THE CLINICAL RELEVANCE OF THE GROWTH OF THE HEAD AND JAWS AFTER BIRTH
1/77
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
78 Terms
how many bones are in the human head
28 bones
8 cranial
14 facial
6 auditory
(+ 1 hyoid)
is post natal growth of the head and face proportional in each bone
no, post-natal growth is not due to simple proportional enlargement of each bone
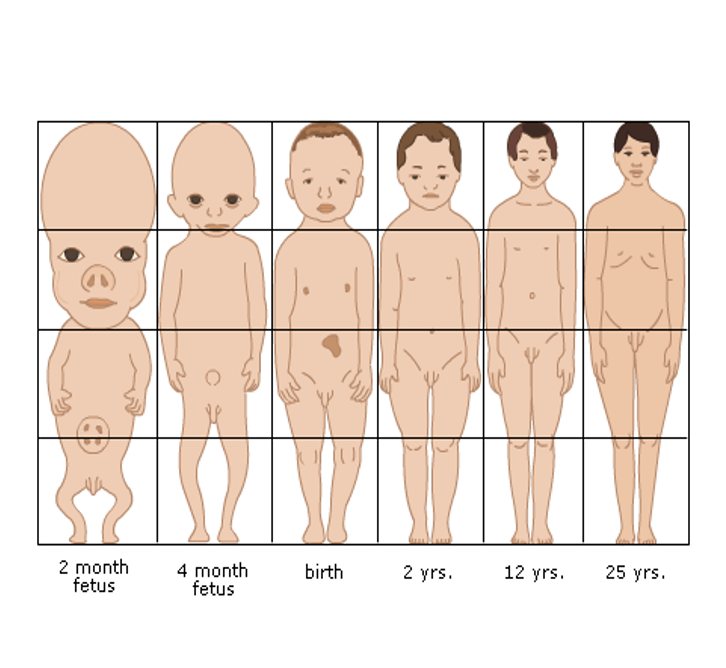
what is the ratio of head:body at birth VS in adulthood
birth 1:4
adult 1:8
what are the two types of growth occurring in the head and face
intramembranous bones grow by periosteal remodelling
endochondral bones grow by cartilaginous replacement
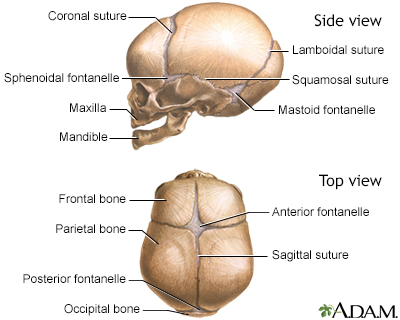
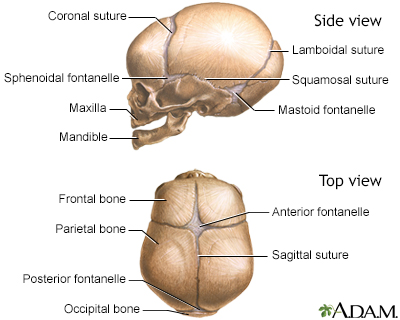
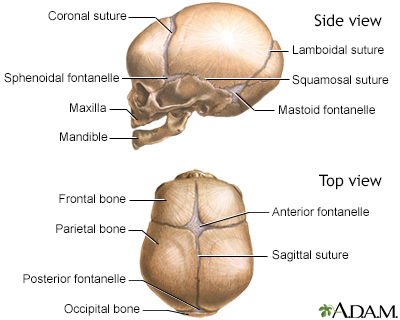
what is the function of fontanelles
fontanelles give the skull flexibility as it goes through the birth canal
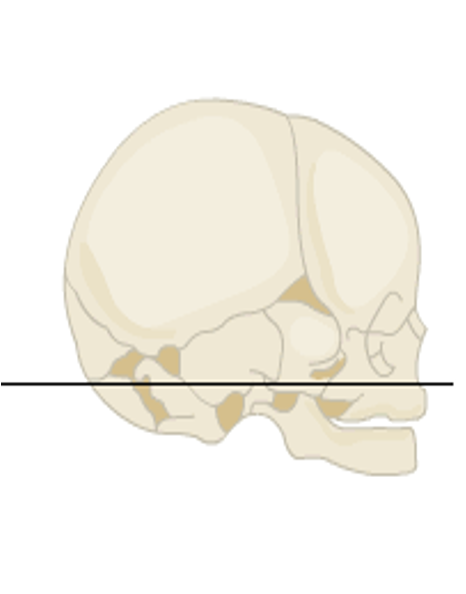
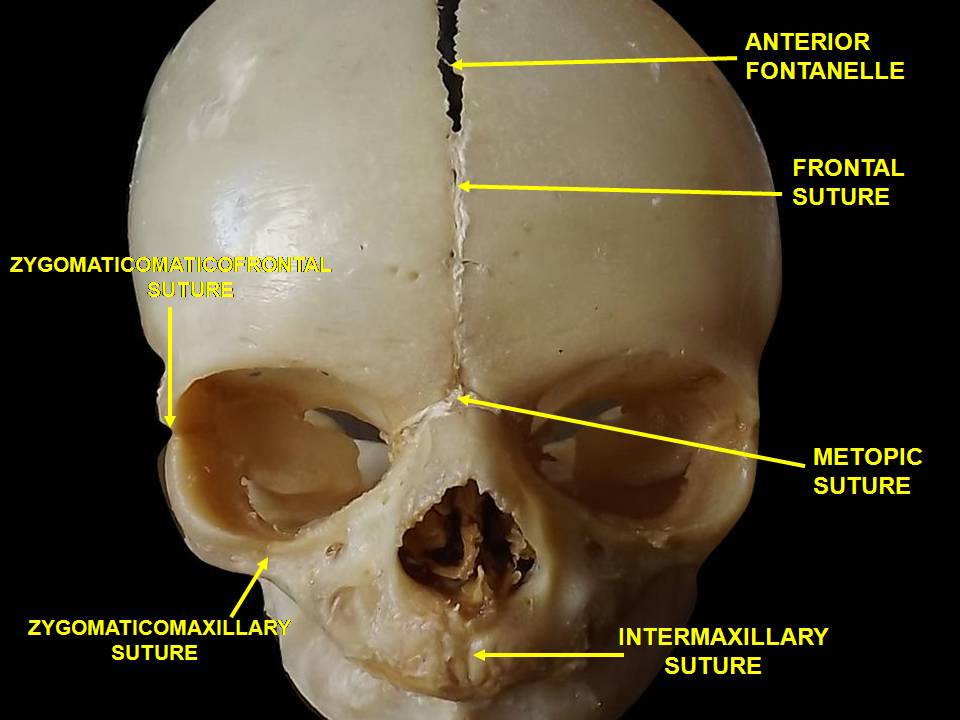
outline the skull at birth
sutures
6 fontanelles (posterior, anterior, x2 sphenoid, x2 mastoid)
define cranial vault
cranial vault: the part of the skull that encloses or protects the brain i.e. calvaria, skullcap
outline the growth of the brain in terms of its weight
1yr = 50% of what it will be in adulthood
3yrs = 75%
7yrs = 90%
