3. Post-traumatic stress disorder
1/47
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
What is the history of PTSD?
previously called: “soldier’s heart”, “Shell Shock”, “Battle Fatigue”, “delayed stress”
PTSD originally defined in DSM III (1980)
medical diagnosis led to a search for biological markers
Greater understanding has led to wider diagnosis in the general population
What is the key criteria for PTSD which isn’t involved in other disorders?
A defined stressor events
What are the 5 key symptoms/criteria of PTSD?
A stressor event
Intrusion symptoms
Alterations in arousal/ reactivity
Negative alteractions in cognition/ mood
Avoidance behaviours
What is complex PTSD?
Trauma related to multiple events over an extended period of time
How can we define an experienced stressor in order to diagnose PTSD?
Person expose to: death, threatened death, actual or threatened serious injury, or actual or threatened sexual violence via:
direct exposure
witnessing trauma
learning relative/ close friends was exposed to a trauma
indirect exposure to aversive details of trauma
How can we define alterations in arousal and reactivity in order to diagnose PTSD?
Trauma related arousal and reactivity began or worsened after trauma
irritability or aggression
risky or destructive behaviour
hypervigilance
heightened startle reaction
difficulty concentration
difficulty sleeping
How can we define intrusion symptoms in order to diagnose PTSD?
Traumatic event persistently re-experiences via
unwanted upsetting memories
nightmares
flashbacks
emotional distress/ physical reactivity after exposure to reminders
How can we define Negative alterations in cognitions/mood in order to diagnose PTSD?
Negative thoughts/feelings began or worsened after trauma
inability to recall key features of the trauma
overly negative thoughts/assumptions about oneself/the world
exaggerated blame of self or others for causing the trauma
negative affect
decreased interest in activities
feeling isolated
difficulty experiencing positive affect
How can we define avoidance in order to diagnose PTSD?
Avoidance of trauma-related stimuli after the trauma, in the following ways:
trauma-related thoughts or feelings
trauma-related external reminders
What are the 3 criteria that symptoms have to meet in order to get a diagnosis?
symptoms last for more than 1 month
symptoms create distress of functional impairment
symptoms are not due to medication, substance use or other illness
Which brain regions are implicated in intrusion symptoms?
rostral anterior cingulate cortex
ventro-medial prefrontal cortex
amygdala

Which brain regions are implicated in avoidance?
cingulate
amygdala
hippocampus

Which brain regions are implicated in cognition and mood?
medial prefrontal cortex
cingulate
thalamus
amygdala
hippocampus
Which brain regions are implicated in arousal and reactivity?
dorsal anterior cingulate cortex
ventromedial prefrontal cortex
orbitofrontal cortex
amygdala
PAG
LC
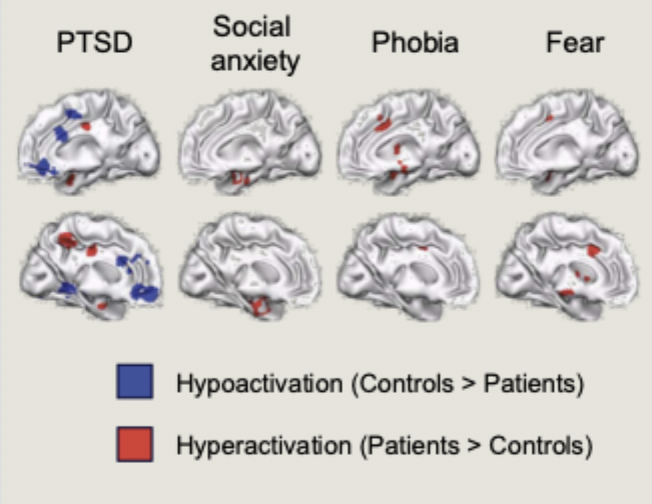
What did Etkin & Wager’s meta-analysis find comparing fMRI studies of PTSD, social anxiety, phobias and fear?
