Substance Abuse and Addictive Disorders
1/34
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
35 Terms
What is substance abuse?
Harmful consequences of use (social/legal/occupational)
What is substance dependende?
Tolerance, withdrawal, and loss of control over use
What is substance use disorder?
Cluster of cognitive, behavioral, and physiological symptoms indicating continued substance use despite significant substance related problems
Addiction is not an official DSM-5 diagnostic term but commonly used to describe the most severe, chronic stage of substance use disorder
Loss of self control and compulsive drug seeking behavior despite desire to stop
Negative connotations with term
Epidemiology of Substance Use Disorder
More prevalent in males than females
More prevalent in younger individuals: peak rates in late adolescence and early adulthood, declining after age 26
More common among:
White and Native American individuals
Unmarried or previously married adults
Lower education and income
High income North American and Eastern/Western European show disproportionately high rates
High income North America → highest prevalence of cannabis, cocaine, and opioid dependence
Eastern European → highest alcohol use disorder
Etiology of Substance Use Disorder
Genetic and environmental
Key genes implicated (do not need to know specific gene type)
ADH1B and ALDH2 for alcohol related
CHRNA5-CHRNA3-CHRNA4 for nicotine related
OPRM1, DRD2, DRD4, BDNF, and SLC6A4 associated with multiple substances
Early initiation of substance use is critical risk factor
Adverse childhood experience → dose response relationship between the number of traumatic events and substance use disorder risk
>= 4 ACEs < 18 y/o multiplies risk for smoking by 3, alcohol by 4, and any substance misuse by 7
DSM 5-TR Criteria for Substance Use Disorder
Requires meeting at least 2 of the 11 criteria within 12 month period
Criteria organized into 4 domains
Impaired control
Social impairment
Risky use
Pharmacological criteria
Severity
Mild: 2-3 criteria
Moderate: 4-5 criteria
Severe >= 6 criteria
Impaired Control
Criteria 1-4
Larger amounts or longer use: taking the substance in larger amounts or over a longer period than originally intended
Persistent desire or unsuccessful efforts to cut down: expressing a persistent desire to regulate substance use with multiple unsuccessful efforts to decrease or discontinue use
Great deal of time spent: spending a great deal of time obtaining a substance, using it, or recovering from its effects and in severe cases all daily activities revolve around the substance
Craving: experiencing an intense desire or urge for the drug, more likely when in an environment where the drug was previously obtained or used. Can be assessed by asking if there has ever been a time when urges were so strong the individual could not think of anything else
Social Impairment
Criteria 5-7
Failure to fulfill major role obligations: recurrent substance use resulting in failure to fulfill major obligations at work, school, or home
Continued use despite social/interpersonal problems: continuing substance use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the substance's effects
Giving up important activities: important social, occupational, or recreational activities are given up or reduced because of substance abuse
Risky Use
Criteria 8-9
Recurrent use in hazardous situations: recurrent substance use in situations in which it is physically hazardous
Continued use despite physical/psychological problems: substance use is continued despite knowledge of having persistent or recurrent physical or psychological problem likely caused or exacerbated by the substance
The key issue is the individual’s failure to abstain despite the difficulty it is causing
Pharmacological Criteria: Criteria 10-11
Tolerance: requiring a markedly increased dose to achieve the desired effect, or experiencing a markedly reduced effect when the usual dose is consumed. The degree of tolerance varies greatly across individuals and substances