11yrs = 100%
—
the surrounding cranium expands to accommodate it
expansion of the cranium is due to _____ ______
expansion of the cranium is due to brain growth
outline sutural growth
at birth the 6 fontanelles are present and closing at 18 months
bone is laid down at sutures in response to brain growth and increasing pressure
some sutures begin to fuse at approx. 7yrs
all mostly fused mid-late teens

outline the growth of the cranial vault in later childhood and adolescence
development of lower 2/3 of face
downwards and forwards growth of maxilla and mandible
elongation of nose
backward shift of orbits
—
dramatic physical changes during puberty often occurs up to 2 years earlier in girls than in boys
define cranial base
cranial base: the bony floor of the skull that separates the brain from the face and neck
involves the frontal, ethmoid, sphenoid, temporal, occipital bones
what is the post natal growth of the cranial base via
endochondral
surface remodelling
what are synchondroses
synchondroses: isolated regions of cartilage that joins bone
once growth has ceased, the cartilage is then replaced by bone

what are the cranial base synchondroses
spheno-ethmoidal
spheno-occipital
inter-sphenoid (ISS)

outline the spheno-ethmoidal synchondroses
anterior cranial base
neural growth pattern - genetically controlled
fuses at the age of 7
stable by 8-10yrs

outline the spheno-occipital synchondroses
posterior cranial base
somatic growth pattern
present into mid-late teens
stable by late teens
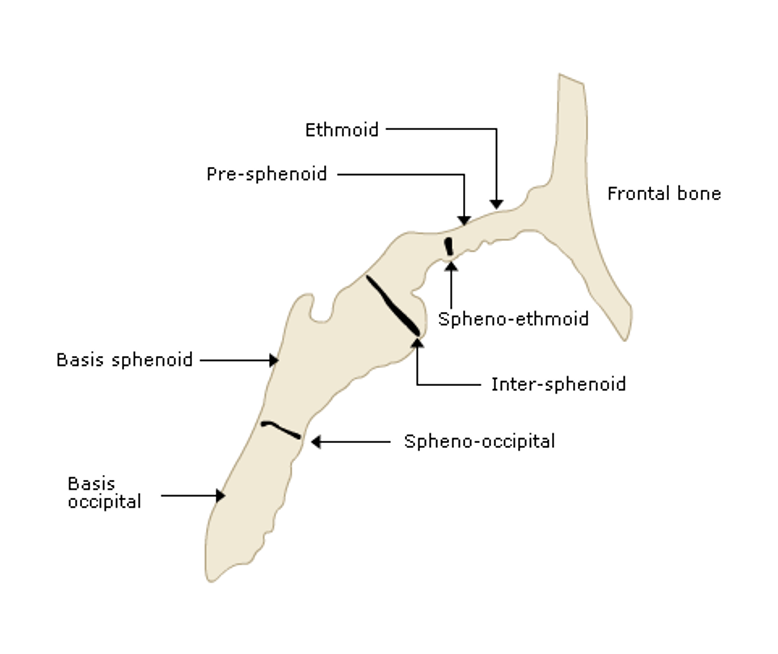
outline the inter-sphenoid (ISS) synchondroses
fuses between 2-3yrs of age
outline the nasomaxillary complex
consist of the maxilla, some bones of the nasal cavity and parts of the orbit
outline the growth pattern of the maxilla
grows downwards and forwards - appears to move downwards more than forwards
new bone added to both sides of sutures
also grows in width due to midpalatal suture which fuses around puberty
—
remodelling continues on bone surfaces
floor of nose is resorbing
bone added to FOM

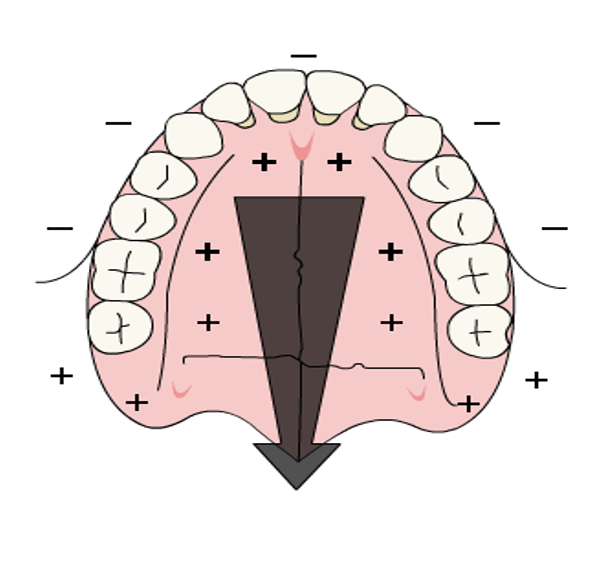
why is knowledge of the growth pattern of the maxilla relevant to dentistry
can incorporate fusion of sutures into treatment for certain patients
expansion of maxilla can be done as a narrow arch can result in crowding of teeth (image)
bone will be laid down at the mid palatal suture - this takes a few months
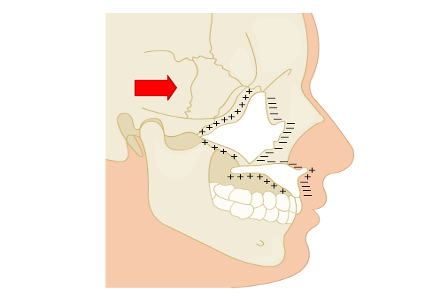
state the direction that surface remodelling takes place in relation to bone translation in the maxilla
surface remodelling occurs in the opposite direction to bone translation


