Cardio: congenital defects, heart failure, pericarditis+ effusion, mitral valve disease, murmurs, DCM
1/195
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
196 Terms
what differences would you see PM on patient euthanised with intracardiac injection?
crystalline deposits on endocardium
acute hemopericardium
abnormal blood texture
myocardial pallor (chemical burn)
what is in the pericardial space and what is its function
lubricate layers of the heart during movement
the cardiac myocytes exist within _______ in the myocardium
fibrous connective tissue scaffold
left ventricle is ____x thicker than right ventricle
why is this?
3x thicker
because left ventricle sends blood to systemic circulation, which has increased volume and increased total resistance to blood flow relative to pulmonary circulation. so L ventricle has to work harder to send out blood
why are cardiac myocytes more susceptible to hypoxia / anoxia than skeletal myocytes?
they rely on aerobic glycolysis and have continuous activity
explain what happens when myocardial cells die
they are non-regenerative, so myocardial death results in fibrosis as there are no new cells to replace them
what is the impact of fibrosis on the heart
fibrosis to one part of the heart can effect the entire heart function due to synergy of the heart
what part of the endocardium looks different than the other parts?
the endocardium covering atria is thicker and whiter and more opaque than the endocardium than in ventricles
what would you look for in the pericardium on PM
thickening
adhesions between pericardium and other tissues (look at lung, mediastinum, thoracic wall)
adhesions between pericardium and epicardium
free fluid in pericardial sac
what would you look for in the myocardium on PM
size, weight, outline, color
expose all chambers, valves, great vessels
look at endothelium of great vessels- plaques? endarteritis?
measure R:L ventricular wall ratios (should be 1:3)
common appearances of heart on PM
R. ventricle can be flabby after death- do not mistake for DCM or dilation!
don't confuse PM blood clots with thrombi (clots wash away, thrombi stick to vessels)
in horses, chickenfat clots are common PM
the endocardium might be stained dark red due to haemoglobin imbibition- not pathological
pericardial fat may be seen in obese patients
serous atrophy of cardiac fat is seen in starved patients
clear, gelatinous fluid is common in epicardium
what is the AV ring?
segregation of atria and ventricles by fibrous ring
allows for synchronised cardiac conduction
only way to bypass the ring is through the AV node
how many bundle branches on right and left ventricles
one on right
two on left
what is function of bundle branches
rapidly conducting system
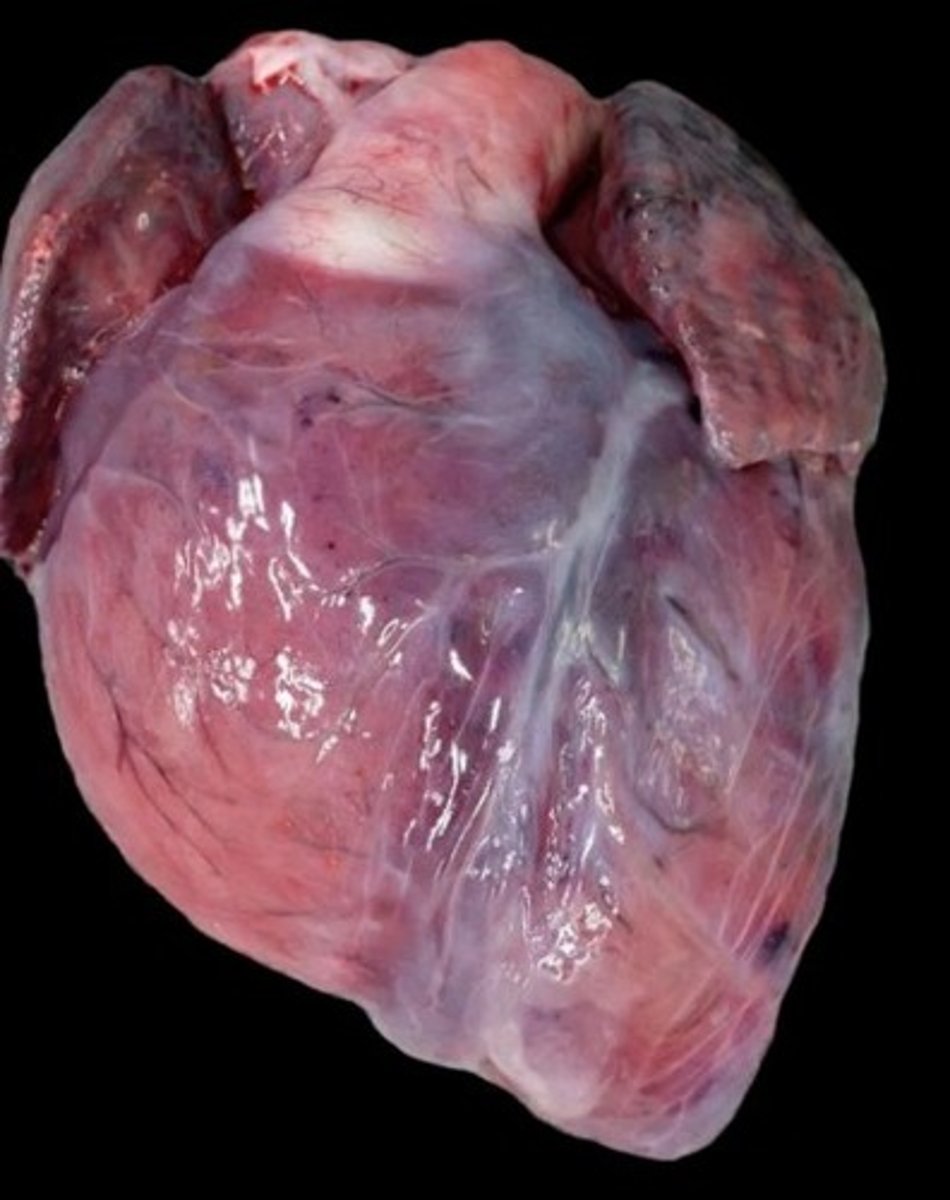
chicken fat clot in a horse (non-pathological, common PM finding in horses)
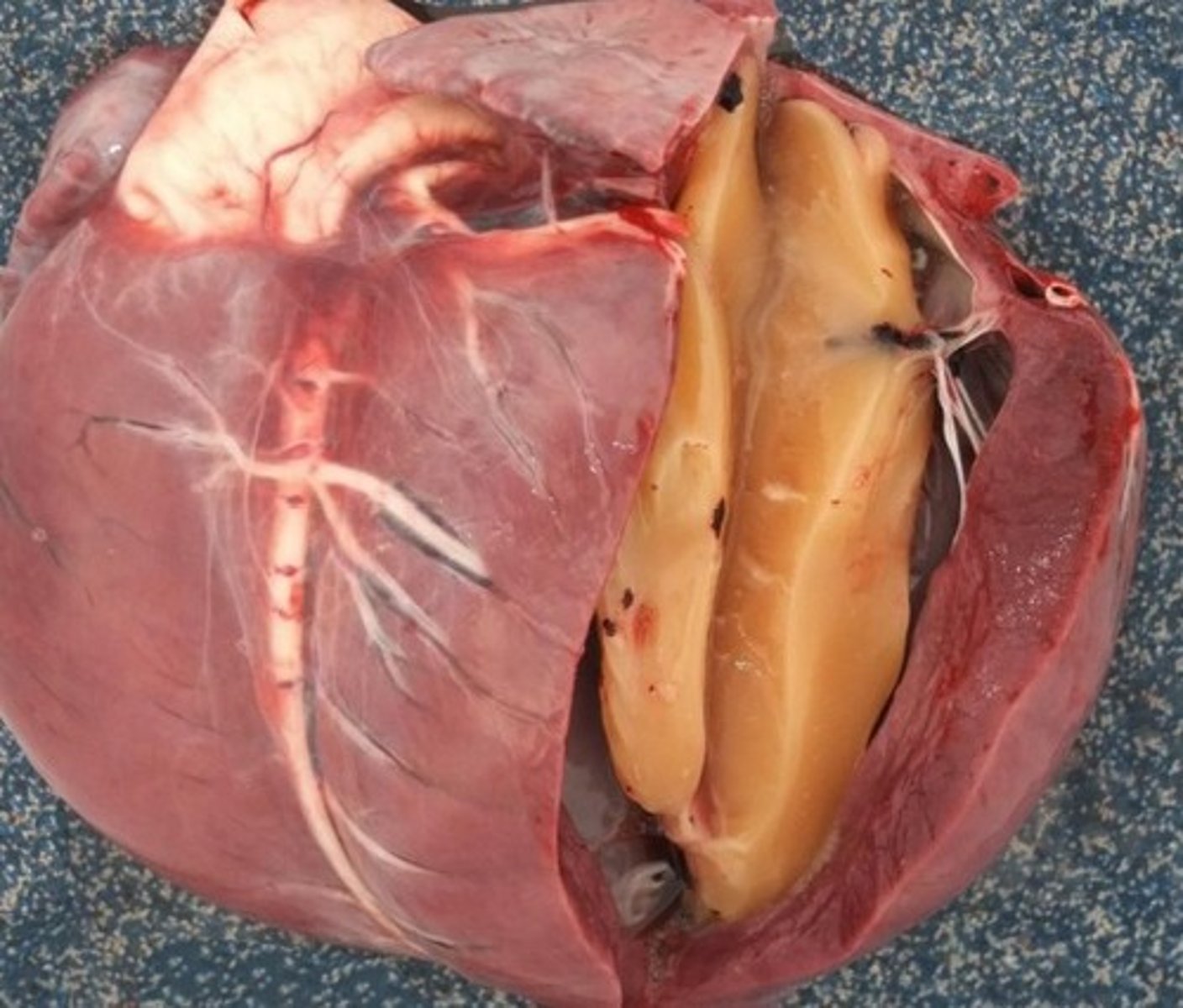
serous atrophy of cardiac fat. seen with starvation
dog euthanised by intra-cardiac barbituates, chemical burn of right ventricle
all congenital defects (talked about in this course) will result in a ________ due to turbulent / abnormal blood flow
heart murmur
in the fetus, the ____ side is the high pressure system
what happens to pulmonary vessel pressure?
