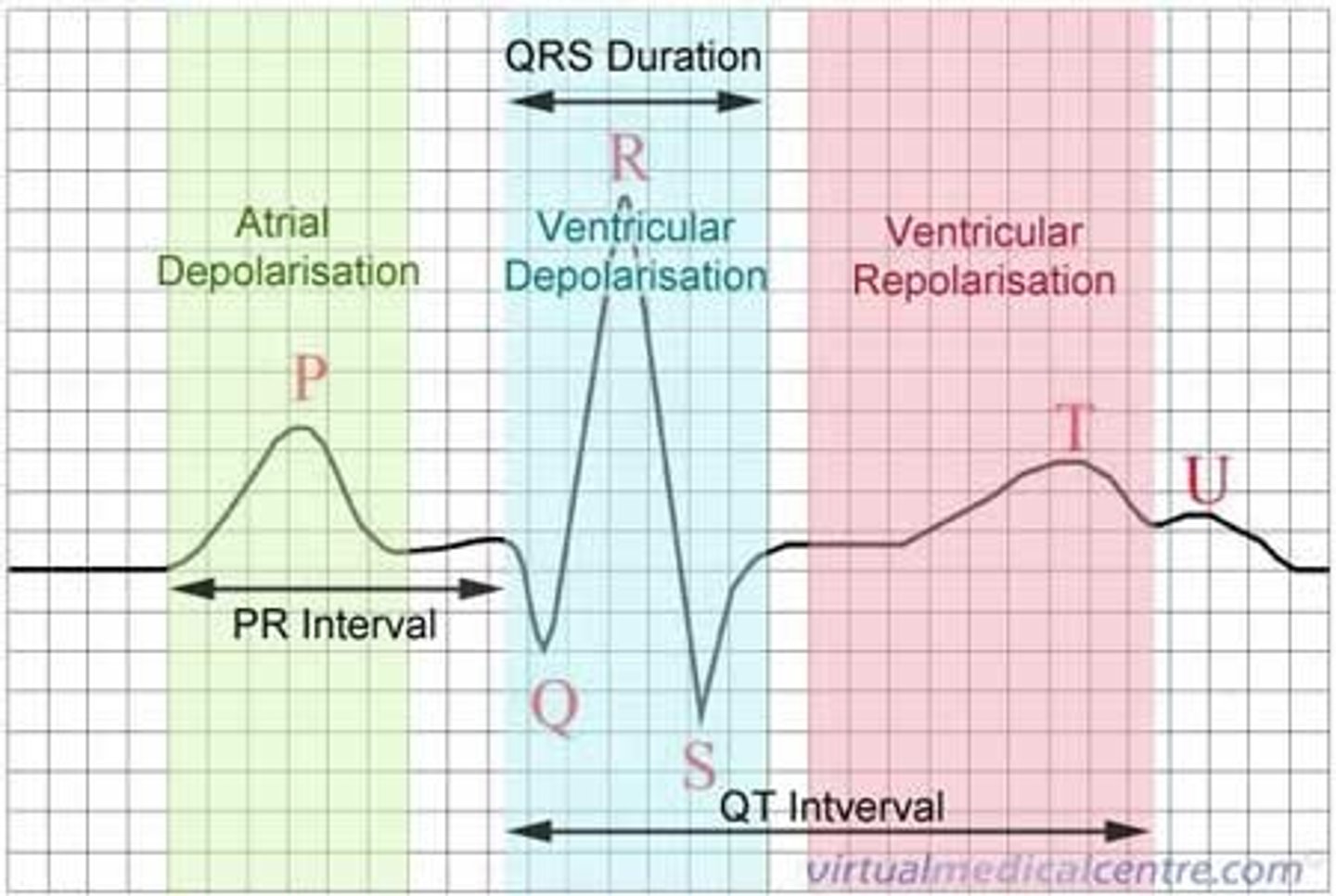
what is an electrocardiogram (ECG)?
the graph that shows the heart's electrical activity/voltage/potential difference
what is the heart's electrical activity/voltage/potential difference measured in?