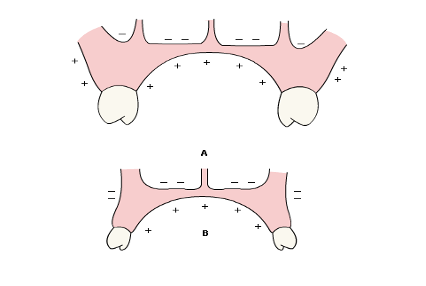
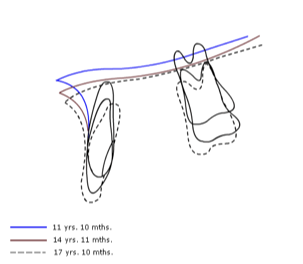
in what manner does the mandible grow
the mandible grows in height and length
growth appears forwards and downwards away from the base of the skull
there is also a rotational pattern to mandibular growth (image)
reflections of differential growth in anterior and posterior face heights
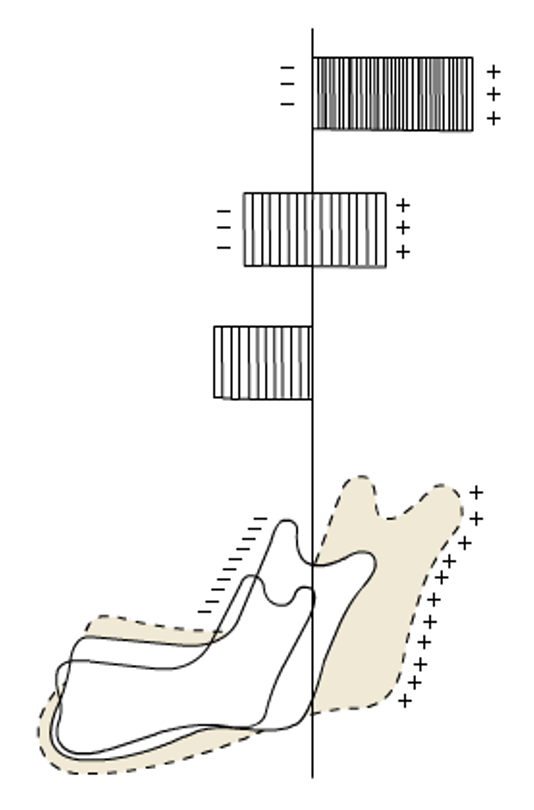
outline the growth pattern of the mandible
one area of growth: condyle
grows in length by cartilage replacement which then becomes ossified
proliferative cell zone can differentiate into chondroblasts
growth also seems to occur via resorption from anterior surface and deposition on posterior surface
remodelling of glenoid fossa also occurs
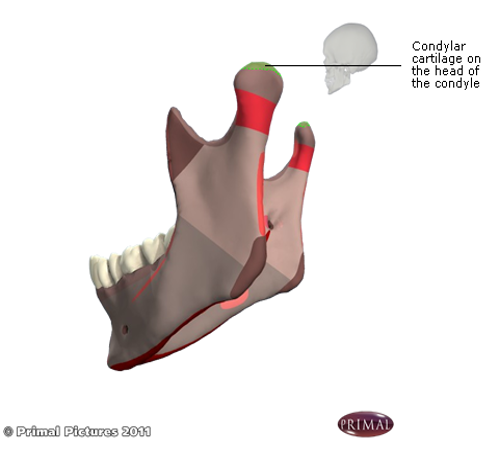
what does the condylar cartilage in the mandible resemble in long bones
the epiphyseal plate cartilage of long bones
what type of grows does the mandible undergo
appositional (increase in thickness/ width/ diameter), not proliferative
state the histological appearance of the mandible (in growth)
not organised into parallel columns
histologically, it has a different appearance to the organisation at the spheno-occipital synchondroses cartilage
when does growth in mandibular length cease