All studies examined brain activity when attending to disorder relevant stimuli
And what did PTSD specifically show
patients with any of the three disorders showed greater activity than matched comparison subjects in the amygdala and the insula
PTSD specifically showed hypoactivity in the prefrontal cortex, thalamus and the cingulate
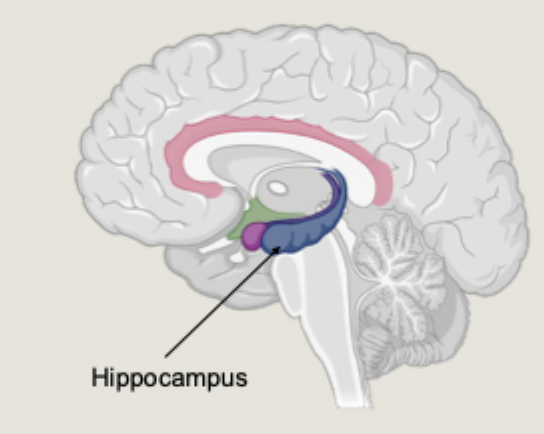
How is the Hippocampus implicated in PTSD?
part of the limbic system
involved in memory processing of all kinds
PTSD is a condition centred around an emotional (traumatic) memory
a reduction in hippocampal volume is one of the most consistently reported differences in brain structure when looking at PTSD
What did Logue et al’s meta-analysis find regarding hippocampal size in PTSD patients?
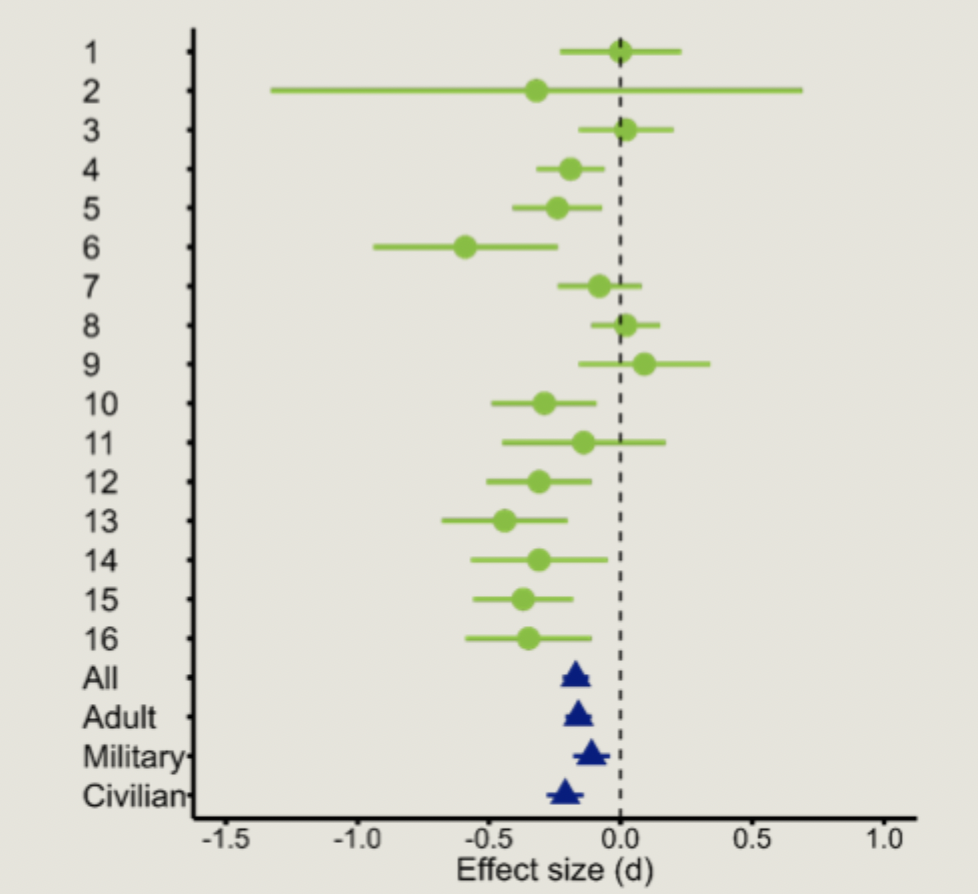
A smaller hippocampus = increased chance of having PTSD
What did Gilbertson et al find in their MZ twin study examining if hippocampal volume was the cause or result of a trauma?
in this study one twin was combat exposed and one was not
results showed hippocampal volume predicted severity of PTSD in the combat twin and the non-combat exposed twin
smaller hippocampus increases likelihood of mental illness
A risk factor for PTSD, not a result of trauma
How does the neurotrophic hypothesis of depression influence the conclusion that hippocampal differences influence PTSD
Could the involvement of the hippocampus be due to depression rather than PTSD?
Human post-mortem data shows decreased BDNF in hippocampus
this impairs memory processes
demonstrates neuroplasticity at a very specific anatomical level
not clear if this is a cause or a result of depression
What is the hippocampus involved in during “online” states?