Withdrawal: experiencing characteristic withdrawal syndrome for the substance or raking the substance (or closely related substance) to relieve or avoid withdrawal symptoms
Note that withdrawal symptoms are not specific for certain substances, including phencyclidine, other hallucinogens, and inhalants
Screening
CAGE
2 or more on the questionnaire is (+)
Not as sensitive to diagnosing someone with alcohol use disorder
Good screener but not diagnostic tool
Anyone who tests (+): should explore more
AUDIT
Gold standard for alcohol screening
Score of 8 or greater increases likelihood of alcohol use disorder
DAST-10
Specifically for drug disorder, excludes alcohol
Can be combined with AUDIT to include other substances
Alcohol Use Disorder General
Mean age at AUD onset is 26.2 years
Men have substantially higher rates than women
Only 19.8% of individuals with lifetime AUD have ever received treatment
Genetic factors account for 40-60% of AUD risk
Alcohol activation of brain reward regions through increased dopamine release in the mesolimbic dopamine system → projects to the orbitofrontal and prefrontal cortices
Alcohol affects GABA, glutamate, cannabinoids, NE, 5HT, and HPA
Repeated exposure → neurotransmitter responses are blunted → tolerance and withdrawal symptoms
Mental health conditions that show significant association
Anxiety
Depression
PTSD
Schizophrenia
Bipolar disorder
Antisocial and borderline personality
Pathophysiology of Alcohol Use Disorder
Drinking releases dopamine in mesolimbic pathway → repeated drinking → brain tries to balance and reduces natural dopamine activity → need more EtOH to get same reward, which builds tolerance
GABA: increases
Glutamate: decreases
Overtime, brain will decreases GABA and increase glutamate
Withdrawal → too little GABA and too much glutamate
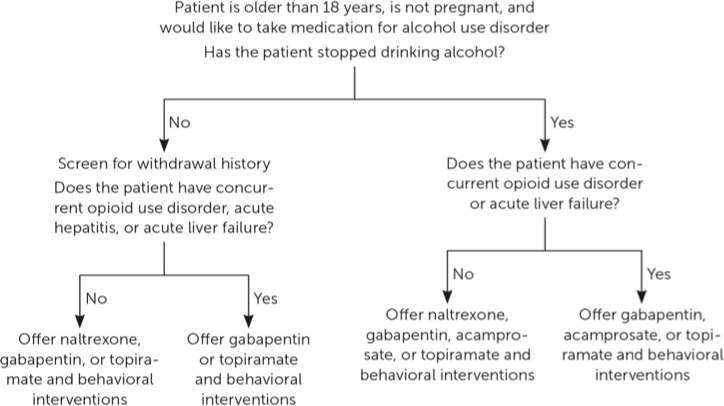
Alcohol Use Disorder Management
First-line medications: naltrexone (first line) and acamprosate
Naltrexone: opioid receptor antagonist that reduces craving and alcohol consumption
Contraindications: acute hepatitis, liver failure, and opioid use
Acamprosate: modulates glutamatergic neurotransmission and promotes abstinence
Contraindications: severe kidney impairment
Disulfiram: causes adverse reaction (flushing, nausea, tachycardia, hypotension) with EtOH consumption by inhibiting aldehyde dehydrogenase (produced toxic levels of acetaldehyde)
Contraindications: advanced liver disease
Second line medications: topiramate and GABA
Topiramate: potentiates GABA-A and inhibits glutamate activity
Gabapentin: increases abstinence rates but has abuse potential and overdose risk when combined with opioids
Motivational Interviewing
Identify individual values and invoke inwardly motivated change to align behavior with said values
CBT
What is alcohol intoxication?
Behavioral:
Disinhibition
Impaired judgment
Mood lability
Aggression
Physical:
Slurred speech
Ataxia
Nystagmus
Impaired attention/memory
Severe:
Stupor, coma
Respiratory depression
Chronic use:
Acute rosacea
Palmar erythema
Hepatomegaly
Dupuytren’s contracture
Testicular atrophy
Gynecomastia
Elevations: GGT and transaminases, LDH, MCV
Decreases: BUN, LDL, RBC volume
What is alcohol withdrawal?
Onset: 6-24 hours after cessation
Autonomic:
Tremor,
Tachycardia (>100 bpm)
Hypertension
Hyperthermia
Diaphoresis
Neuropsychiatric:
Anxiety
Restlessness
Insomnia
Agitation
GI: Nausea, vomiting
Severe complications (10% of symptomatic patients):
Seizure: peaks at 24 hours but can occur 8-48 hours after
Hallucinations: 12-24 hours after
Delirium tremens: severe confusion, disorientation, severe autonomic hyperactivity
Onset 72-96 hours
Can see complications beyond the 96 hours: do not cut off benzodiazepines right at 96 hours and continue until entire duration of symptoms has passed
MUST NOT MISS
Duration: symptoms peak at day 2, improve by days 4-5