millivolts
heart rate (bpm) equation
60/time taken for 1 heartbeat (secs)
what happens when the heart contracts (in relation to charge)?
depolarises - loses charge
what happens when the heart relaxes (in relation to charge)?
repolarises - recharges/gains charge
what does P represent on an ECG?
atria contract (depolarise)

what does the QRS complex represent on an ECG?
ventricles contract (depolarise)
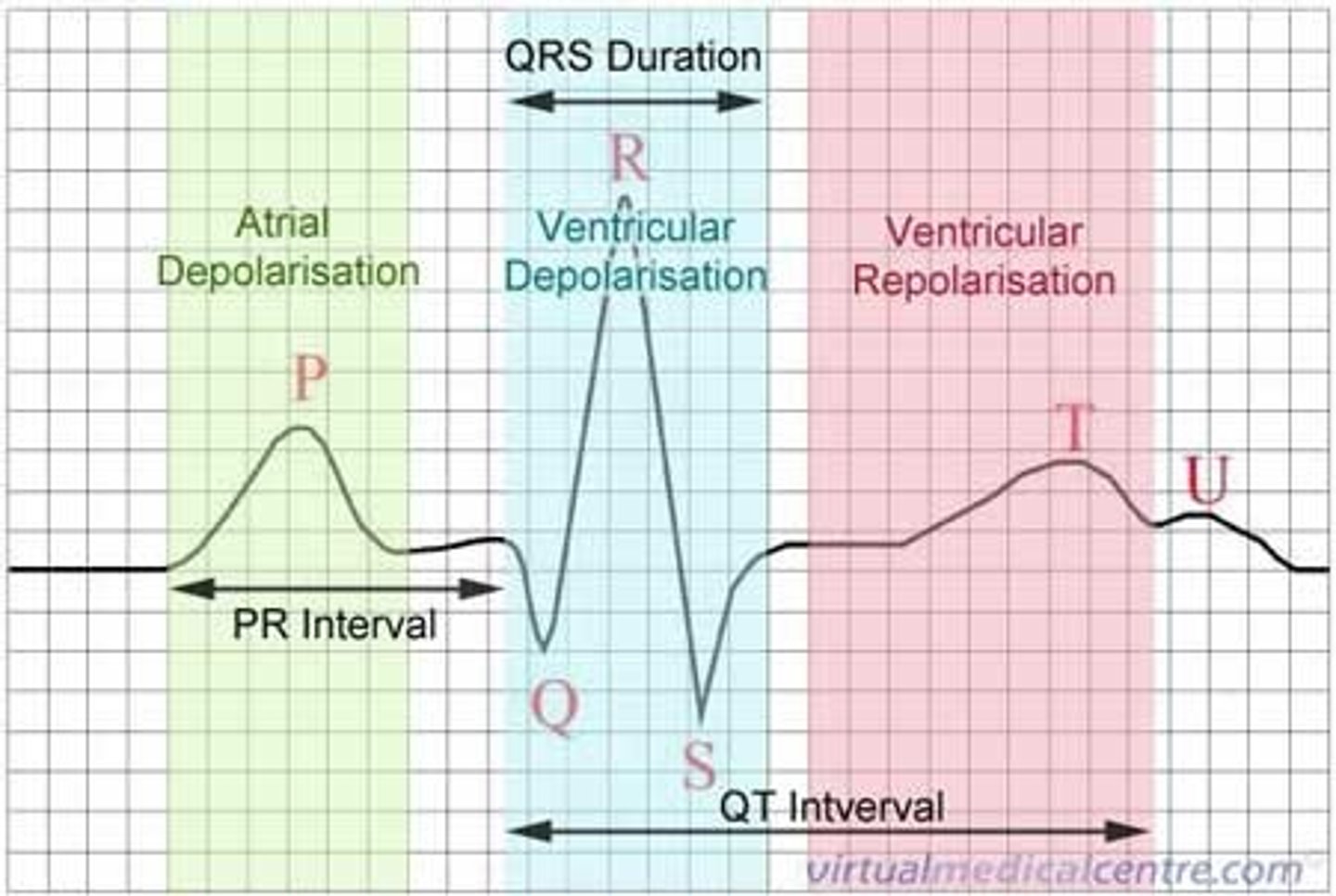
what does T represent on an ECG?
