Brain Disorder Unit 2 Study Guide Key Terms
1/72
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
73 Terms
X-ray
2D structural image created by differential radiation absorption. Useful for imaging skull fractures and foreign objects
CT Scan
Computed tomography - acquires series of 2D X-ray images to create 3D image. Best for quickly viewing skull fractures, stroke, bleeding, and brain swelling
MRI - T1
Structural MRI where gray matter is darker than white matter (and water appears dark). This is the more 'normal' brain image. Good for examining detailed anatomical structures (and tumors with contrast dye)
MRI - T2
Structural MRI where water appears bright and white matter is darker than gray matter. This is also called a 'diffusion-weighted' image, as it is measuring fluid content/motion in the tissues. Good for viewing brain swelling, stroke, bleeding, MS lesions (loss of myelin = increased CSF), and infection (swelling from immune system)
DTI
Diffusion Tensor Imaging - MRI technique that images white matter tracts and connectivity by a computer analyzing many diffusion-weighted scans to track water/fluid movement along major axon bundles
EEG
Electroencephalogram - functional measurement that records electrical activity of the brain using scalp electrodes. Temporal resolution is similar to neural activity timing, but spatial resolution is not so good. Useful for seizures, arousal level, and brain death
ECoG
Electrocorticography - functional measurement that uses invasive recording of electrical activity directly from brain surface. Better spatial resolution than EEG as the electrical activity does not have to travel first through the meninges, skull, and scalp
PET scan
Positron Emission Tomography - functional measurement that measures brain metabolism using radioactive tracers. Good for dementia, stroke, and tumors
fMRI
Functional MRI - measures blood oxygenation changes (BOLD signal) to detect when neurons are active. This is a very good but indirect measure of neural activity. Excellent for cognitive disorders and research
Visual Field
The entire area that can be seen when an eye is fixed straight at a point in space
Vertical Meridian
Line dividing field into left/right halves
Horizontal Meridian
Line dividing field into top/bottom halves
Hemifield
Half the visual field (typically left/right)
Quarterfield
One quadrant of the visual field
Optic Nerve - visual pathway
Axons of retinal ganglion cells
carrying visual information from eye to the optic chiasm
axons continue on as the optic tract to synapse in the lateral geniculate nucleus of the thalamus on vision's path to the brain
Optic Chiasm - visual pathway
Where nasal (inner) fibers cross
allows left visual field information from both eyes to go to right hemisphere and vice versa
Optic Tract - visual pathway
After chiasm
GN (Lateral Geniculate Nucleus) - visual pathway
Relay in thalamus
Optic Radiations - visual pathway
Pathway to cortex
Primary Visual Cortex (V1) - visual pathway
Occipital lobe
Midget RGCs → Parvocellular Pathway
Small receptive fields
Specialized for: COLOR, fine detail, high spatial resolution
Sustained response
Parasol RGCs → Magnocellular Pathway
Large receptive fields
Specialized for: MOTION, low spatial resolution
Transient response