During online states such as learning or memory tasks, the hippocampus is involved in encoding or retrieving memories
What is the hippocampus involved in during “offline” states?
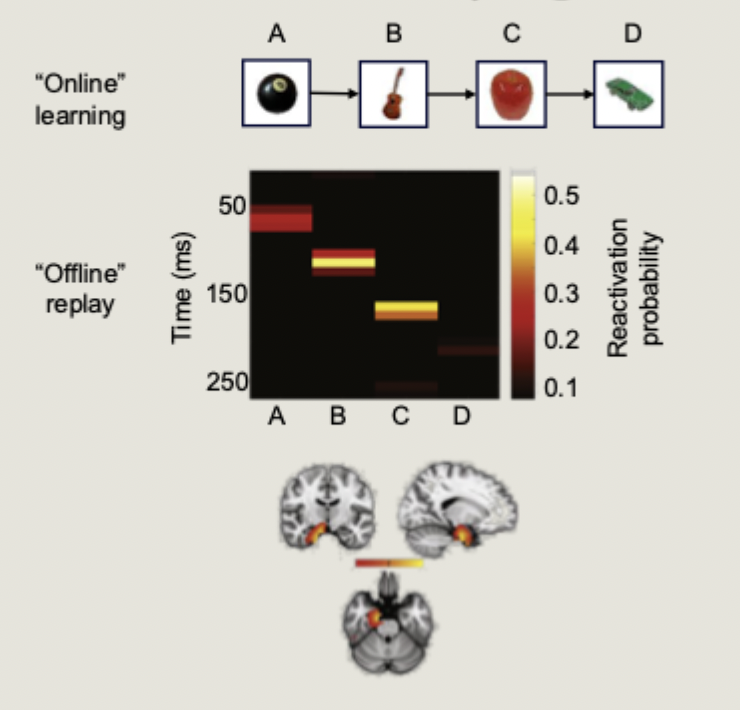
During offline states like rest or sleep, the hippocampus spontaneously replays previously encoded information.
Liu et al (2019): Used MEG to show memory replay during periods of rests in humans
How might hippocampal memory replay be involved in PTSD?
Spontaneous replay of traumatic replays could trigger memory intrusions and “flashbacks in PTSD
What is the think/no-think paradigm?
An experimental task to test memory suppression ability
What did Catarino et al find using the think/no-think to compare memory suppression in PTSD patients compared with trauma exposed controls?
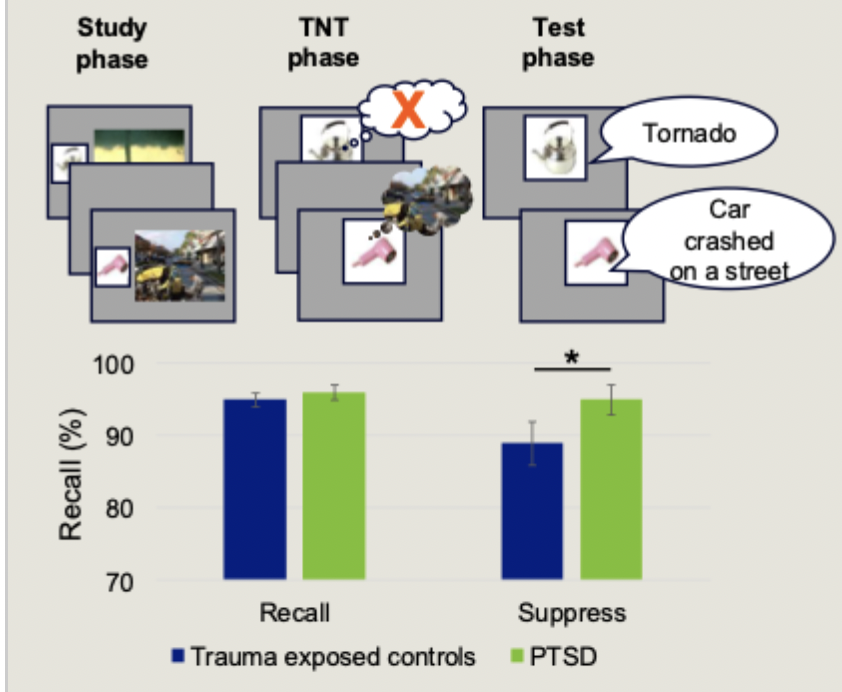
PTSD patients showed worse memory suppression, indicated by better memory for suppressed items
memory suppression ability correlated with thought control ability and PTSD symptoms
didn’t seem to show ability to memory suppress
DLPFC vs Hippocampus: when does each region activate?
