Lecture 1- From curing illness to promoting health (SG)
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
What does the biomedical model say about disease?
All diseases can be explained by disturbances in physiological processes, resulting from injury, biochemical imbalances, bacterial or viral infection etc.
Give 3 advantages of the biomedical model
Increased life expectancy
Increased quality of life for chronic patients
Advances in medical technology (heavy use of scientific method and value of evidence)
Give 4 disadvantages of the biomedical model
Not all conditions can be cured
Reductionist- mechanistic, dualistic (doesn’t really consider anything outside the body)
Disease (not health) oriented (either healthy or ill, wellbeing not part of the vocabulary)
Patriarchal and capitalist (experts have all the power in decision making, often over-treatment)
According to the biomedical mode, what causes illness?
Diseases come from outside the body and invade it OR originate as internal involuntary physical changes
According to the biomedical model, who is responsible for illness?
Individuals not responsible for their illness, something that happens to us
According to the biomedical model, who should illness be treated?
Medical treatments e.g. vaccination, surgery, chemotherapy
According to the biomedical model, who is responsible for treatment?
Medical professionals
According to the biomedical model, what is the relationship between health and illness?
Seen as qualitatively different, no continuum between the two
According to the biomedical mode, what is the role of Psychology?
Illness may have psychological consequences but not causes
Give 3 examples of chronic diseases
Heart disease, cancer, diabetes
Give 4 key lifestyle risks for chronic disease
Tobacco use
Poor nutrition
Lack of physical activity
Excessive alcohol use
How does the biomedical model apply to chronic conditions?
Disease can no longer only be cured, it needs to be managed. Biomedical model is unsuccessful in addressing this management aspect
What does the biopsychosocial model (Engel, 1977) say about health?
More wholistic perspective of health, not solely caused by biology but interacts with our psychology and the social context in which we live. Treatment should also consider how to improve our social context
Give 4 examples of the ‘biology’ part of the biopsychosocial model
Genetic vulnerability
Immune function
Neurochemistry
Medication effects
Give 4 examples of the ‘psychology’ part of the biopsychosocial model
Attitudes/belief
Personality
Coping skills
Emotions
Give 4 examples of the ‘social’ part of the biopsychosocial model
Social support
Family background
Cultural traditions
Socioeconomic status
According to the biopsychosocial model, what causes illness?
A combination of biological, psychological and social factors
According to the biopsychosocial model, who is responsible for illness?
Individual behaviours seen as one of many causes, we have the power to influence our health and can have an active role in managing our health
According to the biopsychosocial model, how should illness be treated?
Modifying the person as a whole, via many different means to address multi-causality
According to the biopsychosocial model, who is responsible for treatment?
Multiple professions, delivery of care is collaborative
According to the biopsychosocial model, what is the relationship between health and illness?
Continuum between health and illness, even if not ill we can be more healthy
According to the biopsychosocial model, what is the role of psychology?
Illness may have psychological causes and consequences, emotions, beliefs and behaviours influence health trajectories
What is WHO’s definition of health (1948)?
‘Health is a state of complete physical, mental and social wellbeing and not merely the absence of disease or infirmity’
What is health psychology?
Discipline of psychology being applied to promotion and maintenance of health, the prevent and treatment of illness, the identification of etiological and diagnostic correlates of health, illness and related dysfunctions, and the improvement of the health-care system and health policy formation
What is evidence-based practice?
Operating principle in health sciences- integration of the best research evidence with our clinical expertise and our patient’s unique values and circumstances
What falls under clinical expertise?
Ability to use clinical skills and past experience to rapidly identify each patient’s unique health state and diagnosis, their individual risks and benefits of potential interventions/exposures/diagnosis tests, or their personal values and expectations. Also non-specific therapeutic factors like warmth, therapeutic alliance etc.
What is patient centred care?
Medicine is moving towards being personalised and the weight of the patient’s role in health management is increasing
What falls under patient’s values and preferences?
Concerns and expectations that each patient brings to a clinical encounter and that must be integrated into shared clinical decisions if they are to serve the patient
What falls under patient’s circumstances?
The patient’s clinical state and the clinical setting where they are
What falls under best available research evidence?
Qualitative- describe populations, observational- find relationships, and experimental- cause and effect
Very interested in the causal relationship between treatments and outcomes, focus on RCTs
Research is shifting to not only focus on RCT’s but also things like…?