growth in mandibular length ceases in late teens
when does growth in mandibular height cease
growth in mandibular height continues very slowly throughout life
outline studies done by Björk in Copenhagen in the 1950-60s
longitudinal studies
using metal implants in the jaws to study growth
done because sequential radiographs had no reliable reference point so metal pins were inserted as a reference point instead
unethical: no therapeutic benefit, radiation exposure
how was growth observed in Björk’s studies
can see internal rotation in the core of the mandible relative to the cranial base
done by superimposing serial radiographs with metal implants
masked by surface apposition and resorption
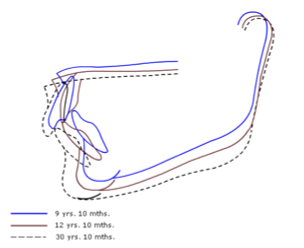
Björk’s findings pt. 1
majority had an ‘anterior’ rotation
mandibular plane angle decreases by 2-4°
increasing overbite
more skeletal class III occlusion (underbite)
leads to late lower incisor crowding?
genetic link?
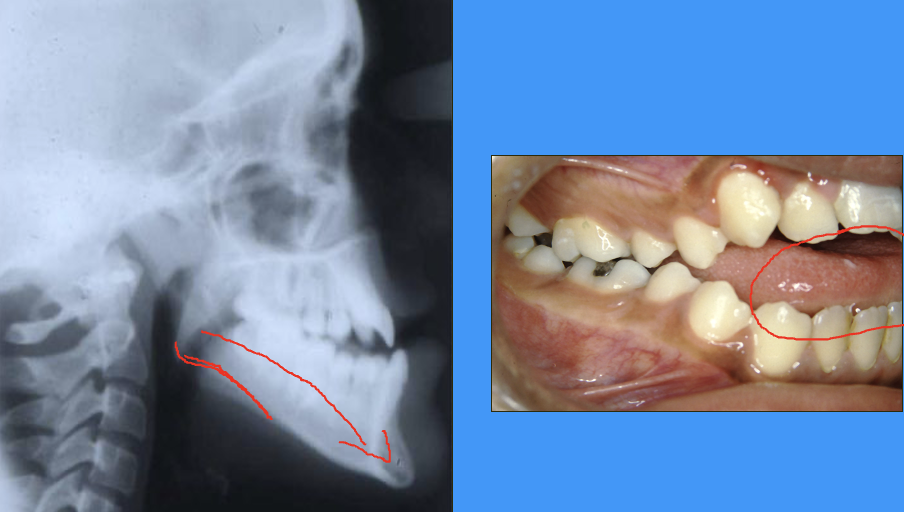
radiograph and clinical image showing anterior growth rotation of mandible

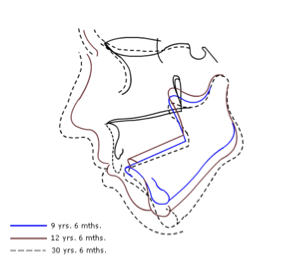
Björk’s findings pt. 2
minority had a ‘posterior’ rotation
mandibular plane angle increases » anterior open bite
more skeletal class II occlusion
leads to late lower incisor crowding?
genetic link?