Residual anxiety/insomnia may persists for 3-6 months
Alcohol Withdrawal Management
Ambulatory care is suitable for most uncomplicated cases
Hospitalization for high-risk patients → history of seizures, concurrent medical or psychiatric illness, GABAergic drug dependence, lack of safe home environment, CIWA
Long acting benzodiazepines with active metabolites (diazepam, chlordiazepoxide) effective for most patients
Carry risk of misuse and possible encephalopathy in advanced liver disease
Short acting benzodiazepines without active metabolites (oxazepam, lorazepam) preferred for patients with liver disease
Symptom-triggered medication reduces both the dose and duration of benzodiazepine treatment compared to fixed-schedule medication and is recommended in settings where frequent monitoring can be provided
Severe withdrawal requiring intensive care warrants IV administration of midazolam, phenobarbital, etc…
CIWA >= 15 or starting to show signs of what could be DT or seizures
Thiamine supplementation to prevent Wernicke's encephalopathy
Symptom-triggered: diazepam 10mg or chlordiazepoxide 50-100 mg every hour if CIWA >= 10
Fixed-dose taper: diazepam 10 mg every 6 hours on day 1, every 8 hours on day 2, every 12 hours on day 3, and at night on day 4
Front loading: for severe withdrawal (CIWA >= 19) → diazepam 20 mg every 1-2 hours for 3 doses or 10 mg every hour and then transition to symptom triggered dosing
Reduces symptom duration, withdrawal seizure incidence, and delirium duration
Alternatives:
Phenobarbital can be used as monotherapy or adjunctive to benzodiazepines
Advantages: rapid onset, long half life, wide therapeutic range, and minimal sedation at moderate doses
DO NOT FOCUS ON DOSING/TIMING
Wernicke’s Encephalopathy
Acute, potentially reversible neurological emergency caused by thiamine (vitamin B1) deficiency
Symptom triad:
Mental status changes
Ocular abnormalities
Ataxia
Clinical diagnosis based on the Caine criteria (require at least two of four signs):
Dietary deficiencies
Eye signs: nystagmus, lateral rectus palsy, conjugate gaze palsies
Cerebellar dysfunction
Either altered mental status or mild memory impairment
MRI is the most valuable para-clinical tool, typically showing symmetric T2/FLAIR hyper-intense signals in specific brain regions
Alcohol is the MC risk factor
Reduces thiamine absorption from gut and increases renal loss
Alcoholic liver damage impairs thiamine storage
Alcohol impairs thiamine dependent enzyme activity
Magnesium deficiency (common in heavy alcohol use) reduces thiamine cofactor function
Treatment → high dose IV thiamine (500 mg TID for 2-3 days)
Korsakoff Syndrome
Chronic, largely irreversible sequela of untreated or inadequately treated Wernicke encephalopathy
Approximately 80-85% of patients with untreated WE develop KS
Symptoms:
Severe anterograde and retrograde amnesia
Confabulation
Executive dysfunction
MRI shows similar to Wernicke: symmetric T2/FLAIR hyper-intense signals in specific brain regions
Treatment: prevention
Opioid Use Disorder General
Third most prevalent substance use disorder worldwide
Fentanyl has been the MC cause of opioid overdose deaths since 2016, accounting for 88% of opioid overdose deaths (47,369) in 2024
Higher rates among men than women, young adults (ages 18-25) than older adults
Risk factors:
History of anxiety disorder increases risk by 50%
History of another substance use disorder increases risk by 300%
Mood disorder, personality disorders, psychotic disorders, PTSD
ACE
Drug availability, peer substance use, social disadvantage, poor educational attainment
Opioid Use Disorder Management
First-line treatments
Methadone: full u opioid receptor agonist
Can only be dispensed at federally regulated opioid treatment programs
Side effects
Sweating
Constipation
Sedation
QT prolongation
Endocrine suppression
Buprenorphine: partial u opioid receptor agonist