right
at birth there is a drop in pulmonary vessel pressure as the lungs fill with air. this switches the high pressure system to the left side
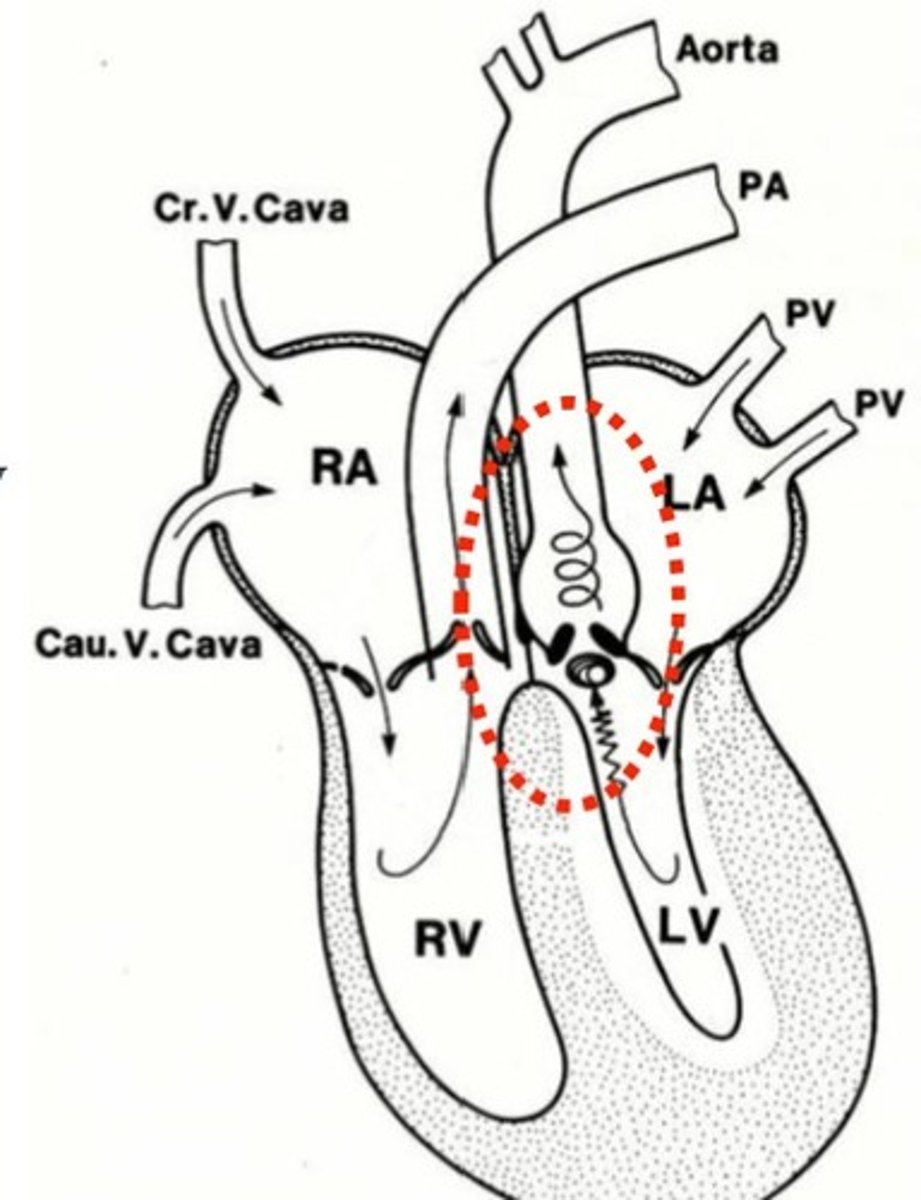
atrial septal defect (image)
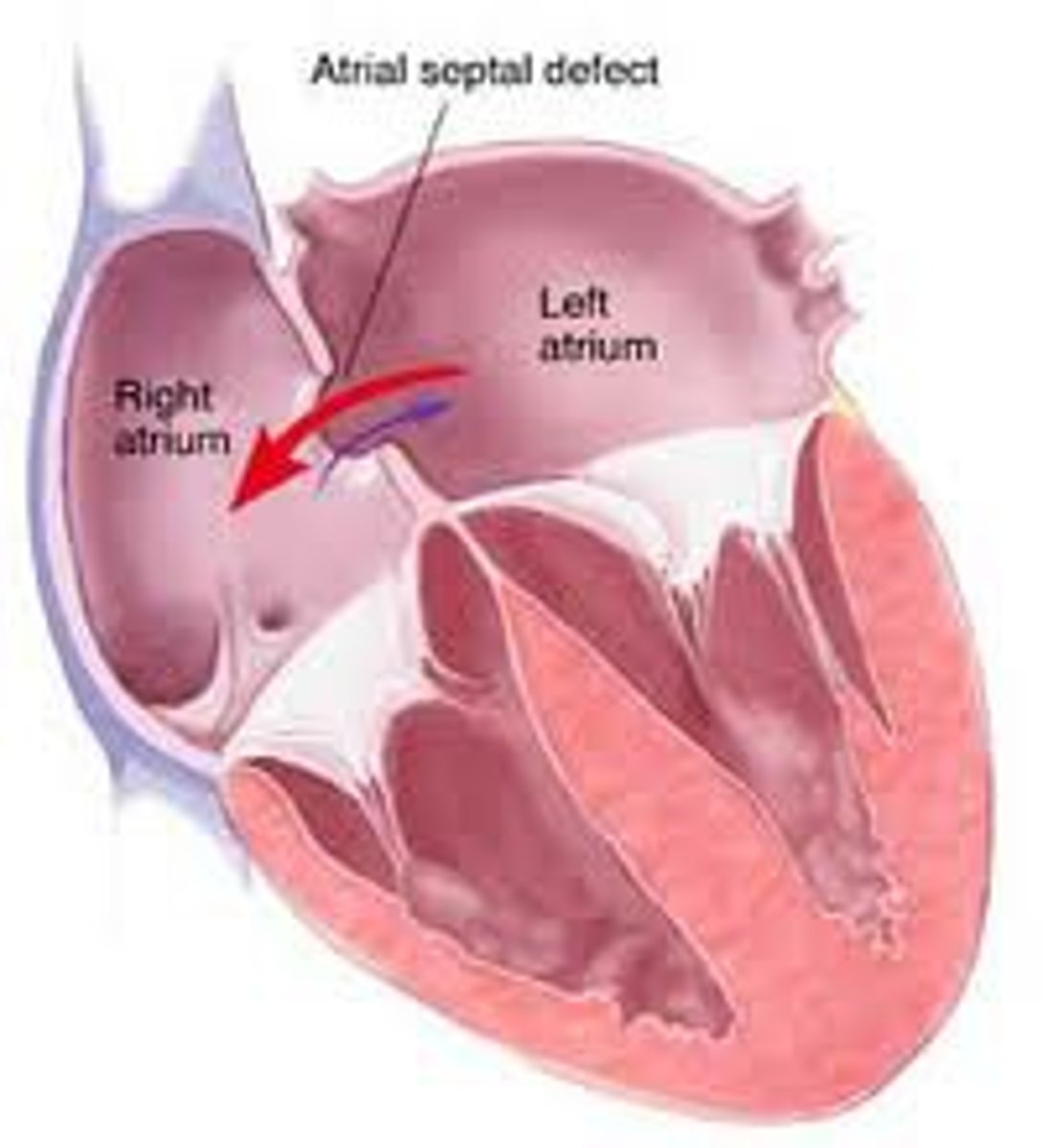
what determines the severity of atrial septal defect
the degree of failed closure of the septum
what is an atrial septal defect caused by
failure of the foramen ovale to close during fetal development
what type of shunt results from an atrial septal defect
left to right shunt
what causes the foramen ovale to close after birth (takes a few weeks)?
pressure switch (systemic circulation becomes the high pressure system at birth when lungs fill with air) pushes the septum primum over the foramen ovale, closing the hole
what are the long term consequences of an atrial septal defect?
right ventricle dilation and hypertrophy
dilation of both atria
audible murmur due to dilation of pulmonary artery
a severe / large shunt can result in secondary hypertension, fibrosis, increased pulmonary vascular pressure, and a right --> left second shunt --> cyanosis due to blood bypassing lungs
ventricular septal defect (image)
is ventricular septal defect common or rare in small animal?
one of the most common congenital abnormalities
is the ventricular septal defect more often cranial or caudal
cranial
what type of shunt results from a ventricular septal defect?
left to right shunt
what are the long term effects of ventricular septal defect?
small defect: can live normal life, asymptomatic
larger defect:
hypertrophy of both ventricles
secondary hypertension and fibrosis
LV overload ---> CHF
a right to left shunt, resulting in cyanosis
in a VSD, the intensity of a murmur is _______ to severity of the defect
inversely proportional
patent ductus arteriosus (image)
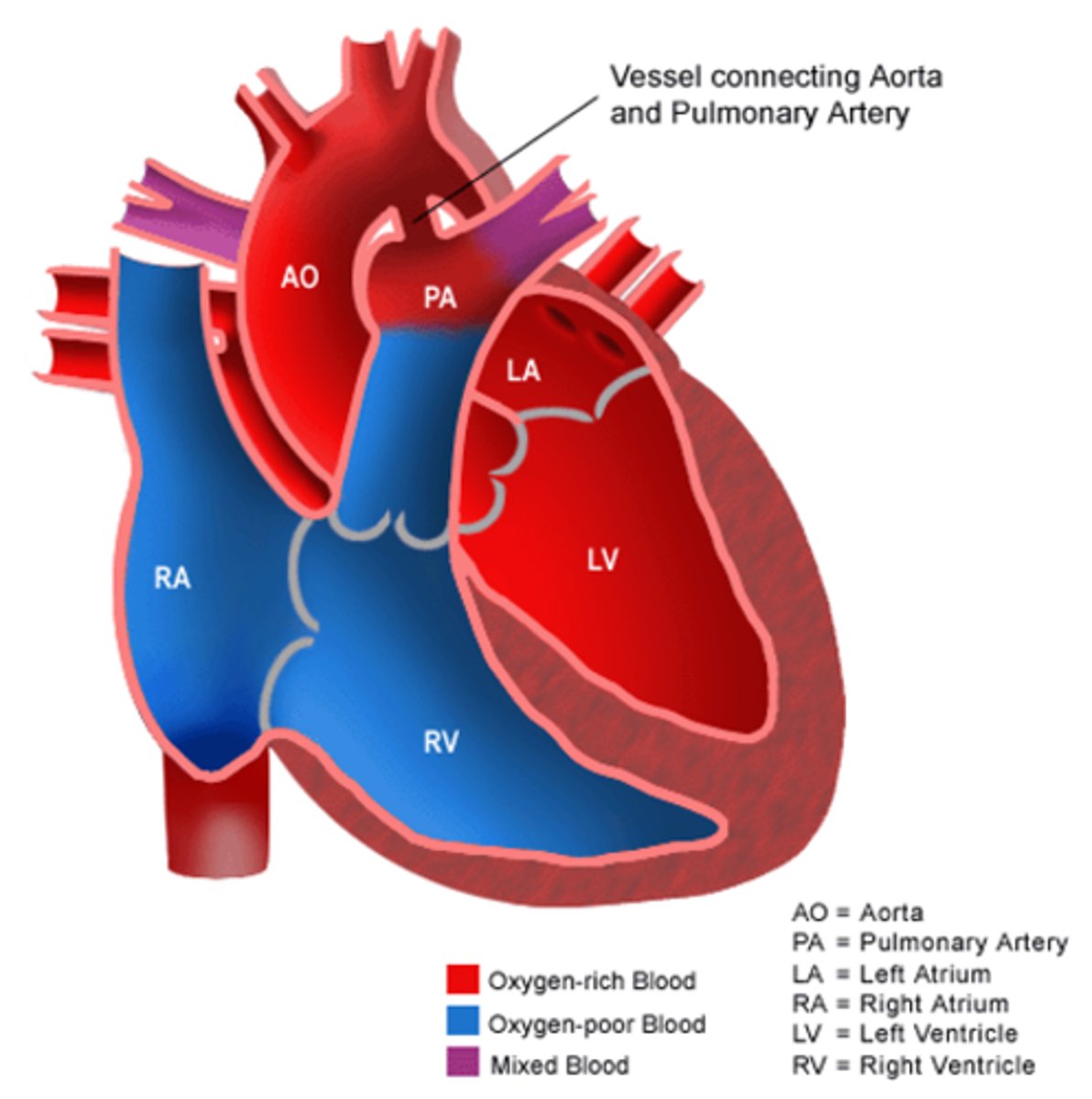
what is the ductus arteriosus and does it close?