radiograph and clinical image showing psoterior growth rotation of mandible
(not same radiograph and clinical image)
why may waiting until a patient is older to start treatment planning be wise (if they are showing early signs of atypical jaw relationship)
may wait until a patient is older so we know the exact relationship between mandible and maxilla so treatment planning is more certain and stable
this means we will not be fighting against the natural growth of the jaws
what else did Björk identify in the mandible
‘stable’ anatomical structures
these can be used as a reference point instead of the metal pins
does the maxilla also have rotational growth patterns
small but variable rotations - majority are anterior so the upper can occlude on the lower
there is a mean 3° anterior (rotation) - but can be backwards
genetic link?
outline the growth pattern of soft tissues
grow and change throughout life
most rapid growth occurs around puberty
these may mask or enhance hard tissue growth changes
genetic link?
why is knowing the growth patterns of the bones that make up the head important in dentistry
need to decide if the problem is due to underlying skeletal problems or the teeth themselves
sometimes it may not only be limited to just the teeth
define growth site VS growth centre
growth site: a location at which growth occurs
growth centre: is a genetically controlled growth site where growth occurs
—
therefore all growth centres are growth sites but the converse is not true
what are the theories of postnatal head and face growth
remodelling theory
sutural theory
cartilaginous theory
functional matrix theory
part-counterpart principle
servo-system theory
outline the remodelling theory
remodelling theory
emphasis upon remodelling as primary mechanism by which all bones witthin the craniofacial complex grow
very little emphasis on sutures and cartilages
outline the sutural theory
sutural theory
primary growth of craniofacial skeleton is genetically regulated and was being controlled within sutures and cartilages
outline the cartilaginous theory
cartilaginous theory
emphasis was placed on the role of the cartilage in producing the driving force for craniofacial growth
nasoseptal cartilage, synchondroses, condylar cartilage etc.
outline the functional matrix theory
functional matrix theory