More qualitative interviews about experience, could help explain why a treatment didn’t work/worked in a different way than expected
Describe the process of clinical decision making (diagram)
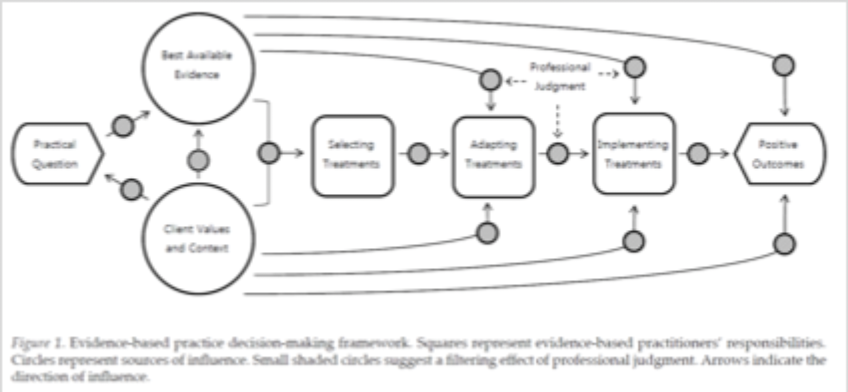
What are the desired outcomes of this clinical decision making?
Improve the results of decisions, increase the use of practices leading to desired outcomes, eliminate dysfunctional practices
Why does all of this matter? (8 reasons)
Quality (want to know what has the highest quality)
Accountability (if not using the evidence or using it wrong, can be held accountable)
Healthcare management
Policy influence
Growth of evidence base
Common language for transdisciplinary collaboration
Production of meta-synthesis (putting together lots of data, increases confidence in findings)
Tool for lifelong learning
What is the response to the critique that EBP is one-size-fits all approach to practice decisions?
EBP involves substantial adaptation of evidence to fit with local conditions and practitioner judgement
What is the response to the critique that EBP stifles innovation?
EBP helps diffuse new practices that may otherwise have spread more slowly and has lead to new forms of research to provide more useable evidence to practitioners (could argue that without it treatments that don’t work will stay around for longer)
What is the response to the critique that EBP relies solely or primarily on RCTs?
Reviews and evidence synthesis incorporate the diverse array of studies relevant to practice questions
What is the response to the critique that EBP relies heavily on human judgement, which may create biases or conflicts of interest?
EBP integrates quality control procedures, such as transparency in reporting or disclosure requirements
What is the response to the critique that EB guidelines can end up undermining EBP, if based on how quality, not subjected to regular updates etc.?
Transparency in methods, use of qualifiers in recommendations e.g. could be useful, strongly recommend
Briefly describe what happened with NICEs ME guidelines
Graded exercise therapy (GET) for chronic fatigue, progressively increase amount of activity you do in your day. Had to go back and re-examine the evidence, research base had a lot of limitations- recommendations not that strongly supported by evidence and didn’t meet patient preferences (patient voice should have come into play much earlier)
What did Luebbe et al. (2007) find in terms of clinical psychologist students perceptions of EBP?
1,195 students enrolled in Clinical Psychology programs, USA
When looking at how psychology students make decisions, they found evidence based was actually quite low in the hierarchy
What is the scientists-practitioner model (APA, 1947)?
Training of psychologists must put equal emphasis on research and practice. Psychologists must be able to apply available scientific knowledge and inquiry into practice
What falls under best available research evidence (competences of the scientist-practitioner psychologist)?
Adopt a scientific view of psychology
Knowledge of research design and methods
Strategies for accessing best available research
Ability to critically appraise the evidence
What falls under clinical expertise (competences of the scientist-practitioner psychologist)?
Understand role and limits of clinical judgement
Skills in relationship building
Assessment and diagnosis skills
Skills to implement empirically supported treatments (EST)
Integration of EST with client characteristics
What falls under patient values and needs (competences of the scientist-practitioner psychologist)?
Healthcare delivery as collaborative endeavour
Knowledge of diverse groups
Ability to ascertain patient values and preferences
Respond effectively to patient preferences and values
Give 4 critiques of the scientist-practitioner model
Difficulties of translating the medical model to psychology
Unclear what is the right balance between the 3 skills set in the model
Not all therapists need to be scientist-practitioners, especially if they are applying well established treatments
Practical difficulties of implementing the model (time sharing, access to resources, access to funding etc.)