vascular channel connecting fetal pulmonary artery to aorta
does not close in gestation. At birth, when L heart becomes high pressure system, the flow through the ductus arteriosus is prevented. It gradually fibroses, forming the ligamentum arteriosum
what causes the patent ductus arteriosus?
failure of formation of ligamentum arteriosum
what type of shunt results from PDA?
left to right shunt (aorta --> pulmonary artery)
what long term effects result from PDA?
secondary pulmonary hypertension
hypertrophy of LV
LV and LA dilation
predisposition from thromboses due to turbulent blood flow
what does PDA look similar to on an echo?
DCM
triple knuckle x-ray bulge
what happens if you don't correct a PDA?
animal will die in a year. Curative surgery is the treatment
what does PDA sound like on auscultation?
pathognomonic murmur, but requires echo to definitively diagnose
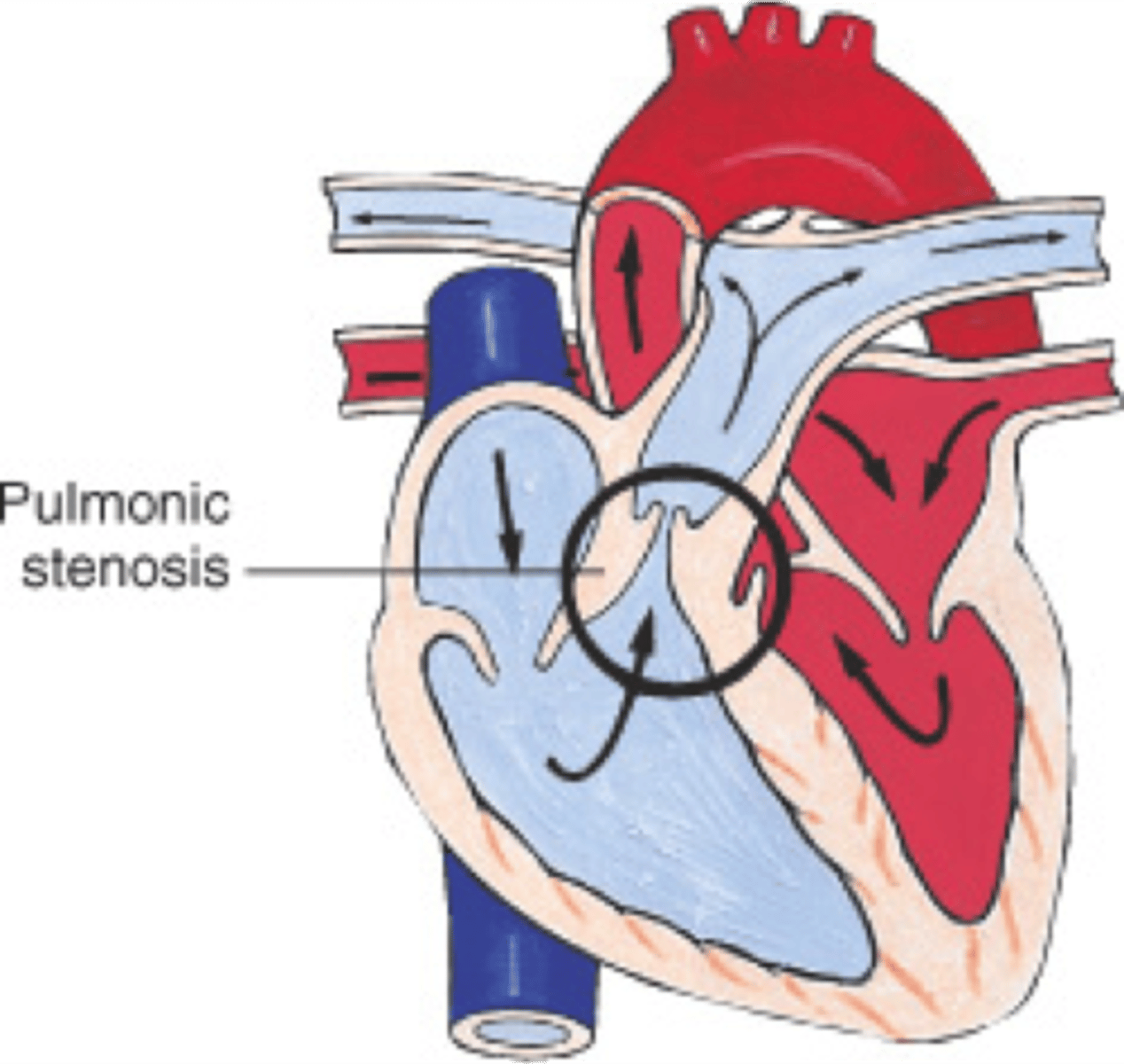
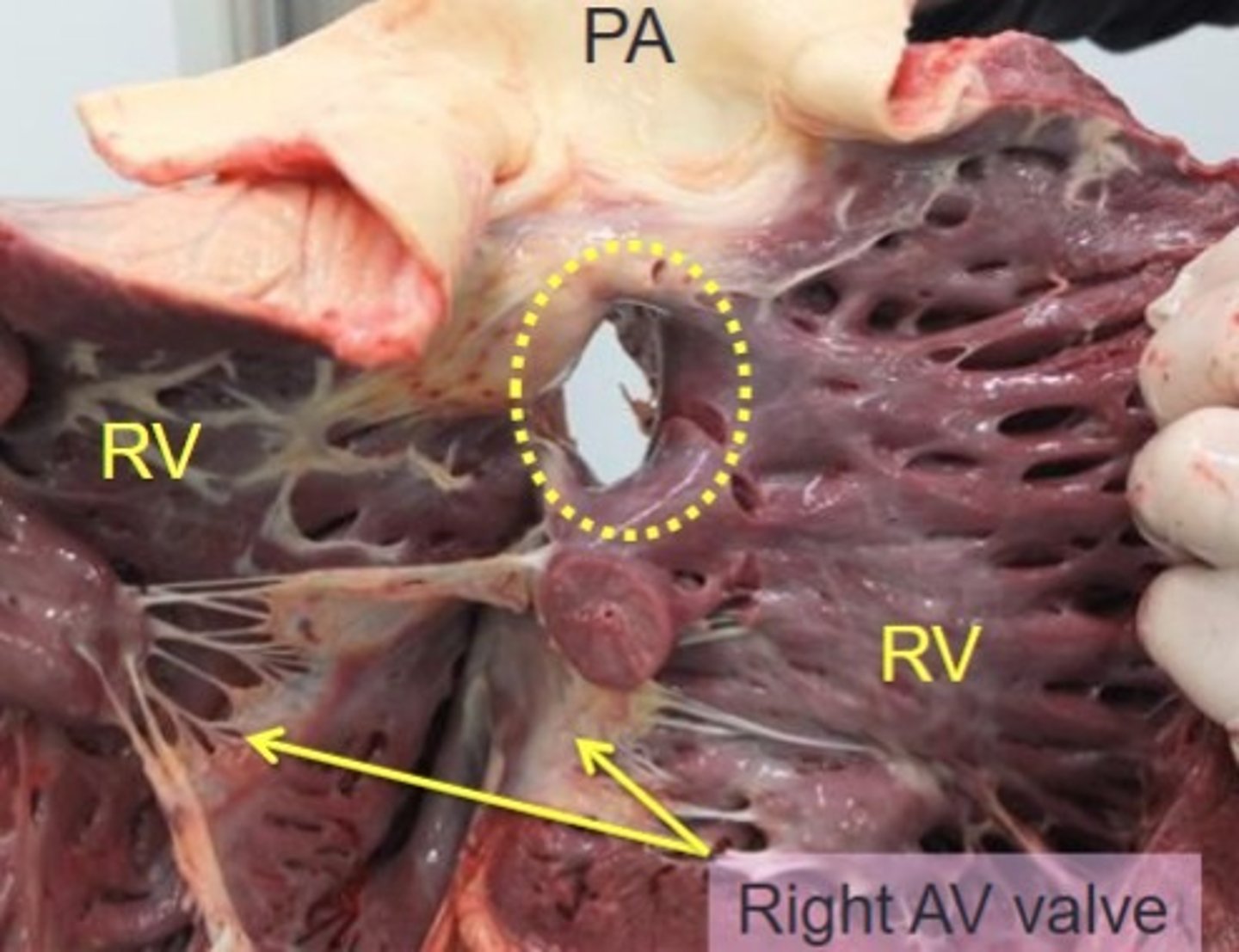
pulmonic stenosis (image)
what is the most common congenital heart disease in dogs?
pulmonic stenosis
what is pulmonic stenosis?
narrowing of the outflow of the pulmonary artery
what is the most common site of pulmonic stenosis?