ventricles relax (repolarise)
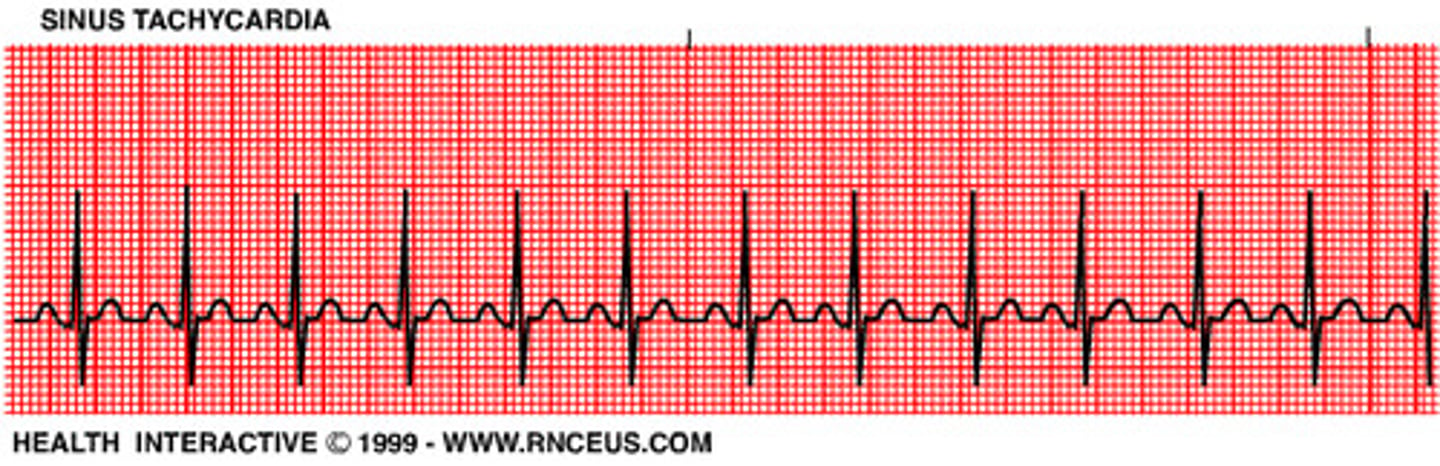
what is tachycardia? what would it look like on an ECG?
abnormally fast heart rate (~120+bpm at rest)
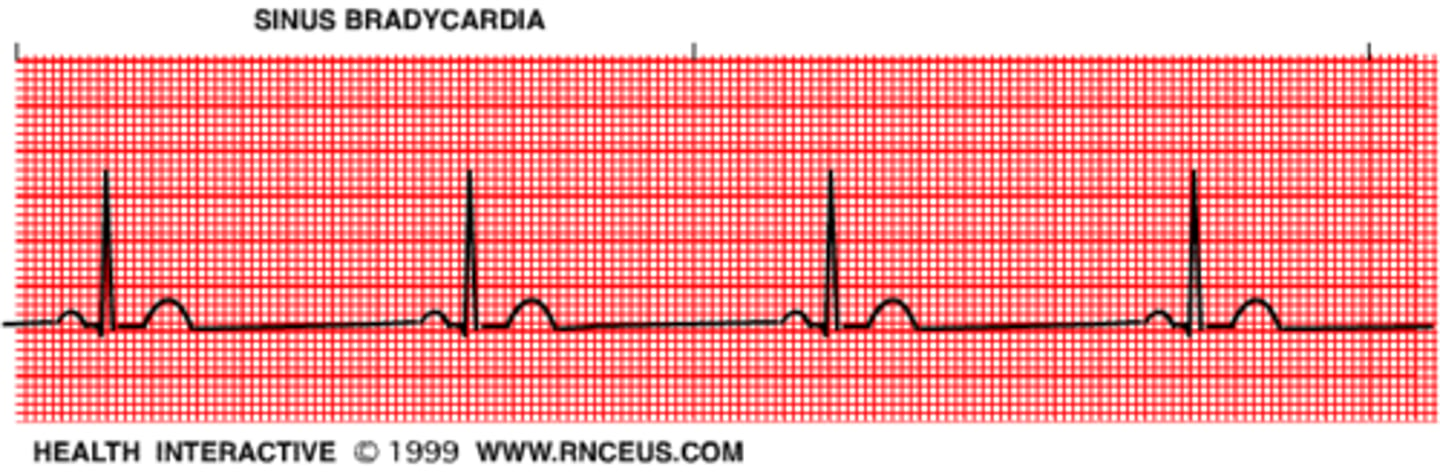
what is bradycardia? what would it look like on an ECG?