DLPFC: activates when we engage top-down regulatory control
hippocampus: activates when we retrieve a memory
What did Benoit et al find successful memory suppression requires from the DLPFC and the Hippocampus
Successful memory suppression requires increased activation of the DLPFC and decreased activation of the hippocampus (in healthy ppts)
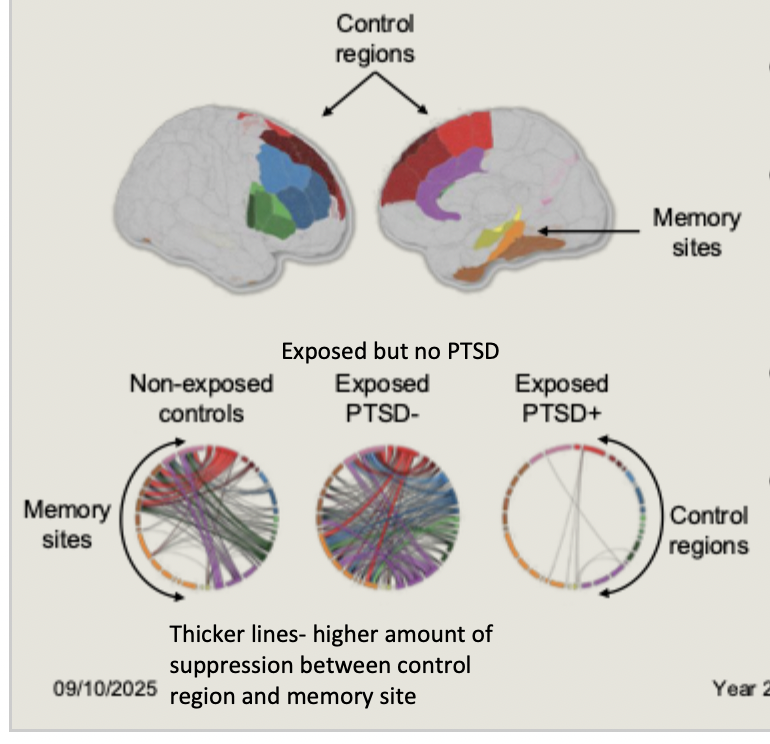
What were the 3 groups in Mary et al study of memory suppression in survivors of the 2015 Paris terrorist attacks?
non-exposed controls
exposed pps who didn’t develop PTSD (PTSD-)
those exposed who did develop PTSD (PTSD+)
In Mary et al study of Paris terrorist attack survivors, what was found across ppt groups during no-think trials?
What was the conclusion?
during no-think trials, PTSD- and non-exposed controls showed widespread suppression of hippocampus by prefrontal control regions
PTSD+ showed no top-down suppression of memory retrieval networks
Memory suppression is a general risk factor that influences vulnerability or resilience to PTSD following trauma
How much time is spent in each sleep stage?

N1 - 5%
N2 - 45%
N3 - 25%
REM - 25%
What are the different examples of sleep disturbances common in PTSD?
insomnia
longer sleep latency
more awakenings during the night
shorter total sleep time
frequent nightmares (trauma replay)
disruptive nocturnal behaviours (night terrors, sleep paralysis, dream enactment)
How is arousal seen in PTSD?
Increased 24-hr cognitive, emotional, physiological and cortical hyperarousal
How is cortical hyperarousal seen during sleep
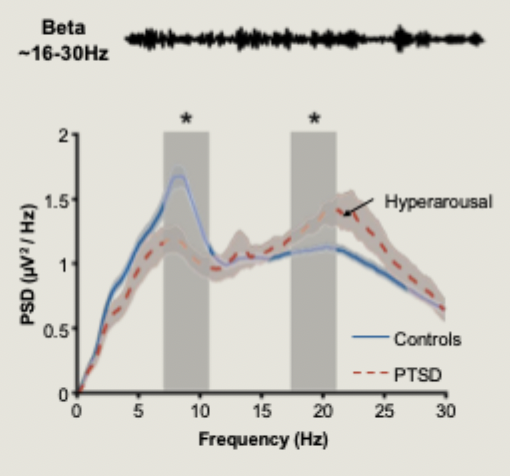
during sleep, cortical hyperarousal indexed as increased power in high frequencies (beta and gamma bands)
Denis et al (2023): increased levels of cortical hyperarousal during sleep in PTSD patients
hyperarousal suring sleep interacts with other domains of hyperarousal experienced during the day
How does sleep consolidate memories and in which stages?
sleep consolidates memories by strengthening memory traces during NREM sleep
sleep preferentially consolidates emotionally charges experiences
What did Denis et al find in memory is amplified by sleep?