narrowing is usually at the level of the valve, resulting in valvular stenosis (fusion)
what are long term effects of pulmonic stenosis?
hypertrophy of the right ventricle (narrowed pulmonary artery, RV pressure overload)
dilation of the pulmonary artery just outside the steonisis
mild stenosis can live normal life
even in severe stenosis, patients are often asymptomatic
occasionally you see exercise intolerance, syncope, RSHF
poor prognosis if the patient is a Frenchie
how do you determine the severity of pulmonic stenosis?
based on echo- the pressure difference across the lesion
also the murmur intensity is proportional to the disease severity
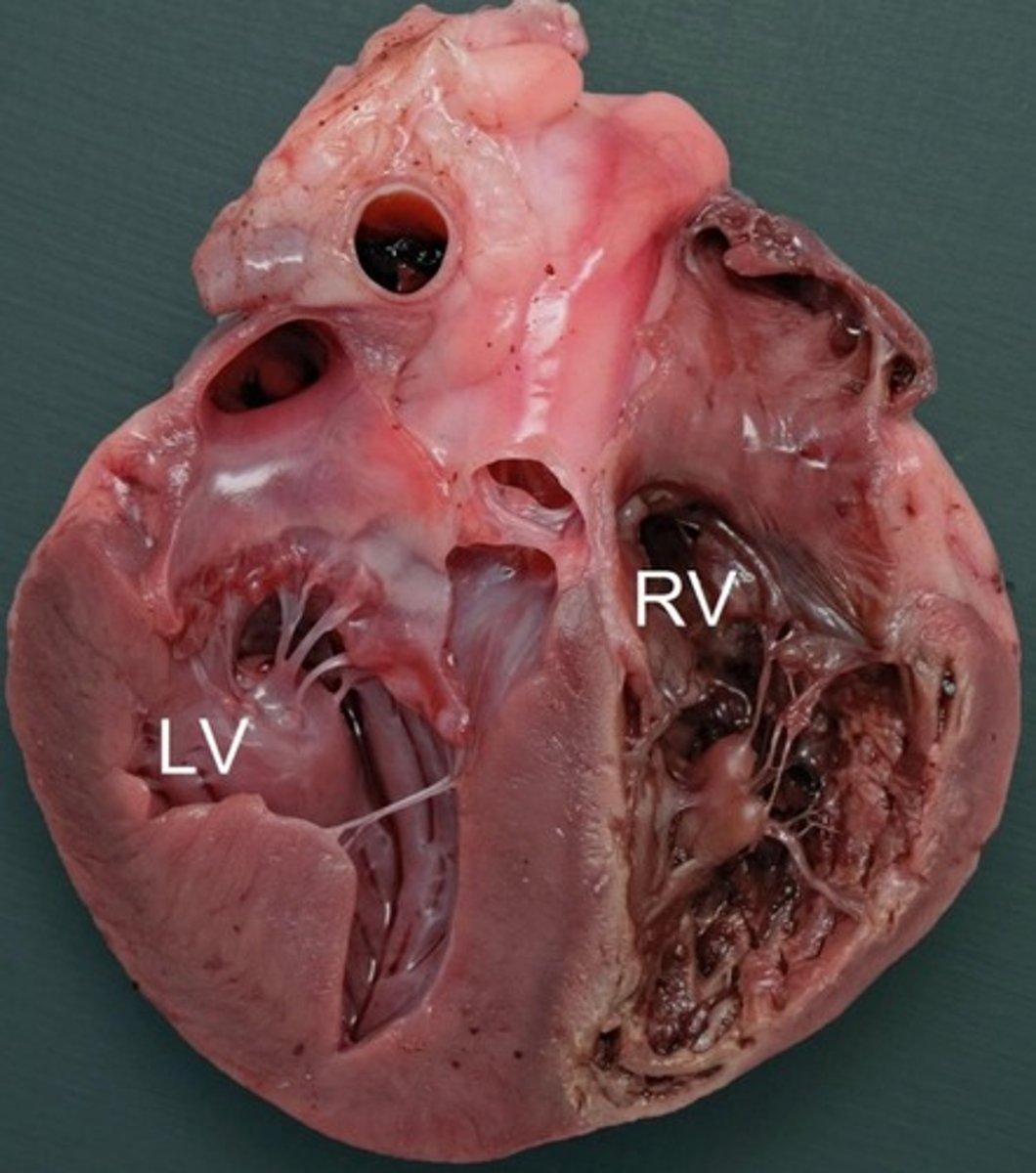
image PM of a VSD
in pulmonic stenosis, the murmur intensity is _______ to the disease severity
proportional
image PM of ASD
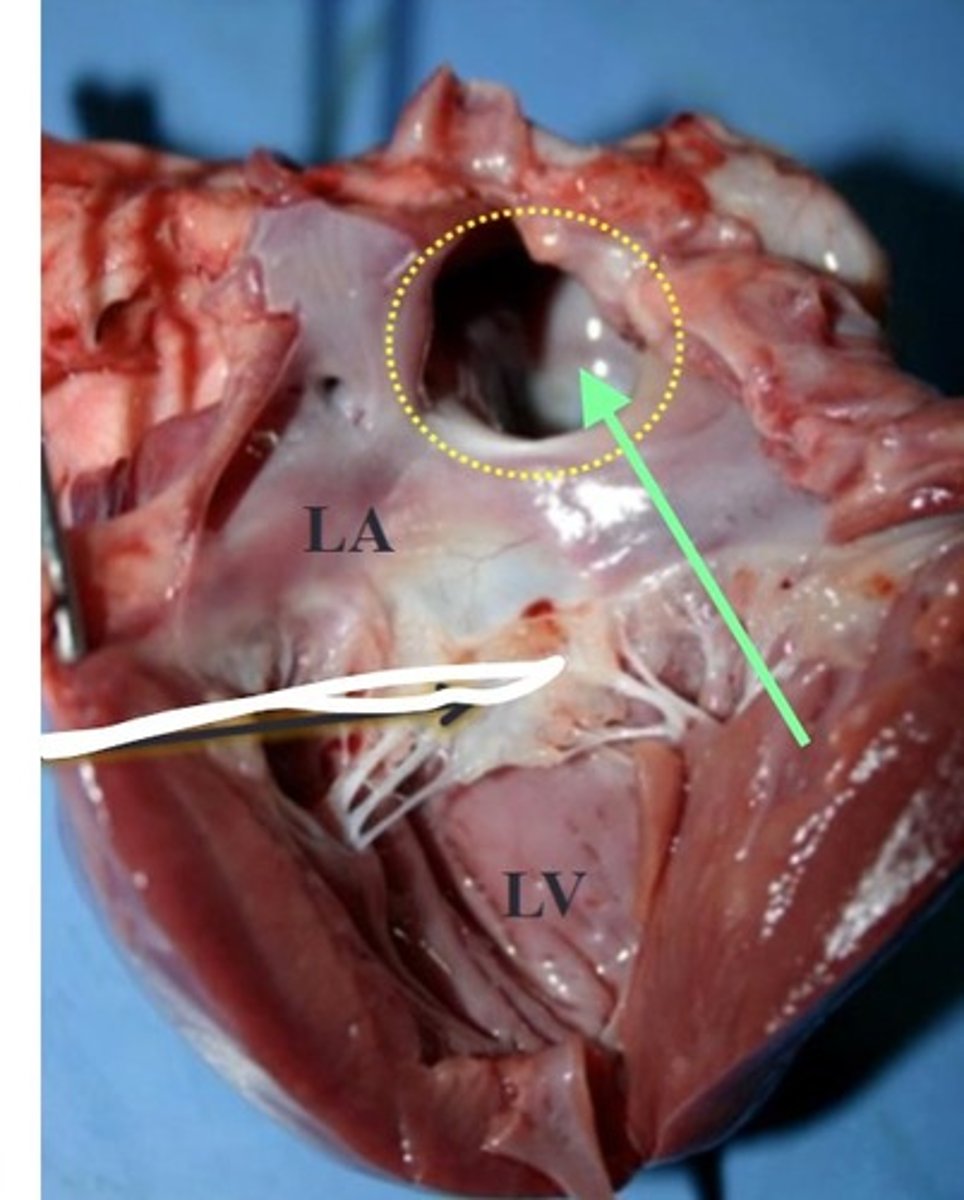
image PM of PDA
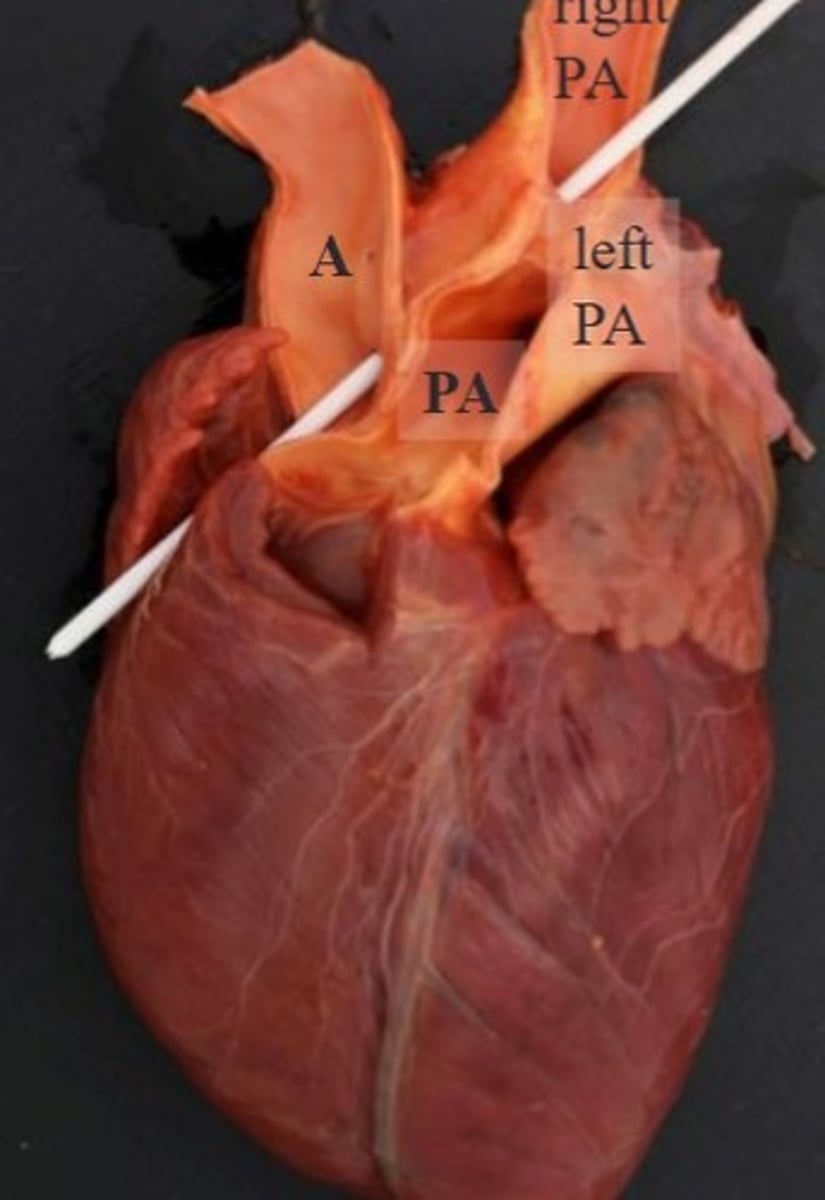
image PM of subaortic stenosis
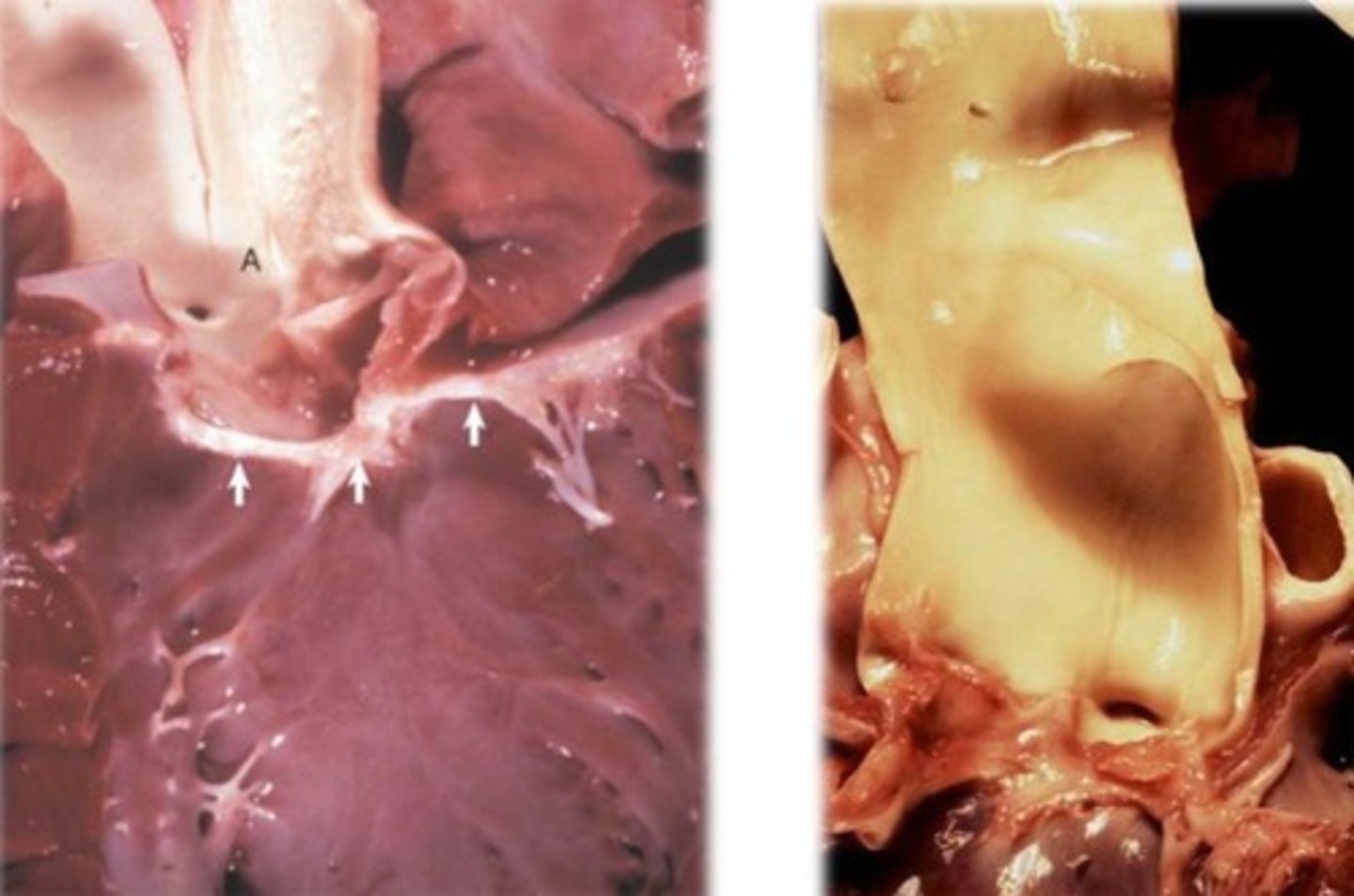
subaortic stenosis (image)
what is a subaortic stenosis?
narrowing of the outflow of the aorta at or just below the aortic valves
what species is subaortic stenosis more common in?
pigs and dogs
what are long term effects of subaortic / aortic stenosis?
LVOT obstruction --> pressure loaded LV --> LV hypertrophy
post-stenotic dilation of the aorta