Reduces cravings and withdrawal symptoms while blocking effects of illicit opioids
Sublingual formation taken 1-3 times daily at home: can be prescribed in office based setting
Risk of precipitated withdrawal if initiated while patient has opioids in system
Side effects
HA
Nausea
Sedation
Constipation
Endocrine suppression
Naltrexone: opioid antagonist
Completely blocks opioid effects
Requires 7-10 days of opioid abstinence before initiation to avoid precipitated withdrawal
Side effects
N/V and abdominal pain
Naloxone is Narcan
Opioid Intoxication
Classic Triad
Miosis (pinpoint pupils)
Respiratory depression
Decreases consciousness
CNS:
Euphoria
Sedation/drowsiness
Impaired judgment
Psychomotor retardation
Physical:
Bradycardia
Hypotension
Hypothermia
Constipation/nausea
Severe:
Coma
Apnea
Death from respiratory arrest
Opioid Withdrawal
Onset
6 hours (short acting: fentanyl/heroin) to 1-3 days (long acting: methadone, buprenorphine)
Autonomic: mydriasis, piloerection, hyperhidrosis, tachycardia, hypertension, hyperthermia, lacrimation, rhinorrhea, yawning
Neuropsychiatric: anxiety, restlessness, irritability, dysphoria, insomnia, cravings
GI: nausea, vomiting, abdominal cramping, diarrhea
Musculoskeletal: myalgias, bone/joint aches
Duration:
Days to weeks
Protracted withdrawal (dysphoria, cravings, insomnia, hyperalgesia) may last months
Note:
Uncomfortable but rarely life threatening
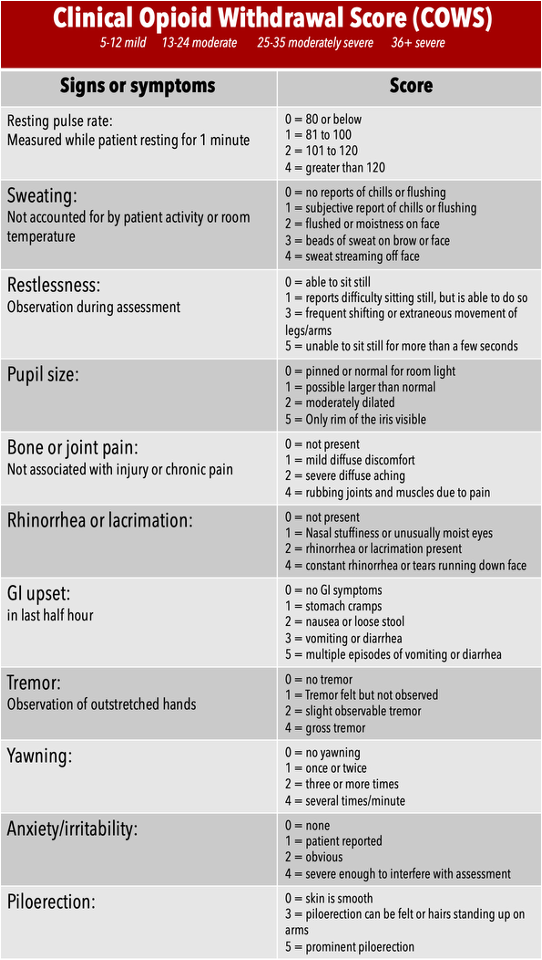
Withdrawal Score:
COWS
Mild: 5-12
Moderate: 13-24
Severe: > 24
Opioid Withdrawal Management
Medications for withdrawal:
Opioid agonists: methadone and buprenorphine (preferred)
Alpha 2 receptor agonists: lofexidine (FDA approved) and clonidine
Symptomatic: ibuprofen for pain, ondansetron for nausea
Withdrawal management without long-term MOUD is associated with increased relapse, morbidity, and death
Cannabis Use Disorder General
Cannabis is general term for all forms of cannabinoid compounds
Have natural and synthetic
Active ingredient is THC: acts on CB1 and CB2 cannabinoid receptors throughout CNS
THC metabolites lipid soluble and accumulate in fat cells
Intoxication lasts 2-4 hours but behavior changes can last many hours longer
Routes of ingestion
Smoked, ingested, vaporized, edibles
About two-thirds of persons with CUD have at least one other current substance use disorder, most commonly alcohol or tobacco
Almost half have a current non-substance psychiatric disorder
Cannabis potency has doubled over the past two decades
Increased cannabis induced psychosis?
Psychosocial interventions is mainstay treatment
Cannabis Intoxication
Psychological: euphoria, relaxation, altered time perception, impaired judgment, anxiety, paranoia
Cognitive: impaired attention, concentration, working memory, reaction time
Physical: conjunctival injection, increased appetite, dry mouth, tachycardia
Severe: panic attacks, psychosis (especially with high THC), cannabinoid hyperemesis syndrome (cyclic vomiting with chronic heavy use)
Cannabis Withdrawal
Onset: 1-2 days after cessation
Peak: days 2-6
Psychological (predominant): irritability, anxiety, restlessness, depressed mood, anger/aggression
Sleep: insomnia, disturbed sleep, strange/vivid dreams
Physical (less common): decreased appetite, weight loss, abdominal cramps, muscle aches, tremor, headache, sweating, chills
Duration: several weeks but some symptoms may persist longer
Usually mild and self limiting
Behavioral/emotional symptoms more prominent than physical symptoms
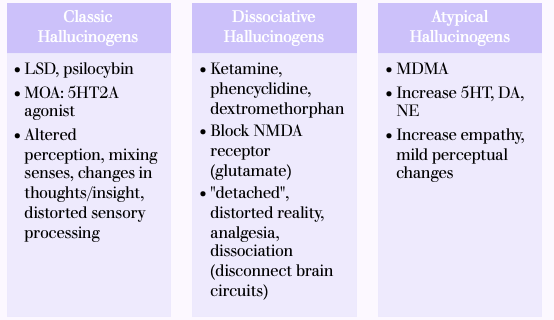
Hallucinogens General
Disrupt how the brain processes perception, mood, and reality mainly by altering serotonin, glutamate, or dissociative pathways
Hallucinogen Persisting Perception Disorder (HPPD):
Rare chronic condition with re-experiencing of perceptual disturbances (visual snow, trails, halos, geometric patterns) when sober
Can be episodic or continuous, lasting weeks to years
Primarily after LSD use
Sedative Hypnotics General
Includes:
Benzodiazepines and benzodiazepine-like drugs
Barbiturates and barbiturate like drugs
Carbamates
Benzodiazepines:
Most widely prescribed medications: only small subset actually abuse them
Intoxication: symptoms dose related
Lethargy, impaired mental function, poor memory, irritability, self neglect, emotional disinhibition
As it progresses: slurred speech, ataxia, impaired coordination
Retrograde amnesia can occur
Severe: paradoxical agitation, respiratory depression
Reversal with flumazenil (can elicit seizures)
Withdrawal: similar to EtOH
Stimulant Use Disorder General
68-82% have a co-occurring mental health disorder and 72-78% had another substance use disorder
Amphetamine, methamphetamine (also includes Adderall)
Enters the neuron → pushes dopamine out of storage vesicles through reverse transporters → dump dopamine into synapse → massive dopamine surge
Cocaine, methylphenidate
Block reuptake transporters for dopamine and NE so that they stay longer in synapse
Happens in nucleus accumbens (euphoria/addiction) and prefrontal cortex (focus/attention)
Medical complications (vary by route of administration):
Cardiovascular: MI, arrhythmias, stroke, aortic dissection, sudden cardiac death
Pulmonary: coughing, bronchitis, pneumonitis (smoked), pneumothorax
Neuropsychiatric: cognitive impairment, psychosis, seizures, increased risk of schizophrenia and PD
Infectious: HIV, hepatitis B/C, endocarditis, osteomyelitis (injection), STIs
Other: nasal septum perforation (IN), meth mouth, malnutrition, weight loss
Standard of care: contingency management
Provides tangible rewards (vouchers/prizes) to reinforce behaviors such as abstinence and treatment attendance
Stimulants Intoxication
Psychological: euphoria, increased energy/confidence, grandiosity, hypervigilance, interpersonal sensitivity, impaired judgment
Behavioral: talkativeness, psychomotor agitation, repetitive/stereotyped behaviors, aggression
Autonomic: tachycardia or bradycardia, hypertension or hypotension, mydriasis, hyperthermia, diaphoresis
Severe: paranoid ideation, hallucinations (auditory, tactile), psychosis, seizures, cardiac arrhythmias, myocardial infarction, stroke, hyperthermia, death
Stimulants Withdrawal
Onset: within hours to several days after cessation
BIG MOOD CRASH (looks like depression)
Psychological: dysphoric mood (most prominent), anhedonia, fatigue, anxiety, irritability, emotional lability
Sleep: insomnia or hypersomnia, vivid unpleasant dreams
Physical: Increased appetite, psychomotor retardation or agitation
Duration:
Typically 12-24 hours of somnolence/irritability
Depressive symptoms can meet criteria for major depression but usually resolve within 1 week (can last for 1 month)
Note: suicidal ideation is the most serious withdrawal complication
Stimulants Intoxication Management
First-line for agitation = benzodiazepines
Antipsychotics for psychotic symptoms
Hyperadrenergic states
Benzodiazepines
Phenobarbital
Propofol
Alpha 2 agonists
Beta blockers with alpha 1 antagonism
Not propranolol: increase vasospasm and lead to MI/stroke
CCB
Nitroglycerin
Nicotine General
Stimulant that works by activating specific receptors in the brain, leading to a dopamine release (reward)
Nicotine acetylcholine receptor agonist: when nicotine binds → opens ion channels and sodium and calcium enter the neuron → neuron becomes excitable → leads to release of multiple neurotransmitters
Dopamine: reward/addiction
NE: alertness
Acetylcholine: attention
Glutamate: learning/memory
With repeated use: receptors become desensitized and brain up regulates more receptors
Nicotine Use Disorder Management
First line pharmacological treatment
Varencicline
Combination NRT (long acting patch and short acting form)
Bupropion
Single form NRT
Initial treatment duration is typically 12 weeks but can be extended to 6 months or longer for patients who need continued support to maintain abstinence
Black box warning was removed from Chantix