growth was not genetically determined
no real role of genetics
more to do with function of the head and face complex as a whole
outline the part-counterpart principle
part-counterpart principle
skull is composed of numerous structural components whose growth and development is complemented by a series of counterparts
e.g. growth of maxilla as a component as how the mandible grows in response to it - this needs to be matched to maintain normal occlusion
outline the servo-system theory
servo-system theory
there is genetically regulated growth of primary cartilages within cranial base and nasal septum
these provide a changing reference which is mediated by dental occlusion
the mandible is to respond to this changing occlusal reference by muscle adaptation
the theories of head and face growth go from entirely _______ to entirely _____________
genetic, environmental
graph showing growth
dark green = maxilla
light green = mandible
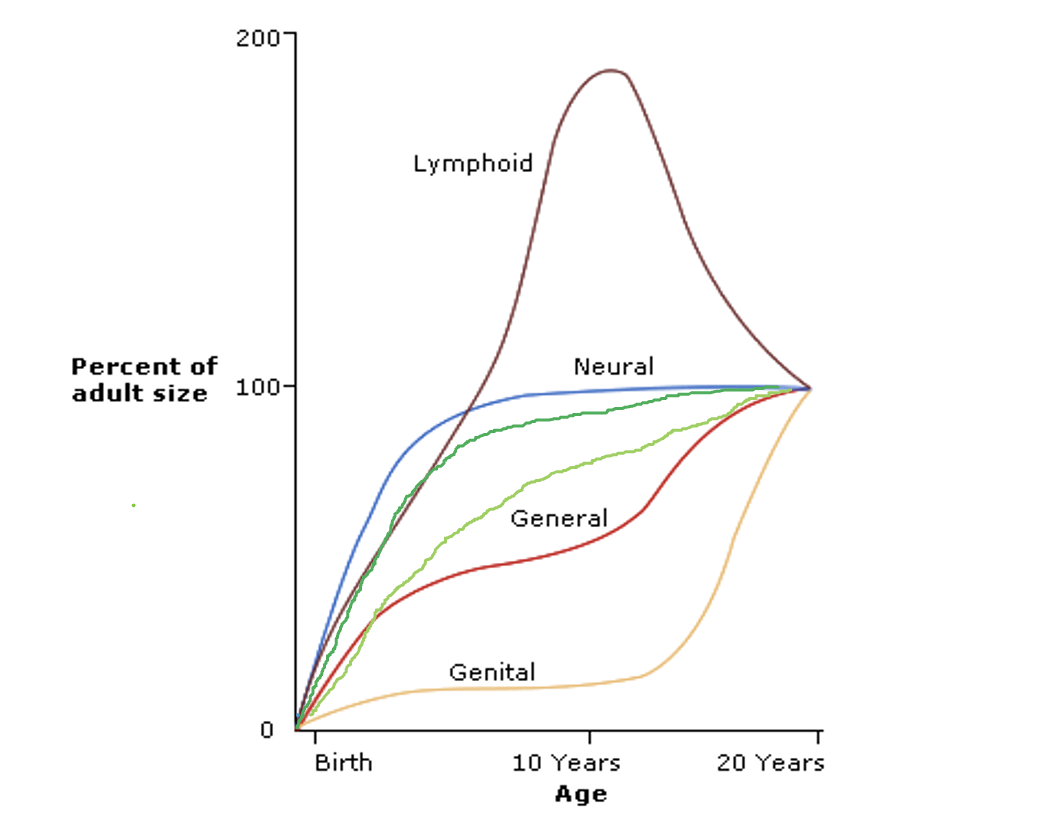
periods of rapid facial growth occurs at about the same time as…
periods of rapid facial growth occurs at about the same time as rapid growth in height
Björk and Bergensen
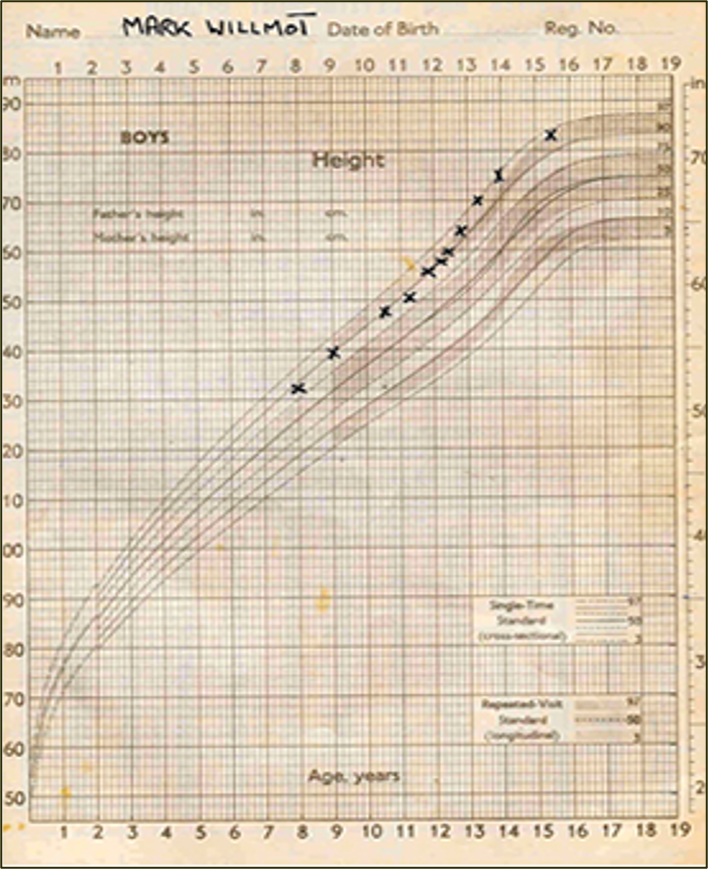
if someone is tapering off in their height, what can be inferred about their jaw growth
it can be inferred that their maxilla and mandible will also almost be at their final size for adulthood
standing height can essentially be used as a proxy for facial growth
image of growth chart for children
graph showing increase in height overtime
red dots = height
blue dots = velocity
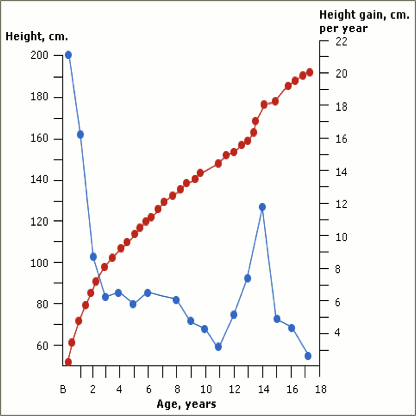
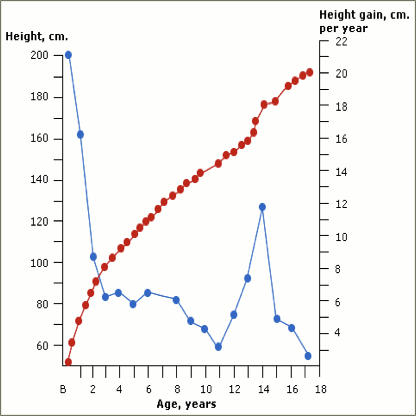
what can be inferred from this graph
velocity of height growth is very fast in babies and during puberty
outline methods of measuring head and face growth
hand wrist radiograph
cervical spine maturation radiograph

outline hand wrist radiographs
ulnar sesamoid bone ossifies at the start of pubertal growth spurt
median bone maturity stage for each chronological age and sex identified and compiled as atlases
limited value
is not really done anymore

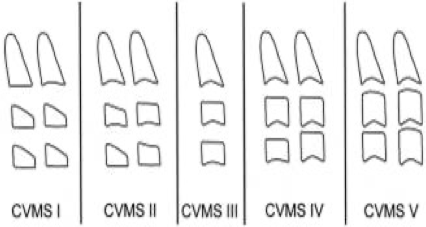
outline cervical spine maturation
undertaken on a lateral cephalometric radiograph
Baccetti suggested a method based on examining 3 cervical vertebrae
not used frequently
cervical spine maturation shapes