fibrosis and thickening of walls of arteries within myocardium --> reduced blood flow within the heart itself --> focal areas of myocardial necrosis
what does a murmur from subaortic/aortic stenosis sound like?
similar to pulmonic stenosis murmur: left basilar systolic
requires an echo
in subaortic/aortic stenosis, the murmur grade is _____ to disease severity
proportional
what is the prognosis of subaortic / aortic stenosis?
mild: asymptomatic
severe: exertional syncopy --> collapse, sudden death with exercise
which carries a worse prognosis- pulmonary stenosis or aortic/subaortic stenosis?
aortic/subaortic stenosis
which valve dysplasia is more common in cats?
left AV dysplasia
what are different ways that mitral and tricuspid/AV valve dysplasias present?
focal or diffuse thickening of leaflets
fusion of valves with cardiac wall
shortening of cordae tendinae
shortening of papillary muscles
what are long term results of mitral and tricuspid/AV valve dysplasias?
imcompetent / leaky valves
dilation of atria
secondary dilation of ventricle of the affected side
what is valve dysplasia not to be confused with?
endocarditis
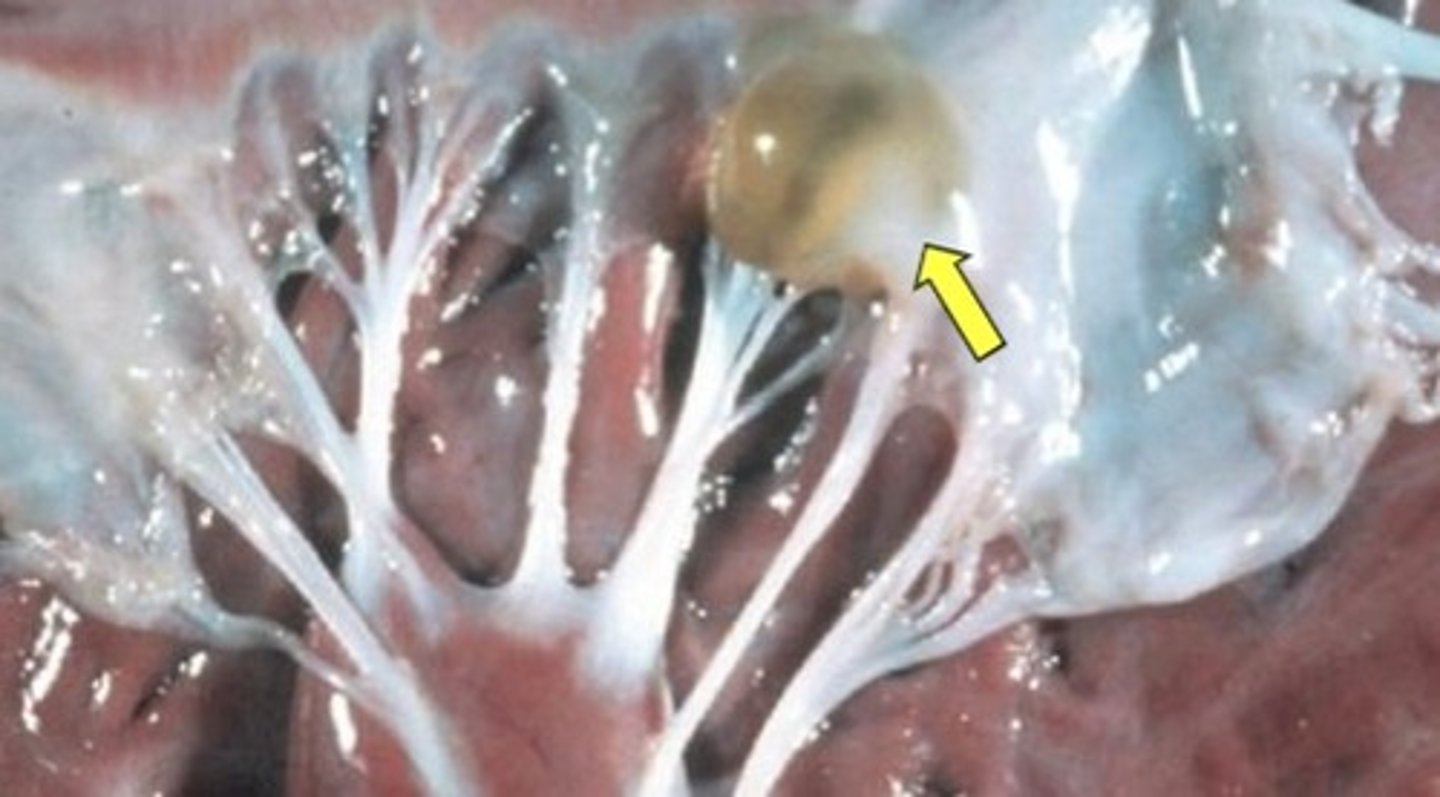
image of valvular hematocyst

where do you commonly see valvular hematocysts and lymphocysts?
on the AV valves of young ruminants (found incidentally)
what is the clinical significance of valvular hematocysts and lymphocysts?