abnormally slow heart rate (~50-bpm at rest)
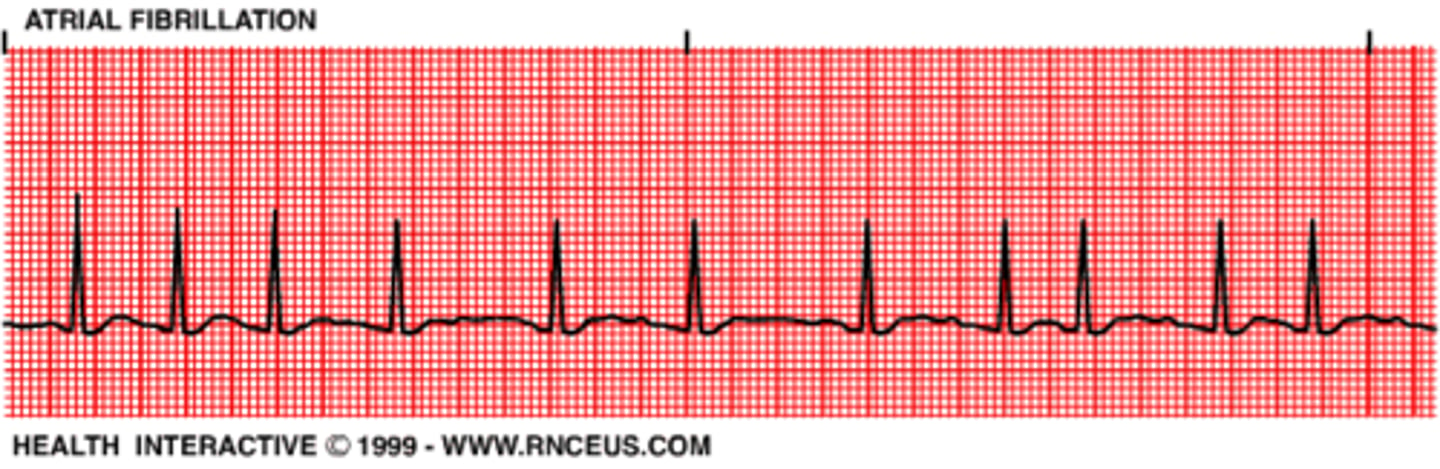
what is fibrillation? what would it look like on an ECG?
irregular (& often abnormally fast) heart rate
what is an ectopic heartbeat? what would it look like on an ECG?
changes in heartbeat leading to extra/skipped heartbeats

what is haemoglobin (Hb)?
protein that carries oxygen
how does the structure of haemoglobin allow it to bind to/react w/ oxygen?
quaternary protein - made up of 4 polypep. chains.
each polypep. chain contains a haem group (these bind to O2) - allows to bind to 4 O2 molecules at once
what is oxyhaemoglobin (HbO8)?
the molecule formed when Hb is carrying oxygen
what reversible reaction happens when oxygen associates/dissociates with/from haemoglobin?