how can radiographs be used to compare growth
can compare rapid growth between ages by superimposing radiographic images taken
observe when change has stabilised so treatment can start
what are the ways growth can be affected to result in atypical postnatal growth
congenital
primary growth disorders - e.g. condylar hyperactivity, condylar hyperplasia, hemi-mandibular elongation
acquired - e.g. juvenile idiopathic arthritis (can affect mandible growth)
trauma - e.g. fractured condyle
what is the term for the early fusion of sutures
craniosynostosis
in what syndromes are craniosynostosis seen
Crouzon
Apert
Pfeiffer
outline Crouzon syndrome
birth defect
abnormalities caused by fusing of both sides of the coronal suture
often causes skull to be short in the front and back
flat cheek bones and flat nose are typical
outline Apert syndrome
craniofacial abnormality characterised by abnormal head shape
small upper jaw
fusion of fingers and toes
outline Pfeiffer syndrome
birth defect
abnormalities of skull, hands, feet
wide-set, bulging eyes
underdeveloped upper jaw
beaked nose
brachycephaly is caused by the premature fusion of which suture(s)
coronal
Kleeblattschädel syndrome is caused by the premature fusion of which suture(s)
almost all of the fibrous sutures
results in a cloverlead skull shape
Oxycephaly is caused by the premature fusion of which suture(s)
coronal and sagittal sutures
Scaphocephaly is caused by the premature fusion of which suture(s)
sagittal suture
Trigonocephaly is caused by the premature fusion of which suture(s)
fusion of the two halves of the frontal bones at the metopic suture

outline achondroplasia
short stature
large head
prominent forehead (frontal bossing)
small midface
flattened nasal bridge
—
genetic link
outline cleft lip and palate
syndromic or non-syndromic
1 in 700 births
issue with pharyngeal arches rather than sutures or cartilages
cleft lip and palate statistics
unilateral CLP 40%
CP 30%
bilateral CLP 10%
CL 10%
other 10%
which tooth is commonly affected by CLP
canine development
outline result of those who have CLP that have been operated on after birth
lip minimal effect
hard palate surgery » maxillary retrusion
mandible would be small
outline result of those who have CLP that have not been operated on after birth
(fairly) normal maxilla development
mandible is smaller