don't cause functional issues
may regress spontaneously
image of valvular lymphocyst
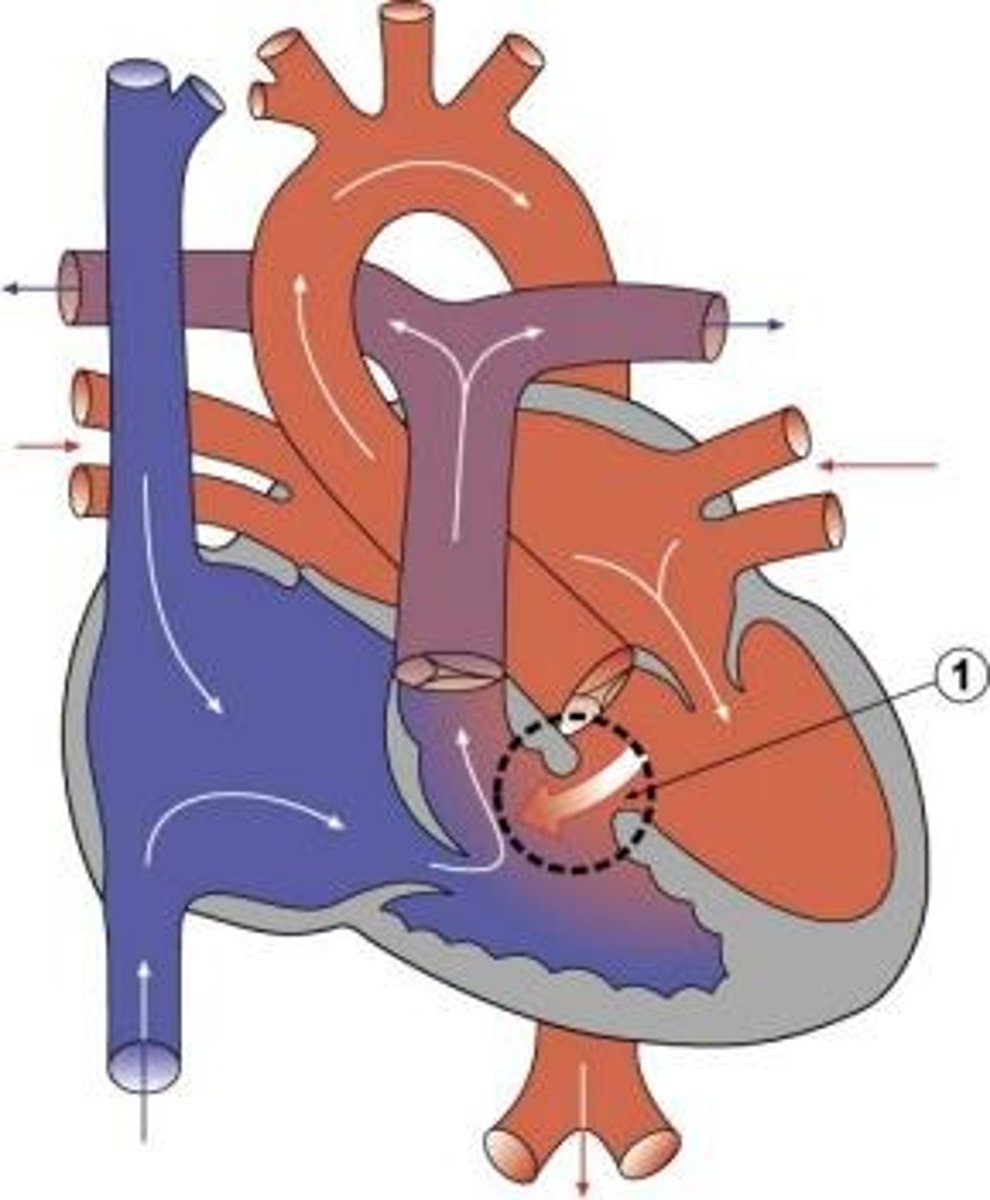
what are the 4 degrees of transposition of the aorta and pulmonary artery? which ones are compatible with life?
1. overriding aorta
2. partial transposition
3. overriding pulmonary aorta
4. complete transposition
only #1 is compatible with life because aorta receives blood from both ventricles
image of transposition of aorta and pulmonary artery
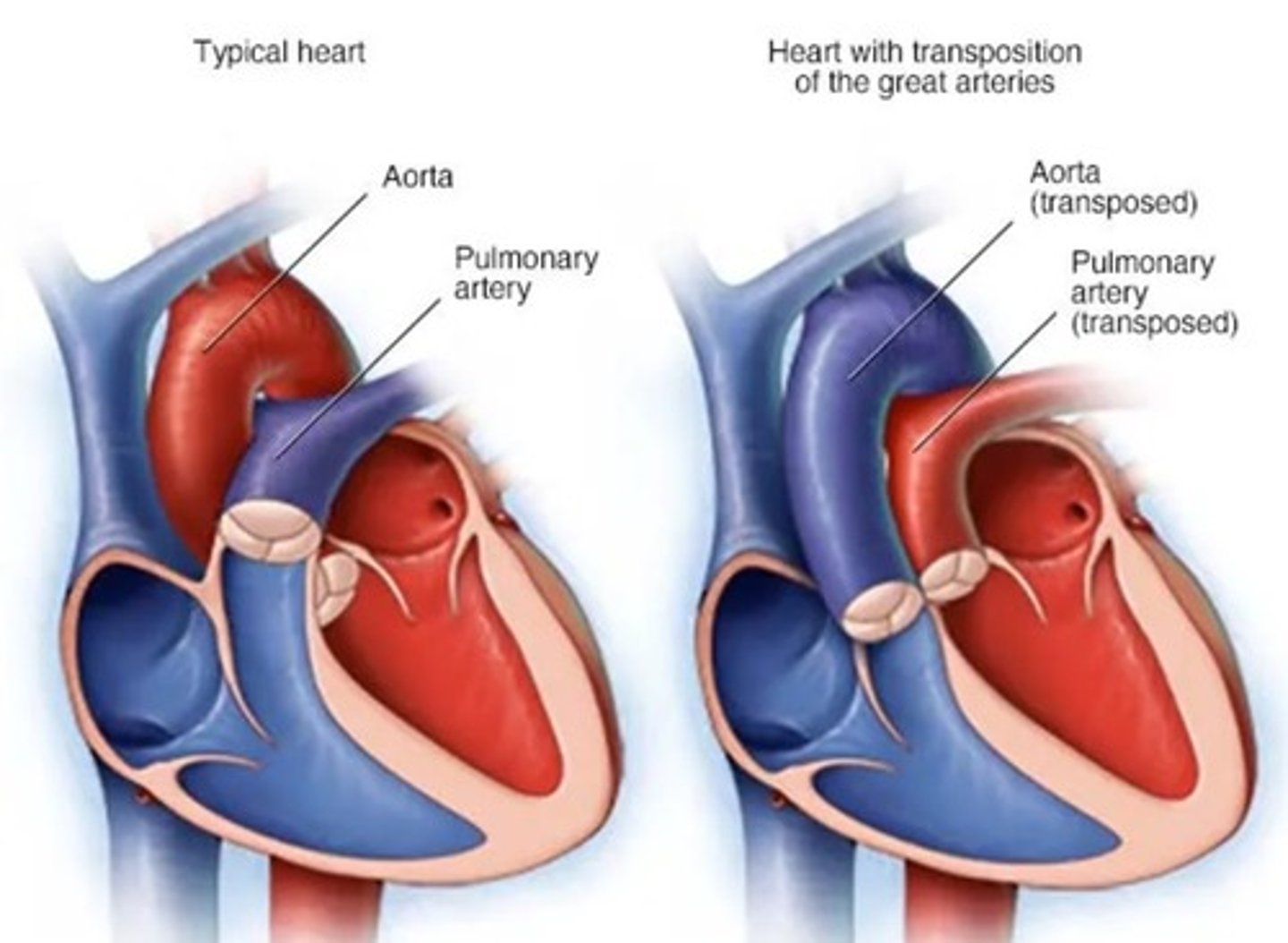
image of persistent right aortic arch (aka vascular ring anomaly)
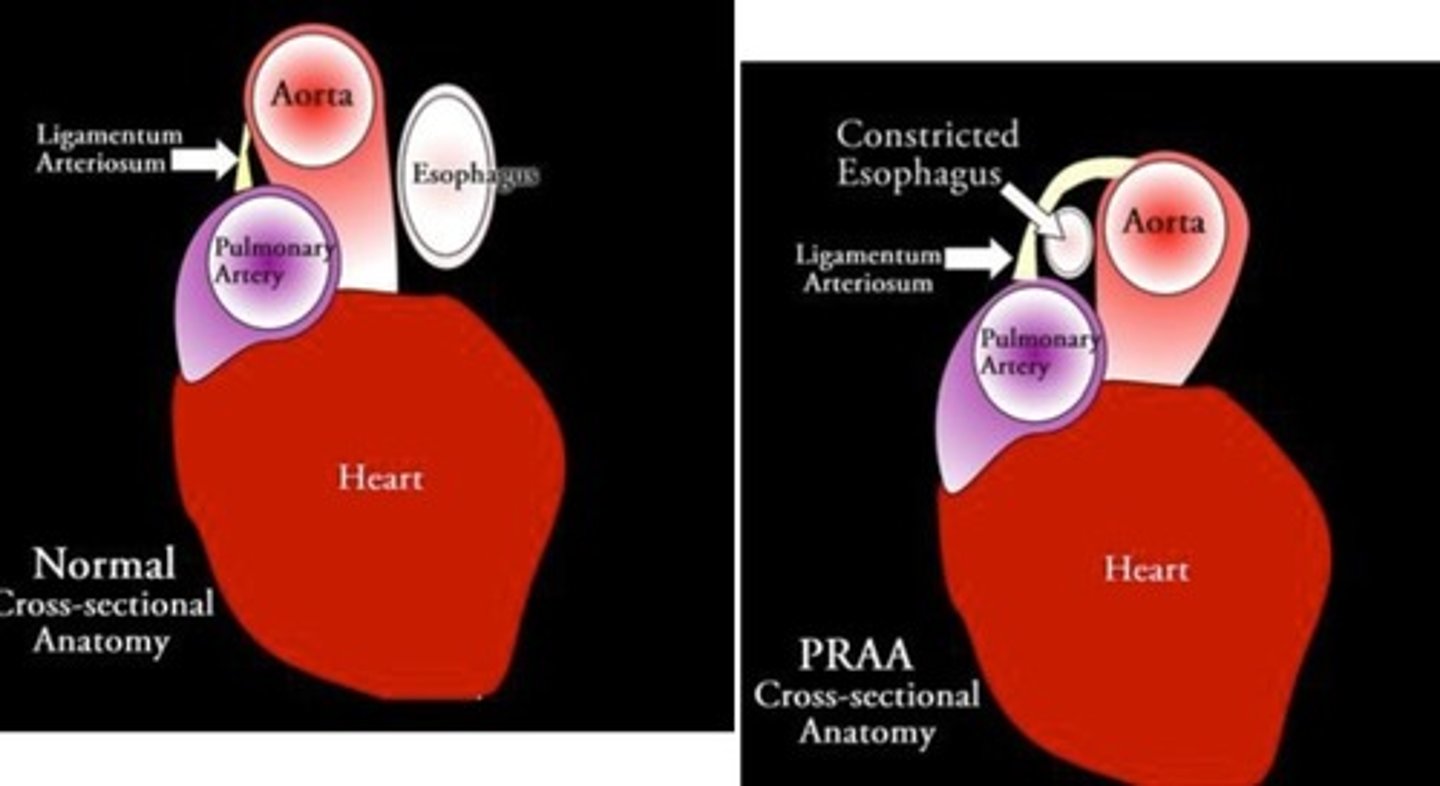
what is a vascular ring anomaly?