Small Bistratified RGCs → Koniocellular Pathway
S-cone pathway inputs (blue)
Low acuity visual information
Support
Three Opponent Channels
Red vs. Green: L (red) cones vs. M (green) cones
Blue vs. Yellow: S (blue) cones vs. combined L+M (yellow)
Dark vs. Bright (Luminance): Combined L+M+S
Primary Visual Cortex (V1) Function
First cortical area to receive visual input; processes basic features like edges and orientation
Cortical Magnification
Disproportionately large representation of fovea in V1 → higher acuity in central vision
more brain area is devoted to parts of the body or visual field that is needed for high precision
Dorsal Visual Pathway ("Where/How" - Perception for Action)
V1 → Parietal regions
Spatial awareness, guiding actions
Motion processing
perception for action: motion & spatial location
Ventral Visual Pathway ("What" - Perception for Recognition)
V1 → Temporal regions
perception for recognition: objects, faces, color
Object recognition
Face processing
Color processing
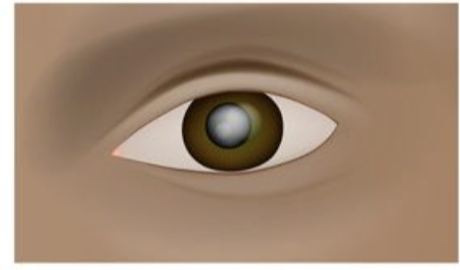
Cataract
Opacity (clouding) in the LENS that blocks light from reaching retina
Often age-related due to UV exposure
Surgical lens replacement needed

Scotoma
Area of impaired or lost vision in visual field
Can result from damage anywhere from: Retina → Optic nerve → V1
Brain often "fills in" missing region, so patient may not see black spot unless in center
MONOCHROMACY: Rod Monochromacy
All cones non-functional; vision relies entirely on rods
Complete color blindness
Low visual acuity (no functional fovea, only periphery working)
Sees in black and white only
MONOCHROMACY: Blue-Cone Monochromacy
Only rods & S (blue) cones functional
Can see ~100 colors (vs. normal 10 million)
Sex-linked; men most likely to have it
DICHROMACY (Two Cone Types): Protanopia
Missing: L (red) cones
Red-green (X-linked)
DICHROMACY (Two Cone Types): Deuteranopia
Missing: M (green) cones
Red-green (X-linked) - MOST COMMON dichromacy
DICHROMACY (Two Cone Types): Tritanopia
Missing: S (blue) cones
Blue-yellow (NOT sex-linked) - VERY RARE
ANOMALOUS TRICHROMACY (MOST COMMON)
All three cone types present BUT shifted sensitivity
ANOMALOUS TRICHROMACY: Protanomaly
red-weakness
ANOMALOUS TRICHROMACY: Deuteranomaly
green-weakness - MOST COMMON colorblindness overall
ANOMALOUS TRICHROMACY: Tritanomaly
blue-weakness
Tetrachromacy
Condition where person has 4 cone types (2 types of L-cones)
Can see ~100 MILLION colors (vs. normal 10 million)
2-3% of women
** Brain circuitry can form normally even with extra cone type!
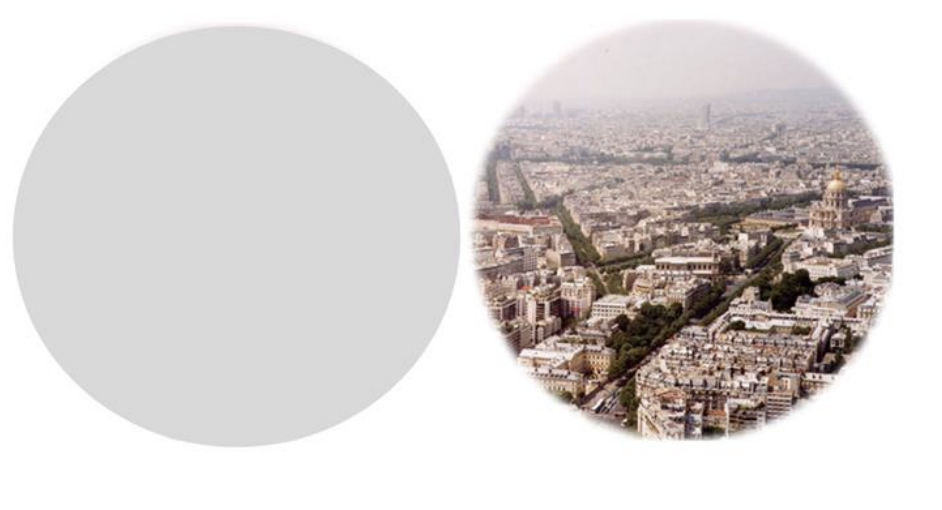
Visual Field Defects (Hemianopsias): Unilateral Field Loss
Complete blindness in ONE eye
damage: Optic nerve (before chiasm); tumor or trauma
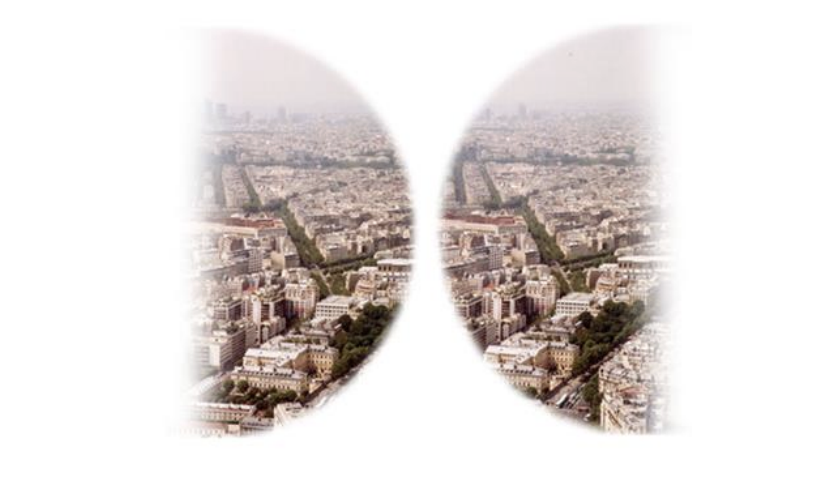
Visual Field Defects (Hemianopsias): Bitemporal Hemianopsia
Outer (temporal) halves (hemifields) of BOTH eyes
damage: Optic chiasm (often tumor)
Visual Field Defects (Hemianopsias): Binasal Hemianopsia
Inner (nasal) halves of (hemifields) BOTH eyes
damage: Uncrossed fibers (calcified carotid arteries); hydrocephalus

Visual Field Defects (Hemianopsias): Homonymous Hemianopsia
SAME half of both eyes (e.g., right half of both)
damage: Opposite V1 or optic tract (e.g., left V1 → right hemianopsia); stroke, trauma

Sensation