where does association of oxygen (to haemoglobin) occur in the body?
alveoli/ near the lungs
where does dissociation of oxygen (from haemoglobin) occur in the body?
near respiring cells
what is an affinity for oxygen?
the tendency for a molecule to bind to oxygen
what is haemoglobin's affinity for oxygen affected by? (x4)
• partial pressure of oxygen
• Hb oxygen saturation
• whether it's fetal or adult Hb
• partial pressure of CO2/CO2 conc.n
(describe) how does partial pressure of oxygen (pO2) affect haemoglobin's affinity for oxygen?
• high pO2 = high affinity for O2 => association at lungs
• low pO2 = low affinity for O2 => dissociation at respiring cells
(describe) how does haemoglobin's O2 saturation affect it's affinity for oxygen?
Hb changes shape depending on its O2 saturation (can carry 4 O2)
• difficult (low aff.) when empty
• easy (high aff.) w/ 1 or 2 O2 mols
• difficult (low aff.) w/ 3 O2 mols bound
(describe) how fetal and adult haemoglobin have different affinities for oxygen?
fetal Hb has a higher affinity for O2 than adult Hb
explain why it's important for fetal haemoglobin to have a higher affinity for oxygen than adult haemoglobin
fetuses get their oxygen from the mother, through the placenta. as there's a low O2 saturation, the fetus must be able to associate w/ O2 - the process is: the mother's O2 dissociates & the fetal HB associates w/ this O2
explain why it's important for babies' haemoglobin to change from fetal Hb into adult Hb by 6 months of being born
since adult Hb has a lower affinity for O2, it allows the O2 to dissociate at respiring tissues (this wouldn't happen if the baby kept fetal Hb as it has a very high aff. for O2 & wouldn't dissociate so the baby wouldn't get O2 to its tissues)
what graph shows oxygen saturation of haemoglobin against partial pressure of oxygen?
oxygen dissociation curve
where would you find fetal haemoglobin on an oxygen dissociation curve, in relation to adult haemoglobin?
the fetal Hb would be seen to the left of the adut Hb graph
(describe) how does partial pressure of CO2 affect haemoglobin's affinity for oxygen?
• high pCO2 = low affinity for O2
• low pCO2 = high affinity for O2
what is the Bohr effect?
the shift to the right on an oxygen dissociation curve when partial pressure CO2 increases
what is the partial perssure of CO2 like at (a) the lungs & (b) respiring cells?
a) low
b) high
explain the Bohr effect (x steps) (for 90% CO2)
In the blood at respiring cells:
1) CO2 reacts w/ H2O to form carbonic acid (H2CO3) (catalysed by carbonic anhydrase)
2) the H2CO3 dissociates into H+ and hydrogencarbonate ions (HCO3-)
3) the H+ lowers the blood pH (more acidic)
4) HbO8 unloads its O2 so that:
5) it takes up the excess H+s to form haemoglobonic acid (HHb) & 4O2 (& prevent blood => too acidic)
6) HCO3- diffuses out of red blood cells (around resp. cells) & go to blood plasma
7) to compensate for this: Cl- diffuse into red blood cells (chloride shift)
When blood reaches lungs:
8) HCO3- & H+ react to form CO2 & H2O (CO2 goes to alveoli & is breathed out)
what is the role of carbonic anhydrase when transporting CO2 to the lungs?
catalyses reaction of CO2 & H2O -> H2CO3 (carbonic acid)
what is the importance of haemoglobonic acid (HHb) in the transport of CO2 to the lungs?
HBO8 unloads its O2 & binds to excess H+ ions & 'mops them up' to prevent the blood becoming to acidic (this forms HHb & 4O2)
what happens when hydrogencarbonate ions (HCO3-) diffuse out of the blood when transporting CO2 to the lungs? why?
chloride shift - Cl- ions (dissolved in blood) diffuse into the blood to compensate for the loss of HCO3- molecules - to balance the charge (lost) between plasma & red blood cells