when the ductus arteriosus entraps the esophagus against the trachea
when would you see a vascular ring anomaly clinical signs?
when the animal switches from milk to solid food, resulting in obstruction of the esophagus
clinical signs of vascular ring anomaly
dysphagia
regurgitation
megaoesophagus
image of tetralogy of fallot
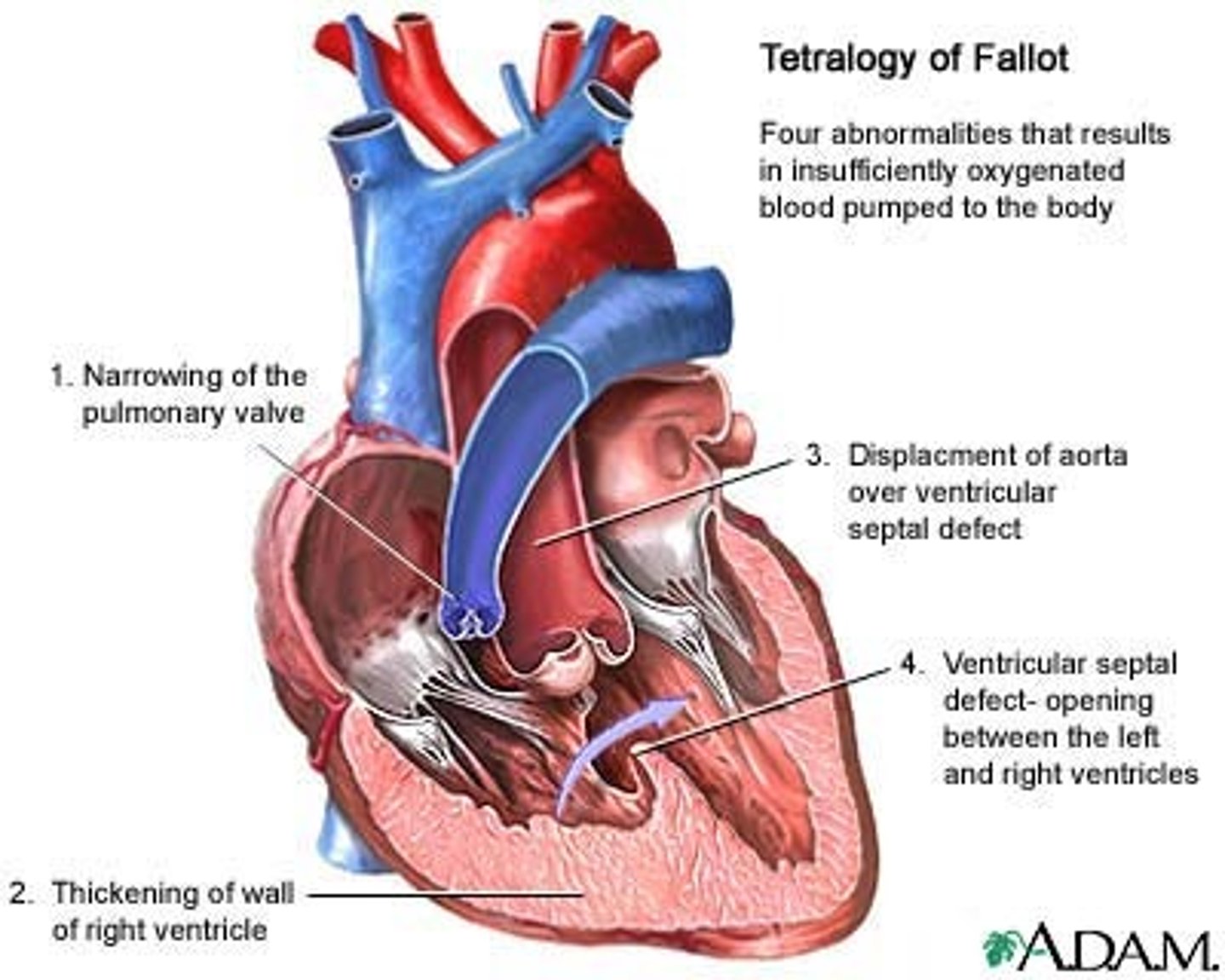
what are the 4 features in tetralogy of fallot?
1. VSD
2. Pulmonary stenosis
3. secondary RV hypertrophy
4. Overriding aorta (aortic transposition)
will you see clinical signs of tetralogy of fallot?
always:
retarded growth rate
heart failure (due to RVH --> DCM)
cyanosis due to poor pulmonary perfusion
polycythemia (compensatory for hypoxia)
what are the 3 possible causes of heart failure?
1. lack of circulating fluid due to loss of blood or plasma (ex massive hemorrhage, dehydration)
2. failure of the blood vessels to maintain good tone, resulting in decreased blood pressure
3. heart damage resulting in insufficient blood flow
what is the definition of heart failure
when the heart is unable to pump blood at a rate sufficient to meet the oxygen demands of the body
what are the two subtypes of left sided CHF and what causes them?
systolic HF: caused by decreased contractility
diastolic HF: caused by increased afterload
what happens in systolic left CHF
left ventricle is dilated
left ventricle has decreased ejection
decreased CO due to low contractility
what happens in diastolic left CHF
left ventricle is hypertrophied, resulting in decreased ventricular filling
decreased cardiac output due to decreased preload
what two cell types respond to decreased CO?
baroreceptors
juxtaglomerular cells
what happens when the baroreceptors detect decreased CO?
they increase sympathetic activity (by increasing epi and norepi)
heart rate increases (beta receptors)
stroke volume increases (alpha receptors)
afterload increases as a result, worsening the heart failure by triggering hypertrophy
preload also increases as a result of baroreceptor response, causing dilation
what happens when the juxtaglomerular cells in the kidney detect decreased CO?
they increase production of renin, thus increasing aldosterone (which increases ADH, increasing reabsorption of sodium and water by the kidneys and resulting in fluid retention and oedema)
this is a compensatory response that overall increases stroke volume, increases afterload, and increases preload (further worsening the heart failure by causing hypertrophy and dilation)
what causes acute heart failure?
sudden big drop in blood flow that compensatory mechanisms can't cope with
what causes chronic (congestive) heart failure?
small drop in cardiac output that compensatory mechanisms can keep up with for a while, but as heart condition worsens decomposition occurs
clinical signs of acute heart failure
difficult to diagnose, difficult to see on PM
exercise intolerance
respiratory issues for a few hours or days before compensatory mechanisms fail
pale mucous membranes
cold extremities
oliguria (low urine output)
what are the compensatory mechanisms employed in chronic / congestive heart failure?
increased heart rate
increased force of contraction
increased peripheral vascular resistance
redistribution of blood away from non-vital organs
what is the reflex arteriolar constriction and when does it happen?
during acute heart failure, initiated by the baroreceptor triggering due to sudden drop in arterial BP
baroreceptors increase sympathetic tone
adrenaline released --> HR increased
reflex constriction of peripheral arterioles shunts the blood away from non-vital organs. Occurs in skin, GIT, kidneys
explain why acute heart failure results in dyspnoea?
left ventricle fails --> reduced ventricular output --> increased preload
pulmonary vascular congestion (exacerbated by the right ventricle still pumping to the lungs)
hydrostatic pressure in pulmonary capillaries increases, causing pulmonary oedema
pulmonary oedema is what causes clinical sign of dyspnoea
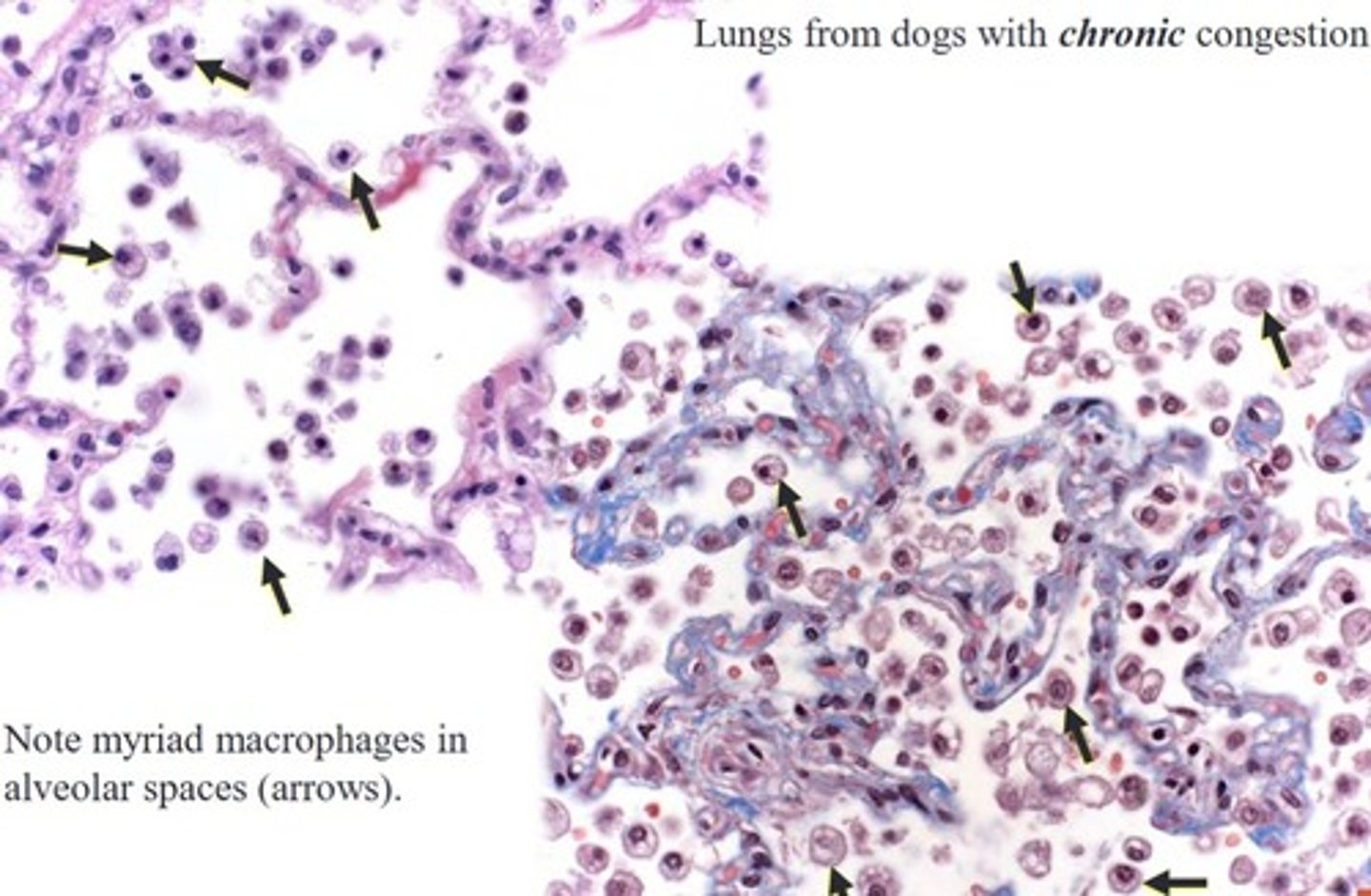
what does chronic left sided heart failure look like histologically in the lungs?