First stage of sensory function - information at peripheral sensory receptors
Perception
Process of recognizing, organizing, and interpreting sensory information
Optic Radiation
nerve fibers carrying visual info from thalamus - V1 (primary visual cortex)
Optic Radiation: inferior retina
temporal love (meyer’s loop): carries upper visual field
Optic Radiation: superior retina
occipital lobe: carries lower visual field
Visual Field Mapping: left visual field
right brain
Visual Field Mapping: right visual field
left brain
Blindsight
Phenomenon where people with V1 damage are perceptually BLIND but show some unconscious response to visual stimuli
ability to respond to visual stimuli w/o conscious awareness (blind)
damage to V1
alternative pathways send info directly to motion area (MT)
Visual Agnosia
Inability to recognize objects, scenes, or faces DESPITE intact elementary visual perception
vision intact, but object recognition impair
damage occurs after V1
Visual Agnosia: Apperceptive Agnosia
Cannot name, copy, OR recognize objects (impaired shape perception)
BUT knowledge of objects is intact
Visual Agnosia: Associative Agnosia
Cannot identify OR name the objects (meaning disconnected from perception)
BUT can perceive object shape and copy
Object Agnosia
cannot recognize objects by sigh, but can recognize by touch or sound
Vision neurons: fovea (center vision)
lots of neurson
Vision neurons: peripheral vision
fewer neurons
Gestalt Grouping & Object Recognition
brian uses prior knowledge to organize visual input
Fusion Face Area (FFA)
specialized for face recognition, active in both hemispheres
Prosopagnosia
(face blindness) Inability to recognize FACES despite normal vision and object recognition
Associative:
Prosopagnosia (Apperceptive)
problem with recognizing face vs. other objects (fruit face)
Prosopagnosia (Associative)
able to tell it’s a face, but problem with recognition
Capgras Syndrome
belief that a loved one has been replaced by an identical impostor
face recognition works, but emotional response is disconnected
Rare delusional misidentification syndrome
Fregoli Syndrome
belief that multiple people are actually one person in disguise
over-activation of face familiarity systems
Rare delusional misidentification syndrome
Simultanagnosia
inability to perceive more than one object at a time in a scene
can identify individual items, but cannot understand the whole scene
Simultanagnosia: Dorsal Simultanagnosia
perceives only one stimulus at a time, single word or object, may appear blind
Simultanagnosia: Ventral Simultanagnosia
Can see multiple objects but cannot recognize them, one at a time
Can navigate and count but cannot read
Cerebral Achromatopsia (Cortical Color Blindness)
loss of color in both visual field
caused by cortical lessions: stroke, trauma, dementia
Cerebral Achromatopsia: Hemiachromatopsia
Loss of color in ONE half of visual field
Cerebral Achromatopsia: Transient
Temporary loss (hours) from TIA or transient ischemic attack
Akinetopsia (Motion Blindness)
Inability to perceive MOTION smoothly (which affects temporal processing)
series of still images
damage to V5 and MT
stroke, trauma, antidepressants
Troxler Effect
Visual phenomenon where fixating on one point causes stationary peripheral images to fade