Sleep amplifies memory for negative scene components at the expense of accompanying background information
What is the affective tone of a memory?
the physiological reactivity and emotional response
What did van der Helm find when ppts were asked to rate emotional images after sleep? What was this result associated with and what does it suggest?

following sleep, participant rated emotional images as less emotionally intense
this was associated with reduced amygdala activity after sleep, and correlated with amount of time spent in REM sleep
suggests NREM sleep strengthens memory representations
while REM sleep reduces affective tone
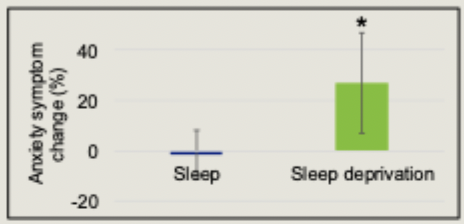
What did Ben Simon et al find examining participant’s anxiety levels before and after a night of sleep deprivation?
Significantly elevated anxiety levels after sleep deprivation
What happened in the brains of Ben Simon et al’s sleep deprived patients when shown a series of emotional pictures?
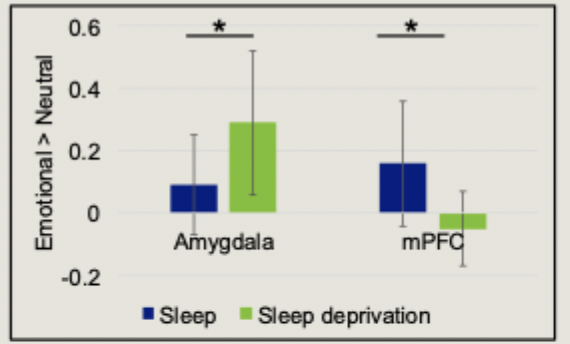
sleep deprived participants showed greater amygdala activity and reduced PFC activity when viewing negative images
What did Harrington et al find in the brain when sleep deprived patients took part in think/no-think task?
more intrusions of suppressed memories after sleep deprivation
this coincided with reduced DLPFC activity and increased hippocampus activity during suppression trials
therefore, sleep deprivation disrupts memory control
What did Klein et al find when showing ppts an experimental analogue film either in the morning or in the evening and then sleeping after?
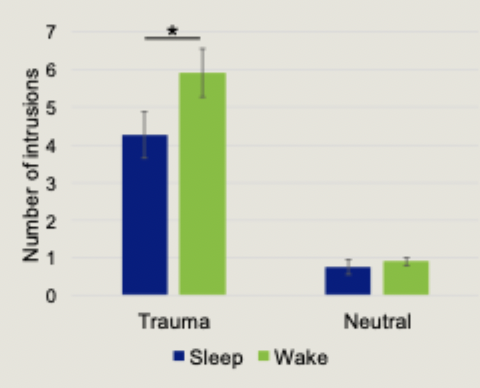
Sleep participants reported fewer intrusions and lower associated distress than wake participants
What is the theory of extinction as treatment of PTSD?

pairing the conditioned stimulus and unconditioned stimulus leads to the conditioned response
extinction is the reduction of the CR by repeated presentation of the CS in the absence of the US
extinction retention is essential for long-term attenuation of fear responses
What did Milad et al find when PTSD patients and trauma exposed controls underwent a fear conditioning and extinction programme?