In addition to increased alveolar macrophages containing hemosiderin ----> heart failure cells
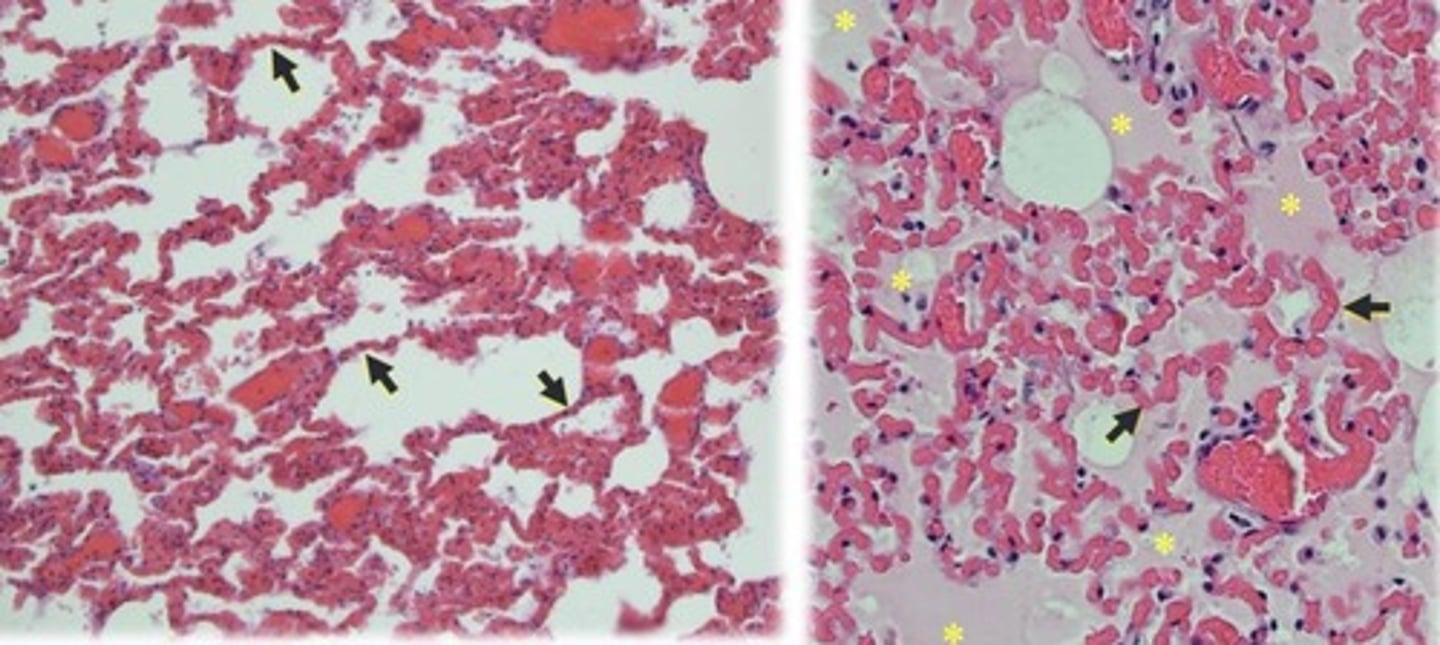
what does acute left sided heart failure look like histologically in the lungs?
Alveolar septae (arrows) are filled with blood. The alveolar spaces are filled with eosinophilic oedema fluid
how can chronic left sided heart failure affect the right side of the heart?
persistent increased pulmonary pressure can eventually result in interstitial lung fibrosis with subsequent right-sided heart
damage and failure (cor pulmonale)
more workload for the right side of the heart
what are some causes of left sided heart failure?
valve defects
myocarditis, pericarditis, endocarditis
cardiac tamponade
cardiomyopathies
systemic hypertension
infarction (uncommon in domestic animals)
how would right sided heart failure present differently from left sided heart failure?
left sided: lung oedema, dyspnea
right sided: liver congestion, ascites
how does right sided heart failure cause "damming back"?
reduced output to pulmonary circulation results in congestion of blood in the right atrium, vena cavae, systemic veins, liver, and spleen
why doesn't acute RSHF cause oedema despite congestion?
systemic veins can accomodate much more blood than pulmonary veins
what happens in acute RSHF? (response of body)
left side of heart is not receiving much blood because right side failed--> immediate drop in systemic arterial blood pressure --> peripheral arterial constriction reflex (mediated by adrenaline)
Heart rate increases
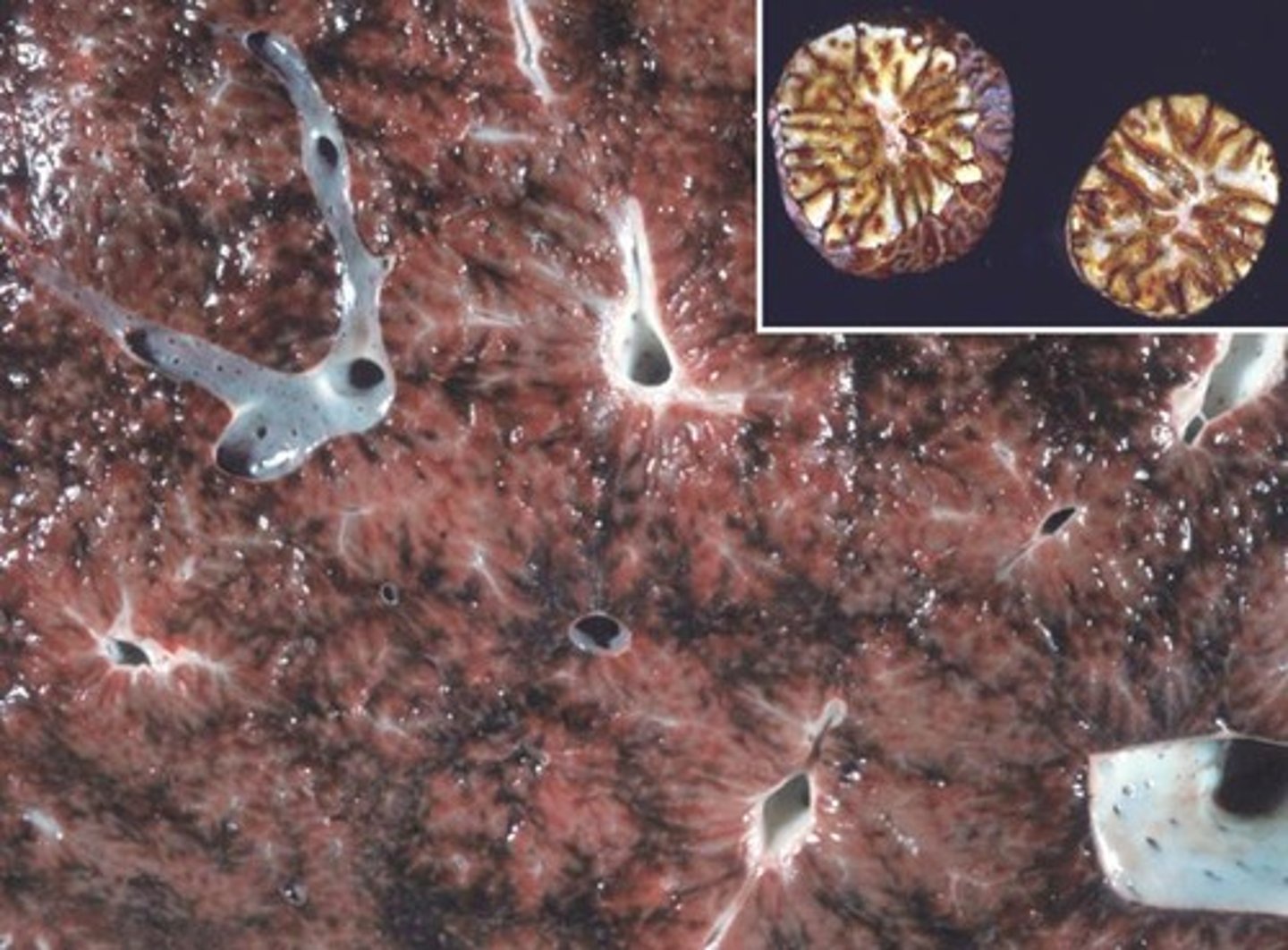
what pathological effects are seen with chronic RSHF?
prolonged damming of blood back in the liver --> liver oedema
hepatocellular hypoxia, necrosis, and fibrosis in the liver
results in the "nutmeg liver"
what are some causes of RSHF?
pulmonary disease
valvular disease and defects
myocarditis, endocarditis
cardiomyopathies
secondary to LSHF
what can cause biventricular failure?
myocarditis, myocardia toxins, acute cardiac tamponade