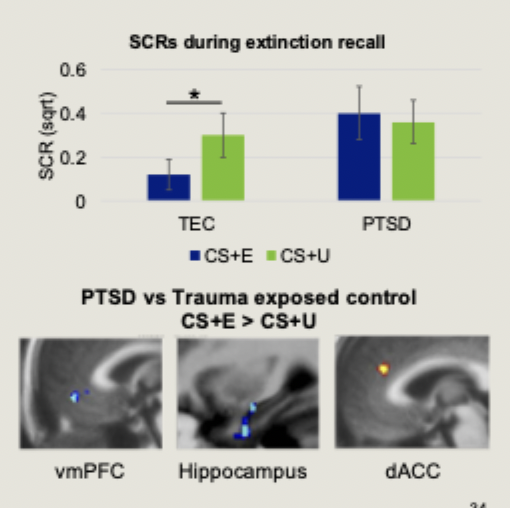
no group differences in fear acquisition or extinction learning. PTSD patients can extinguish fear
24 hours later, PTSD patients were unable to retain memory for extinction
This was associated with reduced vmPFC and hippocampal activity during extinction recall
a failure to retain extinction memories could underpin PTSD development and maintenance
What effects to hyperarousal and slow oscillation/sleep spindles have on extinction recall?

hyperarousal impairs extinction recall
Slow oscillation and sleep spindles enhance extinction recall
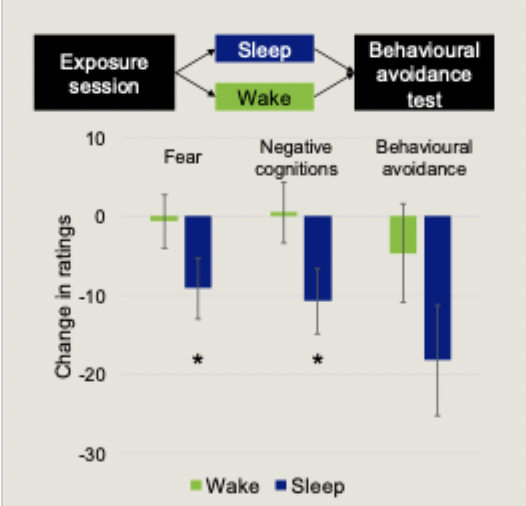
What is exposure therapy? And what enhances it’s effectiveness
exposure therapy is one of the main psychological therapies for PTSD
also used for treating phobias, panic disorder, social anxiety disorder and more
therapist creates a safe environment to expose patients to the thing they fear
exposure therapy fosters new extinction learning in a safe environment
Kleim et al: Sleeping after an exposure session enhances therapeutic effectiveness
What is involved in Eye movement desensitisation and reprogramming (EMDR)
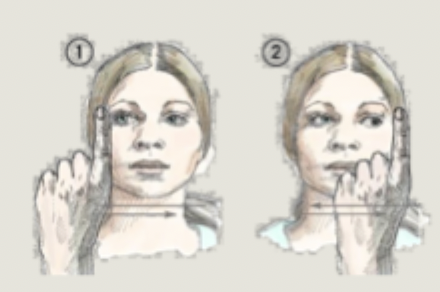
the patient follows with their eyes a rapidly moving stimulus (often the clinician’s finger) while holding different aspects of a traumatic event in mind
works as well as exposure therapy
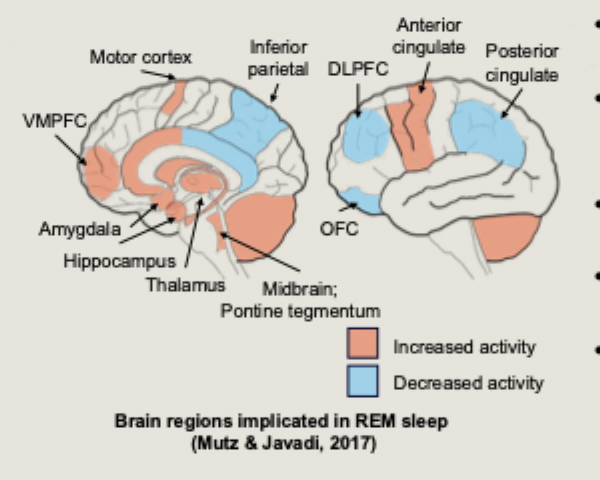
What is the suggested relationship between EMDR and REM sleep?
one theory is that EMDR is related to memory processes
PTSD arises when the brain fails to appropriately consolidate traumatic memories
REM sleep is important for emotional memory re-processing
could EMDR induce a similar physiological state to REM?
What did Rousseau et al find that EDMR changes in the brain?
EMDR changes activity in the PFC, amygdala, thalamus and caudate nucleus
What is targeted memory reactivation and how is it used with EMDR?
an experimental technique to bias memory reactivation during sleep
sound cues associated with learning are played back to the participant while they are sleeping
van der Heijden et al 2024 played EMDR clicks during periods of slow wave sleep - showed significant improvements in PTSD avoidance symptoms.